
Abstract
Observation stays are an outpatient service used to diagnose and treat patients for extended periods of time while a decision is made regarding inpatient admission or discharge. Although the use of observation stays is increasing, little is known about which patients are observed and which are admitted for similar periods of time as inpatients. The aim was to identify patient characteristics associated with being observed rather than admitted for a short stay (<48 hours) within the Veterans Health Administration (VHA). In our longitudinal analysis, we used logistic regression within a generalized estimating equation framework to model observation stays as a function of patient characteristics, time trends, and hospital fixed effects. To minimize heterogeneity between groups, we limit our sample to patients with a presenting diagnosis of chest pain. Our analysis includes a total of 121 584 hospital events, which consist of all observation and short-stay admissions for chest pain patients at VHA hospitals between 2005 and 2013. Both the absolute and relative use of observation stays increased markedly over time. The odds of an observation stay were higher among women, but lower among older patients and rural residents. Despite strong evidence that chest pain patients are increasingly more likely to be observed than admitted, suggesting a substitution effect, we find little evidence of within-hospital disparities in VHA observation stay use.
Introduction
Observation stays allow for a period of evaluation and treatment in which to either reach a clinical point for safe discharge or identify a clinical need requiring further inpatient stay. 1 During initial evaluation, the clinical team must balance expected patient needs, clinical course, and financial impacts when deciding whether to admit a patient to observation or inpatient status. With observation stays, the clinical team must determine a disposition in a finite time (less than 24 hours during our study period), whereas inpatient stays may be longer. However, unnecessary inpatient admissions may result in short lengths of stay (less than 48 hours) that could be managed under observation status.
The effects this decision may have on patients makes it important to understand which patients get observed and which get admitted for short stays, particularly as observation stays are being used more frequently in various settings. For example, between 2007 and 2009, the prevalence of observation stays in fee-for-service Medicare increased by 26%. 2 Similarly, the observation stay rate in the Veterans Health Administration (VHA) more than doubled over the last decade. 3 However, it is unclear whether this increase represents a greater tendency to observe patients who would have been discharged, or a substitute for patients who would have been admitted.
Moreover, there is a significant variation in observation stay use across hospitals in both Medicare and VHA populations.2,3 This variation may be driven by differences in the treatment of patients by race, gender, rurality or other specific characteristics, or by differences in hospital-specific factors.2,4-13 In the VHA, a number of hospital-level factors have been identified that partially explain the variation in observation stay rates across VHA hospitals, including bed size and patient case mix. 14 However, to our knowledge, no prior studies have explored how patient-level factors may influence the physician’s decision to place a patient in observation status. To our knowledge, the VHA does not operate dedicated observation units, meaning that for a patient in a given bed, the decision to classify a veteran as an inpatient or place one in observation status is merely a decision made using a code in the electronic health record, with no distinction in the care provided. However, this decision is important because observation stays are an outpatient service, leading to substantially different payments for hospitals and out-of-pocket costs for beneficiaries. Specifically, observation stays subject the veteran to a $50 copayment, whereas inpatient hospitalizations subject the veteran to a $1288 copayment. Thus, the objectives of this study are to (1) identify patient characteristics associated with being observed rather than admitted for a short stay (ie, 48 hours or less) and (2) determine the extent to which observation stays are being used as a substitute for short-stay admissions.
Methods
For this study, we used acute admissions and enrollment data from fiscal years 2005-2013 of the VHA Patient Treatment (Inpatient) files and VHA enrollment files. The inpatient files contain information on dates of service, diagnoses, provider type, and provider location, for all veterans who used VHA hospital services in that year. The enrollment files contain veteran age, race, gender, and dates of enrollment, birth, and death, for all enrolled veterans.
First, we identified all observation stays and short-stay admissions (≤48 hours) in the data. Then, we limited our study sample to individuals who had at least 1 observation stay event or at least 1 short-stay admission with an initial diagnosis of chest pain (to minimize case mix heterogeneity between groups) during a given year. Starting with over 4.4 million acute admission records, we excluded approximately 4.3 million records as shown in Figure 1, leaving 123 976 records during our 9-year study period. We excluded individuals who were identified as short-stay admissions because they died or were transferred within 48 hours, as these stays might have otherwise extended beyond 48 hours. Twelve VHA hospitals were excluded from our model because they had no variation in the outcome, yielding an analytic sample of 121 584.
