
Abstract
Uninsured and underinsured near-elderly may not have timely investigation, diagnosis, or care of cancer. Prior studies suggest Medicare eligibility confers significant and substantial reductions in mortality and increases in health service utilization. We compared 2245 patients diagnosed with lung cancer at ages 64.5 to 65 years and 2512 patients aged 65 to 65.5 years, with 2492 patients aged 65.5 to 66 years (controls) in 2000 to 2005. Compared with controls, patients diagnosed with lung cancer before Medicare eligibility had no statistically significant differences in cancer stage, time to treatment, type of treatment, and survival. Study power was sufficient to exclude mortality reductions and health service utilization changes of the magnitude found in prior work, suggesting that typically, appropriate lung cancer care may be sought and delivered regardless of insurance status.
Introduction
There is broad agreement that health insurance coverage is generally associated with better health outcomes and with receipt of appropriate care.1-3 Access to care and some outcomes were better with lower co-pays in the Health Insurance Experiment. 4 Losing and continuing not to have health insurance has been associated with declines in overall health.5-8
Yet there is less evidence for this in the near-elderly.9-11 If subsidizing and extending coverage to these patients yields better and more cost-effective outcomes, making such transfer payments may make good policy. While the Affordable Care Act is likely to cover many previously uninsured people with subsidized private coverage in state insurance exchanges, 12 some states may reject the Medicaid expansion options. 13
Some have looked at differences in health before and after the age of 65 years. Before this age, there are many uninsured and underinsured. 6 It is estimated that 13% of the near-elderly in the 55 to 64 years age group are uninsured. 14 Additional large numbers of patients are underinsured patients with less generous (eg, high deductible individual policies) or less widely accepted means-tested public insurance such as Medicaid. 15
After age 65 years, nearly all are eligible for universal insurance under Medicare. Improvement and increases in health, 16 services use, 17 self-reports of health, 18 disease control, 19 and survival after acute conditions have been reported. 15
The magnitude of estimated improvements is strikingly large. Card et al 15 found a 20% relative reduction in deaths for severely ill patients treated urgently immediately after the age of 65 years, compared with similar patients treated immediately before the age of 65 years, a mortality gap that persisted for at least 9 months after the index admission. Similarly, large relative increases of between 11% and 23% in nonurgent medical procedures were found in those above 65 years compared with those below 65 years. 18
However, the complex methods used in some investigations have sparked debate about the true existence of beneficial effects16,20,21 and the interpretation of results.7,20,22
Others have not found any relative slowing of health decline after 65 years among the previously uninsured, 20 nor any population mortality impact in the 10 years following Medicare enactment. 23 These discrepant findings may in part be due to different types of health conditions studied. Still others point to the risk that generous insurance may lead to patient moral hazard, 24 which could cause patient harms through overdetection, overdiagnosis, or even overtreatment of disease.
It has been argued that Medicare’s insurance effects could also lead to differences in outcomes and costs among cases of common, serious cancers diagnosed around the 65th year of age. 25 In this study, we examine lung cancer and seek to understand whether the magnitude of beneficial insurance effects is as high as suggested by the prior literature.15,18
Our objective is to understand these potential associations and we examined staging, treatment and outcomes for patients diagnosed before and after Medicare eligibility among US patients.
Conceptual Framework
Lung cancer is typically a fast progressing cancer after diagnosis and leads to more deaths in the United States than any other type of cancer. 26 Among patients with a lethal cancer such as lung cancer, insurance status may be associated with outcomes and costs in 2 ways.
First, patients may receive a lung cancer diagnosis before they are eligible for Medicare. They may then face delays in receiving appropriate disease-specific and stage-specific care until they are eligible for Medicare. Such patients may then face significantly longer treatment delays, different treatment, or different outcomes than patients diagnosed considerably later, after Medicare eligibility.
Second, patients may face delays in investigation of the symptoms and signs of lung cancer before they are eligible for Medicare. They may then not have a diagnosis made until they are newly eligible for Medicare. These patients may then have significantly more advanced disease, different treatment, or different outcomes than patients diagnosed later after Medicare eligibility.
