
Abstract
Operation cancelations are a serious problem with undesirable consequences. The Health Transformation Plan was launched in the health system of Iran on May 5, 2014, to enhance the efficiency and quality of services in public hospitals. Comprehensive coverage of patients’ basic treatment needs and reduction of patients’ out-of-pocket expenditures through insurance for all are other objectives of Health Transformation Plan as well. Then, the present study aimed to determine the impact of the Health Transformation Plan on the number of surgical operations and the cancelation of elective surgeries within public hospitals of Iran. This retrospective comparative study was conducted in 2017 within 2 tertiary public hospitals in the South-East of Iran. Using systematic random sampling method and census, 8138 scheduled surgical files and all canceled operations files were reviewed from April 2012 to March 2017, respectively. A standard checklist was used for data collection. The data were analyzed using χ2 test and a logistic regression model in SPSS, version 21. The study population was 8138 patients with mean age of 33 ± 19 years. Female patients comprised about 51% of the study population (n = 4115), and nearly two-third of them were married (n = 5192 [63.79%]). Coverage by Iranian health insurance was reported in more than half of patients (n = 4415 [54.79%]). The common reason for surgeries was injury and poisoning (n = 2814 [34.52%]) followed by delivery (n = 1747 [21.46%]). The number of operations increased from 26 677 before Health Transformation Plan (cancelation rate = 1.5%) to 33 190 after Health Transformation Plan (cancelation rate = 2.0%). The cancelation rate had a significant relationship with age (odds ratio = 1.009; confidence interval: 1.00-1.01), health insurance status (odds ratio = 2.12; confidence interval: 1.33-3.38), outpatient service referrals (odds ratio = 0.5; confidence interval: 0.43-0.62), inpatient service referrals (odds ratio = 1.5; confidence interval: 1.36-1.77), and surgical types (P < .05). In general, the Health Transformation Plan was markedly associated with a rise in the number of surgeries and cancelation rate in the public hospitals. The information obtained in the present study concerning the causes of operation cancelations can be used to decrease the number of future cancelations.
Keywords
Access to health services in developing countries is limited because of cost of these services and sometimes quality of these services are less than of standards.
The Health Transformation Plan was launched in the health system of Iran on May 5, 2014, to enhance the efficiency and quality of services in public hospitals.
As the Health Transformation Plan increases patient’s access to higher quality services, it is recommended to implement Health Transformation Plan in other countries that have similar settings as Iran.
Introduction
Surgical operations constitute an indispensable part of health care and an integral component of any country’s national health system at all levels of development. 1 Operation cancelations and their undesirable consequences result in serious problems for health services around the globe in that they are a source of emotional trauma and inconvenience not only for patients and their families but also for medical teams.2,3 Indeed, the cancelation of scheduled surgical operations leads to wastage of resources, false increase in hospital bed occupation, and pointless equipment preparation; reduce physician/patient satisfaction; diminish medical teams’ morale; and cause stress to patients and their companions. 4 Such cancelations are culpable for the inefficient usage of operating rooms, wastage of resources,5-7 creation of logistic and financial burden associated with extended hospital stays and repetitions of preoperative preparations, and loss of time and income.8-12 What can also be compromised is not only the overall perception of the quality of care 13 but also the clinical outcome. As a case in point, Bottle and Aylin 14 found that delayed surgery was associated with an increased risk of in-hospital death, and Devon 15 reported that surgical delay in hip-fracture care contributed to increased morbidity and mortality. Likewise, some studies have shown that the rate of surgical cancelation is one of the most important quality indicators threatening hospital efficiency.3,16,17 Operation cancelations are a worldwide problem, with reported rates ranging from 1.96% to 24%. 18 An approximate rate of 11.7% has been reported in Iran as well. 19 There are numerous reasons for the cancelations of elective surgical cases, and the reasons vary from one hospital to another. 20
The reasons varied from inadequate preoperative assessment and preparation to patient-related factors, surgeon-related issues, lack of operating-room time, unavailability of hospital beds, and emergency surgery disrupting the elective list.21-23 Many of the factors that result in the cancelation of operations can be detected in time to avoid gaps in the surgical schedule and inconvenience to patients. 24
