
Abstract
This study evaluated the effectiveness of a depression literacy program on depression literacy, mental health stigma, and help-seeking attitude among adolescents with a monthly household income of RM3900 a month or less (B40) in Malaysia. The program included a lecture, mental awareness activities, and a short video on depression. Residents from a boarding school for lower income families were involved in this study (N = 101); 53 of them underwent the program and another 48 served as the control group. There were significant improvements for all variables in the intervention group (better depression literacy, reduced self-stigma, reduced negative beliefs on mental health, and increased help-seeking) at posttest. However, the results were sustained at 3-month follow-up only for the depression literacy, mental help-seeking attitude, and self-stigma of seeking help variables when compared with the control group. The findings highlight the need to improve the program to enhance the effectiveness and sustainability of the outcomes.
Keywords
Depression literacy has an impact on stigma and help-seeking attitudes. Adolescents from the bottom 40% socioeconomic group are at a compounded risk of suffering from depression and other mental health issues. Most current mental health literacy programs do not specifically target adolescents with depression or had depended on 1 mode of delivery (eg, presentation of information) which may not be appealing to the adolescent population.
This dynamic depression literacy program targets lower socioeconomic adolescents with elevated depression scores, to decrease stigma and improve help-seeking attitudes through a combination of intervention modes, which are small-group activities, video animation, and information presentation.
The Depression Literacy Program which employs multiple modes of delivery has been shown to be effective in increasing depression literacy and help-seeking attitudes while decreasing stigma toward mental illness. Thus, it should be implemented nationwide.
Introduction
There are various factors that prevent individuals from seeking help when they experience emotional disturbance. The barriers may originate from difficulty accessing treatment from health service providers, 1 cost and financial considerations,2,3 and prejudice, ill-treatment, and bias from health providers. 4 The individuals themselves may also have personal issues that hinder them from seeking help, such as a negative perception about confidentiality and the effectiveness of therapy, 5 a lack of insight about the illness and the need for treatment, 6 belief on self-efficacy to get help, 7 and stigma about the mental disorder or the act of seeking help for it.8,9
Stigma has been listed as one of the top reasons that caused those affected by mental illness to forgo mental care. A recent review of 144 studies involving 90 189 participants indicated that stigma was the fourth out of 10 highest barriers to help-seeking. 10 The main types of stigma preventing people from accessing care were “treatment stigma,” that is, the stigma associated with using mental health services or receiving mental health treatment, and “internalized stigma,” such as shame and embarrassment. 10 The direct impact of public stigma on the utilization of psychological services has been indicated in earlier studies. An individual is more likely to hide his or her psychological concerns and avoid treatment if there is fear of stigma from society. 11 A mentally ill patient could be perceived as being “crazy” 12 and dangerous. 13 Meanwhile, those who seek help were viewed less favorably 14 and are rated as being more emotionally unstable. 15 The other type of stigma, namely self-stigma, also plays a significant role in the decision whether to seek and receive help or not. Self-stigma has been explored by a number of researchers.15,16 Recent studies have established its role in predicting psychological help-seeking attitudes.17,18 Studies by Vogel et al18-20 revealed that self-stigma is indeed a unique and different concept of stigma that independently predicted the help-seeking attitude of an individual. Although self-stigma may originate from external influences such as societal expectations, the complex internalization of these negative perceptions and prejudices could lead to shame and loss of self-esteem. 21 This subsequently affects an individual’s attitude and willingness to seek counseling or therapy.22-24
An estimated 29.2% of the Malaysian population suffer from a mental disorder, 24 and 11.0% of adolescents reported severe depression. 25 However, there is a low rate for help-seeking for mental illness, and psychiatric disorders are treated at a late stage. 26 This could stem from a lack of knowledge and cultural variations such as making a spiritual rather than a medical diagnosis for the mental disorder. 27 There is also evidence of perceived stigma toward mental illness among patients, caregivers and health care providers.28-31 In spite of the magnitude of the problem, there is a paucity of intervention studies which focus on improving mental health literacy, stigma, and help-seeking attitudes among mentally ill adolescents in the Southeast Asian region. For this reason, a concise module on depression and the stigma that surround it was developed and evaluated in a depression literacy program for the Malaysian population, specifically among adolescents.