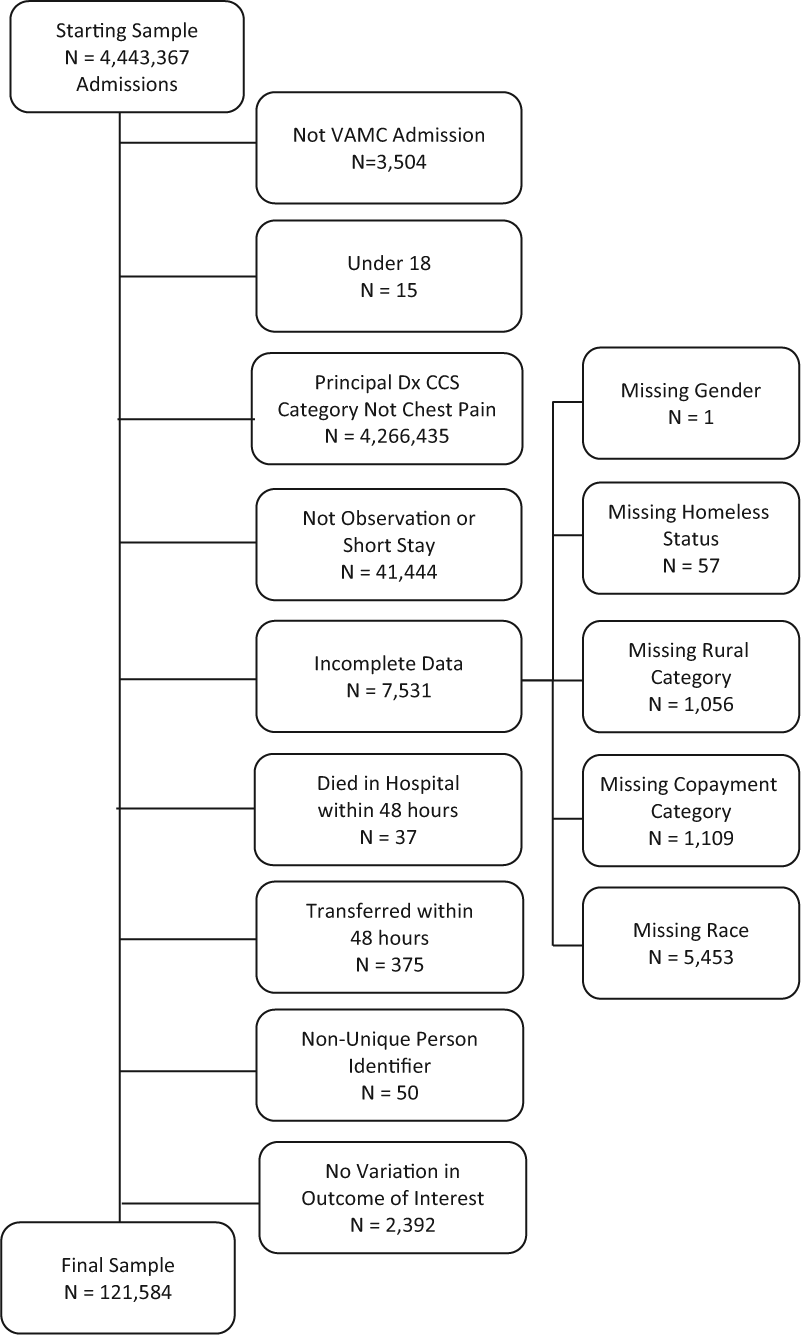
Selection of inpatient admissions sample.
Next, we generated descriptive statistics by fiscal year across 3 groups of veterans: those with observation stays only, those with short-stay admissions only, and those with both observation stay and short-stay admissions in each year. Within each group, we identified unique individuals by their first event in each fiscal year, so that descriptive statistics would not be skewed by high utilizers. We used chi-square tests to detect differences in categorical variables and the Wilcoxon rank-sum tests to detect differences in continuous variables between the 3 groups.
