
Abstract
The purpose of this research was to explore and compare common health system factors for 5 Community Living Centers (ie Veterans Health Administration nursing homes) with high performance on both resident-centered care and clinical quality and for 5 Community Living Centers (CLC) with low performance on both resident-centered care and quality. In particular, we were interested in “how” and “why” some Community Living Centers were able to deliver high levels of resident-centered care and high quality of care, whereas others did not demonstrate this ability. Sites were identified based on their rankings on a composite quality measure calculated from 28 Minimum Data Set version 2.0 quality indicators and a resident-centered care summary score calculated from 6 domains of the Artifacts of Culture Change Tool. Data were from fiscal years 2009-2012. We selected high- and low-performing sites on quality and resident-centered care and conducted 12 in-person site visits in 2014-2015. We used systematic content analysis to code interview transcripts for a priori and emergent health system factor domains. We then assessed variations in these domains across high and low performers using cross-site summaries and matrixes. Our final sample included 108 staff members at 10 Veterans Health Administration CLCs. Staff members included senior leaders, middle managers, and frontline employees. Of the health system factors identified, high and low performers varied in 5 domains, including leadership support, organizational culture, teamwork and communication, resident-centered care recognition and awards, and resident-centered care training. Organizations must recognize that making improvements in the factors identified in this article will require dedicated resources from leaders and support from staff throughout the organization.
Keywords
Nursing homes (NH) have been influenced by 2 divergent paradigms: The medical model focused on standardized clinical care quality and resident-centered care (RCC) targeting improved quality of life. In 1987, the Omnibus Budget Reconciliation Act (OBRA) created both compliance requirements for quality of life and incentives for nursing homes to provide care consistent with a medical model, one that emphasizes standardization, safety, and clinical quality. 1 Beginning in the mid-1990s, many nursing homes also began implementing various culture change models focused on promoting RCC, which was in reaction to OBRA not achieving its outcomes related to quality of life. The RCC models involve shifting the care focus from the medical care paradigm to one that also promotes better resident quality of life and resident self-direction, including individualized care, transformed physical environments, and changed staff roles.2,3
Although the 2 paradigms focus on different aspects of care provision, they are theorized to be related and affect NH performance. For example, RCC could be a means of improving resident quality of life, which in turn can lead to improvements in clinical care quality via having more information about resident status or medical issues. 4 Studies in the private sector on RCC on quality outcomes such as those measured through the Minimum Data Set (MDS) or other survey deficiencies (eg, The Joint Commission citations) have found no effect or mixed effects.4-8 In the Veterans Health Administration (VA), cross-sectional research from 130 Community Living Centers (CLCs) (ie, VA-owned and VA-operated nursing homes) showed a relationship between the use of RCC and a composite measure of quality based on the MDS, 9 but more recent longitudinal research (fiscal years [FY] 2009-2012) found no relationship.10,11 Sullivan et al noted there were a few CLCs that were consistently high and low performers on care quality and RCC measures (ie, “high”- and “low”-performing facilities). 15 In the high-performing facilities, improvements in RCC were associated with increases in quality, whereas in the low-performing facilities, declines in RCC were associated with decreases in quality. These findings suggest that there may be system factors that distinguish between high-performing facilities (ie those that perform well on both quality and RCC) and low-performing facilities (ie those that perform poorly on both quality and RCC).