Data and Methods
We analyzed a national convenience sample, the Surveillance, Epidemiology, and End Results (SEER) registry data maintained by the National Cancer Institute (NCI). 27 Due to differences in course of disease, we constructed different sized analytical cohorts for the 2 different cancers (Figure 2). The NCI administers 15 SEER registries, which cover approximately 26% of the national population. 28 We used the Patient Entitlement and Diagnosis Summary File (PEDSF) files, which link SEER registry data with Centers for Medicare & Medicaid Services’ master enrollment file data. 29
The PEDSF file contains each patient’s month and year of birth, date of death (if any), sex, marital status, race, ethnicity, state of residence, Census Bureau data on basic socioeconomic status at the census tract and zip code level, reason for Medicare entitlement, and Medicare Part A, B, or C enrollment. Diagnosis information contains site, grade, extent of disease, staging, and manner of confirmation. Treatment information is available for month and year of treatment with radiation, and for cancer-directed surgery. 30
We obtained all SEER-Medicare PEDSF files for lung cancer patient diagnoses made between 2000 through 2005. The linked Centers for Medicare and Medicaid Services (CMS) data in the PEDSF files allowed vital statistics follow-up through the end of 2007. We included SEER-Medicare patients with a diagnosis of lung or bronchus cancer (SEER 2-digit site recode 39). We excluded patients whose lung or bronchus cancer diagnosis was not the first in the SEER registries as patient characteristics and physician behavior may be systematically different in patients with a second occurrence of cancer. We excluded patients with missing or invalid data for diagnosis month and/or year and patients eligible for Medicare on the basis of disability or end-stage renal disease.
We used birth month and year and diagnosis month and year to create age-specific cohorts from the total of 7249 patients who met our inclusion criteria (Figure 1). We constructed a cohort of 2245 patients aged 64.5 to 65 years (which we refer to as “pre-eligible”), a cohort of 2512 patients aged 65 to 65.5 years (“newly eligible”), and a control cohort of 2492 patients aged 65.5 to 66 years (“control eligible”) at time of diagnosis.

Cohorts and frequency of cases by cancer type, age, and eligibility.
For baseline cohort characteristics, we present frequencies for categorical variables and means with standard deviations for continuous variables. We tested the significance of changes in categorical (stage, diagnostic confirmation) and ordinal (tumor size) variables using chi-square tests. We used Kruskal-Wallis equality of populations tests for changes in continuous variables and median tests for equality of medians. For diagnostic categorical variables, we present frequencies in each cohort. We collapsed diagnoses of small cell lung cancer into 1 category. We also collapsed diagnoses of stage I and stage II non-small cell lung cancer into 1 category, and cases of stage III and stage IV non-small cell lung cancer into another category.
For outcome variables, we present frequencies and unadjusted risks in each cohort. We compared proportions surviving 0, 3, 6, 12, and 24 months and proportions receiving initial cancer-directed therapy within 0, 1, 2, 3, 4, 6, and 12 months of diagnosis using chi-square tests of crude risk ratios. Separately we compared the proportions of patients receiving radiation and/or surgery for patients in whom therapy was started within 4 months of diagnosis. We had data through December 31, 2007, or at least 24 full months following diagnosis, allowing event rates to be calculated for all patients.
Our data were interval censored at the month level. For outcome proportions and rates, we treated an outcome occurring in the same month as diagnosis as occurring at month 0, though this may have happened from 0 to 61 days after diagnosis. We maintained the assumption that over any time period this bias was mean zero and not differential over the cohorts under comparison. In our 12- and 24-month outcomes data, the possible magnitude of this bias is small in relative terms.
In event history analyses, we plot crude rates of outcomes and rates adjusted for competing risks.31,32 We used Kaplan-Meier graphs to plot cumulative failure for the outcomes of receipt of radiation or cancer-directed surgery, and for the outcomes of death from all causes and death from lung cancer alone. Survival from all causes and treatment data was treated as censored after December 31, 2007. Survival from lung cancer alone was treated as censored after December 31, 2006, the latest death certificate follow-up in the SEER data. We used the log-rank test to compare failure distributions across cohorts in analyses not adjusting for competing risks.