Mental health literacy has a clear relationship with the help-seeking attitude of an individual. 32 Those who have better information about the symptoms, causes, and treatment of mental illnesses generally have more favorable and positive attitudes on seeking mental help. 32 Among adolescents, a relationship was observed between low mental health literacy and higher levels of depression. 33 However, adolescents who knew how to obtain mental health services and maintain a positive mental health reported higher mental well-being levels. 34 Unfortunately, the rate of health literacy, especially mental health literacy, in emerging economies such as Malaysia is low. As indicated by the National Health and Morbidity Survey, adequate health literacy was observed for only 5.1% among those with a secondary school education. 35
This study seeks to test the efficacy of the program on the bottom 40% (B40) population in Malaysia. B40 refers to households with an average income of RM3900 a month or less. They are the bottom group in the 3 household categories in Malaysia (bottom 40%, middle 40%, and top 20%) 36 and includes those who earn an income below the poverty line index. Poverty is closely related with the increased incidence of mental illness.37-39 Lower socioeconomic status is usually associated with a lower educational level, and this is closely associated with lower levels of mental health literacy. 39 In Malaysia, adequate health literacy was observed in only 3.6% among those with a monthly household income of less than RM3000, compared with 11.6% among those whose household earned above RM6000. 35 Therefore, there is a need to target the mental health literacy of adolescents from the lower socioeconomic background.
There are a number of mental health literacy programs developed or adapted for adolescents, such as the Youth Mental Health First Aid (YMHFA), Question Persuade Refer (QPR), and Signs of Suicide (SOS).40-44 A review of mental health interventions for adolescents revealed that most of these programs were developed and tested in high-income countries, with a few notable exceptions from Thailand, Nigeria, Tanzania, and Brazil. 42 In addition, most had targeted suicide and self-harm, 44 or a number of common mental health problems (eg, YMHFA). 40 As most mental health literacy programs do not specifically target depression literacy or had been developed in high-income contexts, this study aims to demonstrate the efficacy as well as stability of a Malaysian Depression Literacy Program immediately after the program ended and at 3-month follow-up among adolescents with elevated depression levels.
Method
Sample Selection
Participants of this study were recruited from a boarding school managed by a nongovernmental organization located in Rawang, Selangor. There were 156 students from B40 households from all over Malaysia in this school aged between 13 and 17 years old. The warden of the boarding school selected 127 students who were deemed to benefit from the Depression Literacy Intervention, such as those observed to be depressed or had exhibited problematic behavior. The researchers screened the participants based on their depression level measured by the Kutcher Adolescent Depression Scale (KADS) 45 to include only adolescents with significant depression symptoms in the study, that is, students who scored above the 50th percentile on the KADS.
Instruments
The effectiveness of the program was measured by 4 instruments. The Depression Literacy Scale (D-Lit) by Griffiths et al 46 is a 22-item scale which assesses depression-specific mental health literacy (eg, “People with depression may feel guilty when they are not at fault”). There are 22 items in the questionnaire and the participants choose 1 response from 3 options: “True,” “False,” or “Don’t Know.” One point is given for each correct response, and a higher depression literacy is indicated by higher scores. The original questionnaire has an internal consistency of α = .70. 46 In this study, the questionnaire achieved the internal consistency of α = .831.
The Mental Help Seeking Attitude Scale (MHSAS) by Hammer et al 47 consists of 9 items used to measure an individual’s evaluation of help-seeking from mental health services if they find themselves dealing with a mental health concern. Participants respond on a 7-point semantic differential scale anchored by bipolar adjectives (good vs bad). The questionnaire has an internal consistency of α = .93 to .94. 47 In this study, the questionnaire achieved the internal consistency of α = .928.