To date, research exploring clinical care quality and RCC has primarily focused on the relationship between the 2 paradigms. Far less is known about how and why some facilities are able to provide high levels of both RCC and care quality, whereas others are not. Furthermore, qualitative research in NHs has centered on examining factors associated with either care quality or RCC. The literature regarding factors affecting NH performance are influenced by 2 facets: (1) structural characteristics, including patient mix,12-14 staffing levels,15,16 administrator tenure,17-19 and monetary resources,20,21 and (2) organizational infrastructure, including organizational culture,22-24 utilization of quality improvement/systems redesign infrastructure,21,25-27 alignment/coordination,20,22,28-31 teamwork and communication,32-34 and supportive leadership.25,35-38
To address gaps in the literature, the objective of this article is to examine factors that distinguish between facilities providing high and low levels of both care quality and RCC utilizing data from a larger mixed methods study focused on care quality, RCC, and costs in VA CLCs. 10 The VA is an ideal setting to conduct this research because it is an integrated national network with a large number of CLCs. Similar to the private sector, the VA requires CLCs to monitor quality by undertaking assessments of long-stay residents (those staying over 90 days) using the Resident Assessment Instrument (RAI) MDS. The RCC paradigm was implemented in VA about 10 years ago and data on RCC have been collected using the Artifacts of Culture Change Tool to assess progress. In 2017, VA also began incorporating a new RCC measure—resident/staff engagement. 39
Methods
This study used a sequential explanatory mixed methods design.40,41 Figure 1 displays a visual model. First, we identified high and low performers on clinical care quality and RCC using previously published methods.10,15 Next, we selected CLCs based on these data and conducted primary data collection by means of staff interviews at 12 CLCs and systematic content analysis of the transcripts. The purpose of the qualitative in-person site visits was to investigate the “how” and “why” some CLCs are able to deliver high levels of RCC and high MDS-based quality of care. After analyzing the qualitative data, we integrated the quantitative and qualitative data to identify the qualitative health system factors related to performance on Quality and RCC dimensions (high versus low on both dimensions). We received Institutional Review Board (IRB) approval from VA’s Central IRB to conduct this study.
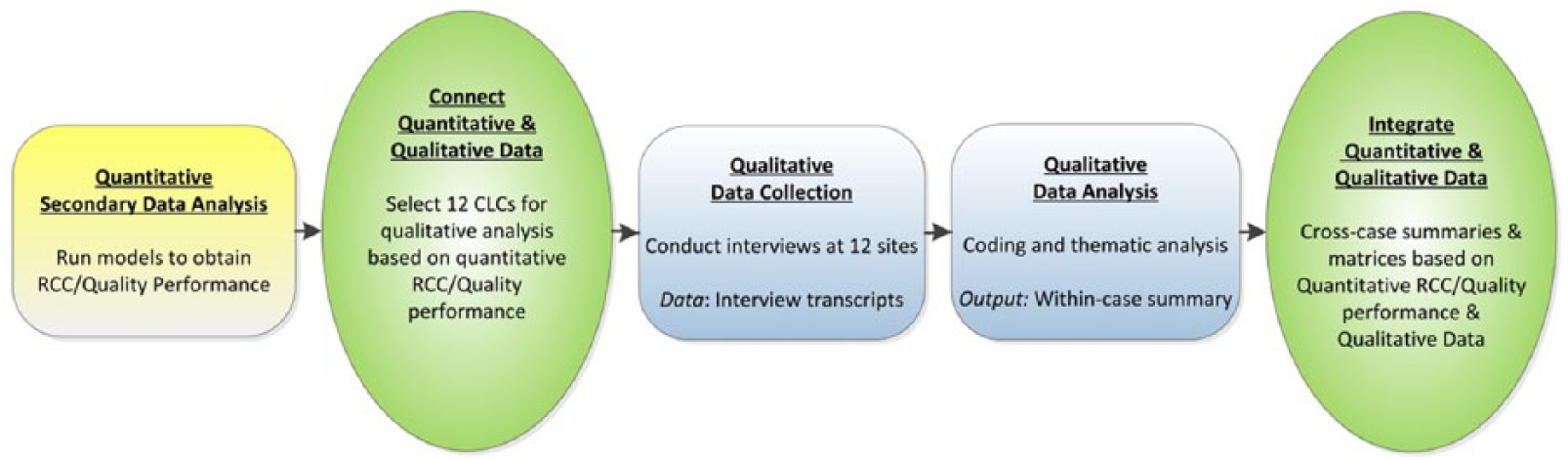
Visual model for mixed methods sequential explanatory design procedures.