Finally, we used logistic regression within a generalized estimating equation (GEE) framework to model placement in observation as a function of patient characteristics. Our dependent variable was a binary indicator for a hospital visit that was set to 1 if the record was for an observation stay and 0 if the record represented a short-stay admission. As individuals could have multiple hospital events annually, we accounted for correlated data within patients using the GEE method with an exchangeable working correlation structure and robust standard errors clustered at the patient level.
Our key independent variables were patient race/ethnicity and rurality of residence, as we aimed to identify racial, ethnic, and/or geographic disparities in observation stay use within the VHA. We also controlled for other patient characteristics, including age, gender, homelessness, copayment status (based on a veteran’s income and service connected disability), and the number of comorbid conditions a person had within 1 year of admission, based on International Classification of Diseases, Ninth Revision, Clinical Modification algorithms originally developed by Charlson and updated by Quan and colleagues. 15 To detect time trends in observation stay use, we included a series of year dummy variables. Finally, we included hospital-specific fixed effects to capture any time-invariant hospital factors associated with observation stay use. Inclusion of hospital fixed effects in the model implies that our estimates capture within-hospital variation over time in observation stay use. This study was approved by the University of Iowa institutional review board with a waiver of informed consent (201403793).
Results
Descriptive statistics are shown in Table 1 separating patients into 3 different groups based on the type of qualifying admission they had each year. Due to the large sample size, all comparisons between the 3 groups are statistically significant. Although these groups are not randomly assigned, differences between groups are generally small, which suggests that veterans with an observation stay, veterans with a short-stay admission, and veterans with both types of stays do not differ substantially from one another.
Descriptive Statistics.

Note. For all variables, P < .001.
The regression model results are shown in Table 2. Female gender was the only patient factor significantly associated with an increase in the odds of being placed in observation rather than admitted for a short stay. Specifically, women had 10% greater odds of being placed in observation than men, holding all else constant. By contrast, both residence in an isolated rural area and increasing age were significantly associated with a decrease in the odds of being placed in observation. Compared with urban residents, residents of isolated rural areas had 10% lower odds of being placed in observation. Relatively large age differences are needed to observe a meaningful change in the odds of observation. For example, a 10-year increase in age is associated with a 4% decrease in the odds of being placed in observation rather than admitted. Notably, other patient characteristics, including race/ethnicity, homelessness, copayment status, and number of comorbid conditions, were not significant predictors of a patient’s likelihood of being placed in observation rather than admitted for a short stay.
Hospital Fixed Effect Model Predicting Odds of Observation Versus Short Stay.

Note. CI = confidence interval.
There was a very strong increase in observation stay use over time. All else being equal, a veteran presenting with chest pain had 14% higher odds of being placed in observation rather than admitted for a short stay in 2006 compared with 2005, and this trend continued over the study period. By 2013, a veteran presenting with chest pain had 7.3 times the odds of being observed compared with 2005. Figure 2 shows the trends in the absolute volume of both observation stays and short-stay admissions over the study period. Although it depicts an increase in observation stays over the entire period, clear evidence of observation stays being used as a substitute for short-stay admissions first appears between 2010 and 2011. Finally, though we do not report the individual fixed effects for each VHA hospital, these were also jointly significant (P < .0001), indicating that time-invariant unobserved hospital-level characteristics also contribute to a veteran’s likelihood of being placed in observation.

Observation stays and short-stay admissions for chest pain, 2005-2013.
Discussion
We examined a cohort of chest pain patients to identify patient characteristics associated with being placed in observation status versus admitted for a short stay (≤48 hours) while controlling for differences between VHA hospitals and the increase in observation stays over time. We also examined the absolute volume of observation stays and short-stay admissions over time to gauge the extent to which the former are being used as a substitute for the latter. Our results suggest that few observable patient characteristics are significant predictors of being placed in observation rather than admitted. More importantly, we find little evidence of within-hospital disparities in VHA observation stay use. Finally, we document a striking increase in the tendency to place chest pain patients under observation rather than admit them for a short stay, which descriptive data suggest is at least partially due to a substitution effect that emerged suddenly between 2010 and 2011.
