
Abstract
Medical tourism organizations have increasingly recognized that loyalty makes a medical clinic a marketing success. To increase understanding of the importance of medical clinics, this study examined the roles of servicescapes, emotions, and satisfaction in the development of customer loyalty toward medical clinics and destination. Data were collected among international medical tourists visiting Korea. Results identified that dimensions of medical clinics’ servicescape (ie, medical clinic environment, medical treatment, staff, and doctor) influenced emotions and satisfaction among international medical tourists. Also, positive emotions and the 2 dimensions of satisfaction with a medical clinic and doctor mediate the influence of medical clinics’ servicescapes on 2 types of loyalty (the medical clinic and Korea for medical care). Overall, these findings indicate that the interrelationship of servicescapes, positive emotion, and satisfaction is essential in influencing international medical tourists’ loyalty to a medical clinic.
Keywords
Introduction
Medical care–centered businesses and medical tourism have been considered one of the most profitable areas of the tourism industry, including travel, airlines, lodging, and foodservice, among others. 1 Due to collaboration among areas such as travel, medicine, airlines, lodging, and foodservice, the global medical tourism industry attained a value of $10.5 billion in 2012, with 17.90% annual growth according to “Medical Tourism Market—Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2013—2019.” Medical tourists can conveniently and quickly receive higher quality medical care and services at more affordable prices than they can in their native country (eg, $62 000 in the United States vs $7000 in Thailand for spinal fusion). 2 Due to the excessively competitive market situation, medical tourism administrators have not only attracted new medical tourists via various marketing activities, but they have also motivated medical tourists to repeatedly purchase a medical tourism product through service strategies and efforts. 3 Interestingly, the cost of attracting new customers is more than 5 times the cost of keeping existing customers in the medical tourism context. 1 This is because unlike tourists in other contexts, medical tourists pay a medical clinic for long-term, ongoing treatment and care. For example, the “2015 Medical Tourism Association Medical Tourism Patient Survey” indicates that medical tourists are spending between $3600 and $7600 on medical care or treatments per medical travel trip. 4 Therefore, identifying the vital factors of repurchase decision making processes among medical tourists is necessary for both medical clinics and other tourism industries in a country.
From a theoretical perspective, previous studies1,5,6 have regarded higher service and product quality, trust, and satisfaction as key drivers of predicting medical tourist postpurchase behavior. However, they focus more on the medical service quality (medical and care services, major and minor surgeries, and aesthetic and psychological therapies) than a medical clinic’s personnel (eg, doctors and nurses) or facility (eg, cleanliness, lighting, and layout) when examining a clinic’s success in the medical tourism context.1,6 Due to recent advances in medical technology and a paradigm shift in the medical industry emphasizing the patient as customer, 7 most medical organizations have already provided a comparable quality of medical products to tourists. Therefore, medical organizations’ competitiveness is determined by the quality of their services. Based on the limitations of the existing literature as well as the growth trend of medical tourism, this study investigates the importance of a “medical clinic’s servicescape,” where benefits are generated and consumed, by extending environmental psychology theory. 8 Servicescape, according to the theory, 9 is the environment in which the service is produced and where sellers and consumers interact, integrated with tangible commodities facilitating communication or performance of the service, and which impacts the emotional responses they experience in the particular environment. 8 Eventually, these emotional responses drive postpurchase behavior among customers. 8 Based on the theory, previous studies10-12 have considered servicescape, emotion, and satisfaction as key antecedents of visitor loyalty. Considering the interrelationship of these determinants, every enterprise in the tourism industry has become even more interested in effectively managing and reinforcing the servicescapes, emotions, and satisfaction of visitors. 11
Medical tourism is a form of tourism that provides good facilities and physical conditions to a tourist seeking not only treatments for his or her illness or dental/cosmetic needs or enhancements, but also an enjoyable space and pleasurable service in which to recover his or her well-being. 13 Based on the optimistic expectations of medical tourism, prior research has focused on the role of a medical clinic and its impacts on a tourist’s psychological states, satisfaction, and behavioral intention.13-15 While the existing literature has investigated the influence of servicescapes’ dimensions on tourists’ perceptions, attitudes, and behavioral intention,10-12 to date, few studies have been conducted identifying the components of the servicescapes of medical clinics. The current study is designed to close the research gap. In particular, the purpose of this research is to (1) identify the medical clinic’s servicescape components through a comprehensive literature review and empirical testing process, (2) examine interrelationships among the medical clinic’s servicescapes, positive and negative emotions, satisfaction, and loyalty toward the medical clinic and country of the medical care; (3) empirically verify a theoretical model based on environmental psychology theory; and (4) test the mediating roles of emotions and satisfaction dimensions.
Review of Related Literature
The Concept of Medical Tourism and Korean Medical Tourism
Medical tourism is defined as the act of traveling overseas for medical treatment and care. 6 Medical tourism has been considered to be a niche product encompassing both tourism packages and medical services. 16 Hence, the link between the tourism and health care industries has enabled medical tourism to emerge as one of the most beneficial areas of tourism for many countries. 1 Due to its significant monetary benefits, the medical tourism industry is rapidly expanding, with an annual growth rate of 17.90%. 17 An increasing number of global medical clinics have improved their services and amenities to maintain greater market share in the competitive medical tourism sector. 18 The medical facilities commonly provide not only a first-class range of services but also high quality of medical care to their international customers. Thus, medical tourists can conveniently receive medical care and service during travel at a higher quality and at a lower price in a host country than in their native countries. 6 In particular, service-oriented medical clinics, which are a combination of health care/aesthetic center, hospital, restaurant, and accommodation,19,20 have worked to resolve possible inconveniences or difficulties (eg, unkind staff, uncomfortable atmospherics, language barriers, low-quality services and medical care, and inefficient communication)21,22 that were once frequently encountered by international patient travelers.