Site Selection
In total, 130 CLCs were identified based on their rankings on a clinical care quality composite measure calculated from 28 MDS version 2.0 quality indicators 10 and an RCC summary score calculated from 6 domains of the Artifacts of Culture Change Tool. We were unable to use Artifacts data from 12 CLCs due to lack of matching MDS quality indicator data. Data were from FY 2009- 2012. The Supplementary Appendix contains information on how we calculated the quality and RCC measures. We assessed both the most recent score from FY2012 Quarter 3 and change in the score over an 18-month period prior to FY12 Quarter 3. We ranked the CLCs on both quality and RCC and selected 4 sites ranked highest on both quality and RCC domains, 4 sites ranked lowest on both quality and RCC domains, and 4 sites with mixed performance (eg, high on quality and low on RCC). Overall, this site selection process is driven by what Yin describes as “replication logic” for qualitative research involving multiple cases: Cases should be chosen such that some are expected to be similar on theoretically relevant dimensions, whereas others will be expected to differ. 42
As previously reported, due to changes in performance status between initial site selection and qualitative data collection, our final data set included 5 high- and 5 low-performing sites. 15 Because available quality and RCC data were 2 years older than when the site visits occurred, we triangulated the qualitative data we collected with site visitor impressions of performance on RCC and quality at the time of data collection. Comparison of the data with the impressions resulted in the recategorization of 2 mixed sites. In particular, 1 site became a high performer and 1 site became a low performer. We omitted 2 mixed sites from our analysis because both the qualitative data and site impressions suggested their performance status no longer met our inclusion criteria (ie, either high performance on both quality and RCC or low performance on both quality and RCC).
Sample of CLC Staff
We recruited a diverse group of staff members from the CLCs in our sample, including executive leaders, middle managers, and frontline CLC staff, to provide viewpoints from staff at all levels at the CLC. Prior to scheduling the site visits, VA Central Office sent a notice to the selected sites indicating support for the study. Thereafter, we contacted each CLC director (or their administrative support staff), who provided us with the names of potential respondents (eg, CLC staff members) via e-mail group lists. We then contacted staff members and set up in-person site visits. To avoid coercion, the CLC director and the employee’s actual supervisor were not involved or told which employees had agreed to be interviewed.
Data collection
Semi-structured interview guide
We developed our interview questions based on the literature including structural characteristics and organizational infrastructure.12-38 We created an interview guide consisting of 33 semi-structured questions corresponding to these domains. We also asked questions regarding clinical care and RCC processes to understand how care was provided at the CLC. We pilot-tested the guide with a CLC staff member at our home site and found the respondent understood the questions and did not feel additional questions were need. We then created 3 versions of the interview guide—one each for frontline staff, middle managers, and leaders. The consolidated interview questions can be found in the Supplementary Appendix.
Site visits
We collected data through 2-day in-person site visits. Teams consisted of 2 experienced health care researchers with specific knowledge of CLC care and VA structures and processes. All team members were blinded to the performance status of the CLCs they visited in an effort to minimize the selective attention that could be induced by preconceptions about conditions at “highly ranked” and “poorly ranked” CLCs. Site visit team pairings were rotated to mitigate any bias that might arise if 2 people always worked together. Individual interviews were approximately 60 minutes in length and were audio-recorded.
Data analysis
Figure 2 displays our data analysis workflow for this study. Verbatim interview transcripts were the primary source for data analysis. A team of 5 analysts (J.L.S., R.L.E., D.T., M.K.A., K.G.) coded the transcripts in NVivo qualitative software for evidence of a priori domains based on the literature. We used an inductive approach to identify additional emergent domains relevant to the study’s goals. The domains and definitions can be found in the Supplementary Appendix. Inter-rater reliability of 75% was established using a “check-coding” process where all coders independently coded the same interview transcript, and initial reliability estimates between all coders were computed. Coders then met to compare their coding, discuss areas of disagreement, and reach consensus. This process was repeated until a stable level of agreement of 75% was achieved across all coders. 43

Data analysis workflow diagram.
Within-case site summaries for each site were created from the coded transcripts and were organized by a priori and emergent domains. Quotes included in the site summary represented views from multiple levels within the organization (frontline, middle manager, and senior leader). To determine data sufficiency within a CLC, the analysts assessed the level of agreement among informants within the organization (eg, if 2 or more informants described a phenomenon, then it would be considered for inclusion). We not only captured views of the majority of staff within a site but also included verbatim quotes when there was an alternate viewpoint from at least 2 staff members. All team members participating in analysis were blinded to hospitals’ performance status until all single-site summaries were complete.
We then created cross-site summaries based on performance categories. Guided by the analytic approach Miles and Huberman, 43 the coding team assessed whether there were similarities for sites in comparable performance categories.