Safe affordable surgical care is beyond the reach of a considerable number of individuals across the world, and every year a great number of patients face catastrophic health expenditures—primarily for surgery. 1 Iran is not an exception to this global concern. With the objective of tackling this serious issue, the Iranian Ministry of Health and Medical Education in 2014 launched a series of stepwise reforms under the umbrella term “Health Transformation Plan (HTP).” The HTP encompasses various interventions aimed at increasing the coverage of basic health insurance, improving the quality of care and the referral system in hospitals affiliated to the ministry, providing incentives for physicians (eg, updating tariffs to more realistic values) to work in public hospitals, and reducing patients’ out-of-pocket expenditures for inpatient services.25-27
A study in Iran showed that 11.7% of the elective operations were canceled in a general hospital before the HTP. 19 Elsewhere in another general hospital in Iran, the cost of operation cancelations was remarkably high, while more than half of the cost (62.1%) of these cancelations was due to avoidable reasons. 13
Given the importance of operation cancelations in each country’s health system, the present study aimed to determine the impact of HTP on the number of surgical operations and the rate of their cancelation in public hospitals in the southeast of Iran. The findings can be helpful for Iranian health policymakers and hospital managers in their efforts to rationalize the country’s health system.
Methods
Study Design
This was a retrospective comparative study of scheduled surgeries trend, elective surgery cancelation rates, and their causes over a 4-year period before and after the implementation of HTP in Iran (2012-2017). It was conducted in 2 tertiary general public hospitals (hospital no. 1 with 532 beds and hospital no. 2 with 270 beds) in Sistan and Baluchestan—the largest deprived province of Iran. 28 The study population included all patients scheduled for elective surgery in the 2 aforementioned hospitals between April 2012 and March 2014 (before the implementation of HTP) and between April 2015 and March 2017 (after the implementation of HTP), and it was 59 867 cases (26 677 operations were scheduled before the implementation of the HTP and 33 190 afterward; 24.4% increase). Given the high volume of surgeries, about 13.5% of scheduled surgeries were selected as study sample. Furthermore, all cancelation surgeries (1088 cases from 59 867) were evaluated in the study. In total, 8138 medical records related to surgical operations were studied (4003 cases before implementation of HTP and 4135 cases after the implementation of HTP).
Systematic random sampling and census methods were used for selecting records among performed and canceled surgical operations, respectively. In systematic random sampling method, the researchers first randomly picked the first medical record from the population. Then, the researchers selected each medical record systematically from the list.
Inclusion Criteria
Inclusion criteria were having surgical operation between 2012 and 2017 in the 2 hospitals and completeness of medical record. Besides, files of the canceled elective surgeries were included in the current study if they were complete and contained surgical codes as well as reasons for the cancelation. Exclusion criteria were files with inadequate medical records.
Outcomes, Data Collection, and Instruments
A standard checklist introduced in a previous study was used. 19 The list comprised demographic variables such as age, sex, place of residence, marital status, and medical variables such as types of health insurance, inpatient and outpatient service referrals, surgical types, and reasons for cancelations.
The profiles of all recorded elective surgeries and all those canceled in the 2 hospitals in the 4-year period were reviewed. Thereafter, using the systematic sampling method, data on 8138 samples were gathered through the Hospital Information System (HIS) based on the patients’ registration code in the 2 hospitals. Subsequently, the reasons for operation cancelations were extracted from the medical files of the patients with canceled elective surgeries and were divided into 7 categories of issues relating to the surgeons, patients, other personnel in the operating team, organization, equipment, anesthesia, and medical treatment. Classification was done in accordance to the International Classification of Diseases (ICD)-9 and ICD-10 coding books.
Statistical Analysis
The data were entered into SPSS, version 21, and analyzed. Frequency tables (number and percentages) and figures were used to describe data. The association between single variables and canceled operations was examined by χ2 test. Multivariate analysis was done using logistic regression model. The study protocol was approved by the Ethics Committee of ZAUMS (ethics code: IR.ZAUMS.REC.1395.293), and ethical issues—particularly vis-à-vis patient anonymity—were fully considered.