Asia has several major medical tourism countries, including South Korea, the Philippines, Malaysia, India, Jordan, Singapore, the United Arab Emirates, and Thailand, which has resulted in much competition in the medical tourism sector. 6 The contributing factors to medical tourism in Asian countries are lack of waiting time, low costs, and developments in Internet services and information technology. 23 More specifically, South Korea, which is a new medical tourist destination, had approximately 300 000 foreign patients in 2014, showing an increase of 34.7% annually. 24 South Korea has made efforts to minimize the aforementioned inconveniences and difficulties by enhancing the quality (and therefore success rate) of medical services and care by offering innovative medical facilities (eg, a 98.1% survival rate for thyroid cancer and a 95% liver transplant success rate), 25 a lower nurse-patient ratio, various medical care products (eg, organic aromatherapy, a traditional Korean medicine program, and obesity and diet package options), 24 and more capable medical professionals and high service performance (eg, hotel-style service training for employees, bilingual staffs for more efficient communication). In addition, the government has issued medical visas to international tourists to attract more foreign patients. 26 As a result, many clinics in Korea have attracted numerous international medical tourists primarily from Japan as well as China.19,27 The medical clinics, acting as service providers, have helped medical tourists to have pleasant experiences and have consistently attracted greater numbers of international medical tourists, who arrive at Korean medical clinics for medical health care/aesthetic/treatment services. 19
The Medical Clinic’s Servicescapes
Environmental psychology theory is based on the notion that environmental cues act as a catalyst affecting customers’ negative or positive emotions toward an environment, which, as a result, lead to their postpurchase behavior. 10 The concept of environmental cues is based on the service platform’s physical environment in which a service transaction occurs. 28 The meaning of environmental cues is defined as the general atmosphere or characteristics which can impact consumer support or patronage. 29 Because environments offer a variety of service/product benefits, they can play roles as cues for how a visitor may behave as well as feel. 30 For example, a well-designed buying environment in a store can produce specific emotional responses in a buyer by enhancing his or her purchase probability. 31 For service providers of medical clinics, emotional responses may be more important than in other settings due to their complementary and supportive role in relieving the physical and mental problems of patients. 7 While environmental cues focus more on a store’s atmosphere or ambiance, the servicescape is based on a physical setting where service transactions are performed, experienced, and consumed by a customer and employee. 32
Servicescape is defined as “the environment in which the service is assembled and in which seller and consumer interact, combined with tangible commodities that facilitate performance or communication of the service.”9(p36) By definition, the term “medical clinic servicescapes” addresses the general environment experienced by medical tourists. 33 More specifically, the medical clinic servicescape is defined as a health care service’s specific location with both intangibles and tangibles captured via a customer’s senses of sound, smell, taste, sight, and touch. 31 Thus, servicescapes involve diverse environmental cues, just as in the context of retail and service organizations, and these tangible environmental cues may influence medical tourists’ attitudes and behaviors. 10 While the perception and significance of physical environmental cues may vary through distinct types of service enterprises, 34 a private medical clinic’s servicescape needs to consider particular social elements (eg, staff care, employees’ behavior, and staff welcome) because the empathy and characteristics of employees, as well as the number of employees, can be components of the medical service quality of a medical clinic. 31 Doctors or nurses, for instance, may have a greater influence on medical clinic experiences than restaurant experiences. In a medical clinic context, thus, doctors and staffs as well as promotional material, lighting, layout, color, music, other noise, and even other medical tourists all influence satisfaction, intentions, and behaviors. 35 The existing research on environmental cues has focused on the stimuli regarding servicescapes, 10 physical/service environment, 36 atmosphere, 37 and quality. 38 Because servicescapes have been closely connected with perceptions of particular components in every service interface, the term includes all controllable physical features of a service. 37
Servicescapes have been classified into 3 distinct dimensions for explaining how tangible environments influence consumers 28 : (1) “ambient conditions,” (2) “spatial layout and functionality,” and (3) “signs, symbols, and artifacts.” A medical clinic’s servicescapes, similarly, refer to the specific design of a medical clinic’s physical environmental features perceived by medical tourists, facilities/space, and symbols and signs. 39 From the medical tourist’s perspective, more specifically, the perception of a medical clinic’s servicescape also involves nonvisual or ambiance cues (eg, lighting and sound), design and layout, and the social service atmosphere, encompassing the interactions between service providers (eg, doctors, nurses, and the staff of a medical clinic) and medical tourists. 40
In line with the aforementioned research,1,6,13 this study suggests that new environmental cues for a medical tourism context be divided into physical components (eg, the medical clinic’s cleanliness, layout, interior, and ambience), intangible factors (eg, medical service and care), and social components (eg, doctors and nurses). In particular, the important role of intangible service performance is emphasized when a customer develops behavioral intentions as well as affective and cognitive responses toward a store’s servicescape. 28 To expand the perspective on medical servicescapes, any health care services can be included as part of the servicescape as well. 31 These cues come together to determine how the medical clinic is perceived affectively and functionally by medical tourists in terms of individual experience. Building on the existing literature on servicescapes, environmental cues, and tourism areas, this study explores a medical clinic’s components related to cues influencing a medical tourist’s experience.