We took several steps to stay reflexive during this study. As mentioned above, we made use of site visitor impressions. Site visitors would write their impressions about the site and interviews at the end of each day. At the end of the site visit, visitors were also asked to rate the level of quality and RCC at the site. Team members were then expected to debrief on how the visit was going and what their impressions were. We used a semi-structured interview guide which helped mitigate some of our internal biases as the same questions were asked of the respondents. In addition, our team met regularly to discuss questions and potential biases with regard to the data collection and analysis. Finally, within-case site summaries were prepared by a team member who was not on-site for the site visit and unaware of the site teams’ site impressions regarding status of quality and RCC at that site. Thus, these practices helped us be mindful of how we conducted the research.
Results
The purpose of this study was to identify health system factors present in CLCs that ranked highly on both quality and RCC dimensions in comparison with CLCs that ranked poorly on both care quality and RCC. Table 1 shows site characteristics and quality/RCC rankings by performance category. In particular, the rankings were used to select the sites for participation in our study. The selected CLCs were spread out throughout the United States and had average 18-month long-stay resident census that ranged from 14.8 to 86.6. Table 2 displays the distribution of our sample across site and by performance. In total, we interviewed 108 respondents distributed equally among high-performing CLCs (n = 51) and low-performing CLCs (n = 57). Frontline staff made up about half of our sample.
Site Characteristics and Quality/RCC Ranking by Performance Category.

Note. Lower ranking have the best (eg, high) performance. RCC = resident-centered care; MDS = Minimum Data Set; FY = fiscal year; Q = quarter.
Average 18-month Long-stay Resident census is calculated from the MDS version 2.0 quality data denominators from FY2010 Quarter 2 to FY2012 Quarter 3.
Sites were initially considered mixed performance given their rankings on quality and RCC. Based on the qualitative results and staff impressions, the sites were recategorized—one as a high performer (site E) and one as a low performer (site D).
Respondents by Site and Site Performance.

Note. Executive leaders included Medical Center Directors, Chiefs of Staff, Nurse Executives, and Associate Medical Center Directors. Middle managers included Nurse Managers, CLC Medical Directors, other Department Managers, and Program Managers (eg, Geriatrics, Hospice, Systems Redesign). Frontline staff included Nurses, Providers, Social Workers, Dieticians, Psychologists, and additional allied support staff. CLC = community living center.
Of the health system factors identified, we found variations between high and low performance sites on 5 domains, including leadership support, organizational culture, teamwork and communication, RCC training, and RCC rewards and recognition. Table 3 summarizes the themes. We present each domain in the sections below and include illustrative quotes from high- and low-performing sites in the Supplementary Appendix. We had insufficient data (ie, less than 2 or more informants described a phenomenon at that site) to make comparisons for 5 domains, including safety and medical care protocols, quality champions, personal involvement in quality initiatives, staff awareness of RCC practices, and personal involvement in RCC initiatives.
Health System Factor Variation in High- and Low-Performing Sites.

Note. RCC = resident-centered care; CLC = community living center.
Leadership support
There were many common themes across sites regarding leadership support. In many sites, participant perceptions of senior leader support for RCC were mixed, although the extent to which they were mixed varied. Common elements of senior leader support for RCC included providing resources, providing recognition, and being available (via mechanisms such as leadership rounds or town hall meetings). Senior leader support for quality was reported to be strong in every site, although the forms of that support differed.
Almost all high-performing sites mentioned middle management support, while mentions of this support were absent from all but one of the low-performing sites. Middle management support was described in terms of middle managers being available, visible, accessible, listening and recognizing needs, and being more concrete. High-performing sites mentioned updates and open communication in the context of senior leader support for quality, as well as assistance in garnering necessary staffing. In high-performing sites, senior leader support for RCC was generally characterized as including encouragement, provision of necessary resources, and communicating support through large-scale communications such as broadcast messages. To the extent reports were mixed, it was a minority view, and the reported deficiencies related to lack of financial support for RCC.
In low-performing sites, the mixed view of senior leader support for RCC was not a minority standpoint and was often linked to leader turnover and lack of continuity. Others reported that senior leadership was slow but ultimately responsive. Others found senior leaders to make decisions without input or to provide inadequate recognition. The low-performing site view of senior leader support for quality was less linked to availability and resources and more illustrated by leadership focus and desire for data. For example, leaders at low-performing sites seemed less focused on prioritizing quality or RCC and often requested seeing data supporting quality/RCC before supporting additional improvement efforts.
Organizational culture
One common theme across high and low performance categories was the commitment to veterans as an influential component of the culture and values in the organization, even when faced with the challenges to delivering resident-centered care.