Results
The demographic variables of the study population are shown in Table 1. The sample size was a total of 8138 patients, with the mean age of 33 ± 19 years, scheduled for elective surgery. Approximately, half of the cases were women (n = 4115 [51%]); closely tow-third was married (n = 5192 [63.79%]), and most of the individuals lived in Zahedan—the capital city of the Iranian province of Sistan and Baluchestan (n = 5987 [73.56%]). In addition, more than half of the patients had Iranian health insurance (n = 4415 [54.79%]).
The Demographic Variables of the Patients in Operation Services in the Public Hospitals in Iran.
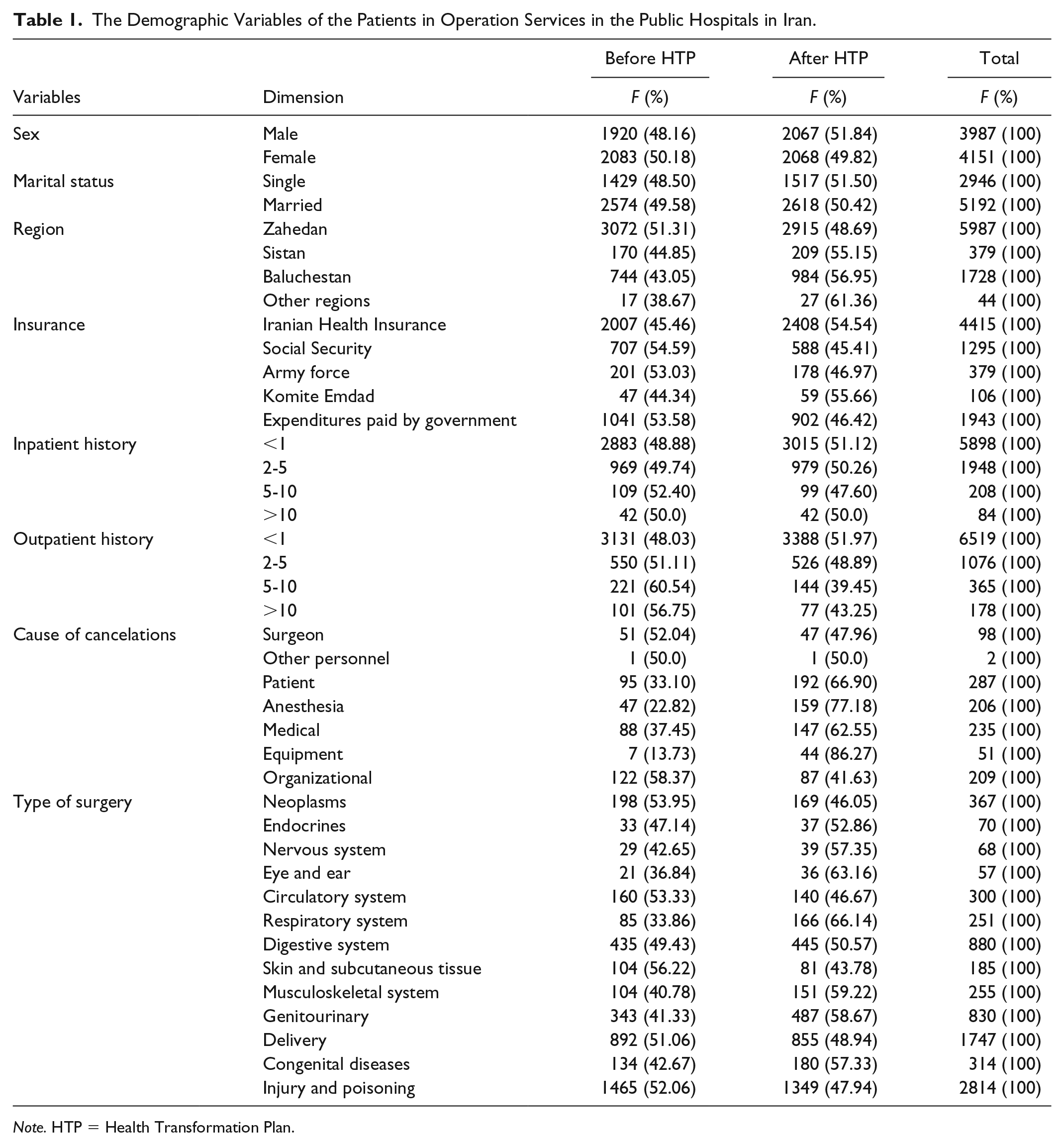
Note. HTP = Health Transformation Plan.