Emotions
Emotion has been considered an important determinant in consumer reactions and consumption experience. 10 Emotion plays a mediating role between cognition (eg, perceived disconfirmation and product performance) and other critical outcomes associated with customer loyalty as well as satisfaction. 41 It is arguable that tourists’ emotional status directly influences satisfaction and loyalty intention. 42 Rather than considering consumers as purely rational decision makers, current research has indicated that explanations regarding consumer behavior failing to take emotional states into account are still incomplete. 11 The existing research on the emotional responses of consumers generally employs 2 dimensions to indicate consumption emotion. For example, emotions were measured with a negative emotion dimension (angry, displeased, nullified, anxious, ignored) and a positive emotion dimension (satisfied, proud, contented, excited, attractive, and pleased). 10
In general, environmental psychology theory uses 3 dimensions of emotional responses (ie, arousal, pleasure, and control or dominance), and arousal and pleasure tend to be encompassed in retail environment research. 43 Common measurements were used to indicate arousal (feeling rewarded, surprised, interested, excited, and aroused) and pleasure (content, happy, satisfied, and relaxed). The third dimension of emotional experience is control or dominance (submissive, dominant, important, controlled, or feeling influential). However, many scholars omit the control or dominance dimension when conducting research on consumer emotions because of expectations of low predictive value.10,44
Other scholars in tourism settings have used similar emotion dimensions. For example, 3 emotional dimensions are employed to assess visitors’ emotions toward the 2002 World Cup. 45 The 3 dimensions of emotion capture negative or positive emotion: nasty-nice, unpleasant-pleasant, bad-good. They found that negative and positive emotions significantly influenced visitors’ satisfaction and positive word-of-mouth intention. Most studies in tourism areas employ negative and positive emotional responses to investigate the emotions of tourists in some way. To keep with prior studies, therefore, the medical clinic’s servicescape atmosphere will be captured employing an emotional inventory with 2 emotional dimensions: negative and positive emotions.
Satisfaction and Loyalty
Satisfaction and loyalty are necessary concepts to explain consumer psychology in terms of leisure, hospitality, and tourism, which ultimately lead to tourist destinations’ success.11,46 Loyalty is defined as “a deeply held commitment to rebuy or repatronize a preferred product or service consistently in the future.”47(p34) Satisfaction comes when the experiences of one party achieve the expectations or goals of the other. 47 In this regard, tourist satisfaction toward a destination is retrieved from a tourist’s “cognitive-affective judgments” related to the tourism experience.11(p730)
In many regards, if satisfaction is an outcome of past experience, then loyalty is the desired consequence of the future.11,48 Loyalty is the focal point of tourist experiences, enabling destination marketers to achieve optimum performance across the entire experience of a destination. 48 In general, a satisfied tourist is considered loyal, and loyalty is viewed as a key consequence of satisfaction.10,11,49 Loyal tourists tend to have favorable attitudes and the intention to revisit.1,48 Therefore, it is pivotal for destination marketers to pay attention to the influences that increase tourist satisfaction and loyalty. 11
Hypotheses
Understanding emotional states is crucial when determining tourist behavior as tourism has experiential components and ambiguity. 50 Therefore, a person’s emotional response has received much attention in the tourism literature based on appraisal theory developed by Lazarus in 1991.50-52 According to the theory, a tourist’s emotional state is impacted by his or her interpretations and evaluations of a tour. 52 The cognitive appraisal of the participant-tour situation determines his or her emotional state. 51 In the context of a medical tour package, tourists’ evaluation of and beliefs about a tour package can influence their emotional state. 50 Following appraisal theory, this study sees environmental perceptions such as evaluations, emotional responses, satisfaction, and loyalty as outcomes of emotions and satisfaction. The hypotheses for this research are illustrated in the model presented in Figure 1. The medical clinic’s servicescape model, like other environmental psychology models, encompasses positive and negative emotions in a key explanatory role. 10 Positive and negative emotions have been viewed as outcomes of environmental perceptions and determinants of the satisfaction and future intention of tourists. 11 The medical clinic’s servicescape model is logically based on consistent predictions. Negative environmental perceptions should lead to negative emotions and vice versa. If the aroma of an environment is pleasant, for example, negative emotions should be lower and positive emotions should be higher. Thus, we hypothesize as follows:

A proposed model.
Emotion has been shaped in the form of pleasure or excitement. 53 Furthermore, a person’s emotional status directly influences perceived satisfaction. 10 It was found that World Cup participants’ emotions affected their satisfaction with the World Cup. 45 Similarly, festival participants’ positive and negative emotions had a significant impact on their satisfaction. 10 According to an expectation and disconfirmation approach, the more positive the emotional response while visiting a destination, the higher the level of satisfaction with the destination. 50 Medical tourists’ positive emotions toward medical clinics fulfill their needs, thereby driving satisfaction with the medical clinic and doctor, and vice versa. Hence, the hypotheses are developed as follows:
Positive emotions influence a tourist’s desire to remain in a destination and associate with other tourists. Emotional states are related to the number of activities, amount of time and money spent in a destination, and whether the tourist liked the environment of the destination.10,11,44 In-destination emotions affect attitude toward the destination, current and future behavioral intentions, 10 and destination loyalty. 11 Thus, this study hypothesizes that positive emotion increases a medical tourist’s desire to be affiliated with the medical clinic and Korea for medical care by continuous loyalty and vice versa. Thus, hypothesize as follows:
Loyalty in the tourism literature includes tourists’ willingness to recommend to others and revisit intention. 11 For example, loyalty was measured with positive word-of-mouth endorsement and revisit intention. 54 To assess the influences of service evaluation factors (eg, satisfaction, equity, value, and quality) on behavioral intentions among travelers, previous research established a research model and found that satisfaction positively influences word-of-mouth referrals and intention to revisit. 55 In this study, loyalty includes the extent to which medical tourists to a medical clinic are satisfied with the medical clinic and its doctor, have a desire to revisit, and articulate to others positive things about the medical clinic and Korea. Thus, the following hypotheses are proposed:
Methodology
Sample and Data Collection
The data were collected from medical tourists through a convenience-sampling method. From a list of regional medical tourism clinics from visitmedicalkorea.com, the authors contacted 25 medical clinics located in Seoul, Korea, that served a significant number of international medical tourists and obtained permission to collect data at 10 of the contacted medical clinics for the field survey approach. Visit Medical Korea provides various medical tour packages from mild to specialized, such as plastic surgery/aesthetic, medical examinations, Korean traditional medicine, and wellness. A plethora of attractions are available near the medical clinics, and international health care/medical tourists account for most of their customers. Because Chinese or Japanese medical tourists account for most of the international customers, the authors developed and prepared 2 different versions of the questionnaire. To minimize translation errors, the authors used a blind translation-back-translation approach, which is the most frequently employed method due to its accuracy as well as consistency. 1 Japanese- and Chinese-speaking tourism institutions reviewed and improved the Chinese and Japanese versions of the translated questionnaires 2 times. For randomization, the questionnaires were distributed to every third international health care/medical tourist at the main entrance lobbies of 10 medical clinics by well-trained graduate students. To ensure the participants had had an experience relevant to this study, the graduate students asked only actual medical tourists who had utilized the medical health care/aesthetic/treatment services of the medical clinics by offering a detailed depiction of the questionnaire to the participants. A Korean souvenir was offered to the respondents as a reward after checking for completeness (ie, a Korean tradition flat bookmark). A total of 390 questionnaires were returned, and finally, 337 responses were deemed fit for data analysis after excluding unusable responses and outliers.