The Self-Stigma of Seeking Help Scale by Vogel et al consists of 10 items which measure an individual’s level of self-stigma experienced when they consider seeking professional mental health services (eg, “I would feel inadequate if I went to a therapist for psychological help”). Participants answer on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Higher scores indicate higher self-stigma. The questionnaire has an internal consistency of α = .86 to .90. 25 In this study, the questionnaire achieved the internal consistency of α = .747.
Beliefs Toward Mental Illness (BMI) by Hirai and Clum 48 is a 21-item questionnaire designed to measure negative and stereotypical views of mental illness. Three subscales derived from factor analysis were dangerousness, poor social and interpersonal skills, and incurability. Participants answered on a 6-point Likert scale ranging from 0 (completely disagree) to 5 (completely agree). Higher scores reflect more negative beliefs on mental illness. The questionnaire has an internal consistency of α = .89 to .91. 48 In this study, the questionnaire achieved the internal consistency of α = .904.
Procedure
This was a quasi-experimental study using preintervention and postintervention measures with a 3-month follow-up to evaluate the effectiveness of the Depression Literacy Program. Out of the 127 participants referred by the boarding school warden, 101 participants who reported depression scores above the 50th percentile on the KADS and who came from Selangor and Kuala Lumpur were assigned to the intervention group (n = 53); 48 participants who scored similar levels of depression and came from other states were allocated into the control group whereas the rest who scored lower levels of depression were excluded from the study. Each participant and their guardian gave informed consent to voluntarily participate in this study.
For the intervention group, the participants received depression literacy intervention in the form of small group activities, an explanatory talk, and an animation video. The development of the program was based on a thorough literature review of existing mental health programs.40-44 Facts on mental health statistics in Malaysia, especially among adolescents, have also been incorporated. To build activities to elicit adolescents’ expression of knowledge and perceptions on depression, a brainstorming session was conducted among the researchers (N.I., A.M.S., and S.S.). The lead author (N.I.) wrote the script and commissioned the animation video on depression. The following are features unique to the Malaysian depression literacy program:
Information on mental health and depression presented in the lecture were culture-specific and context-specific to Malaysia, for example, the importance of spirituality and religion, and statistics on mental health in Malaysia.
The animation video depicted Malaysian characters and settings and was delivered in the Malaysian language.
Before the intervention, they answered a set of questionnaires to gather pretest data for depression literacy, mental help-seeking attitude, self-stigma on seeking help, as well as negative beliefs that they have on mental illness. After pretest was completed, participants were divided into multiple small groups and participated in the following activities:
Who am I? Participants draw pictures based on their perception of depression and the healthy mental state, followed by a group discussion.
Post-it graffiti: Participants express their thoughts and beliefs of mental illness by writing them down on a post-it sticker and paste it on a board, followed by a group discussion.
Body drawing: Participants express their knowledge and perceptions of a person with depression by writing them down on a body picture, followed by a group discussion.
The tasks were intended to elicit their current knowledge and understanding in identifying symptoms of depression, the stigma they have on depression and their initiatives in helping friends who are seen to be mentally disturbed and troubled. Facilitators evaluated if the participants expressed wrongful knowledge or stigmatizing attitudes on depression based partially on the vignette procedure by Mannarini and Boffo49,50: (1) etiological beliefs (eg, failure to adopt a biopsychosocial perspective or attributing moral weakness as the reason for developing depression); (2) stereotypes (eg, always dressed sloppily or smelled bad); (3) the degree of dangerousness; and (4) the desire for social distance. Facilitators then discussed the correct facts on depression, what consists of a stigmatizing attitude, and the impact of stigma on persons with depression.
