
Abstract
The objective of this study was to examine positive predictive value (PPV) of medication therapy management (MTM) eligibility criteria under Medicare Modernization Act (MMA) and Affordable Care Act (ACA) in identifying patients with medication utilization issues across racial and ethnic groups. The study analyzed Medicare data (2012-2013) for 2 213 594 beneficiaries. Medication utilization issues were determined based on medication utilization measures mostly developed by Pharmacy Quality Alliance. MMA was associated with higher PPV than ACA in identifying individuals with medication utilization issues among non-Hispanic blacks (blacks) and Hispanics than non-Hispanic whites (whites). For example, odds ratio for having medication utilization issues to whites when examining MMA in 2013 and ACA were 1.09 (95% confidence interval [CI] = 1.04-1.15) among blacks, and 1.17 (95% CI = 1.10-1.24) among Hispanics, in the main analysis. Therefore, MMA was associated with 9% and 17% higher PPV than ACA in identifying patients with medication utilization issues among blacks and Hispanics, respectively, than whites.
Keywords
Minorities are less likely to obtain preventive and specialty services such as medication therapy management (MTM) and are more likely to have higher health care costs due to worse health outcomes partly caused by medication utilization issues.
This study compared the positive predictive value (PPV), or efficiency of MTM eligibility criteria, under Medicare Modernization Act (MMA) and Affordable Care Act (ACA) in identifying individuals with medication utilization issues across racial and ethnic groups, and found that MMA eligibility criteria were more efficient than ACA among non-Hispanic blacks and Hispanics than non-Hispanic whites.
Given the critical role played by MTM in improving health outcomes among older patients with chronic diseases, the findings of the current study provide evidence that may assist policy makers in improving efficiency of Medicare Part D MTM eligibility criteria and reducing disparities associated with MTM services.
Introduction
Eliminating racial and ethnic disparities has been a top national agenda item exemplified by Federal efforts such as Healthy People 2010 and 2020.1,2 Research consistently demonstrate that, compared with non-Hispanic whites (whites), non-Hispanic blacks (blacks) and Hispanics are more likely to lack comprehensive health insurance coverage, encounter discrimination by professionals in clinical settings, and have problems accessing high-quality health care. 3 As a result of this and other factors, minorities are less likely to obtain preventive and specialty services or experience improved health outcomes.4,5 They are also more likely to have higher health care costs due to worse health outcomes caused by medication utilization issues.6,7
Racial and ethnic disparities in medication therapy management (MTM) eligibility criteria provide an example of institutionalized disparities in health care access.8-18 According to the Medicare Prescription Drug and Modernization Act (MMA) of 2003, Medicare prescription drug (Part D) plans are required to offer MTM to patients with multiple chronic conditions, using multiple Part D drugs, and likely to incur annual costs for covered Part D drugs that exceed a prespecified threshold. 19 Minorities could particularly benefit from MTM services because they are more likely than whites to have certain chronic conditions (eg, diabetes, hypertension) targeted by MTM programs and undergo medical procedures that are indicators of poor management of these conditions.6,7 MTM services are perfectly positioned to reduce these health outcome disparities, as the purpose of MTM is to ensure optimal therapeutic outcomes from covered Part D medications prescribed to targeted beneficiaries. 19
Despite the importance of MTM for racial and ethnic minorities, a series of studies found that minorities are less likely to be eligible for MTM services than whites.8-18 Such findings are not surprising because MTM eligibility criteria are predominantly utilization-based, and racial and ethnic minorities typically use fewer prescription medications and incur lower prescription drug costs than do whites.20-24 Further aggravating racial and ethnic disparities is the fact that Part D plans have the flexibility to determine their own MTM eligibility thresholds within the legislative framework, and these Part D plans typically set their thresholds using the highest possible minimum. For example, during 2017, slightly more than 84% of Part D plans set their threshold as at least 3 chronic conditions (range, 2-3 conditions), and approximately 66% selected a minimum threshold of at least 8 drugs (range, 2-8 drugs), with the threshold for annual drug cost set at $3919 in 2017 by Centers for Medicare & Medicaid Services (CMS). 25 Besides disparity issues associated with MTM eligibility criteria, low participation in MTM is also a challenge. While CMS has a goal of covering at least 25% of Medicare beneficiaries, currently only approximately 10% of Part D beneficiaries are enrolled in MTM. 26
Although less well-known, the Patient Protection and Affordable Care Act (ACA) also laid out a set of MTM eligibility criteria for organizations to target patients in demonstration programs. 27 ACA suggested that patients with the following characteristics should be targeted: (1) taking at least 4 prescribed medications (including dietary supplements and over-the-counter medications); (2) taking high-risk medications; (3) having at least 2 chronic diseases; OR (4) having experienced a care transition, or other factors, that are likely to cause a high risk of medication utilization issues. 27 Note that these criteria are less restrictive than eligibility criteria under the MMA. Furthermore, MMA requires patients to meet all eligibility criteria while ACA does not. A study by Wang et al found the MTM eligibility rate under ACA MTM eligibility criteria could be over 80% if applied to Part D enrollees. 16 CMS stressed the importance of analyzing the MTM eligibility criteria in ACA because such analysis can solidify the evidence base for improving the Medicare Part D MTM program. 26 The objective of this study was to examine positive predictive value (PPV) of MTM eligibility criteria under MMA and ACA in identifying patients with medication utilization issues across racial and ethnic groups.