As is shown in Table 1, injury and poisoning (n = 2814 [34.52%]) followed by delivery (n = 1747 [21.46%]) were main reasons for recorded elective surgeries in the 2 public hospitals. In addition, most of the patients (5898 [72.47%]) used inpatient services for less than once. Organization-related factors (n = 122 [58.37%]) and patient-related factors (n = 192 [66.89%]) constituted the principal reasons for the cancelation of the elective surgeries before and after the launch of HTP, respectively.
A total of 26 677 operations were scheduled before the implementation of HTP and 33 190 afterward (24.4% increase). According to the findings, 411 operation were canceled before HTP (cancelation rate = 1.5%) and 677 operations after HTP (operation rate = 2.0%) (Figure 1).

The frequency of operations and the number of cancelations before and after the HTP in the hospitals in Iran.
Table 2 demonstrates the number of the surgeries performed and the percentages of operations canceled based on the study population’s demographic and medical variables.
Frequency of Operations and the Percent of Cancelation Based on the Demographic and Medical Variables in the Public Hospitals in Iran.

As is demonstrated in Table 2, the probability of operation cancelations had a significant statistical association with sex, marital status, surgical types (P = .001), and health insurance types (P = .003). The findings revealed that being male, single, and covered by Emdad committee (covers low-income individuals through a variety of services—particularly in same manner as the Green Card in Turkey) increased the likelihood of operation cancelations in the public hospitals. Furthermore, according to Table 2, the probability of cancelation was higher among the patients in respiratory (28.3), musculoskeletal (23.9), and injury and poisoning (22.8) surgery services (P < .05).
Table 3 illustrates the relationship between the study population’s age and inpatient and outpatient service referrals on one hand and the probability of operation cancelations on the other hand.
Relationship Between Demographic Variables and Probability of Operations Cancelation in the Public Hospitals in Iran.
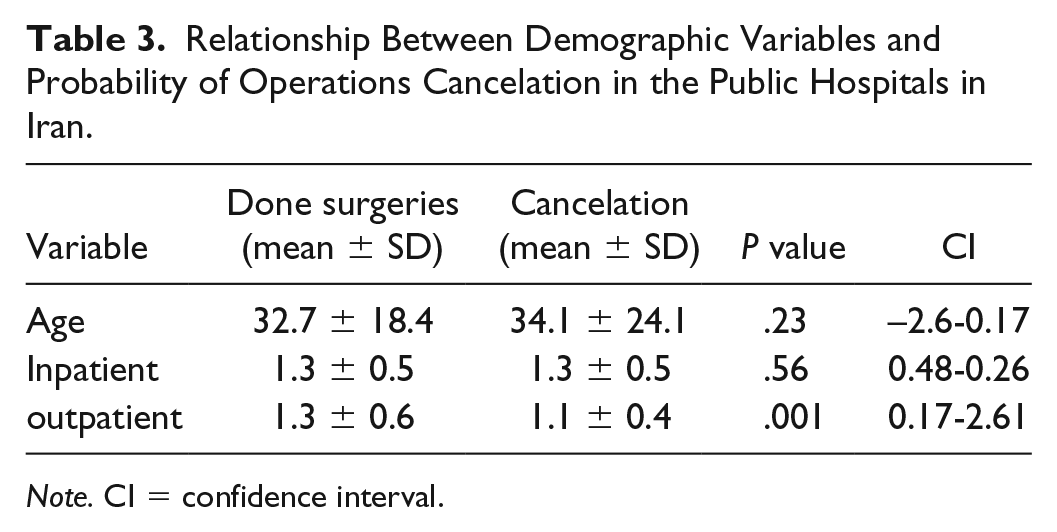
Note. CI = confidence interval.