After completing the activities, the program then continued with the presentation and explanation of depression. It covered topics on causes of the illness and risk factors (eg, a biopsychosocial perspective), 51 symptoms of depression (eg, depressed mood, anhedonia), 51 and steps to overcome and how to treat the illness (eg, seeking professional help, psychopharmacological interventions). 52 Participants were also informed of the stigma that surround this particular mental disorder. Facilitators distinguished the 2 types of stigma that exist, which are the stigma toward depression itself, as well as the stigma that hinders a person from seeking help when they experience depression. Facilitators also presented information on the myths and facts of mental illness.
Last, to strengthen the participants’ understanding on the symptoms and treatment of depression, the participants watched a 4-minute depression-related animation video. This video was produced based on the Major Depressive Disorder symptoms stated in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 51 The rationale of placing the video at the end of the program was based on the peak-end rule, a psychological theory proposed by Kahneman et al, 53 whereby the remembered feelings of an experience were predicted by the most intense (peak) experience near the end of an event. This means that the pleasant or unpleasant memory of an individual incident or event depends on this crucial timeframe. This particular theory has been tested in medical, financial, and workplace settings.54-56 Table 1 outlines the content of the intervention program.
Details of the Depression Literacy Program for B40 Adolescents.

Participants were then given the same set of questionnaires to measure their response immediately after completing the depression literacy program (posttest data). The same procedures were replicated for the control group, with the exception that they were not given any intervention, and therefore no posttest measures were collected. To determine the stability of the program, participants in both the intervention and control groups were given the same set of questionnaires 3 months after completion of the program (follow-up). This study was granted ethical approval from Ethics Committee from the Universiti Kebangsaan Malaysia (PPI/111/8/JEP-2018-267). Figure 1 outlines the procedures of the study.
