
Abstract
The psychological well-being of the siblings of hospitalized children is at risk. This study examined the variables related to siblings’ internalizing problems and personal growth during hospitalization from the perspectives of mothers and other main caregivers who temporarily assumed the main caregiver role to the siblings of hospitalized children in place of mothers in the period of children’s hospitalization. A cross-sectional, exploratory survey conducted in Japan examined 113 mothers’ and 90 other main caregivers’ perspectives regarding the psychological state of 2- to 18-year-old siblings of hospitalized children. Mothers and/or other main caregivers of siblings during their brothers’ or sisters’ hospitalization completed the Child Behavior Checklist and the Siblings’ Personal Growth Scale. Multiple linear regression analysis was performed with Child Behavior Checklist internalizing problems and total Siblings’ Personal Growth Scale scores as dependent variables for mothers’ and caregivers’ perspectives. From mothers’ perspectives, environmental factors that change with hospitalization affected siblings. From the perspectives of the other main caregivers, children’s and families’ demographic factors affected siblings’ psychological state. Frequency of e-mail contact between mothers and siblings, explanation of the hospitalized child’s condition, and hospital visitation rules (F = 5.88, P = .001) explained 12.3% of variance in mothers’ Siblings’ Personal Growth Scale scores. Among other main caregivers, 11.6% of variance in the Child Behavior Checklist scores was explained by hospitalized children’s birth order and main caregiver’s prehospitalization residence (F = 5.51, P = .006). Results suggest that the perceived variables related to siblings’ psychological changes differ between mothers and other main caregivers.
Keywords
The psychological well-being of the siblings of hospitalized children is at risk, yet little is known about the frequency of personal growth occurring in their siblings and the related variables thereof.
Internal problems and personal growth of siblings at the early stage of a child’s hospitalization were investigated, and the related variables of those 2 concepts were examined to determine how they differ from mothers’ and other main caregivers’ perspectives.
Health care providers should assess the psychological state of the siblings of hospitalized children by communicating with all caregivers from the environment in which the siblings are currently living, be that at home with the father or at the house of another relative.
Introduction
Siblings of children with chronic illness are at risk of having more internalizing and externalizing problems and less positive self-attributes than siblings of healthy children.1-3 Older siblings are reportedly more likely to experience psychological problems and observable difficulties.2,4 Siblings’ age and gender and ill children’s diagnoses also reportedly predict siblings’ psychological condition2,5; however, little is known of other variables that are related significantly to siblings’ psychological health.
In the patient- and family-centered care philosophy,6,7 parents are expected to spend 24 hours/day with their hospitalized children and encouraged to participate in care processes. 8 This increases the number of parents’, mostly mothers’, overnight stays, resulting in extended separation from their other children. 9 Under this increase, siblings separated from their mothers temporarily receive the majority of care from someone else—eg, their fathers, grandparents, or other relatives. This changing role often occurs in Japan; however, little is known about how these caregivers perceive the siblings’ psychological states during this temporary period of assuming the main caregiving role from the mother during a child’s hospitalization. Furthermore, the variables related to siblings’ psychological states from the perspectives of main caregivers other than mothers were not evaluated in prior research.
Most studies focus on ill siblings’ specific diagnoses (eg, cancer 1 ) and few on the effects of ill children’s hospitalization on their siblings.10,11 Furthermore, psychosomatic and behavioral problems and a poor quality of life prevail among siblings shortly after ill children’s diagnosis, although those issues gradually decrease following treatment commencement.12-14 Few studies have quantitatively evaluated environmental changes such as separation, hospital visitation frequency, or the healthy sibling’s residence during hospitalization in relation to their psychological condition.
Most studies have focused on hospitalization’s negative effects on siblings, instead of its positive effects or effects on their development, sense of responsibility, independence, or empathy. 1 Moreover, with increasing responsibility, some siblings may experience personal growth. 15 Furthermore, recent research on siblings of people with intellectual and developmental disabilities have suggested that a positive psychology framework is more appropriate in describing siblings’ psychosocial attributes.16-18 Although previous studies have assessed siblings’ personal growth by quantitatively focusing on the situation of a brother’s or sister’s hospitalization, 19 little is known about the frequency of personal growth occurring in siblings and the related variables thereof.