As is depicted in Table 3, the mean age of the patients who had canceled their operations was higher than that of the patients who had undergone surgery. Outpatient service referrals were associated with a higher likelihood of operation cancelations (P = .001), whereas inpatient service referrals had no relationship with the cancelation of the elective surgeries (P > .05). The effects of the study variables on the probability of operation cancelations were determined via a multivariate analysis, whereby all the variables were entered into a logistic regression in a backward model. The results of the multivariate analysis are presented in Table 4.
The Relationship of Study Variables and Operations Cancelation Probability in the Public Hospitals.

Note. OR = odds ratio; CI = confidence interval.
Base group: neoplasms.
As is shown in Table 4, age was associated with operation cancelations so that the probability of cancelations rose in line with the increase in the patients’ age. Outpatient service referrals reduced the probability of cancelations by 50% (odds ratio [OR] = 0.5; confidence interval [CI]: 0.43-0.62). Comparably, the inpatient cases were 50% more likely to cancel their operation than others (OR = 1.5; CI: 1.36-1.77). According to Table 4, the probability of elective surgery cancelation in patients in trauma services who were exempted from treatment costs, according to the law of accidents in Iran, were more than those who had health insurance (OR = 2.12; CI: 1.33-3.38).
Limitations
The present study did not include the costs sustained by the hospitals and the patients in consequence of the cancelations. In addition, this study was done in only 2 hospitals affiliated with ZAUMS; further investigations in other hospitals across Iran are required to provide a good picture on this issue.
Discussion
The present study was designed to assess the impact of HTP on the number of surgical operations and their cancelation rate in the 2 public hospitals in Iran. The findings showed that after the HTP, the number of operations rose in the hospitals. One possible reason for this increase is the reduction of treatment costs by the HTP plan, whereby patients pay between 3% and 6% of all hospital expenditures, whereas before the introduction of this plan, they paid about 30% of the costs. Additionally, the implementation of HTP has conferred considerable improvement in the quality of services supplied by public hospitals, encouraging patients to benefit from such good-quality low-cost services. In line with our findings, Bastani et al 19 reported a rise in the rate of surgical operations following the launch of Iran’s HTP. It, therefore, appears that the HTP has attained one of its goals by extending community access to hospital services. Given the positive impact of this program, continuation of the program is suggested.
Operation cancelations are very costly and their rate is recommended to be kept below 5%. 29 Study findings demonstrated that operation cancelation rate was 1.5% and 2.0% before and after the HTP in the studied hospitals, respectively. This increase may be due to increase in the number of surgeries in the last years in public hospitals of Iran. However, other factors maybe effect on cancelation rate including patients’ failure to follow presurgical procedures that should be examined in hospitals. Kaddoum et al 5 reported a 4.4% rate of operation cancelations in a tertiary-care teaching hospital in Beirut, Lebanon, in 2016, and Olson and Dhakal 24 reported a rate of 1.2% in an academic tertiary-care hospital in North Carolina in 2015. The use of effective plans may decrease the cancelation rate in hospitals. Lee et al 30 found that after the implementation of a nurse-patient preoperative call log whereby nurses called patients or their guardians on 2 separate occasions during a 2-week period before surgery to review their health history, give them instructions, and answer their queries about the upcoming surgery, the rate of cancelation was decreased from 16.8% to 8.8%. For decreasing cancelation rate, Six Sigma could be used, the latest quality management system, which holds that an improvement in quality boosts speed and diminishes cost—a systematic organizational approach that relies on eliminating defects and errors by solving problems and promoting projects. 4 Gheysari et al 4 reported that the use of Six Sigma lessened the cancelation rate among their study population from 3.6% to 1.4%. Turunen et al 31 conducted an evidence-based structured preoperative protocol project that incorporated a multiprofessional team of nurses, physicians, secretaries, and hospital management staff in a single university hospital in Finland and reported that promoting scheduled arrivals of surgical patients to the hospital, achieved primarily through preoperative phone calls by the nurses to the patients, succeeded in lowering the rate of operation cancelations. Cancelations have very serious negative consequences and huge financial implications for both patients and hospitals. This is especially important in developing countries such as Iran, which face severe budgetary constraints.