New Contribution
PPV is a widely used measure in evaluation of lab tests, which has been increasingly used in policy evaluations. PPV determines the extent of true positives, when patients with a positive lab test truly have the disease of interest. In the context of MTM, an examination of PPV can help to determine the efficiency of MTM eligibility criteria in identifying patients with medication utilization issues. Economic considerations of disparity reduction strategies have gained increased attention in recent years due to limited resources and tightened health care budget.28,29
Methods
Study Design, Population, and Data Sources
This retrospective study analyzed Medicare databases in 2012-2013 of 3 million Medicare beneficiaries linked to the Area Health Resource File (AHRF).30,31 In Medicare databases, Part D Prescription Drug Event (PDE) file, Master Beneficiary Summary File (MBSF), and Medicare Parts A & B claims were used. The AHRF was linked with the Medicare databases to provide characteristics of Medicare beneficiaries’ residence at the county level. Patient inclusion criteria used in this study were (1) 65 years or older at the beginning of 2012 (to increase population homogeneity); (2) alive at the end of 2013; and (3) enrolled in Medicare throughout 2013 with continuous Parts A, B, and D coverage. The study included 3 major racial and ethnic groups: whites, blacks, and Hispanics. Racial and ethnic disparities were examined by comparing whites with blacks and Hispanics, respectively. Data from 2013 were used for most analyses except when 2012 data were used to determine patients’ health insurance status in the year before the study year to define some independent variables.
Conceptual Framework
Andersen’s Behavioral Model for Health Services Utilization was used in this study as a conceptual framework because the study outcomes are predominantly based on the utilization of pharmaceutical products. Both individual and community (county)-level factors were included in the model. 32 Three classes of variables were included: predisposing (factors that predispose patients for health services utilization), enabling (factors that enable health services utilization), and need factors (measures for patient health care needs). Specifically, predisposing factors included age, gender, race and ethnicity (based on Research Triangle Institute race code instead of traditional race code), and the county-level information of percentage of nonwhite population, percentage of married-couple families, per capita income, percentage of population living in poverty, percentage of various educational achievements among 25 years or older, percentage of population eligible for Medicaid, percentage of unemployed population, and percentage of population without health insurance. Enabling factors included metropolitan statistical area, census regions, and whole/part of county as a health professional shortage area (HPSA) for primary care. Need factors included the Deyo-adapted Charlson Comorbidity Index, and a risk adjustment summary score developed by CMS.33,34 Deyo-adapted Charlson Comorbidity Index was used instead of other indices because it has been widely used. 33 The risk adjustment summary score was calculated based on diagnostic information from claims and was developed to risk-adjust payments to Medicare Advantage plans. 34