Discrepancies have been reported between siblings’ and parents’ perspectives.20,21 In contrast, parents and siblings have reported similar changes in feelings and behaviors following hospitalization of a child in the family. 15 Parents and/or closely related adults (eg, grandparents or other relatives) are considered important in sympathizing with siblings’ unexpressed feelings. Furthermore, when a child is hospitalized, health care providers rarely meet the siblings to enquire about their well-being; instead, health care providers often receive information about the siblings from the parents. Cooperation between parents and health care providers 22 facilitates this information exchange. Furthermore, fathers, grandparents, or other relatives temporarily or periodically assume a parental role toward siblings when parents, mostly mothers, care for the ill child. 23 Nevertheless, little is known about these adults’ perspectives regarding siblings of hospitalized children. To establish practices with genuine and appropriate pediatric patient- and family-centered care that includes siblings, the effects of siblings’ separation from hospitalized children, and often mothers, must be examined from the perspectives of the closest and the other main caregivers of siblings during hospitalization.
In the present study, we examined 3 questions. First, did internal problems and personal growth occur in the siblings of hospitalized children during the period of their brother’s or sister’s hospitalization? Second, what variables are related to siblings’ internal problems and personal growth? Finally, are there any different variables related to siblings’ internal problems and personal growth from the perspective of mothers and from the perspective of other main caregivers for the siblings of hospitalized children during their brothers’ or sisters’ hospitalization?
Method
Design
A cross-sectional, exploratory study design was used.
Participants
Participants were 113 mothers and 90 other main caregivers who temporarily assumed the main caregiver role to the siblings of hospitalized children instead of the mother in the period of children’s hospitalization.
Recruitment
In total, 484 medical institutions were recruited, having been randomly drawn from general hospitals with pediatric wards with ≥400 beds from the database of the Japan Municipal Hospital Association and children’s hospitals from the database of the Japanese Association of Children’s Hospitals and related institutions. Thirty-three institutions consented to participate in the research. Head nurses of the pediatric wards of each institution distributed the anonymous, self-administered questionnaires to mothers with >2 children, who were primarily present during children’s hospitalization. We included and analyzed responses of siblings from 2 to 18 years of age, excluding siblings of children hospitalized for >1 year and/or cases when mothers did not visit or stay with inpatients. Also, invalid/incomplete questionnaire responses were excluded. In cases of ≥2 siblings, the questionnaire could be answered with respect to only whichever of these siblings chose to answer. When mothers reported someone else acting as the main caregiver for siblings in the meantime, they were asked to mail or hand in the caregivers’ questionnaires alongside their own. Participants mailed the questionnaires to the principal investigator (PI), using the provided self-addressed stamped envelope. The number of all distributed questionnaires, obtained from all head nurses, was the response rate.
Procedures
The questionnaire was developed and not piloted; however, we used a questionnaire that improved the present study version 24 under the supervision of professors of pediatric nursing. The survey was conducted between January 2015 and March 2015. Questionnaires were returned by 140 mothers (response rate = 37.4%) and 118 caregivers (response rate = 33.4%). Eight-four of the mothers and other main caregivers were from the same family. Of these individuals, 79 responses by the mother and the other main caregiver referred to the same sibling, and the remainder referred to different siblings in the same family. There were 29 mothers and 6 other main caregivers who were the only representative of their family. Note that all responses were pooled because we were not specifically interested in differences among caregivers or families. All participants were contacted once by the researchers. No compensation was given for participation.
Ethics
The Institutional Review Board of Osaka University Hospital approved the study (14499(311-1)-2). Informed consent was obtained from all participants.
Measures
Demographic characteristics
Demographics items were included primarily based on their previously suggested relevance to siblings’ condition (see Table 1).1,10,20,24 These items were surveyed to determine the independent variables for the present regression analysis. The independent variables are shown in Table 2 and were significantly correlated with Siblings’ Personal Growth Scale (SPGS) or Child Behavior Checklist (CBCL) independently from perspectives of mothers’ or the other main caregivers’ models.
Participants’ Demographics and Background Characteristics.

Note. No significant differences were found between mothers and other main caregivers in CBCL and SPGS scores. CBCL = Child Behavior Checklist; SPGS = Siblings’ Personal Growth Scale.
Correlations Between Demographics, Background Characteristics, SPGS, and CBCL.