Our Kaplan-Meier plots for survival, survival from lung cancer, and receipt of treatment assume that earlier death from other causes is not informative. This does not adequately adjust for competing risks.33,34 In lung cancer treatment, decisions and survival are unlikely to be conditionally independent, given patient characteristics. In the older cohorts, we need to take into account an increased risk of death from other causes. We used cumulative incidence graphs to analyze treatment receipt, adjusted for the competing risk of death from any cause. We also plotted the cumulative incidence for death from the primary cancer diagnosis, adjusted for the competing risk of death from any other known cause.
SEER*Medicare data 35 were managed using SAS software, version 9.2; all statistical computations and graphical output were performed using Stata/SE software, version 10.1. All analyses were 2-tailed. No adjustments for multiple comparisons were made. 36 We considered all P values less than .05 to be statistically significant. This study was approved by the institutional review board (IRB) of the study institution’s Health System and declared exempt from IRB review under 45CFR46.101(b)(4).
Results
Baseline characteristics generally did not differ significantly across the pre-Medicare eligible, newly eligible, or eligible cohorts (Table 1). Gender, ethnicity and race, residence in metropolitan areas, and marital status were similar across cohorts. There was a small but significant difference in the extent of poverty in the patient residence census tracts across age cohorts (P < .001). This may represent artifactual variation or changes in residence after retirement.
Lung Cancer Characteristics of Pre-Medicare Eligible, Newly Eligible, and Post-Medicare Eligible Cohorts.

Note. Big metro = counties in metropolitan areas of 1 million or more population.
Diagnostic characteristics were not significantly different in extent of disease, staging, and manner of diagnostic confirmation (Table 2). Across the pre-eligibility, newly eligible, and eligible cohorts, there was no consistent or significant trend in staging.
Lung Cancer, Extent of Disease, Staging, and Method of Diagnostic Confirmation.

Note. Extent of disease based on the <e10sz1>, <e10ex1>, and <e10nd1> SEER data fields for cases in 2000 to 2003. Size excludes “diffuse.” Extent and lymph node involvement: 3 most common values each, except “unknown.” Staging of cases in 2000 to 2003 reflects SEER coding of AJCC (American Joint Committee on Cancer) stage field and in 2004 to 2005 reflects DAJCC (Derived AJCC) stage field. SEER = Surveillance, Epidemiology, and End Results.
The rate of lung cancer diagnosis based on death certificate only, without evidence of clinical, imaging, or pathological conformation was constant and low across the cohorts. Among the pre-eligible cohort, 95.1% of patients had lung cancer confirmed on pathology. In newly eligible Medicare patients, this rate was 94.7%, and in patients already eligible for Medicare for at least 6 months, it was 94.9% (P = .62).
Treatment receipt exhibited no significant differences across cohorts in timing or type of treatment (Table 3). Of the pre-eligible cohort, 78.0% received therapy within 4 months as did 78.5% of the newly eligible, compared with 78.4% of the 65.5 to 66 years old cohort. Unadjusted risk ratios did not differ significantly from equality and were not significant when comparing pre-eligible and control cohorts, or when comparing newly eligible and control cohorts.
Lung Cancer, Time to Initial Therapy, Type of Therapy Received, and Deaths, Crude and Not Adjusted for Competing Risks.

Note. Events at 0 represent same month at diagnosis. Later events refer to events through end of the given month. “Neither” = initial therapy due to other (eg, chemotherapy).
At this 4-month landmark, radiation and/or cancer-directed surgery receipt did not differ across the cohorts.
Treatment event history over time was not different with the hazard of receiving initial cancer-directed therapy identical across cohorts, ignoring the competing risk of death (unreported). Nearly 75% of registry patients had started a cancer-directed therapy within 2 months, with no difference between the pre-eligible and the control cohorts (P = .79). Similar nonsignificant estimates were found for the comparison between the newly eligible and the control cohorts.