Measures
All constructs were measured with multiple items developed in previous research and then tested and scored on a 5-point scale, ranging from “1 = strongly disagree” to “5 = strongly agree.” Medical clinics’ servicescapes are multifaceted. Preliminary survey items were generated from the related literature review pertaining to environmental cues, medical hotels, medical services, and the medical tourism industry.39,56-60 In addition, the authors conducted preliminary open-ended interviews with medical staff (doctors and nurses) as well as medical tourists to identify servicescapes essential in the medical clinic based on the most prominently mentioned cues. The process derived 35 measurement items. Emotion was classified into 2 subdimensions based on Mehrabian and Russell’s Pleasure-Arousal-Dominance (PAD) framework: positive (energetic, excited, satisfied, and pleased) and negative (angry, annoyed, sleepy, and bored). 61 Satisfaction was divided into satisfaction with the medical clinic and satisfaction with the doctor. We developed a measure for 2 satisfactions on the basis of Oliver and Swan’s study. 62 Loyalty was classified into loyalty toward the medical clinic and loyalty toward Korea for medical care. Each subdimension of loyalty was measured using 3 items adopted from Han’s study. 17
Empirical Results
Profile of Respondents
The characteristics of the respondents used in the analysis are demonstrated in Table 1. The nationalities were comprised of 80.4% Chinese and 19.6% Japanese. Males accounted for 32.0% of respondents, while females accounted for 68.0%. The age group breakdown is as follows: 25.2% were in their twenties, 43.9% in their thirties, 16.3% in their forties, and 14.5% were fifty or older. Monthly household incomes were, from most frequent to least frequent, less than $3000 (34.7%), $3000 to $4000 (22.6%), $4001 to $5000 (13.9%), more than $7001 (13.9%), $5001 to $6000 (9.8%), and $5001 to $6000 (9.8%). In terms of education, holders of 2- or 4-year college degrees were the most numerous (50.1%), followed by high school graduates (34.7%) and holders of postgraduate degrees (15.2%). Regarding prior visits to Korea, the survey showed that much more than half of the respondents had visited the country before (84.8%).
Demographic Characteristics of Respondents.

Measurement Reliability and Validity
Exploratory factor analysis (EFA) was performed prior to further analysis. First, using the varimax procedure, the original principal components analysis solution was rotated. Seven factors were identified based on eigenvalues greater than 1. Six of 31 items were eliminated due to low factor loadings (less than .4). As presented in Table 2, 4 underlying dimensions of medical clinics’ servicescapes were derived from the factor analysis: atmosphere, medical activity, nurse, and doctor. Bartlett’s test of sphericity with a value of 5798.917 (P < .001) and Kaiser-Meyer-Olkin statistics of .904 indicate that the data seemed suitable to identify factor dimensions. Most of the reliability coefficients for the data exceeded the .70 minimum standard for reliability. 63 The 4 factors also explained 64.418% of the variance of the sample data.
Results of Exploratory Factor Analysis for the Medical Clinic’s Servicescapes.

Note. Kaiser-Meyer-Olkin (KMO) = .904, Bartlett’s test of sphericity = 5798.917 (df = 300), P < .001.
Second, the remaining items were subjected to confirmatory factor analysis (CFA) for validity testing. 64 Five items, which had factor loadings lower than .50, were removed for further analyses to maintain an acceptable level of convergent and discriminant validity of the medical clinics’ servicescape measures. After the purification process, all standardized factor loadings exceeded .50 (P < .01), signifying evidence of convergent validity. As shown in Table 3, the CFA results also suggest good fits: χ² = 498.616 (df = 164, P < .001), comparative fit index (CFI) = .921, Tucker-Lewis index (TLI) = .908, incremental fit index (IFI) = .921, root mean square error of approximation (RMSEA) = .078.
Results of CFA for the Medical Clinic’s Servicescapes.

Note. χ2= 498.616, df = 164 (χ2 / df = 3.040), P < .001, CFI = .921, TLI = .908, IFI = .921, RMSEA = .078. CFA = confirmatory factor analysis; CFI = comparative fit index; TLI = Tucker-Lewis index; IFI = incremental fit index; RMSEA = root mean square error of approximation.
Items were deleted during confirmatory factor analysis.
Items were fixed at 1.0 during confirmatory factor analysis.
Third, a chi-square difference test was also performed to further check for evidence of discriminant validity of the measures of the medical clinic’s servicescapes using CFA (see Table 4). The test examines whether or not the model constraining the measures is significantly different from the unconstrained model. If the chi-square differences are significant, the evidence of discriminant validity is indicated. 65 The test results supported the evidence of discriminant validity among the constructs at the level of P < .01.
Chi-Square Difference Test for Discriminant Validity of the Medical Clinic’s Servicescapes.

P < .05. **P < .01.