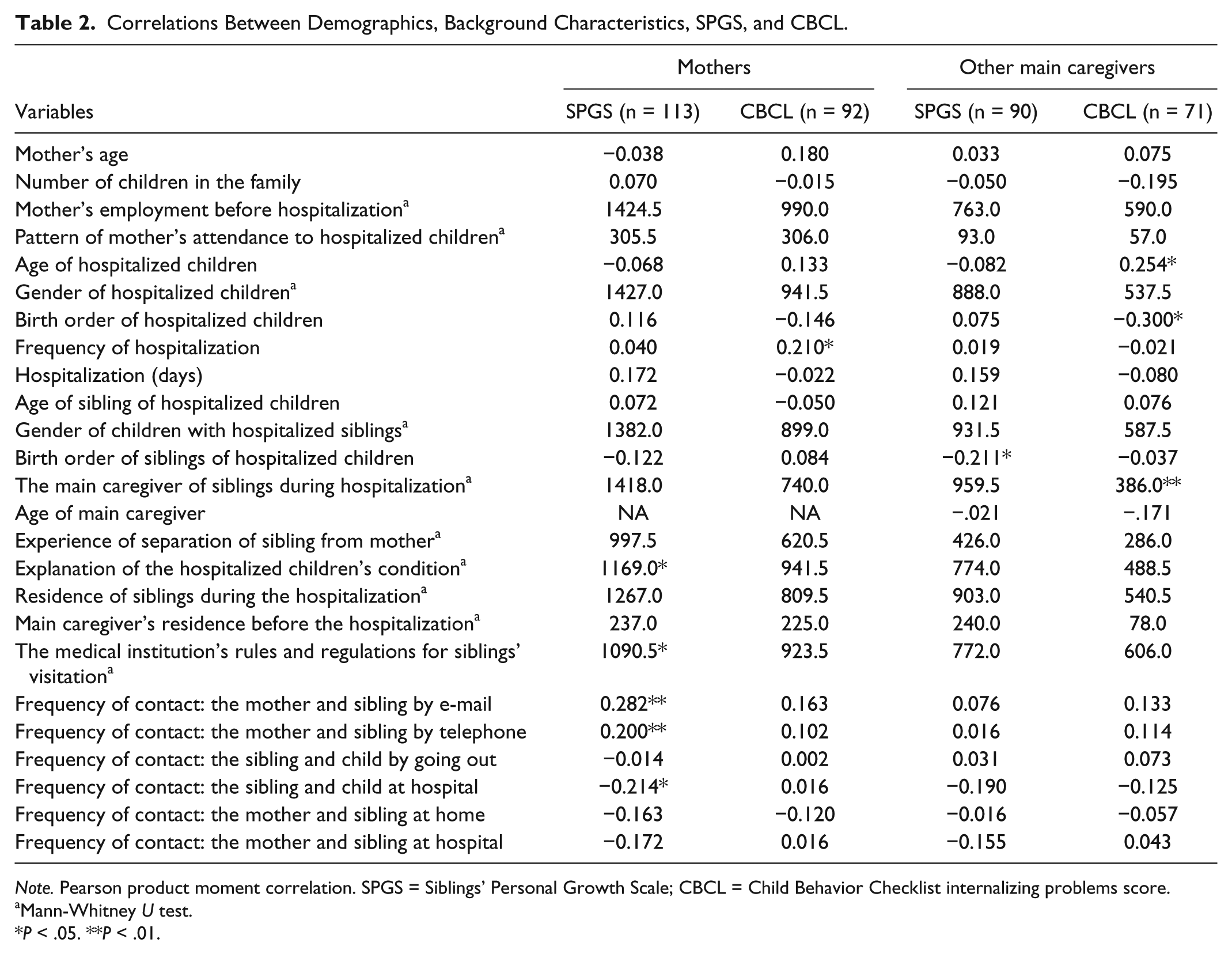
Note. Pearson product moment correlation. SPGS = Siblings’ Personal Growth Scale; CBCL = Child Behavior Checklist internalizing problems score.
Mann-Whitney U test.
P < .05. **P < .01.
The CBCL 25 comprehensively assesses children’s emotional and behavioral problems from parents’ perspectives. We used the validated Japanese version. 26 All 113 items form 2 subscales (internalizing problems/externalizing problems). Considering the questionnaire’s length and previous consideration of siblings’ problems as related to internal problems,2,24,27,28 we used the internalizing problems scale, comprising 31 items. Thirty-one items were distributed across 3 syndrome scales: (1) “withdrawn,” (2) “somatic complaints,” and (3) “anxious/depressed.” Items were answered on a 3-point Likert-type scale, with categories of 0 = not true, 1 = somewhat or sometimes true, and 2 = very true or often true. Higher scores on the syndrome scales indicated greater severity. Scores were classified into the normal, borderline, or clinical ranges based on standardized cutoff points. The clinical range indicates that a child needs professional support. The CBCL Japanese version is appropriate for use with 4- to 15-year-old children. Cronbach α for the CBCL internalizing problems scale in this study was 0.94 with use on mothers and 0.88 on caregivers.