Dependent Variable
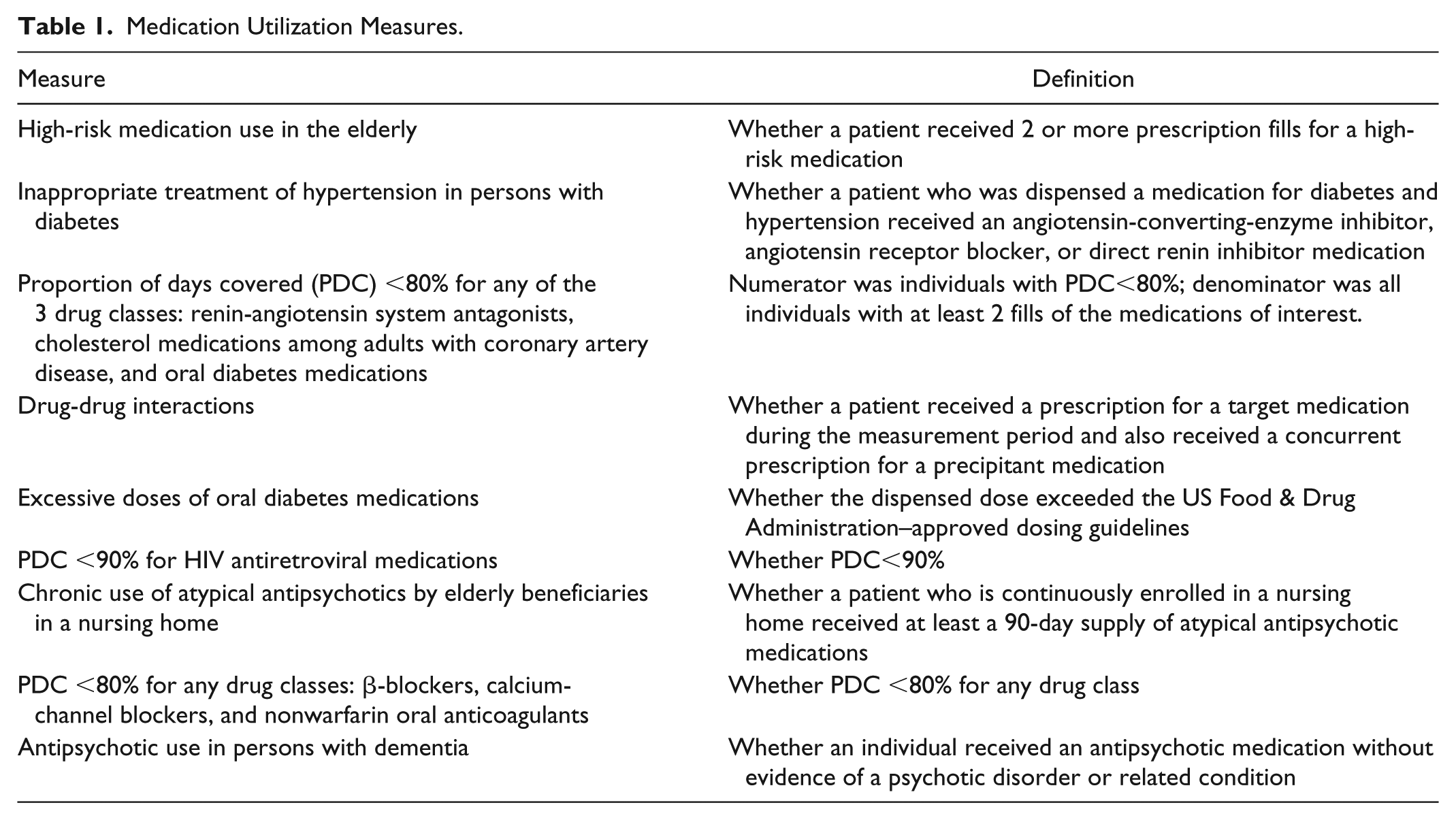
Having medication utilization issues was the dependent variable, which was defined based on the most current medication safety and adherence measures in 2013/2014 at the time of this study developed by the Pharmacy Quality Alliance. 35 Pharmacy Quality Alliance (PQA) is an organization established to develop and maintain quality measures related to medication utilization. 36 Several measures developed by PQA are now used in CMS’s Star Ratings system and are tied to bonus payments to Part D plans. 37 Patients were deemed to have medication utilization issues if they had any issues determined by the following 9 measures (Table 1)35,37: (1) high-risk medication use in the elderly; (2) inappropriate treatment of hypertension in persons with diabetes (this measure has been retired for clinical reasons and is no longer used); (3) proportion of days covered (PDC) <80% for any of the 3 drug classes: renin-angiotensin system antagonists, cholesterol medications among adults with coronary artery disease, and oral diabetes medications; (4) drug-drug interactions; (5) excessive doses of oral diabetes medications; (6) PDC <90% for HIV antiretroviral medications; (7) chronic use of atypical antipsychotics by elderly beneficiaries in a nursing home; (8) PDC <80% for β-blockers, calcium-channel blockers, and nonwarfarin oral anticoagulants; and (9) antipsychotic use in persons with dementia. Note that all measures except 8 and 9 were Star Ratings measures at the time of this study.35,37
Medication Utilization Measures.
Independent Variables
MMA MTM eligibility criteria
The study examined the 2009, 2013, and proposed 2015 MTM eligibility criteria.26,38,39 The year 2010 is an important time point because CMS significantly lowered the eligibility thresholds that Part D plans were allowed to use with a purpose to reduce variability in MTM eligibility and increase MTM participation in 2010. 26 The MTM eligibility thresholds in 2009 represent the most recent MTM eligibility thresholds before 2010. The 2013 thresholds represent the most current thresholds employed by CMS at the time of this study. CMS proposed even lower MTM eligibility thresholds for 2015 to further increase MTM participation but these were not implemented due to stakeholders’ concerns over other proposed Part D reforms along with the MTM provision. Employing 3 sets of thresholds in the analysis allowed comprehensive assessment of MMA eligibility thresholds.