Although there was not total agreement on cultural attributes within high-performing sites, there were some recurring themes. These included the sense that staff members were empowered to speak up and make decisions, a culture of continuous quality improvement, focus on veterans’ preferences being central to care decisions, and norms of honest, open communication. In addition, facilities in this category reported that staff members were open to change and learning about new models of care. Some CLCs had difficulty making changes to negative aspects of past cultures.
The focus on continuous culture change was voiced by many. If staff felt like management was listening to their suggestions, it was perceived as being much easier.
At the low-performing sites, a number of negative cultural attributes were reported, although not all of them extended across all of the facilities in this group. These included a focus on quality to the exclusion of other aims (notably resident-centered care), lack of flexibility, us and them dynamics among different shifts and/or disciplines, high turnover (of staff, leadership, or both), and sense of laboring under negative stereotypes about CLC care and CLC staff. In some of these sites, the last issue is beginning to change, although slowly: In fact, many of the low-performing sites reported recent changes for the better. However, these were often tempered by frustration over repeated changes in leadership perceived to be disruptive to progress.
Teamwork and communication
There were common themes across all sites on the topic of teamwork and communication. All sites utilized interdisciplinary team meetings to work together as a team and communicate information between disciplines. These team meetings consisted of staff from all disciplines involved in care of the resident, as well as the resident and/or family when needed. All sites emphasized the need for a nonpunitive culture in order to foster teamwork and communication. All sites implored similar modes of communication including both formal (eg, electronic medical record, rounds) and informal (eg, one-on-one conversations). Finally all sites, regardless of whether they described teamwork and communication as positive or negative, mentioned that there was room for improvement.
High-performing sites had open communication both at various levels and disciplines. Open door policies were cited that encouraged staff to speak up and bring issues to their managers, as well as encourage staff to communicate with each other about issues that may arise. High-performing sites positively described teamwork and communication between different disciplines to provide care (eg, communication between physicians and nurses). With regard to nonpunitive culture, while all sites recognized the importance of a nonpunitive culture, high-performing sites described communication and teamwork that were friendly and respectful, whereas low-performing sites reported the need to remove barriers that caused interpersonal stress.
Low-performing sites had silos or pockets of positive teamwork and communication, but it was not pervasive throughout the CLC. Variation in teamwork and communication was present at the shift, unit, and department level. High-performing sites were less likely to cite this type of variation in teamwork and communication. Finally, low-performing sites consistently cited barriers to positive teamwork and communication.
RCC training
Staff members at both high- and low-performing sites were able to discuss in detail the formal and informal training they received. All sites discussed having on-the-job training or coaching from their peers. In addition, all sites mentioned having formal training or classes from either an outside in-service or from the facility. Online trainings were also discussed as a training tool that all sites utilized to educate employees. Finally, all sites reported that they received education on RCC during orientation when starting their employment at the VA CLC.
Staff members at high-performing sites were more likely to report attending training. Only 1 site had staff members from a high-performing site who reported they did not receive training, whereas 5 staff members at low-performing sites reported no training. In addition, staff members at high-performing sites reported attending more formal or national trainings, receiving more education between interdisciplinary staff (ie, huddles, in-services, mini conferences, etc.), having paper materials to refer to, and having the hospital make it a priority (ie, mandatory training through the VA Medical Center (VAMC). Additional training that high-performing sites reported were RCC training (ie, dementia, cultural transformation), mini conferences, facility-wide training, lunch and learn series, RCC conferences, national training, brochures, and a RCC handbook.
On the contrary, staff members at low-performing sites were more likely to obtain RCC training or skill sets from their educational training or prior employment and carried those skills into their current position. Furthermore, low-performing sites were more likely to report online trainings as a method of learning about RCC. Also, 1 low-performing site reported that their medical director only got involved with trainings if there was an issue with funding or if there was a controversy around it. Additional training that low-performing sites mentioned receiving was cultural transformation training, ICARE values, and training or skill sets obtained from prior jobs.
RCC rewards and recognition
There were common themes across all sites on the topic of RCC recognition. All sites made use of one or more awards and recognition mechanisms (eg, employee of the month, Integrity, Commitment, Advocacy, Respect, and Excellence (ICARE) values, Caught-in-the-Act) to acknowledge staff who exemplified RCC while providing care or services to veterans. In addition, the notion that there was not enough staff recognition for RCC was also articulated at most, if not all, sites.
