
Abstract
Third-party payer systems are consistently associated with health care cost escalation. Taiwan’s single-payer, universal coverage National Health Insurance (NHI) adopted global budgeting (GB) to achieve cost control. This study captures ophthalmologists’ response to GB, specifically service volume changes and service substitution between low-revenue and high-revenue services following GB implementation, the subsequent Bureau of NHI policy response, and the policy impact. De-identified eye clinic claims data for the years 2000, 2005, and 2007 were analyzed to study the changes in Simple Claim Form (SCF) claims versus Special Case Claims (SCCs). The 3 study years represent the pre-GB period, post-GB but prior to region-wise service cap implementation period, and the post-service cap period, respectively. Repeated measures multilevel regression analysis was used to study the changes adjusting for clinic characteristics and competition within each health care market. SCF service volume (low-revenue, fixed-price patient visits) remained constant throughout the study period, but SCCs (covering services involving variable provider effort and resource use with flexibility for discretionary billing) increased in 2005 with no further change in 2007. The latter is attributable to a 30% cap negotiated by the NHI Bureau with the ophthalmology association and enforced by the association. This study demonstrates that GB deployed with ongoing monitoring and timely policy responses that are designed in collaboration with professional stakeholders can contain costs in a health insurance–financed health care system.
Introduction
Background
Third-party payers have continuously innovated with payment mechanisms to overcome cost escalations resulting from consumer moral hazard and demand induction by providers. In the United States, the initial dominance of cost-plus reimbursement has successively given way to per-diem reimbursement, fixed-rate diagnosis-related group payments, capitation, and most recently, under the Affordable Care Act, population health-driven accountable care organizations. Capitation-based reimbursement systems are complex to manage and unpopular among both providers and patients, particularly in health systems where patients are accustomed to free choice of providers. These issues have led to the increasing use of global budgeting (GB), a population-based expenditure cap that accommodates a fee-for-service base in apportioning payments to providers. Germany was among the earliest to introduce global budgets with expenditure caps in 1992 for physician visits, and subsequently for hospital services. 1 The Netherlands also has a well-established global budget system. 2
Taiwan implemented a National Health Insurance (NHI) system in 1995, mandating universal coverage under a single-payer system. It experienced rapid escalation in health care expenditures, which increased at an annual rate of 6.26% from 1995 to 2001 despite annual population growth of only 5.2% during this period. 3 Premium revenues increased by 4.26% annually, causing repeated financial crises. 3 The cost escalation under NHI is largely due to increasing use of high-tech care (eg, 80% increase in dialysis visits between 1994 and 20003), increased intensity of care within care episodes, and increased lengths of stay. 4 The cost escalation continued even after annual rates of per capita health care encounters stabilized following the spurt in the first NHI year. Increases in volume and care intensity under NHI are documented in several studies. Compared with 1994 (pre-NHI), the year 2000 (5 years since NHI implementation) showed a 16.6% increase in total outpatient visits and a 19.7% increase in inpatient surgeries. 3 These increases were almost entirely accounted for by an initial spurt in utilization by the (pre-NHI) uninsured 43% of the population. 5 The pre-NHI insured population had annual outpatient visit rates of 12 per capita both pre-NHI and in the first year of NHI. This is exactly the visit rate observed among the previously uninsured on becoming newly insured. 5 Other studies document the general population-wide stabilization of outpatient visit rates following the first post-NHI year, fluctuating between 12.2 visits in 1997 and 12.7 visits in 2000. 6 The slight increase in visits is attributed to the increase in the insured population from 92% in 1997 to 96% in 2000, and population aging. 3
Unsustainable cost escalations led to sector-wise GB, beginning with dental clinics in 1998, Chinese medicine clinics in 2000, Western medicine clinics in 2001, and hospitals in 2002. A global budget GB is an overall spending limit to control aggregate health care spending in a health plan, service sector, or health care institution. 7 This study was designed to assess clinical providers’ response to GB in terms of service volume changes and substitution of high-revenue services for low-revenue services, and later changes in provider behavior in response to the Bureau of NHI (BNHI) policy of imposing service caps. We used eye care service changes to study provider behavior.