Next, the other items for emotion, satisfaction, and loyalty used in the survey were subject to reliability and validity analyses. Reliabilities were assessed using Cronbach’s alpha coefficients, which ranged from .817 to .963. The endogenous variables were then subject to CFA for validity testing 64 using AMOS 20.0. Four items, which had factor loadings lower than .50, were dropped from further analyses to maintain an acceptable level of convergent and discriminant validity. As shown in Table 5, the CFA results suggest good fits: χ² = 330.306, df = 138, P < .001, CFI = .964, TLI = .956, IFI = .965, RMSEA = .064. 66 After the purification process, all standardized factor loadings exceeded .50 (P < .01), signifying evidence of convergent validity.
Results of CFA for Endogenous Variables.
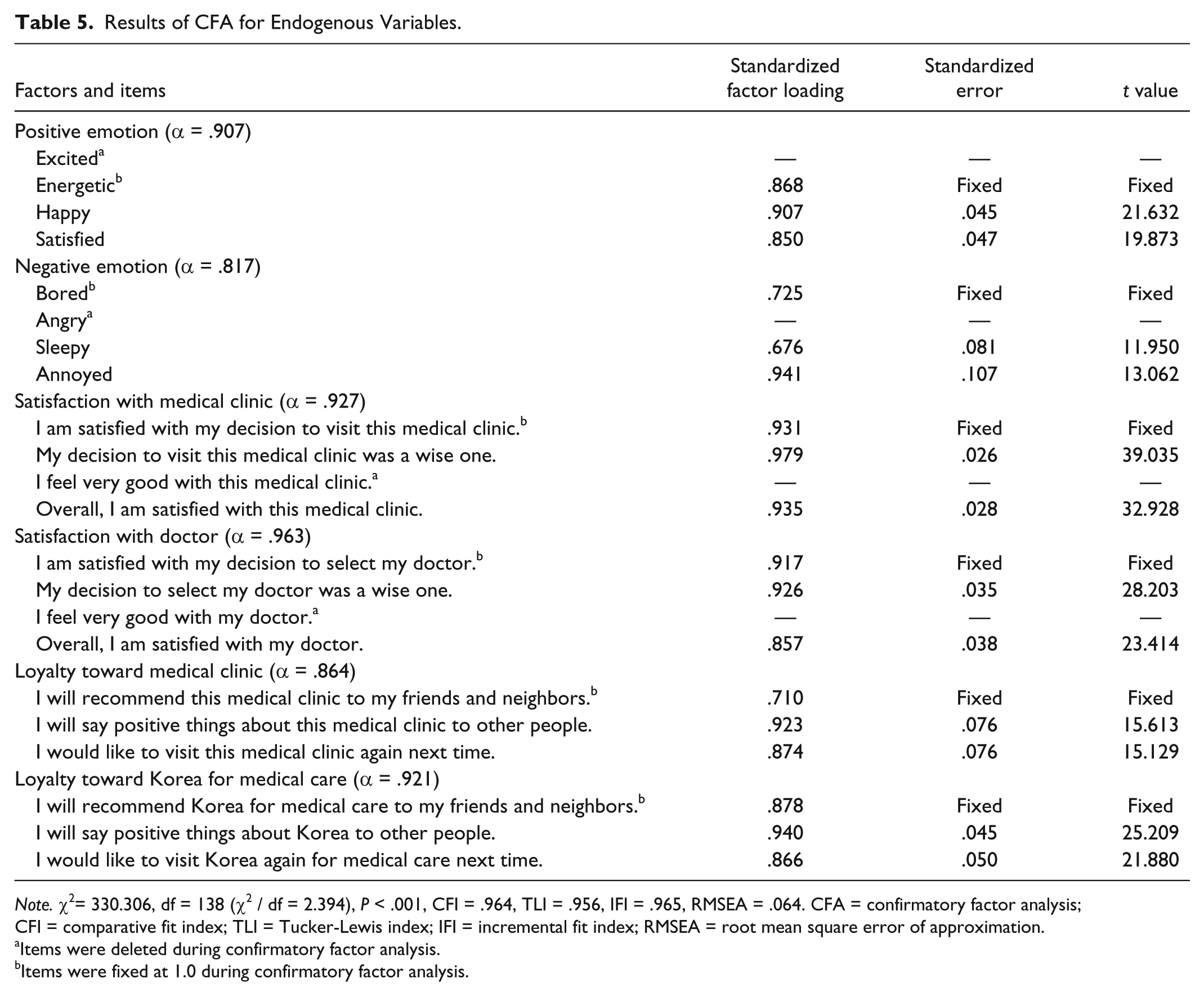
Note. χ2= 330.306, df = 138 (χ2 / df = 2.394), P < .001, CFI = .964, TLI = .956, IFI = .965, RMSEA = .064. CFA = confirmatory factor analysis; CFI = comparative fit index; TLI = Tucker-Lewis index; IFI = incremental fit index; RMSEA = root mean square error of approximation.
Items were deleted during confirmatory factor analysis.
Items were fixed at 1.0 during confirmatory factor analysis.
Discriminant validity was checked by comparing the proportion of variance extracted (AVE). All AVE estimates were greater than their corresponding interfactor squared correlations, 67 indicating good discriminant validity between any 2 factors (see Table 6). The construct reliability (CCR) was also greater than .60 among all variables. 68 Multiple items to measure the medical clinics’ servicescapes, tourists’ positive and negative emotions, tourists’ satisfaction with the medical clinic and doctor, and tourists’ loyalty toward medical care and Korea for medical care were randomly split into 2 groups (separately for each variable) to represent 2 indicators of each construct.10,44,69
Construct Intercorrelations (Φ), Mean, SD, CCR, and AVE.

Note. 1. Atmosphere; 2. Medical activity; 3. Nurse; 4. Doctor; 5. Positive emotion; 6. Negative emotion; 7. Satisfaction with medical clinic; 8. Satisfaction with doctor; 9. Loyalty toward medical clinic; 10. Loyalty toward Korea for medical care. CCR = composite construct reliability; AVE = average variance extracted.
P < .05. **P < .01.