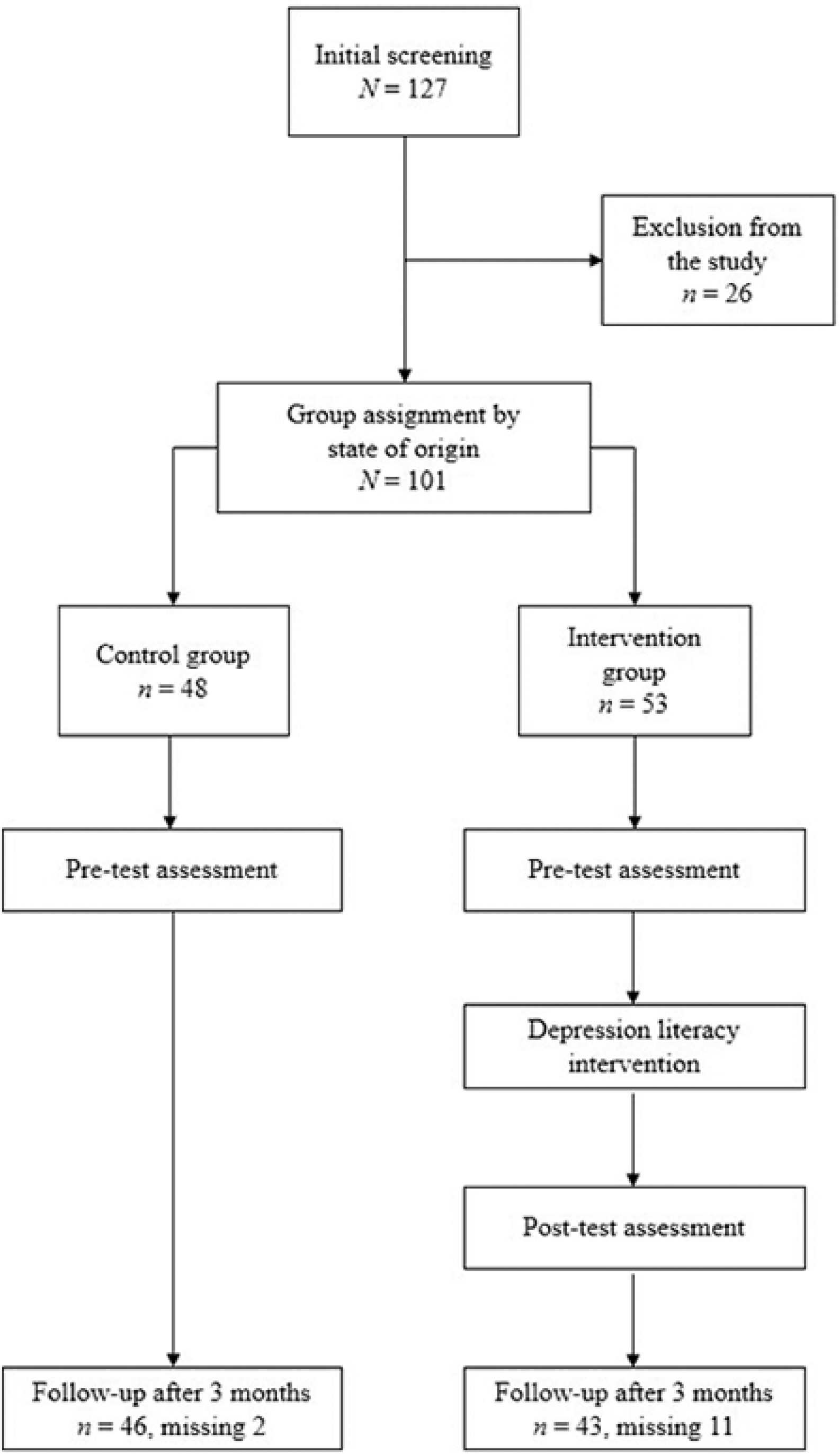
Flow chart of the depression literacy program study.
Results
A total of 101 adolescents (mean age = 14.61, SD = 1.39) participated in the study. The cumulative dropout rate for this study at 3-month follow-up was 12.1%. Missing data were deleted listwise. At baseline, there were more women in both the control group (56.3%) and the intervention group (64.2%). Most of the participants in the control group were 17 years old (25%), followed by 14 (22.9%) and 13 (20.8%), and the rest were those aged 15 and 16 years. For the intervention group, most of participants were aged 14 (35.9%). More than half of the control group participants came from households with income between RM1000 to RM3000 (58.5%) and only 1 participant (1.9%) was from the RM3001 to RM3860 household income group. Similarly, most participants in the intervention group were from the RM1000 to RM3000 household income group (54.2%). Most participants in the control (62.5%) and intervention (52.8%) groups came from moderate size families with 4 to 6 siblings. They were also mostly the older siblings in their family. A total of 64.6% participants from the control group and 62.3% from the intervention group lived with both of their parents when they are away from school. Chi-square analyses revealed that there were no significant differences (P > .05) regarding the demographic information between the intervention and control group (Table 2).
Demographic Data of the Participants at Baseline (N = 101).

The repeated measures analysis of variance (ANOVA) was conducted to evaluate the effectiveness of the Depression Literacy Program to increase depression literacy (D-Lit) and mental help-seeking attitude (MHSAS), and to decrease self-stigma on help-seeking (SSOHS), and negative beliefs on mental illness (BMI). The program significantly increased MHSAS at posttest (P < .001) and follow-up—P = .034; F(2, 84) = 9.939, P < .001,
Repeated Measures Analysis of Variance for the Intervention Group at Baseline (T1), Posttest (T2), and 3-Month Follow-Up (T3) (n = 43).