High-performing sites expressed leadership and/or middle management active support or promotion of RCC recognition, with leadership or middle managers initiating staff recognition events or activities (eg, award initiation, boastfulness about the unit, giving out incentives).
RCC recognition at high-performing sites was visibly more formal and consistent in nature, with a wide variety of opportunities taken to recognize staff. Examples for formal recognition range from incentive awards such as star awards, on the spot awards, caught-in-the-act-of-kindness awards, I-saw-what-you-did awards, to employee of the month, shout-outs, recognition during staff meetings, wall postings, bulletin boards, and newsletters.
Low-performing sites reporting on RCC recognition was less frequent with limited visibility, in the form of compliments or positive feedback to staff, performance appraisals, or the reading to staff of veterans letters praising them. Finally, low-performing sites strongly expressed gaps in RCC recognition on multiple levels, from frontline staff to senior leadership. RCC recognition was limited or inexistent and often portrayed as being part of the culture, or expectation, with the acknowledgement that improvements needed to be made to address this issue.
Discussion
In this article, we assessed whether health system factors varied for CLCs with high quality and RCC performance in comparison with low quality and RCC performance. We found that high performers reported more leadership support, better teamwork/communication, better fit with organizational culture, and greater use of training and provided more awards and recognition targeted at improving RCC. Our findings regarding leadership support, teamwork and communication, and organizational culture are supported by previous literature. Efforts are more successful when senior leaders recognize quality and RCC as organizational priorities and promote changes to create practices supportive of quality and RCC, create a learning environment by spreading lessons of successes and failure, and demonstrate commitment by spending time on activities that support RCC and quality.25,35-38 Interdisciplinary teamwork is crucial in the CLC setting for care provision.32-34 Each team member provides a unique perspective on patients’ care needs, and including them in care planning can facilitate improved quality. Communication among team members is critical for patient information to be relayed in a timely fashion to improve care. Training and rewards and recognition are modifiable ways to appreciate staff and improve job satisfaction. 44
To improve CLC performance on both quality and resident-centered care, a site could immediately begin focusing on improving training, policies, and having awards and recognition. Things such as having active leadership support, quality/RCC fit with organizational culture, and good teamwork/communication can take longer to build. Previous work in the private sector provides some actionable guidance for NHs looking to improve performance. As part of Centers for Medicare & Medicaid Services’s (CMS) National Nursing Home Quality Care Collaborative, a change packet was developed. 45 The strategies presented are in line with many of our findings and include 7 strategies:
Lead with a sense of purpose
Recruit and retain quality staff
Connect with residents in a celebration of their lives
Nourish teamwork and communication
Be a continuous learning organization
Provide exceptional compassionate clinical care that treats the whole person
Construct solid business practices that support your purpose
Implementing the change packet resulted in higher levels of quality as measured by a composite measure of quality. 46 We feel that interventions such as this focused on both clinical quality (which also includes tenants of RCC) could help CLCs and private sector nursing homes target ways to focus on the factors that had an influence in our study.
The characteristics which distinguish our study from past research are (1) the focus on both quality and RCC simultaneously and (2) assessing a large number of factors at one time. Much of the literature to date focus on factors affecting either quality or RCC. There is an inherent tension between quality and RCC,47,48 for example, controlling a diabetic resident’s sugar level while also letting that resident choose the foods they eat, which might not always be healthy options. Sites focused only on quality could find it difficult to implement RCC, or vice versa—sites solely focused on RCC may fall behind on quality expectations (eg, falls, weight). In addition, although many of the factors we report on have been identified in individual studies, our results add to the literature because we assessed these organizational factors together in one study.
In terms of implications for practice within the CLC setting, a key insight of this work is that there is no one prescribed strategy to balance resident-centered care with care quality which works for every resident. In addition, the trade-offs between actions that are resident-centered and those that optimize quality metrics can also vary by resident, and thus the approaches to staff training and staff decision making must be more nuanced than adhering to simple guidelines (such as “always make snacks available”). Despite the apparent emphasis RCC places on personalizing care, within a CLC, there were a limited number of ways by which such personalization could be achieved, suggesting that staff would benefit from a deeper understanding of both RCC goals and the variety of strategies to deploy.