Structural Model
The data were analyzed with AMOS 20.0. maximum-likelihood estimates for the various parameters of the model are given in Figure 2 and Table 7. The chi-square statistic was significant (χ2= 171.943, df = 133, P < .05), as would be expected for a model of this complexity with this sample size. The overall evaluation of fit was completed using a separate incremental goodness of fit index and a separate badness of fit index 66 : CFI = .993 and RMSEA = .030 (see Table 6). Thus, the model fit is adequate for further analysis. The squared multiple correlations (SMCs; R2) for the structural equations for positive emotion (SMC = .421), satisfaction with the medical clinic (SMC = .563) and doctor (SMC = .498), and loyalty toward the medical clinic (SMC = .643) and Korea for medical care (SMC = .588) were found to be high (see Table 7). However, the variance for negative emotion (SMC = .135) explained by the medical clinics’ servicescapes was not enough to be high.

Estimates of structural model.
Standardized Structural Estimates.

Note. χ² = 171.943, df = 133, P < .05, GFI = .953, AGFI = .926, CFI = .993, NFI = .970, RMSEA = .030. SMC = squared multiple correlation; CFI = comparative fit index; RMSEA = root mean square error of approximation; GFI = goodness of fit index; AGFI = adjusted goodness of fit index; NFI = normed fit index.
P < .05. **P < .01.
Hypothesis Testing
Relation of atmosphere to positive and negative emotion, and satisfaction with medical clinic and doctor
Hypotheses 1 to 4 stated that a medical clinic’s servicescapes would affect emotion and satisfaction. As shown in Table 7, the atmosphere dimension had a significant effect on positive emotion (coefficient = .425, t value = 5.233, P < .01), while it did not have a significant influence on negative emotion (coefficient = −.123, t value = −1.368, ns), satisfaction with the medical clinic (coefficient = −.023, t value = −0.329, ns), or satisfaction with the doctor (coefficient = −.010, t value = −0.135, ns). We concluded, therefore, that Hypothesis 1a was supported.
Relation of medical activity to positive and negative emotion, and satisfaction with medical clinic and doctor
The set of Hypotheses 1b to 4b addressed perceptions of medical activity. The medical activity dimension had a significant effect on satisfaction with the medical clinic (coefficient = .184, t value = 2.771, P < .01), while it did not have a significant influence on positive emotion (coefficient = .010, t value = 0.126, ns), negative emotion (coefficient = −.002, t value = −0.017, ns), or satisfaction with the doctor (coefficient = .057, t value = 0.816, ns). Thus, Hypothesis 1c was supported.
Relation of nurse to positive and negative emotion, and satisfaction with the medical clinic and doctor
The set of Hypotheses 1c to 4c posited that the nurse dimension of a medical clinic’s servicescapes is related to emotion and satisfaction. The nurse dimension had significant influences on positive emotion (coefficient = .179, t value = 2.704, P < .01) and negative emotion (coefficient = −.183, t value = −2.360, P < .05), whereas it did not significantly affect satisfaction with the medical clinic (coefficient = .062, t value = 1.115, ns) or satisfaction with the doctor (coefficient = −.112, t value = −1.900, ns). Thus, Hypotheses 1c and 2c were supported.
Relation of doctor to positive and negative emotion, and satisfaction with medical clinic and doctor
Hypotheses 1d to 4d predicted that the doctor dimension would be associated with emotion and satisfaction. As hypothesized, the doctor dimension had significant effects on positive emotion (coefficient = .182, t value = 2.898, P < .01), negative emotion (coefficient = −.154, t value = −2.103, P < .05), satisfaction with the medical clinic (coefficient = .281, t value = 5.217, P < .01), and satisfaction with the doctor (coefficient = .575, t value = 9.696, P < .01), thus supporting Hypotheses 1d, 2d, 3d, and 4d.
Relation of positive and negative emotion to satisfaction with medical clinic and doctor
Hypotheses 5 to 8 addressed the causal relationship between emotion and satisfaction. Positive emotion had positive effects on satisfaction the medical clinic (coefficient = .386, t value = 5.933, P < .01) and satisfaction with the doctor (coefficient = .258, t value = 3.836, P < .01), while negative emotion had a statistically insignificant effect on satisfaction with the medical clinic (coefficient = −.087, t value = −1.759, ns) and satisfaction with the doctor (coefficient = −.018, t value = −0.348, ns). Therefore, Hypotheses 5 and 6 were supported.
Relation of positive and negative emotion to loyalty toward the medical clinic and Korea for medical care
Hypotheses 9 to 12 predicted that emotion would be associated with loyalty. However, positive emotion did not have a significant influence on loyalty toward the medical clinic (coefficient = .079, t value = 1.337, ns) or loyalty toward Korea for medical care (coefficient = .098, t value = 1.594, ns). Also, negative emotion did not have a significant effect on loyalty toward the medical clinic (coefficient = −.020, t value = −0.418, ns) or loyalty toward Korea for medical care (coefficient = .072, t value = 1.446, ns). Therefore, Hypotheses 9, 10, 11, and 12 were not supported.
Relation of satisfaction to loyalty
Hypotheses 13 to 16 stated that 2 dimensions of satisfaction are positively associated with 2 types of loyalty. As hypothesized, satisfaction with the medical clinic significantly affected both loyalty toward the medical clinic (coefficient = .639, t value = 7.527, P < .01) and loyalty toward Korea for medical care (coefficient = .175, t value = 2.061, P < .05). Satisfaction with the doctor also significantly influenced loyalty toward Korea for medical care (coefficient = .586, t value = 8.132, P < .01). However, the dimension did not have a significant effect on loyalty toward the medical clinic (coefficient = .124, t value = 1.813, ns), so Hypotheses 13, 14, and 16 were supported.