We identified a difference in observation stay use by gender, which particularly in the setting of chest pain is likely to reflect clinical uncertainty. VHA physicians typically treat fewer women (eg, women represented fewer than 10% of admissions in our study), and thus the 10% increase in likelihood of observation may reflect a discomfort in predicting clinical course compared with men. However, women more frequently present with atypical chest pain, and clinicians are more likely to evaluate a woman as having a low pre-test probability of significant coronary artery disease causing the chest pain presentation, in which case an observation stay is a logical clinical decision over an inpatient admission.16-19
We identified a difference in observation stay use between urban and rural veterans, but we also hesitate to classify this as a disparity. Veterans from isolated rural areas had 10% lower odds of being admitted to observation. One likely explanation is that veterans living in rural settings are more likely to live a long distance from a hospital. Thus, they would have a lower threshold for meeting criteria for an inpatient admission, as they would have difficulty accessing care if their condition deteriorated unexpectedly at home. In addition, physicians could recognize that rural patients may have longer hospitalizations due to challenges coordinating care on discharge leading to a preference for inpatient admission. Last, this difference may reflect that urban veterans are more likely to present to their local VHA hospital for minor complaints associated with an observation stay, whereas their rural counterparts, particularly those with dual coverage through Medicare, may present to a non-VHA hospital for these conditions.
Regardless of the various personal characteristics that may influence their likelihood of being placed in observation, some well-informed veterans are likely to have a preference for being placed in observation rather than admitted for a short stay because of the financial implications of that designation. A veteran admitted to observation status and paying a full copay would pay approximately 4% of the amount paid by a veteran admitted to inpatient status but having a short-stay admission. 20 Thus, for veterans subject to full copayment amounts, being placed in observation status is financially beneficial. Although the copayment category variables were not significant in our model, a practice pattern may be emerging that defaults patients first to observation, with the knowledge that they will be converted to inpatient status if needed.
Finally, we found that the largest odds ratios were for the year dummy variables. This, in conjunction with the absolute number of observation stays and short-stay admissions over time (Figure 2), suggests that, at least for chest pain patients, the previously documented increase in observation stay use within the VHA over the last decade reflects a shift from short-stay inpatient admissions to observation stays. 3 As to what may be driving this trend, a VHA directive from February 2014 notes that “Mounting concerns about VA medical facility overcrowding and the lack of available beds for patients needing inpatient services have led to the more frequent utilization of observation status and observation beds as an alternative to hospital admission or discharge.” 21 Whether this substitution has had any clinical impact is unknown and warrants further research.
Our study has several limitations. First, not all veterans had an observation stay or short-stay admission during our study period. This might have resulted in our sample being non-representative of the overall veteran population. Second, there may be unobserved differences between patients in our sample that we are unable to account for using administrative data. However, we minimize this potential heterogeneity by limiting our sample to patients presenting with a chest pain diagnosis. Fortunately, both our descriptive statistics and the results from a prior study found that patients held for observation were generally similar to patients with short-stay admissions. 22 Third and finally, we are not able to say whether the use of observation or short-stay admissions was appropriate for a given patient, which is a question that future research should address.
Overall, our results suggest that after controlling for the recent increase in observation stay use across the VHA, and the marked variation in observation stay use between VHA hospitals, there are few differences in how observation status is used among different patients within the same VHA hospital. However, observation stays are increasingly being used as a substitute for short-stay admissions among patients presenting with a chest pain diagnosis. Identifying which patients are placed in observation and which are admitted is the first step in developing clinical protocols and pathways to accurately identify which patients are appropriate for observation. More research is needed to determine whether there are differences in clinical outcomes following observation stays versus short-stay admissions.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Department of Veterans Affairs Office of Rural Health. Drs Vaughan Sarrazin and O’Shea are also supported by the Health Services Research and Development Service of the Department of Veterans Affairs.