The wide range of eligibility thresholds for the numbers of Part D drugs and chronic conditions were accounted for by considering the minimum, median, mode, and maximum of these thresholds. For example, the MTM eligibility thresholds used by Part D plans in 2009 exhibited the following pattern: number of chronic conditions ranged from 2 to 5 (both median and mode = 3), number of Part D drugs ranged from 2 to 15 (median = 6, mode = 8), and drug cost threshold was $4000. 38 Therefore, 4 × 3 × 1 = 12 different combinations of representative thresholds were examined, where 4, 3, and 1 are the number of unique representative thresholds for each eligibility criterion. The main analysis examined the modal values: 3 chronic conditions, 8 covered medications, and $4000 drug costs. The other 11 combinations of eligibility thresholds were examined in sensitivity analyses. There was only one combination of 2015 eligibility criteria: 2 chronic conditions (at least one is a core chronic disease, including cardiovascular disease, diabetes, dyslipidemia, respiratory disease, bone disease—arthritis, mental health, Alzheimer disease, and end-stage renal disease), 2 Part D-covered drugs, and $620 in annual drug costs. 26
The drug cost thresholds were adjusted to dollars in study years based on the consumer price index for medical care. 40 Number of Part D drugs and Part D drug costs were calculated using PDE file. To determine number of chronic conditions, a list of chronic conditions applicable to the Medicare population assembled by Daniel and Malone was applied. 41 These conditions include all chronic conditions targeted by MTM programs as required by CMS. 26 Chronic conditions for each participant were identified using a free Clinical Classification Software developed by the Agency for Healthcare Research & Quality, which aggregates medical conditions and illnesses into 285 mutually exclusive categories. 42
ACA MTM eligibility criteria
Under ACA, the criteria of taking at least 4 prescribed medications and having at least 2 chronic diseases are based on the same aspects of patient characteristics as the criteria under MMA. 27 Therefore, patient eligibility was determined using methods similar to the MTM eligibility thresholds under MMA. Over-the-counter medications and dietary supplements were considered only when they were included in the PDE file. The last eligibility criterion is based on a transition of care or “other factors.” Because “other factors” were not explicitly defined in the regulatory document, the study focused on “transition of care,” which was defined as patient transition from one health care setting to another, including home. “Transition of care” was determined based on patients’ health services records. For a community-dwelling individual, any record of a hospitalization or admission to other facilities, including nursing homes, was considered a transition of care.16,43 Individuals were considered facility-dwelling if they had claims for nursing homes, assisted living and related facilities, long-term hospitals, mental health centers, and various other long-term care settings. For individuals dwelling in facilities, any record of services in another health care setting excluding physician visits and outpatient visits was considered a transition of care. 44 To provide a comprehensive policy recommendation, 15 combinations were analyzed each representing a unique combination of the eligibility criteria in ACA. One main analysis (combination of all 4 eligibility criteria) and 14 sensitivity analyses were conducted.
Statistical Analysis
The study included descriptive, multivariate, and disease-specific analyses. For the descriptive analysis, the proportions of having medication utilization issues for each racial and ethnic group under MMA or ACA MTM eligibility were compared using chi-square test. For multivariate analysis, a logistic regression was conducted to compare the likelihood of having medication utilization issues between the following 4 eligibility categories:
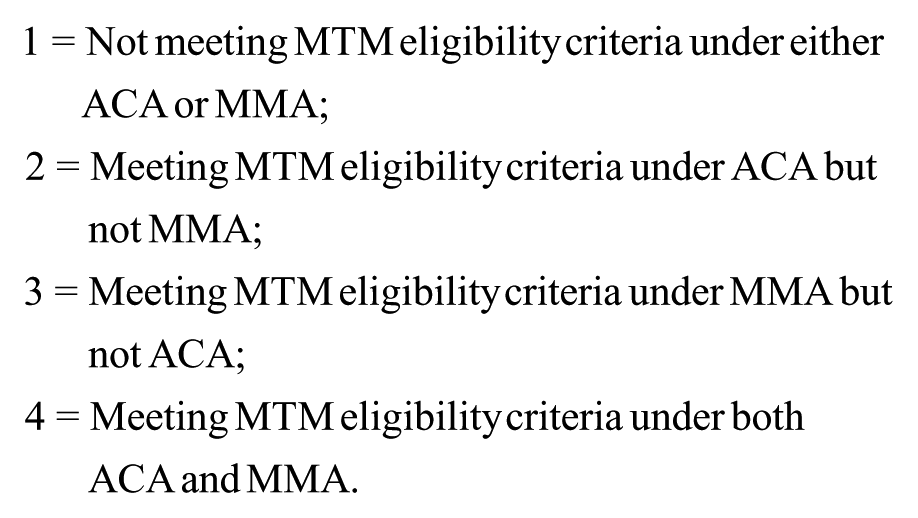
Category 2 was used as reference group and dummy variables for other categories were included as independent variables. Dummy variables were also included for blacks and Hispanics with whites as the reference group. When interpreting study results, odds ratios (ORs) greater than 1 for the interaction term between the dummy variables for category 3 and blacks, for example, would indicate higher comparative PPV for MMA than ACA among blacks than whites. Since nobody was found in category 3 in this study, ORs greater than 1 for the interaction term between the dummy variables for category 4 and blacks would indicate greater comparative PPV for MMA than ACA among blacks than whites. The analysis strategy of need-based and demand-based analyses was applied in the study. 45 When conducting need-based analysis, the variables affecting individuals’ need for health care, such as age, gender, and ethnicity, Deyo-adapted Charlson Comorbidity Index, and risk adjustment summary score, were included. When conducting demand-based analysis, variables that might affect health care demands (ie, all covariates in the Andersen’s Model) were included.