Unlike capitation that limits patient choice of providers, GB targets providers, requiring them to either restrict care, or accept price reductions if the collective service volume exceeds the normative volume assumed in setting the budget. GB is a documented cost-containment mechanism that does not directly alienate the population, as illustrated in the Canadian8-10 and German health care systems.11,12
In Taiwan, each sectoral global budget is allocated among the six BNHI administrative regions. Region-wise GB allocations for the clinic sector were set in 2001 based on population, age/gender composition, standardized mortality ratio, and historic share of health care expenditures. The initial allocation is annually adjusted based on anticipated changes in demographic profile.
13
Each BNHI branch pays providers quarterly, based on the monetary value of a point calculated by pooling provider claim points in the BNHI region and dividing the expenditure cap by the total claimed points. Providers are reimbursed based on their individual claim points. A point is a standardized unit of service or care item, used as the currency for all claims. It has a base value of NT$1 (New Taiwan dollar) set in 2001 when the clinic sector GB commenced. The point value is inversely proportional to the total service volume in the region, fluctuating quarterly with the conversion factor (CF)
14
floating up or down. Service volumes exceeding the region’s cap result in reduced reimbursement rates per unit of service for all providers. Specifically, provider reimbursement in NT dollars is calculated as follows:
Anticipating unnecessary service provision by clinics seeking to increase their respective market shares, the BNHI introduced concurrent policies to monitor provider volumes and audit providers who exceed historic service volumes. 14 The top 10% of providers by point volume are subjected to administrative review by annually appointed medical teams nominated by the regional medical societies. A random sample of claims is reviewed for care appropriateness, and questionable claims are deducted from the provider’s total claims (points neutralized) up to a maximum of 10%. Providers who are not in the top 10% by volume suffer a 1% to 3% neutralization of points for disproportionate increases over the previous year. This policy restrains providers with large market shares from crowding out smaller providers through market power. Underserved areas with health professional shortages are exempt from this policy.
The documented effects of GB in Taiwan are increased inpatient volumes following hospital GB,5,15 and increased outpatient volumes following clinic sector GB. 16 These studies examined total care volumes without the exploration of care intensity or substitution of services by providers. Such studies require specialty-specific data to identify changes in services categorized by care intensity. The present study examines the service provision behavior of clinic ophthalmologists under GB. In Taiwan, clinic doctors are not permitted to additionally work at hospitals and vice versa. Physicians of eye care clinics are reimbursed either through a Simple Claim Form (SCF) or Special Case Claim (SCC). SCF is reimbursed with a low, fixed price for a routine bundle of services, generally a routine office visit or prescription drugs dispensing not exceeding 3 days). An SCC is an itemized claim with potential for discretionary billing, usually used for procedure-based care involving variable provider effort, technology, consumables, or non-routine medicines.
Despite administrative policies to restrain unnecessary services, physicians possess expert power advantage to selectively over-provide high-revenue services while remaining in compliance with BNHI policies. As an administrative third-party payer, BNHI can do little to selectively rein in care provision. We examine GB impacts on both volume and composition of eye care services, fixed-price, low-revenue SCF services versus discretionary billable SCC services. In Taiwan, a physician can choose to be either office based or hospital based but not both. The clinic sector was studied because of separate GBs for the clinic and hospital sector, and because typically most eye services are ambulatory even when provided by a hospital.