The SPGS 19 is a 22-item parent-report measure of siblings’ personal growth, pertaining to their brothers’/sisters’ hospitalization. The scale comprises 3 subscales: (1) “altruistic behavior” (10 items; eg, showed sympathy, showed kindness and warmth, showed empathy, behaved in an encouraging manner); (2) “development of emotional and social skills” (8 items; eg, increased emotional depth, expressed one’s own feelings and intentions, willingly interacted both with people and the wider society); and (3) “self-control” (4 items; eg, stopped using spoiled or selfish speech, became better at dividing attention and following directions, exhibited more patience). The items were answered on a 4-point Likert-type scale, with categories of 1 = not at all, 2 = somewhat, 3 = moderately, and 4 = extremely. The SPGS is appropriate for use with 2- to 18-year-old children. The SPGS was developed and began to be used in Japan. Cronbach α for the SPGS in this study was 0.87 for use with mothers and 0.96 for caregivers.
Data Analysis
Analyses were performed using IBM SPSS Statistics 21 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the demographics, background characteristics, and scores on the CBCL internalizing problems and the SPGS. Pearson correlations assessed associations between the quantitative variables, and Mann-Whitney U test assessed the association between the binary variables, with the CBCL’s and SPGS’s quantitative variables. Variables identified as significant from these results were set as independent variables; multiple linear regression analysis was performed with the total SPGS and CBCL internalizing problems scores as the dependent variables for both mothers’ and the other caregivers’ perspectives. Multicollinearity was examined using tolerance values and variance inflation factors. The percentage of missing data on items for both CBCL and SPGS was <10%; these missing items were replaced with mean values. All other responses with missing or incomplete demographic data were excluded from the analysis. Post hoc analysis indicated enough power (0.82-0.95) for each regression models with effect size of 0.15 (median) and significant level of 0.15.29,30 Values of P < .05 were considered statistically significant.
Results
Participants’ Demographics
The siblings’ mean age was 6.4 years (SD = 3.2 years), based on mothers’ responses, and 5.6 years (SD = 3.6), based on caregivers’ responses (Table 1). Most mothers stayed in the same room as their child inpatients. Slightly less than a quarter of siblings had left their own homes and lived in their respective caregivers’ homes during hospitalization of the child inpatients. Grandmothers living apart from siblings (47.3%) most often assumed the main caregiver role for siblings, followed by fathers (41.8%). The average hospital stay lasted 24.1 days (SD = 53.5 days) for mothers and 26.3 days (SD = 56.0 days) for caregivers; the median was 7.0 and 8.0 days, respectively. The current diagnoses or condition of the hospitalized children varied, including digestive system disease, cardiovascular disease, nephrologic and urologic disease, infections, immunologic conditions, allergies, autoimmune conditions, respiratory issues, neurologic issues, motor system problems, and hematologic or oncologic diseases.
In total, 15.2% (based on 92 mothers’ perspectives) and/or 16.9% (based on 71 of the other main caregivers’ perspectives) of siblings had reached the clinical score range on the CBCL internalizing problems (Table 1). Approximately 30% of siblings were presumably in the borderline or clinical range from the mothers’ and caregivers’ perspectives.
The average score per item in SPGS was 2.13 in total. The average scores based on the mother’s perspective were 2.30 in altruistic behavior, 1.95 in development of emotional and social skills, and 1.95 in self-control based on mothers’ perspective. The average respective scores based on the perspective of other main caregivers were 2.11, 2.26, 2.02, and 1.95.
Correlations were calculated between demographics, background characteristics, and the SPGS and CBCL internalizing problems scores, as provided by mothers and caregivers (Table 2). Greater SPGS gain was associated with explaining the hospitalized child’s condition sufficiently to siblings, siblings not being able to visit the hospitalized inpatient, more frequent contact via e-mail and telephone between mothers and siblings, and less frequent contact between siblings and hospitalized inpatients, from the mothers’ perspective. More CBCL internalized problems were associated with less frequent hospitalization of the child inpatients, from the mothers’ perspective. Greater SPGS gain was associated with a lower birth order of children with hospitalized siblings, from the caregivers’ perspective. More CBCL internalized problems were associated with older age, a lower birth order of the child inpatients, and living with the main caregiver before hospitalization.