Due to the importance of MTM services for chronic disease management, disease-specific analyses for each of the top 10 MTM-targeted chronic conditions were conducted to produce policy recommendations applicable to patients with specific conditions. 26 Data analysis was conducted using SAS 9.4 (SAS Institute Inc, Cary, North Carolina) and STATA 13.1 (STATA Corporation, College Station, Texas). This study was deemed exempt by the Institutional Review Board at the corresponding author’s institution (approval number: 13-02788-XM).
Results
A total of 2 213 594 Medicare beneficiaries were included. Within the study sample, 2 052 997 (92.74%) were white, 96 941 (4.38%) were black, and 63 656 (2.88%) were Hispanic. The differences between whites and minorities were significant for all characteristics (Table 2; P < .05): minorities were younger than were whites. Compared with whites, counties where minorities lived had higher percentages of nonwhite population, individuals in poverty, individuals eligible for Medicaid, unemployed, and individuals without health insurance. Minorities were more likely to live in the metropolitan statistical area, and to live in an area where either whole or part of the county was an HPSA for primary care. Counties where minorities lived also had lower percentages of married-couple families, lower per capita income, and lower percentage of having high school and higher degrees. Minorities and whites also had different geographic distributions across census regions. Minorities were more likely to have higher Deyo-adapted Charlson Comorbidity Index than whites.
Sociodemographic and County-Level Characteristics Across Racial and Ethnic Groups Among the Study Population.

Note. P < .05 for the difference between non-Hispanic whites and minorities for all variables. SD=standard deviation.
According to descriptive analysis for both MMA and ACA, proportions of having medication utilization issues were higher among blacks and Hispanics than whites (P<0.05 for the difference between whites and minorities for all comparisons). For example, for 2013 MMA, proportions of having medication utilization issues were 79.10% to 84.97% (main analysis: 84.97%) for blacks, 76.78% to 80.37% (main analysis: 80.37%) for Hispanics, and 68.20% to 72.70% (main analysis: 72.70%) for whites (Table 3). Findings for comparative PPV were mixed. For example, comparative PPV was higher among MMA than ACA among Hispanics but not blacks compared with whites according to the main analysis of 2013 MMA and ACA (Table 3). Proportions of patients having medication utilization issues under 2013 MMA were 19.27 percentage points, 22.67 percentage points, and 21.34 percentage points, respectively, higher than ACA among blacks, Hispanics, and whites. The comparative PPV therefore for MMA was 2.07 percentage points lower for blacks than whites, and 1.33 percentage points higher for Hispanics versus whites (P < .05).
Proportions of Individuals With Medication Utilization Issues Across Racial and Ethnic Groups.

Note. P< .05 for the difference between non-Hispanic whites and minorities for all comparisons.MTM = medication therapy management.
In the multivariate analysis, evidence was found for higher comparative PPV among MMA and ACA among minorities than whites. Interaction terms for category 4 and blacks were not always significant, but the interaction terms for category 4 and Hispanics were always significant but the point estimates were all greater than 1 (Table 4). For example, in the demand-based model in main analysis for 2013 MMA and ACA, the OR for the interaction terms for category 4 and blacks was 1.09 (95% confidence interval [CI]: 1.04-1.15), and the OR for the interaction term between category 4 and Hispanics was 1.17 (95% CI: 1.10-1.24) in the main analysis of 2013 MMA and ACA. These numbers indicate that comparative PPV for 2013 MMA versus ACA were 9% higher among blacks and 17% higher among Hispanics than whites. However, in need-based and demand-based models, the ORs for the interaction term between category 4 and blacks were 1.03 (not significant with 95% CI = 0.97-1.10), and 1.04 (not significant with 95% CI = 0.98-1.11), in the main analysis of 2009 MMA and ACA.