Our results may also be of interest to CLCs or private nursing homes trying to implement multiple priorities at once. We find that many of our differentiating factors were ones where organizational supports and resources are necessary, including leadership support, organizational culture, training, and rewards and recognition. The Organizational Transformation Model suggests there are 3 necessary drivers to successful change culture including active leadership, alignment throughout the organization, and implementation of the innovation or new processes. 49 We found there were high-performing CLCs with strong leadership support for RCC in the face of also meeting quality expectations, where organizational cultures were able to be aligned with providing more RCC and where practices for improving RCC and quality could be implemented simultaneously. However, given limited resources, implementation of a new initiative may challenge the systematic, sustained implementation of evidence-based approaches or at least limit the ability to focus on more than one priority at once (as was the case in low performers in this study).
Our study has several strengths. We used secondary quality and RCC data on 130 CLCs to identify sites experiencing high and low levels of both quality and RCC. Not every health system has these types of data over time available to draw from. In addition, being able to study both quality and RCC together provides a unique perspective. Most literature focus on one domain or the other when CLCs are to some extent expected to utilize both models, although utilizing standardize care protocols and resident preferences can sometimes conflict. 48 Although VA’s patient population has more men and patients often have more functional limitations and mental health issues, we feel our results are applicable to the private sector. Community nursing homes are increasingly part of vertically integrated health care systems, and as more hospitals convert to Accountable Care Organizations, more facilities may resemble VA. In addition, the VA has also become more like the community in recent years in that patient acuity has been changing to be more oriented around short-stay acute needs of patients. 50 Although the patient population would result in focusing on different types of RCC interests and activities, provision of RCC tenets as a whole would be very similar (eg, taking account of resident’s preferences and providing residents with a home-like environment).
Our study also has limitations. We were only able to collect data on a small number of sites due to budgetary constraints. However, the sites participating in this study differed in size (based on average patient census) and geographic region, suggesting there was some diversity in the sites we visited. The VA CLCs selected may not be representative of all CLCs. For example, our sites were not implementing the small house or greenhouse model of care. We were unable to use data from the time of site visits because the MDS converted from version 2.0 to version 3.0 between our data pull and site visits and the quality indicators also changed. In our previous work, we have found that MDS version 2.0 data are highly correlated year to year. 51 Given budgetary constraints, we were unable to collect additional types of data (eg, observations, statements of practice) which may have provided more insight into our study question. While it is possible that research bias was present even though site visitors were blinded to both quality and RCC status of a site, we did take measures to remain reflexive and mitigate internal bias (eg, semi-structured interview guides, site visitor impressions). Finally, our analyses were conducted at the site level and tried to incorporate viewpoints from staff at all levels; however, we did not do a specific discipline-by-discipline comparison of viewpoints; because there were not always enough respondents in each category, we see this as an area for future research.
In summary, our findings suggest there are some distinguishing characteristics between site high in quality and RCC and low in quality and RCC. Organizations must recognize this will require dedicated resources from leaders and support from staff throughout the organization. More research is needed on figuring out how to allocate limited resources to most efficiently improve CLC quality given multiple priorities. To fully integrate both quality and RCC, adapting current quantitative measures of quality to incorporate RCC may be necessary. In addition, integrating resident perceptions of the extent to which RCC is present and resident satisfaction may be especially useful for residents and caregivers making decisions about CLC placement. More research is necessary to understand the most practical ways to incorporate these data and if such a measure would distinguish high and low performers.
Supplemental Material
Supplemental_Materials – Supplemental material for Is Variation in Resident-Centered Care and Quality Performance Related to Health System Factors in Veterans Health Administration Nursing Homes?
Supplemental material, Supplemental_Materials for Is Variation in Resident-Centered Care and Quality Performance Related to Health System Factors in Veterans Health Administration Nursing Homes? by Jennifer L. Sullivan, Ryann L. Engle, Denise Tyler, Melissa K. Afable, Katelyn Gormley, Michael Shwartz, Omonyêlé Adjognon and Victoria A. Parker in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to thank the project staff who assisted on the study, including Jim Burgess, Kelly Stolzmann, and Emily Rose Lopez. We thank our VA CHOIR colleagues for reviewing manuscripts and providing feedback (Amy Rosen, Qi Chen, Hillary Mull, Barbara Lerner, Christopher Miller, Bo Kim, Judy George. and Nathalie McIntosh). The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the U.S. Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Veterans Health Administration HSR&D IIR 11-356 (Sullivan, PI).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.