In analyses that were robust to the competing risk of death, cumulative incidence for treatment receipt showed no essential differences for the comparison of pre-eligible and control cohorts (Figure 2) as well as for the comparison of newly eligible and control cohorts (unreported).
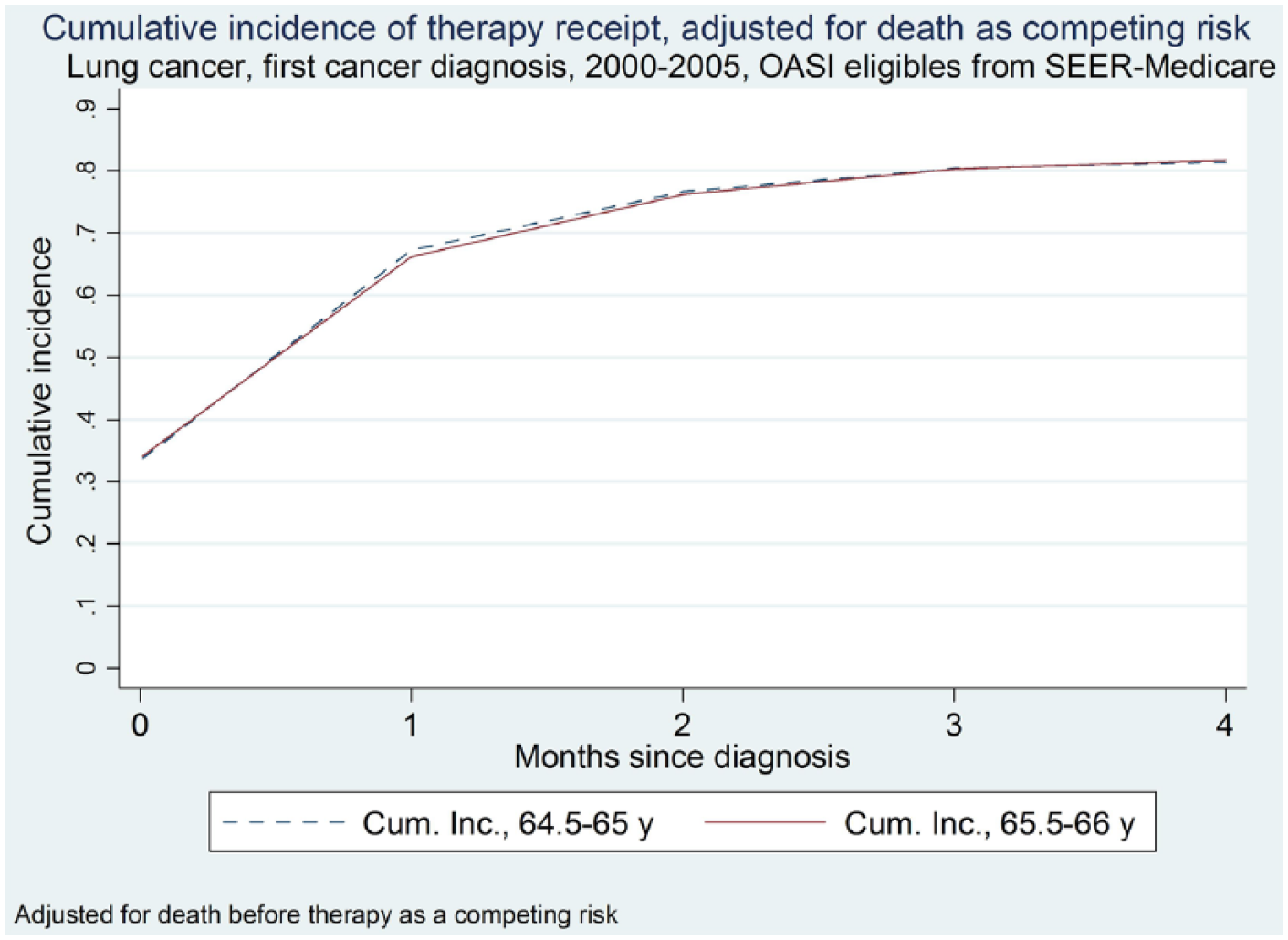
Cumulative incidence for therapy start, adjusted for death as competing risk, for pre-Medicare eligible (64.5-65 years old) and control cohorts (65.5-66 years old).