Regression Analyses
A multiple regression analysis (backward elimination method) showed that 4.4% of the variance in the CBCL from the mothers’ perspective was explained by the frequency of child inpatients’ hospitalization (F = 4.00, P = .049). In total, 11.6% of the variance in the CBCL from the caregivers’ perspective was explained by the hospitalized children’s birth order and living with the main caregiver before hospitalization (F = 5.51, P = .006; Table 3). Moreover, 12.3% of the variance in the SPGS from the mothers’ perspective was explained by the frequency of contact by e-mail between mothers and siblings, explanation of the hospitalized child’s condition, and hospitals’ rules and regulations for visiting (F = 5.88, P = .001). Furthermore, 4.4% of the variance in the SPGS from the caregivers’ perspective was explained by the birth order of siblings with hospitalized children (F = 4.08, P = .046; Table 4). Multicollinearity was not a concern among the independent variables, given the variance inflation factors of all final models.
Multiple Regression Analysis of CBCL.

Note. CBCL = Child Behavior Checklist Internalized problems score; β = standard coefficient; B = unstandardized coefficient; CI = confidence interval for B; VIF = variance inflation factor.
Multiple Regression Analysis of SPGS.
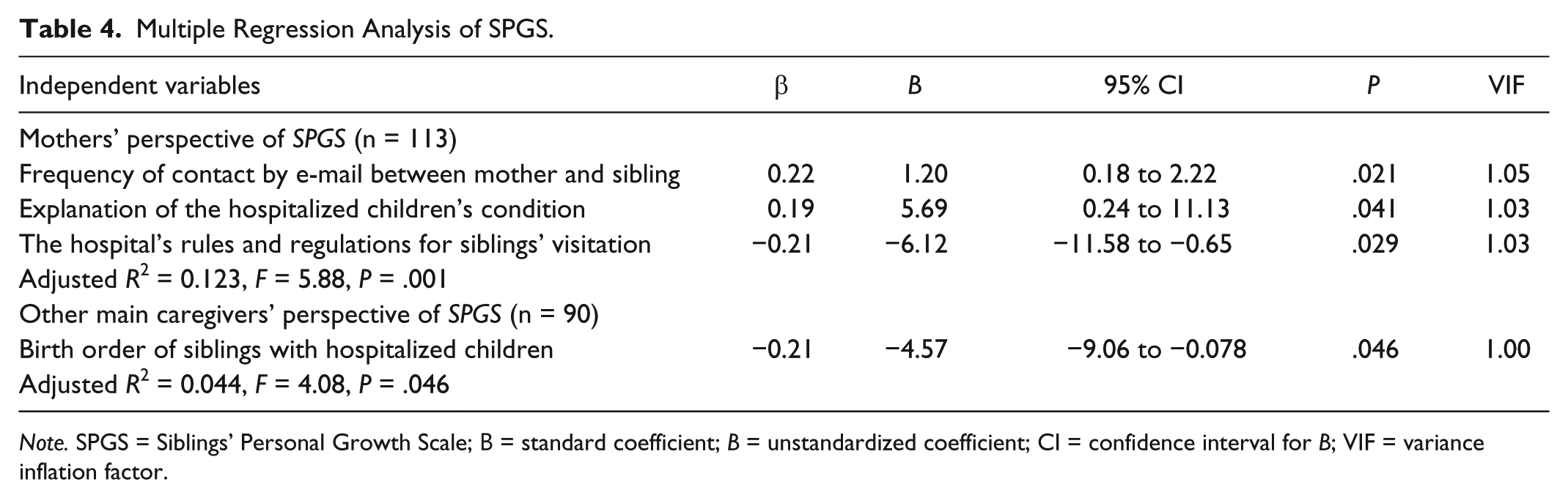
Note. SPGS = Siblings’ Personal Growth Scale; Β = standard coefficient; B = unstandardized coefficient; CI = confidence interval for B; VIF = variance inflation factor.