Comparative Positive Predictive Value of MMA and ACA MTM in Identifying Individuals With Medication Utilization Issues across Racial and Ethnic Groups Based on Logistic Regressions.
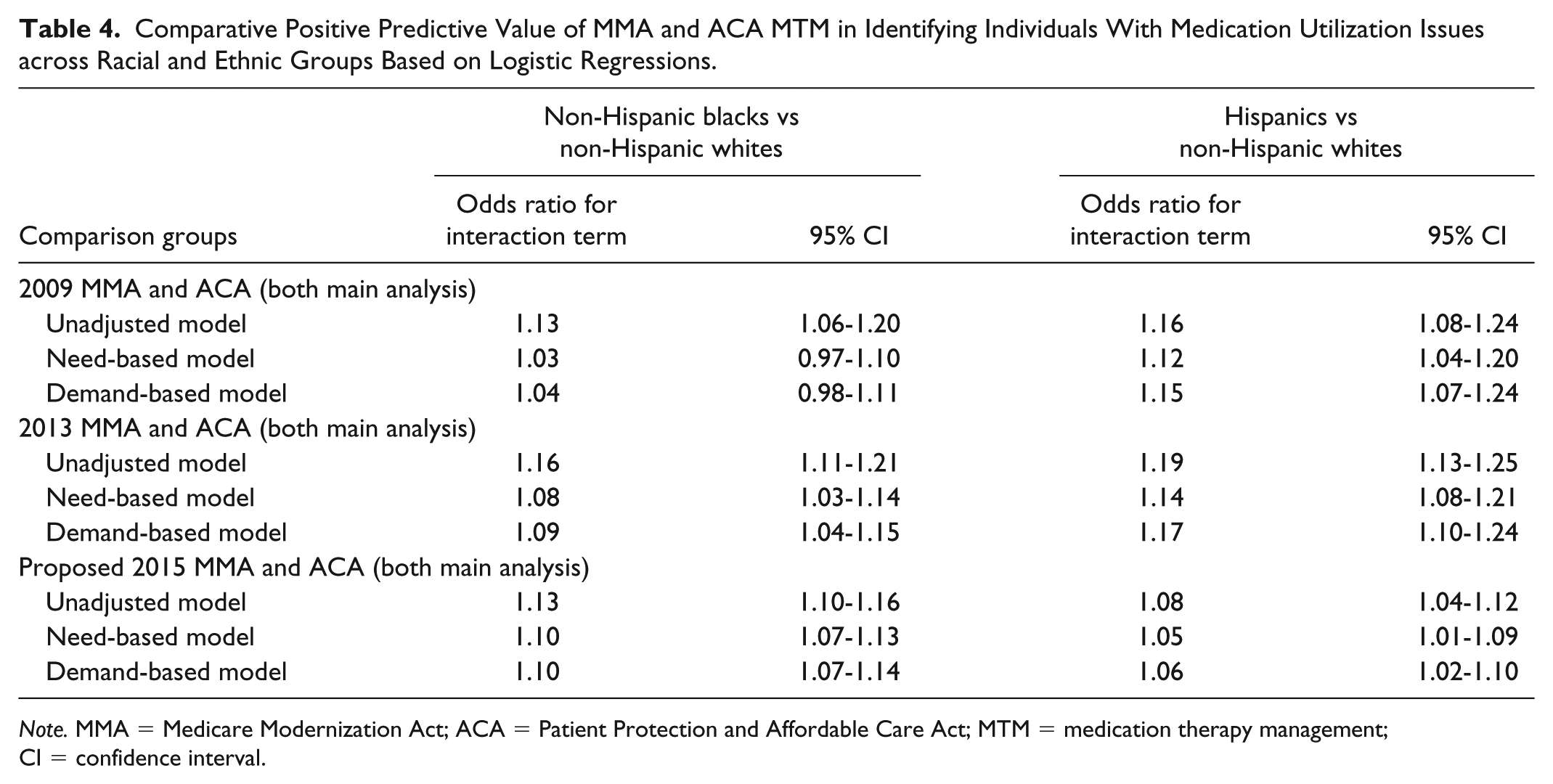
Note. MMA = Medicare Modernization Act; ACA = Patient Protection and Affordable Care Act; MTM = medication therapy management; CI = confidence interval.