Turning to longer term survival (Table 3), point estimates of death rates were consistent with small secular increase over age across the cohorts. The pre-eligible cohort unadjusted rate of death was 36.4% within 6 months, compared with 36.7% for 65.5 to 66 years old control cohort (crude risk ratio 0.99; P = .86).
A total of 36.2% of newly Medicare-eligible patients with lung cancer died within 6 months of diagnosis, indistinguishable from the control cohort (crude risk ratio 0.99; P = .72). Survival event history showed no significant cohort differences (not reported). Kaplan-Meier complements for overall survival overestimate death due to lung cancer, since they do not differentiate between death due to lung cancer and death to other causes.
Cumulative incidence estimates that adjust for the competing risk of death from other causes (Figure 3) show the older control cohorts having statistically identical incidence of lung cancer specific deaths, but slightly higher incidence of other deaths as would be expected given the secular trend in mortality hazard.

Cumulative incidence of death from lung cancer and death from other causes for pre-Medicare eligible (64.5-65 years old) and control cohorts (65.5-66 years old).
We considered three potential threats to the robustness of our results. These hinged around (1) adequacy of the study’s power, whether (2) inclusion in the study was biased by potential nonrandom missingness, and whether (3) the diagnostic threshold for lung cancer was constant. We report in the Appendix that our results appeared robust to these potential threats.
Conclusions
This study used cancer registry data to detail disease, treatment, and outcome differences among the near-elderly and elderly around the age of 65 years for a common and important cancer. Our approach was designed to identify harms from underinsurance and benefits from insurance due to better and more timely access to care. Nevertheless, our study failed to show substantial, consistent, or clinically meaningful differences between patients diagnosed before and immediately after eligibility for Medicare.
In this large, nation-wide study using recent lung cancer data, we found no clinically meaningful evidence that underinsurance or uninsurance harmed patients diagnosed with lung cancer before Medicare eligibility. We found minor but insignificant differences in lung cancer stage. However, in time to treatment, in treatment type, in lung cancer–specific survival, and in all-cause survival, no significant differences were found across cohorts.
Our study was premised on discontinuous change in insurance status caused by exogenous aging into Medicare at age 65 years. Before this age, there are large numbers of uninsured patients6,37 with an estimated 13% of the near-elderly in the 55 to 64 years age group uninsured. 14 Pre-Medicare eligibility, many other individuals are underinsured due to less generous (eg, high deductible individual policies) or less widely accepted insurance (eg, Medicaid).
Improved access to insurance has been found to be associated with better access to health care and improvement in health,16,17 with substantially improved survival after acute conditions, 15 and with substantially increased utilization of care.16-18,38 Yet this adequately powered study was unable to detect differences in survival or utilization of the magnitude found by prior studies.
Our study has several important limitations that remain unresolved despite extensive robustness checks. Our study focuses narrowly on 1 type of cancer, albeit a common, well-known and important one. Our data are not necessarily representative of the entire US population. Currently, the SEER databases cover approximately 26% of the total US population in a nonrandom manner. For example, there is a large concentration of states in the West and Southwest (California, New Mexico, Arizona, and Utah) but far less or no representation in the rural Northeast and much of the large population centers in the Midwest apart from Iowa. Approximately 98% of cancer cases are ascertained in that population. 39 Whether missing data in the cohorts we examined are missing at random is unknown.
Related to this limitation is our inability to compare and contrast variations in small areas of the relationship of insurance coverage and treatment and outcomes. This is driven by the relatively low sample sizes at the individual state level, or the individual counties captured in some states. Our study’s statistical power is inadequate for such comparisons, even though it is possible that there are differences in professionalism among providers and hospitals by geography, and potential differences in access to care without concern about coverage and reimbursement.