Discussion
Our results indicated that most mothers stayed overnight with the child inpatient, whereas the father, grandparents, or other relatives assumed the main caregiver role for the siblings. Furthermore, slightly less than half of the siblings received care mainly from a family member living with them, most from the father, and almost half from a person not living with them—often a grandmother, prehospitalization. Moreover, many siblings stayed at the caregivers’ homes. The descriptive statistics that resulted indicated that each family member possibly swapped roles and took up new daily routines. 31 Also, staying at the caregiver’s home could possibly have induced the psychosocial difficulties induced by many siblings, with some caused by malfunction in daily interaction with friends and teachers 32 ; absence from school may also lead to siblings’ distress.33,34
Our results indicated that more than 15% of the siblings of inpatient children were in the clinical range of the internalizing problem score on CBCL from both mothers’ and other main caregivers’ perspectives in median at a week before and after the start of inpatients’ hospitalization. These results were more severe than suggested by a study of the siblings of children with sickle cell disease (SCD) by Gold et al. 35 Gold et al showed that, from the parents’ perspective, the means obtained on the CBCL scale did not fall into the clinical range, whereas 9.4% of subjects were in the clinical range for the internalizing problems score, with 7.6% being withdrawn, 10.9% having somatic complaints, and 7.6% being anxious/depressed. Also, the survey of CBCL and study of siblings of children with cancer by Cordaro et al 4 indicated that the former’s difficulties were not greater than those of a control group. From the above, it could be assumed that we investigated the impact of hospitalization and separation among siblings in the early stages of hospitalization, considering the median days of hospitalization. Despite the hospitalized children’s illness type, many siblings required professional support, from mothers’ and caregivers’ perspectives.
From the average score per item of SPGS both from the mothers’ and the other main caregivers’ perspectives, it could be considered that some or more personal growth occurred in the siblings of child inpatients. Among the 3 subscales, altruistic behavior occurred in the siblings of inpatients most often in the early stages of a child’s hospitalization.
Our results of multiple regression analyses showed that mothers and other main caregivers differed in the independent variables they believed were related to siblings’ internalizing problems and personal growth, as indicated by the variance explained. It could be considered from the results of the mothers’ perspectives that siblings of hospitalized children are affected by changing environmental factors that accompany a child’s hospitalization. Moreover, from the other caregivers’ perspectives, demographic factors of hospitalized children, their siblings, and the family have implications for the siblings of child inpatients.
On the mothers’ perspective, it was suggested that high-frequency e-mail communication with siblings of child inpatients and explanation of the hospitalized children’s condition support the siblings’ positive personal growth. This result suggests that e-mail communication facilitated easy, direct communication and mutual awareness of the siblings’ and mothers’ states. Then mothers could update the siblings about the hospitalized child’s condition, facilitating mutual support. Our quantitative findings are supported by some previous qualitative studies and review papers that indicate, for example, that information-sharing is important to consider in sibling stress 20 and that sufficient information-sharing with siblings about their brothers’/sisters’ condition can extend their knowledge about the inpatient child’s condition and can reduce excess or unnecessary anxiety and fear.32,36,37
Primarily, visits are important and recommended, as siblings enable the family to spend time together and share accurate information about the inpatient’s and mother’s conditions.15,38 Despite this, our result from the mothers’ perspective indicated that medical institutions’ rules and regulations regarding siblings’ permission to visit child inpatients decrease siblings’ personal growth. In this regard, Simon 39 reported that children visiting their hospitalized siblings daily experienced more stress (anxiety) than those visiting every other day or weekly. In addition, Gold et al 35 reported that more frequent emergency room visits predicted poor psychosocial adjustment among siblings of children and adolescents with SCD. These studies do not detract from the importance of visits to child inpatients by their young siblings for information-sharing. They also do not address the kind of care that is needed for effective visiting, including attention to features of the visit that may have a positive or a negative impact on siblings during hospital visits
Also from mothers’ perspectives, our results indicated that hospitalization frequency was related to internalizing inclinations among the siblings of child inpatients. This result raises the possibility that frequent separation from the mother and hospitalized brother or sister and from regular daily life may facilitate siblings’ psychological distress.