Disease-specific analysis also had similar findings on comparative efficiency of MMA versus ACA across racial and ethnic groups (Table 5). For instance, in demand-based analysis of 2013 MMA and ACA MTM eligibility criteria, the significant ORs for the interaction terms for category 4 and blacks were for cardiac disease (OR = 1.18, 95% CI = 1.12-1.25), dyslipidemia (OR = 1.08, 95% CI = 1.03-1.15), hypertension (OR = 1.16, 95% CI = 1.11-1.22), chronic obstructive pulmonary disease (COPD; OR = 1.23, 95% CI = 1.12-1.35), osteoporosis (OR = 1.11, 95% CI = 1.04-1.18), rheumatoid arthritis (OR = 1.20, 95% CI = 1.01-1.44), and renal disease (OR = 1.21, 95% CI = 1.10-1.32). These numbers indicate that, among patients with these 7 diseases, the criteria under 2013 MMA were 8% to 21% more efficient than the criteria under ACA in identifying medication utilization issues among blacks than whites. The significant ORs for category 4 and Hispanics versus whites in demand-based analysis of 2013 MMA and ACA MTM eligibility criteria were for diabetes (OR = 1.10, 95% CI = 1.01-1.19), cardiac disease (OR = 1.22, 95% CI = 1.14-1.31), dyslipidemia (OR = 1.14, 95% CI = 1.06-1.21), hypertension (OR = 1.17, 95% CI = 1.10-1.25), COPD (OR = 1.27, 95% CI = 1.13-1.43), osteoporosis (OR = 1.19, 95% CI = 1.10-1.28), asthma (OR = 1.17, 95% CI = 1.01-1.35), depression (OR = 1.14, 95% CI = 1.04-1.25), and renal disease (OR = 1.20, 95% CI = 1.05-1.37). These numbers indicate that, among the patients with these 9 diseases, the MMA criteria were 10% to 27% more efficient than ACA in identifying medication utilization issues when comparing Hispanics with whites.
Comparative Positive Predictive Value of MMA and ACA in Identifying Individuals With Medication Utilization Issues across Racial and Ethnic Groups According to Demand-Based Logistic Regressions.

Note. MMA = Medicare Modernization Act; ACA = Patient Protection and Affordable Care Act; CI = confidence interval.
2015 MMA was proposed but not implemented.
Discussion
The purpose of the current study was to examine the comparative PPV of the MTM eligibility criteria under ACA and MMA in identifying patients with medication utilization issues across racial and ethnic groups. Using a national Medicare beneficiary sample, this study analyzed 17 MMA and 15 ACA MTM eligibility threshold combinations and 9 medication safety and adherence measures related to CMS’s Star Ratings system. In general, MMA MTM eligibility criteria were more efficient than ACA in identifying beneficiaries with medication utilization issues for blacks and Hispanics compared with whites. Efficiency is an important aspect of policy evaluation due to tightening budget constraint in health care. As Lee et al also suggested, even a 1% increase in PPV could potentially translate to considerable cost savings for Part D plans due to the large size of the Medicare Part D population. 46
This study documented higher medication utilization issues among minorities than whites among individuals eligible for MTM under MMA and ACA. Such patterns can be expected because higher medication utilization issues among minorities than whites in general have been documented previously.8,47 However, it is harder to pinpoint the reasons for the differential efficiency of MMA and ACA MTM eligibility criteria in identify patients with medication utilization issues across racial and ethnic groups. This may be because MMA MTM eligibility criteria are predominantly based on prescription drug and health services utilization while minorities use fewer medications and health services; when minorities meet stricter MMA MTM eligibility criteria than ACA, they may have worse health status and may experience even worse medication utilization issues than whites.
Our findings also suggest that implementation of ACA’s MTM eligibility criteria guidance should involve caution. ACA implementation improved population’s health insurance coverage and access to health services. 48 Racial and ethnic disparities in access have also been reduced significantly. 48 However, MTM eligibility criteria under ACA were not as efficient as MMA criteria among minorities as whites in targeting patients having medication utilization issues. Wang et al further reported that racial and ethnic minorities may be less likely than whites to be eligible for ACA MTM services, and ACA MTM eligibility criteria may also aggravate existing racial and ethnic disparities in health status. 16 MTM services are important for Medicare Part D. Previous studies have demonstrated that MTM services result in improved patient outcomes in disease management, patient quality of life, and lower health care costs.49,50 For example, Isetts et al reported that for every $1 spent on MTM, $12 was saved. 49 Importantly, these savings are associated with significant improvements in cholesterol and blood pressure control. Wentzlaff et al noted that patients’ rate of blood pressure control almost doubled when pharmacists helped manage medications. 50
The present study found that in populations with cardiac disease, dyslipidemia, hypertension, COPD, osteoporosis, or renal disease, MTM eligibility criteria under MMA are more efficient than ACA in identifying medication utilization issues among both blacks and Hispanics versus whites according to demand-based main analysis of 2013 MMA criteria and ACA criteria. However, MMA were not more efficient among patients with diabetes, asthma, depression, and rheumatoid arthritis based on the same analysis. These findings indicated that efficiency of MMA versus ACA MTM eligibility criteria in targeting medication utilization issues among racial and ethnic minorities would vary depending on different chronic conditions. This adds another layer of complexity when policy makers compare different MTM eligibility criteria.