Mediating effects
The mediating roles of emotion and satisfaction on the relationship between a medical clinic’s servicescapes and loyalty were investigated with the bias-corrected (BC) bootstrapping method and Monte Carlo method to compute their confidence intervals (CIs; see Table 8). 70 It is suggested that, compared with other mediation analysis methods (eg, the Sobel test), these methods of mediation analysis are more suitable for a 2-path indirect effect in structural equation modeling. 71 Thus, these methods enable scholars to test the level of significance of the indirect influence of the independent variable on the dependent variable via multiple mediators. 70 Table 8 shows that atmosphere had significant indirect effects on loyalty toward the medical clinic (coefficient = 0.145, P < .05; 95% bootstrap CI = .026LL, CI = .266UL) and loyalty toward Korea for medical care (coefficient = .119, P < .05; 95% bootstrap CI = .003LL, CI = .233UL) via positive emotion and satisfaction. Medical activity had a significant influence on loyalty toward the medical clinic via satisfaction (coefficient = .128, P < .05; 95% bootstrap CI = .028LL, CI = .251UL). Nurse had a significant impact on loyalty toward the medical clinic via positive emotion and satisfaction (coefficient = .104, P < .05; 95% bootstrap CI = .009LL, CI = .197UL). Finally, doctor had significant effects on loyalty toward the medical clinic (coefficient = .328, P < .01; 95% bootstrap CI = .221LL, CI = .418UL) and loyalty toward Korea for medical care (coefficient = .437, P < .01; 95% bootstrap CI = .336LL, CI = .522UL) via positive emotion and satisfaction.
Results of Mediating Role Estimation of Emotion and Satisfaction.

Note. CI = confidence interval; LL = lower limit; UL = upper limit.
P < .05. **P < .01.
Discussion
Theoretical Contributions
This research applies the environmental psychology theory to the tourism context. In particular, this theory especially helps to understand how a medical clinic’s servicescapes influence emotional responses and satisfaction among medical tourists. The medical tourism industry heavily relies on medical establishments that provide expertise/medical tourism products, such as medicine, treatment, and cosmetic surgery. 23 The success of the medical tourism industry is not achievable without the successful operation and business model of medical establishments at the micro level. Also, the success of medical clinics is not attainable without the supportive policies or attitudes of a government with macro-level insight. From the micro-level perspective, the current study is the first to identify multiple dimensions of medical clinics’ servicescapes and test a research model that accounts for their effects on emotional responses (positive and negative), satisfaction with the medical clinic and doctor, and loyalty toward the medical clinic and Korea for medical care. There are 2 reasons to support this context. First, medical clinics experience strong external pressure from the government through restrictions, policies, rules, and formalities related to medical cares or treatments. 23 Thus, medical clinics have invested in internal resources 1 such as the quality of medical products (ie, medical care, surgery, health care products, medical facilities) and service (ie, efficient/comfortable communication, service delivery skills and competencies, and kindness). If a medical clinic chooses to ignore the importance of these internal resources, then this negligence may result in fewer medical tourists and an increase in medical tourists’ intention to switch to other medical clinics, which, in turn, will threaten the medical clinic’s survival. Second, even though some scholars have focused on the medical tourism industry, much research is centered on perceptions of the medical clinic’s country or destination.23,26,72 Also, previous research has been conducted on the perceived quality of “overall” medical service among medical tourists.1,73 However, general tourists appreciate not only a destination’s service, but also the ambiance, environment, or atmosphere of the destination that aroused their satisfaction and positive emotion. 11 Hence, both physical surroundings and the medical service providers of a medical clinic need to be maintained for it to remain popular with medical tourists. The servicescape in the tourism area has been consistently reported as a multidimensional construct (program, structure, layout, and ambiance 11 and convenience, staff, information, program content, facility, souvenirs, and food 10 ). A principal components analysis in this study revealed the existence of 4 distinct dimensions of the medical clinic’s servicescape in the Korean tourism context, which means that these 4 dimensions of servicescape need to be separately measured and investigated. Thus, more research on the new perspective of the medical clinic’s servicescape with a basis in the medical tourism industry needs to be done. Recognition of the importance of servicescapes enables scholars to develop more sophisticated theoretical models for the medical tourism industry.
Second, based on the environmental psychology theory, in particular, this study supported a critical role for emotional responses in predicting international medical tourist outcomes, indicating that they judged a medical clinic along 4 servicescapes and that these judgments led to behavioral intentions as well as consequent emotions and attitudes. In addition, unlike previous research,1,73 this study proposed 2 types of satisfaction (ie, satisfaction with the medical clinic and satisfaction with the doctor) and 2 dimensions of loyalty (ie, loyalty toward the medical clinic and loyalty toward Korea for medical care). 1 Prior research in the medical tourism context suggests two aspects of trust, such as trust in the staff and medical clinic, by demonstrating that medical tourists have 2 perceptions: (1) staff behavior/performances in a service encounter situation and (2) company performance including its practice and policies. Loyalty is one of the most important goals both from a destination’s and medical clinic’s perspective, and the ability to apply knowledge is a significant starting point in developing and sustaining the long-term competitiveness of the medical clinic as well as the destination. Thus, it is critical that the distinct influences of these 2 aspects of satisfaction and 2 dimensions of loyalty be investigated using conceptual approaches.
Managerial and Marketing Contributions
From a practical standpoint, as the tourism industry has generated foreign exchange earnings and contributed to the industrial development of many countries, medical tourism has also been spotlighted with regard to obtaining a better understanding of a target tourist. 73 The findings of this research may be helpful to those countries whose governments have found a strategy to attract more international medical tourists. As the findings indicated, international medical tourists tend to be dependent on cognitive evaluations of the medical clinic’s servicescape when they decide on a medical tour to Korea. In general, general international tourists are likely to employ both affective and cognitive judgments about a potential country when they make a decision about vacation travel. However, international medical tourists choose a destination and medical clinic at the cognitive level based on their evaluation of the medical clinic’s servicescapes. In this regard, medical clinic administrators need to help medical tourists draw a clear picture of the medical clinic at a cognitive level. The cognitive servicescapes in this study can be a medical clinic’s atmosphere (eg, cleanliness, lighting, overall color, mood, fragrance, or temperature), medical activity (eg, medical treatment, time in the diagnostic process, or consultant hour), or staff (employee kindness, professionalism, explanations about the examination or surgery, and plan of treatment of the nurse and/or doctor). The distinct dimensions of a medical clinic’s servicescapes indicate that medical clinic administrators need to be monitored for the variety and quality of medical treatments and environments as well as the human resources of their medical clinic.