Our results suggest that from the perspectives of the main caregivers who take the place of mothers during a child’s inpatient treatment, earlier birth order of hospitalized children is directly related to more internal psychological problems occurring in their siblings. These results are supported by Hamama et al 40 who compared 9- to 13-year-old and 14- to 18-year-old siblings of children with cancer and showed greater loneliness among the adolescents. Furthermore, other studies of 7- to 18-year-old siblings of children with cancer suggest that older age is associated with more anxiety, poorer physical quality of life, and negative emotions.4,13,41,42 Moreover, Cordaro et al 4 showed that older siblings of children with cancer have more observable difficulties, compared with younger siblings. Another result from the other main caregivers’ perspective suggests that earlier birth of siblings of child inpatients is related to more personal growth. We considered siblings’ and hospitalized children’ ages, and siblings’ birth order—reflecting the age-based relationship between the 2 sets of children—internalizing problems, and personal growth, from the caregivers’ perspective. Presumably, older siblings show more psychological distress, compared with younger hospitalized siblings, due to the latter being relatively young. Moreover, the former are burdened by excessive responsibilities and/or the pressure to undertake an important role within the family. 43 The other main caregivers perceive such changes among siblings more directly than mothers who stay with their inpatient child in hospital. However, others typically expect either too much or little of siblings.
More internalizing problems among siblings were perceived by the other main caregivers with whom they had originally resided, as compared with caregivers who had not previously resided with the siblings. Living together before hospitalization would presumably render caregivers more sensitive or aware of siblings’ change in state before hospitalization.
Implications for Practice
Regardless of the inpatient children’s illness type, health care providers could predict that hospitalization and separation among siblings in the early stage of hospitalization may possibly have an impact on child inpatients’ siblings. In particular, it may forecast internal problems and/or personal growth that could occur in some children who are separated from their inpatient siblings. Therefore, health care providers should focus not only on problem solving but also upon attending to a sibling’s capacity for personal growth, which will be in some degree evident from the child’s present psychological state. Health care providers could intervene and protect and support siblings’ self-esteem through focusing on personal growth and palliate the internal problems the siblings have. Therefore, given the possibility that related variables are different in the perspective of mothers and in that of other main caregivers, health care providers should assess the psychological state of the siblings of hospitalized children by communicating with all caregivers from the environment in which the siblings are currently living, be that at home with the father or at the house of another relative. In addition, it is better for health care providers to focus multilaterally on related variables rather than to limit the variables of interest when considering suitable care for siblings and families.
Limitations and Directions for Future Research
Compared with European and American institutions,38,44 in Japan, visitation by siblings is severely restricted due to developments regarding preventive vaccination, concerns regarding pediatric infections, and cultural practices. Moreover, many Japanese institutions do not have enough experience to welcome healthy children, even if they are siblings of inpatient children into pediatric wards. Therefore, our results are possibly unique to Japan.
Although data were based on caregivers’ reports, to grasp the siblings’ nature of psychological aspects, we should obtain data from people in various positions, beginning with the siblings of child inpatients themselves. Binary independent variables have limitations when interpreting results—ie, although visits are important and recommended for siblings, our results indicated the permission for siblings of child inpatients to visit decreases the siblings’ personal growth. On this point, further qualitative in-depth research is required to describe more fully the meaning of visitation to child inpatients by siblings.
The present study collected data from perspectives of mothers and other main caregivers during inpatients’ hospitalization periods. However, the present study investigated the mothers’ and the other main caregivers’ perspectives independently to elucidate the degree of coincidence or difference from need-paired samples and studied these from both quantitative and qualitative approaches.
CBCL was not aimed at comprehensively evaluating siblings’ experiences. However, arguably, there is no difference between siblings of children with cancer and healthy siblings, 4 possibly indicating limited perspectives regarding siblings of children with chronic illness. Furthermore, a more comprehensive, quantitative scale measuring the experiences of siblings of hospitalized children with illness and/or disabilities is needed. Moreover, future research should adopt in-depth and/or content analysis to comprehensively investigate siblings’ setbacks and personal growth. In addition, we did not investigate the details of differences between responders and nonresponders from each institution which consented to participate in the research.
Conclusion
The present study showed marginal differences and moderate-to-high similarities in the perspectives of mothers and other main caregivers in terms of the behavioral and emotional problems and the personal growth of siblings of hospitalized children. Regardless of the hospitalized children’s type of illness, many siblings needed professional support in the early stages of the hospitalization and separation periods. However, the variables related to siblings’ psychological changes differ between mothers and other main caregivers. From the mothers’ perspective, environmental factors that change with hospitalization affect siblings. However, from the other main caregivers’ perspective, the demographic factors of both the hospitalized children and their siblings and family affect siblings’ psychological state.
Footnotes
Acknowledgements
The authors sincerely thank all participants, nurses, and institutions who cooperated in the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI (grant numbers JP25862189 and JP16K12142).