Although the study showed that MMA eligibility criteria are more efficient for minorities than those under ACA in identifying patients with medication utilization issues, the shortcomings of existing MMA MTM eligibility criteria should be kept in mind. Besides the disparity implications and low participation issues associated with MMA MTM eligibility criteria, effectiveness of these eligibility criteria was also questioned. For example, Stuart et al reported that current MMA MTM eligibility criteria exclude beneficiaries with problematic medication utilization patterns such as low adherence. 51
Using PPV, this current study only examined efficiency of MTM eligibility criteria under MMA and ACA. Future studies need to examine the comparative effectiveness of MMA and ACA MTM eligibility criteria in general and across racial and ethnic groups in specific. Specifically, we need to compare the effectiveness of MMA and ACA MTM eligibility criteria in identifying individuals with medication utilization issues across racial and ethnic groups. This could be measured by using other statistics for lab tests such as sensitivity. In the case of MTM eligibility criteria, sensitivity is the proportion of individuals with positive test results among those with medication utilization issues. After we compare both efficiency and effectiveness of MMA and ACA MTM eligibility criteria, we can make more comprehensive policy suggestions regarding these 2 sets of MTM eligibility criteria. Future studies should also consider changes in Star Ratings and their possible impact. For example, completion rate for comprehensive medication review as part of MTM services is now a Star Rating measure and may improve Medicare beneficiary access to services such as MTM as pharmacies/providers work to increase patient engagement. 37
Since 2017, the MTM enrollment and utilization data have been made available to the research community, so it is finally plausible to examine the real efficiency and effectiveness of MMA MTM eligibility criteria instead of relying on analysis of policy scenarios. However, the analysis of real efficiency and effectiveness of ACA MTM eligibility criteria is still not possible because these eligibility criteria have not been implemented. Currently, CMS is conducting a 5-year demonstrative Enhanced MTM Program, which gives Part D plans complete flexibility in selecting target population instead of limiting these plans with MMA provisions. 52 While awaiting findings from this demonstration program, researchers still need to explore alternative options for the current Medicare MTM program, to supplement findings from Enhanced MTM for future deliberations of effective MTM reform.
Limitations
This study provides crucial and time-sensitive results in comparative efficiency of MMA and ACA’s MTM eligibility criteria in identifying patients with medication utilization issues across racial and ethnic groups based on policy-scenario analysis. This can assist policy makers by identifying the strengths and weaknesses of policies before they are implemented. The main limitation is that this study was based on analyses of policy scenarios instead of MTM claims data, as MTM participation status under MMA and ACA was not available at the time of this study. Furthermore, the 9 measures related to CMS’s Star Ratings may not include all types of medication utilization issues, nor are they the only ways of measuring medication utilization quality; moreover, the goals of MTM are much broader in scope than just addressing these particular medication utilization issues. The technical specifications for these measures may also have limitations such as excluding patients who fail to fill their first and/or second prescriptions because patients were required to have 2 prescription fills to be included in the calculation of medication adherence. 35 However, these technical specifications, which are constantly evolving, represent the current best science in MTM quality measures at the time of this study. Last, while the Research Triangle Institute race code used for race/ethnicity information represents improvement compared with traditional race code in MBSF, Research Triangle Institute race code still has suboptimal sensitivity and specificity. 30
Conclusion
This study compared the PPV or efficiency of MTM eligibility criteria under MMA and ACA in identifying individuals with medication utilization issues across racial and ethnic groups. MTM eligibility criteria under MMA were more efficient in identifying patients with medication utilization issues than those under ACA among blacks and Hispanics than whites. Considering the critical role played by MTM in improving health outcomes among older patients with chronic diseases, this comparison could provide evidence to assist policy makers in improving efficiency and reducing disparities associated with MTM services. Further studies should also examine effectiveness of MTM eligibility criteria under MMA and ACA in identifying patients with medication utilization issues.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under award number R01AG049696. The content of this study is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.