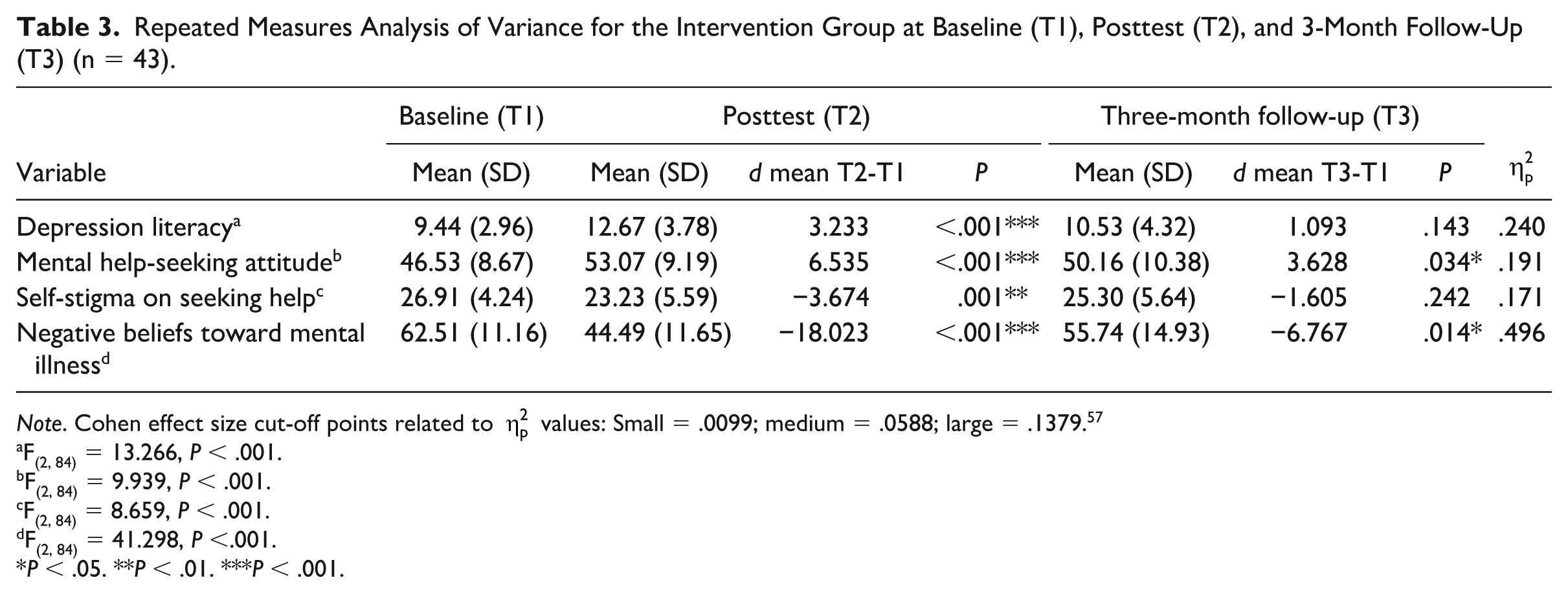
Note. Cohen effect size cut-off points related to
F(2, 84) = 13.266, P < .001.
F(2, 84) = 9.939, P < .001.
F(2, 84) = 8.659, P < .001.
F(2, 84) = 41.298, P <.001.
P < .05. **P < .01. ***P < .001.
The 2 × 2 mixed model ANOVA was conducted to compare the effectiveness of the depression literacy program on the intervention group upon control group at 3-month follow-up, while controlling the pretest scores of the variables. Results indicated that at 3-month follow-up, significant results were maintained for increased D-Lit—F(1, 87) = 4.343, P = .040,
The 2 × 2 Mixed Model Analysis of Variance for the Intervention and Control Group at Baseline (T1) and 3-Month Follow-Up (T3).

Note. d = difference. Cohen effect size cut-off points related to
F(1, 87) = 4.343, P =.040.
F(1, 87) = 8.587, P =.004.
F(1, 87) = 20.517, P < .001.
F(1, 87) = 0.987, P = .323.
P < .05. **P < .01. ***P < .001.