The results illustrated the important roles of a medical clinic’s service providers, that is, the nurses and doctors. Although Korean medical clinics have a large number of English-speaking nurses and doctors, it is important that the staff has a good level of communication with their international patients across the entire treatment and recuperation process. It is important to note that communicating in English may still create a language barrier with Chinese and Japanese medical tourists. Thus, it is more beneficial to employ staff members fluent in Chinese or Japanese. Another finding demonstrated that medical activity could determine satisfaction with the medical clinic, which in turn influences loyalty toward the medical clinic and Korea for medical care. Based on cost and success rates, Korea should be considered the smartest choice in the medical tourism industry. This suggests that the combination of modern medicine and traditional Asian medicine needs to be promoted as a distinct medical activity or treatment for Chinese and Japanese medical tourists. Also, the atmosphere of a medical clinic needs to be established specifically for international medical tourists in order to provide them an efficient and comfortable environment. To do so, medical clinic administrators may need to consider any ethnic, religious, and cultural differences between Korea and other target countries (eg, dietary preferences, prayer rooms, or instructions written in their native language). Most importantly, medical tourist–oriented arrangements need to be designed and implemented to ensure international medical tourists’ privacy and health, which is one of the primary purposes of a medical trip to Korea.
One significant finding involves the role of emotional responses, which directly drive satisfaction and indirectly loyalty among international medical tourists. Both scholars and practitioners need to strive to create a positive experience and avoid negative emotions for medical tourists. Atmosphere, medical activity, nurse, and doctor come together to create medical clinic’s servicescape embodied with particular emotions, thereby leading to desirable outcomes (ie, satisfaction with the medical clinic and doctor, and loyalty toward the medical clinic and Korea for medical care). The fact that negative emotions were not significant drivers of 2 types of loyalty may be explained by the fact that medical tourists visiting medical clinics may have expected some degree of inconvenience and hassle. A future study may need to indicate the frameworks by which medical tourists cope with these negative feelings, thereby decreasing negative reactions to the medical clinic’s servicescape overall.
In the proposed theoretical model, international medical tourists’ emotion and satisfaction were found to have significant mediating roles. Particularly, positive emotion and 2 aspects of satisfaction (ie, with the medical clinic and doctor) significantly mediated the influence of the medical clinic’s servicescapes on 2 types of loyalty (ie, the medical clinic and Korea for medical care). Scholars in the medical tourism arena need to consider the mediating roles of emotions and satisfaction when they establish a theory or model. From a practical standpoint, this suggests that the influence of the medical clinic’s servicescapes on behavioral intentions can be stronger when the mediators are integrated. As the frequent focus of various research on consumer behavior and marketing, effectively dealing with the variables may be the critical driver of successfully retaining customers for the medical clinic as well as the country and destination.
As previously addressed, the capability to effectively communicate is one of the essential characteristics medical tourism professionals must have. They need to be encouraged to understand different cultural backgrounds and learn the native languages of international medical tourists. Additional educational institutions or national qualification schemes need to be established to successfully produce medical tourism professionals. Governments can work to establish and maintain the quality of these institutions.
Limitations
As with all empirical studies, there are several limitations that should be considered for future studies. First, this study tested the research model only in the Korea medical tourism industry. The associative hypotheses this study tested need to be replicated in other contexts or settings to test the generalizability of the empirical results. Second, although this research identified 4 dimensions of medical clinics’ servicescapes, these dimensions were selected from the authors’ subjective perspective. Because various dimensions of servicescapes may be associated with distinct aspects of medical clinics, future research may need to explore how other new dimensions influence outcomes. Third, this study employed self-reported subjective measures (eg, perception of behavioral intention). The measures could have influenced their reliability. Thus, future studies may need to use an objective measure (eg, the actual number of revisits among international medical tourists). Also, longitudinal research on the development of loyalty over time would be useful in identifying any potential changes associated with a particular society and country.
Conclusion
While scholars in the tourism field have pointed out the importance of servicescapes or environmental cues, research is scarce on the role of servicescapes in the tourism industry.10,11,34 To address this shortcoming, this study identified 4 dimensions representing medical clinics’ servicescapes (ie, atmosphere, medical activity, nurse, and doctor) and investigated how these dimensions influence emotion, satisfaction, and, in turn, loyalty in the Korean medical tourism context. Based on the environmental psychology theory in particular, this study supported the critical role of emotion in predicting medical tourist outcomes, indicating that medical tourists judge the medical clinic’s servicescape along 4 medical clinic cues and that these judgments lead to emotional responses, satisfaction, and behavioral intentions. Overall, the results of this study demonstrate that a doctor is the most important driver of emotional responses and satisfaction, which in turn affects medical tourist loyalty. Although the influence is not quite as strong compared with a doctor, a nurse also drives emotional responses (ie, positive and negative feelings). The atmosphere and medical activity dimensions also separately influence positive emotion and satisfaction with a medical clinic among international medical tourists. If medical clinic administrators better understand the roles of servicescapes, their medical clinic can maximize the effects of the dimensions to build a strong relationship with medical tourists. This study extends the existing medical tourism and servicescape literature by studying the relationship among servicescapes, emotions, satisfaction, and loyalty based on the environmental psychology theory. This application in the medical tourism context contributes to the body of knowledge on servicescapes and medical tourism, and confirms the solidity of the theoretical framework.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.