According to our findings, injury and poisoning as well as delivery were the most frequent surgical operations in the 2 study hospitals; however, respiratory (28.3%), musculoskeletal (23.9%), and injury and poisoning surgeries (22.8) accounted for the most frequently canceled operations. In line with this finding, Dhafar et al 32 reported that the highest rate of cancelation was among scheduled orthopedic surgeries (33.8%). Olson and Dhakal 24 reported that general-surgery cases accounted for most of the cancelations among their study population. In addition, a study in Iran showed that the highest rate of cancelation was related to orthopedic surgeries. 4 Bastani et al 19 stated that infant surgery was the most frequent operating-room service after the launch of the HTP, with orthopedic surgeries having the fewest cancelations.
The present study suggests that after the implementation of HTP, the most common reason for the cancelation of the elective surgeries was patient-related causes, including not being NPO (nothing through the mouth). In this regard, Dhafar et al 32 demonstrated that 42.81% of all the operation cancelations in their study were patient-related and 20.03% were facility-related. Likewise, Fitzsimons et al 33 showed that the most common cause of operation cancelations (44%) among their study population was a change in the patients’ health status. Appavu et al 34 found that patient no-shows were the most prevalent reason (63%) for surgical cancelations in their study sample. According to a study by Bhuiyan et al, 35 the most common reason for the cancelation of surgeries was the need for emergency surgery (64.4%), causing the cancelation of the scheduled operations. Elsewhere, Kaddoum et al 5 reported that a lack of financial clearance and incomplete medical evaluation were the causes of operation cancelations in their study. Olson and Dhakal 24 found that the most common cause for the cancelation of surgical operations among their study patients was a new medical condition. In total, hospitals should pay sufficient heed to the abovementioned causes of operation cancelations. To that end, it is vitally important that patient education programs such as patient training on arrival at the hospital and patient training before surgery being undertaken in the hospitals.
Outpatient service referrals decreased the cancelation rate among the patients in our study. Patients’ referral to clinics and benefiting from hospital services, especially physician visits, may decrease the probability of cancelations. In this regard, Fitzsimons et al 33 and Kaddoum et al 5 described that the highest rate of cancelation in their study was among the inpatients (65% and 66%, respectively). Their results are concordant with those given by Xue et al, 36 who found the lowest cancelation rate among their outpatients (about 4.5%).
The univariate analysis revealed that the rate of operation cancelations was high among the patients who lived in the Baluchestan region. Baluchestan is an economically depressed area in Iran, and most of its residents, who are geographically dispersed over a vast expanse, are deprived from proper access to health services. The fact that most of the Baluch have no choice apart from traveling long distances (between 200 and 700 km) to arrive capital city of Zahedan to access high-quality health services might be a good reason for the cancelation of operations in our study.
Conclusions
The HTP was markedly associated with a rise in the number of surgical operations performed in the public hospitals; however, it increased the rate of cancelation. Important factors affecting the surgeries’ cancelation (such as patients’ age, hospital admission type, kind of health insurance, and type of surgeries) should be considered further in the treatment process for controlling and decreasing cancelation rate.
Implications
Reforms similar to the HTP in developing countries are needed for decreasing out-of-pocket expenditures and increasing quality of services and community access to hospital services, especially operation procedures. Based on the study, policy makers and health mangers should pay attention to HTP and identify cause of operation cancelations in their setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was extracted from a project supported by Zahedan University of Medical Sciences (grant no. 8074).