Discussion
The goals of the Depression Literacy Program was to build awareness and understanding about depression, decrease stigma on mental illness, and ultimately increase the willingness to seek help when facing mental health problems among adolescents from B40 households. The results revealed that this program was successful in meeting these goals where the participants were found to have better depression literacy, attitudes toward seeking help, decreased self-stigma toward seeking mental help, as well as decreased negative beliefs on mental illness after the program. However, when compared with the control group at 3-month follow-up, only negative BMI was not significant. Therefore, it could be concluded that the Depression Literacy Program is effective in increasing depression literacy and attitudes toward seeking mental health help and decreasing self-stigma to seek help, but may not necessarily change stigma toward others’ mental health condition. The results are in line with the meta-analysis of Schomerus et al, 58 which revealed even though knowledge of mental illness and willingness to seek mental help increased in the past decades, stigma toward persons with mental illness remained stagnant. This may be because most mental illness programs, while they provided ample information on this issue, did little to expose their participants to real contact with mentally ill persons, who are still considered as “the other.” 58 Especially for adolescents, for whom peer acceptance is important during this developmental stage, mental illness is perceived to incur personal and social risks, leading to the stigmatization of the mentally ill adolescent. 59
Our results suggest that the participants’ knowledge of depression is associated with their attitude toward getting help. This is similar to findings from Schmidt et al, 60 Spagnolo et al, 61 and Strunk et al. 62 Information related to the biological and neurological origins of mental illness, especially, may lead the public to be more open to seeking medical help for their condition. 58 This is relevant in Malaysia, where the perception that mental illness and suicidality stem from moral weakness or spiritual forces alone is still rife.27,63
The consistent and measurable impact of this program on depression knowledge and help-seeking attitudes for at least 3 months’ duration after the 1-day program is believed to be influenced by the use of combined approaches in the program delivery. Researchers provided information and understanding to the participants in 3 ways: (1) traditional lecture using slide presentation, and (2) activities and (3) educational video. The group activities that facilitated the participants’ articulation of knowledge and perceptions, as well as the animation video at the end of the program, may have served to consolidate their knowledge and attitudes while providing an engaging learning environment to facilitate positive affect in the learning process, consistent with Kahneman peak-end rule. 53
This study strongly suggests that the Depression Literacy Program may be efficaciously implemented among B40 adolescents in Malaysia. Testing it among adolescents from a lower income background is important because socioeconomic status is a factor affecting mental health literacy and stigma. The lower mental health literacy among those from lower socioeconomic backgrounds may occur partly due to the lack of access to information through education, which is routinely received by the higher classes. 64 The lack of knowledge may also explain why people of low socioeconomic status have a higher likelihood of developing and experiencing mental health problems. 64
This study has limitations. First of all, the participants were divided into control and intervention groups based on their locality. Therefore, we could not rule out the existence of bias. We have also deleted all missing data listwise and have utilized the per-protocol analysis rather than the intention-to-treat (ITT) analysis. In future clinical trials, to ensure the comparability of the control groups, randomization and ITT analysis should be implemented. 65 Apart from that, the group activities held may prime the participants to socially desirable responses when answering the posttest and follow-up questions. However, social desirability and demand characteristics are checked through the use of a control group, which was not exposed to any activities. There needs to be further studies on the efficacy of the Depression Literacy Program, especially with emphasis on the area of the destigmatization of mental illness.
Conclusion
The current study examined the effectiveness of a literacy program on stigma toward depression and help-seeking attitude among the B40 adolescents. The data suggest that upgrading the knowledge on depression will eventually lead to increasing mental help-seeking attitude. However, this positive outcome is limited as the stigma level of the participants toward those with mental illness was similar to those who did not receive the intervention. Despite this limitation, the study provides an important indication on the efficacy of the Depression Literacy Program to improve depression-related knowledge and increase the potential of seeking help among adolescents from the lower socioeconomic background. Considering the program’s potential and feasibility, it is highly suggested to attempt the trial on older and more heterogeneous populations across the country.
Footnotes
Acknowledgements
The authors wish to convey their gratitude to the director, principal, teachers, and wardens of the boarding school involved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was fully supported by the grant National University of Malaysia Dana Cabaran Perdana (DCP-2017-014/3). The funding agency had no role in the study design, data collection, data analysis, manuscript writing, or publication.