Other limitations are that we included patients from the 2000 calendar year, even though major registry expansion happened in 2000. We also pooled data across multiple calendar years, ignoring possible cohort effects. We did not ascertain the receipt of chemotherapy, which is separately coded in the Medicare claims for patients enrolled in fee-for-service Medicare. 40 Information on cancer-directed surgery was limited to the most extensive procedure among planned procedure(s) performed for the primary cancer or surgery performed within a year if cancer does not recur or progress. 30 We do not observe whether treatment was curative, adjuvant, or palliative. If surgery to relieve metastatic disease differs systematically across cohorts, then we will miss such differences. We were also unable to quantify cohort treatment costs, which are important as cancer costs continue to rise. 41
Other disease-specific limitations include the fact that this study took place in the period of time before the positive trial results on low-dose computed tomography (CT) screening for lung cancer. 42 Our results might have been different in a later period in which screening was reduced. Our data also lack information on patient co-morbidities or preferences, which might drive differences in therapy afforded. However, rates of patients who did not undergo surgery that had been recommended did not differ significantly across the cohorts.
Our study fails to support concerns that patients diagnosed with lung cancer just before Medicare eligibility faced delays in receiving appropriate disease and stage-specific care until they are eligible for Medicare. These results are also not consistent with patients facing delays in investigation of the symptoms and signs of lung cancer before they are eligible for Medicare, with subsequently more advanced disease after Medicare eligibility.
There are a number of alternative explanations for our study’s negative results. For example, differences in care may exist, but their effects may be too small to detect. Given the adequate power in this study, and the prior literature results suggesting substantial changes in general, this explanation may not be compelling.
Another alternative explanation is that most patients with lung cancer present with a poor prognosis. Our failure to find differences in cancer care immediately pre-and post-Medicare eligibility may therefore simply reflect the natural history of this disease. This is plausible but mitigated somewhat by the persisting absence of differences even at 24 months’ follow-up of lung cancer. Finally, differences in cancer care due to reduced pre-Medicare access among the uninsured or underinsured may exist, but could be compensated for by physicians providing differential care to these upon eligibility. Our study could not identify such confounding, but cannot rule this explanation out.
The simplest explanation for our results is also the most reassuring. Patients with serious diseases receive timely investigation, diagnosis, and treatment regardless of insurance coverage. On the patient side, the symptoms and signs of undiagnosed lung cancer may lead a patient to seek investigation regardless of ability to pay. On the provider side, the seriousness of diagnosed lung cancer may ensure the provision of care to such patients regardless of ability to pay.
Even though we found no evidence of Medicare effects in an acute, serious disease, there may be unobserved improvements in patient well-being. For example, access to health care may provide subjective improvements in stress. In lung cancer, the availability of expensive epidermal Growth Factor Receptor (eGFR) tyrosine kinase inhibitors such as erlotinib (Tarceva®) in 2005 coincides with the end of our sample period. Insurance coverage may have allowed patients to derive greater utility from such availability, including decreased symptoms, 43 despite relatively small extensions of life.
Looking forward, low-dose chest CT scans to screen for lung cancer in patients may be increasingly accepted as effective preventive care compared with radiographic screens. 42 Access to insurance is likely to increase access to such advanced preventive care, although patterns of care utilization may not change substantially after insurance is gained. 44
Even if there is no evidence of clinical effects of Medicare, there may be individual utility improvements from access to universal insurance among the near-elderly. 20 Inadequate access to actuarially fair insurance prevents consumption smoothing. Unaffordable access to private coverage for uninsured newly ill near-elderly households may lead to severe household wealth shocks. 45 Since the near-elderly are risk-averse and financially constrained, both of these nonclinical effects matter.
In conclusion, this study of an important and common cancer suggests that insurance status is not substantively associated with differences neither in access, treatment type and delay, nor in outcomes around the time of Medicare eligibility. Although extending Medicare-like benefits to the uninsured and underinsured near-elderly may be justified on many grounds, our results suggest that for these serious diseases there would be no significant improvements in outcomes.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.