The response to a change from fixed-rate fee-for-service to a GB system with a variable point value is similar to a non-zero-sum game. Game theory posits that participants choose actions that maximize their utility considering the choices of others. An expenditure cap should incentivize providers to restrict output to maximize the revenue from each service. In other words, total income may be maximized at a lower service volume if each point (CF) is worth more. However, in a context of limited, shared resources (such as a prospectively fixed budget with no control on individual provider volumes), individuals can increase income at the expense of others or maintain a target income by raising their own service volume and increasing market share even if the per-service revenue is reduced. Each individual realizes that the most rational choice for all other players is to increase output, causing all players to increase their own output, even though it will lead to a decline in the average reimbursement rate for all players. This scenario is described as the tragedy of the commons, 17 a multi-player version of a standard game, the prisoners’ dilemma. In the context of eye services in a GB environment, providers faced with a choice between SCC and SCF may be incentivized to maximize their billable points by increasing SCC services relative to SCF. The only penalty for increasing point volume is the neutralization of excess points. However, from a social welfare perspective, there may be an actual social welfare loss. The floating point value may decline so precipitously due to greatly increased service volumes, that the marginal cost of providing an extra service may exceed its marginal revenue. This may result in substandard service using inadequate or inferior resources, thereby compromising quality. Furthermore, to the extent that the services were unnecessary, patients are exposed to increased risk of iatrogenic injury or adverse drug reactions, a socially harmful outcome even though budget neutral for the BNHI. Recognizing the potential for harm, BNHI implemented a major policy in 2005-2006, setting a 30% ceiling on SCC points out of each clinic’s total claim. 18 This study will also investigate the impact of this payer-initiated policy on service volume and composition.
The present study explores two research questions based on the conceptual framework and regulatory change. The first research question examines whether clinic sector GB, effective 2001, was associated with a post-GB increase in service volumes, particularly high-revenue SCC services relative to low-revenue SCF services. At any point in time, the total patient market (population) is fixed, and provider time and energy are finite. Under these circumstances, GB implementation may cause physicians to favor SCC over SCF services in increasing their service volume. We also examined the concomitant changes in SCF to answer the following question: Did providers (1) increase their total care effort (SCC plus SCF), or (2) sustain their total care effort at 2000 levels but displace effort to more profitable services, or (3) engage in unremitting care escalation of all types to maximize their market share of points? Our second research question examines the impact of the BNHI service cap policy on SCC and SCF volumes. Our study hypotheses were as follows:
Our study controls for market competition in the empirical specifications used to test both hypotheses. Large urban centers with more competitive markets may witness more service inducement than less competitive markets in keeping with highly competitive attitudes rather than cooperation in highly competitive markets. Moreover, in competitive markets the potential to increase services on the extensive margin (eg, the number of different patients or office visits) is limited whereas it is still possible to increase services on the intensive margin (eg, the number and intensity of services provided during each consultation). Our study also tests whether service provision was restrained in the second period in 2007 (post-BNHI enforcement) relative to 2005 (pre-BNHI enforcement), and whether the service volume change was limited to the BNHI-targeted sector (SCC) or accompanied by compensatory increases in the unrestrained service sector (SCF).
Materials and Methods
Since the launch of universal coverage, single-payer health insurance system in 1995, health insurance coverage in Taiwan increased from 56% to more than 90% the following year, and to 99.6% for its 23 million people in 2011. Because clinics and hospitals are required to document all care provided to claim reimbursement, the secondary claims data are considerably reliable. In the present study, claims data on outpatient ophthalmology clinics for the years 2000, 2005, and 2007 were used. Clinic sector GB was implemented in 2001, and the SCC service cap policy was implemented in 2006. We used 2000 claims data representing the pre-GB year, 2005 data representing post-GB, but prior to service cap policy period, and 2007 the post–service cap year. The unit of observation is the clinic. Clinics were included in the analysis if they were represented in the claims data in all 3 years.
Eye care falls under the umbrella of the Western medicine clinic sector GB, and is reimbursed through SCF and SCC mechanisms. SCF applies to most routine outpatient visits consuming a standard amount of provider time and up to a 3-day supply of cost-predictable prescription drugs. A fixed fee is reimbursed per SCF claim. SCC applies to non-routine care episodes, involving variable provider time or skill, outpatient procedures involving non-standard care items or technology or prescription drugs. SCC claims are required to show itemized treatments, consumables, and pharmaceuticals provided. SCC claim amounts are typically higher and more profitable than SCF, but because they have to be itemized, filing is lengthy and cumbersome.
Outpatient claims of all eye clinics were extracted from the NHI’s de-identified claims database. Although clinics in general limit services to office visits and minor procedures, ophthalmology (unlike most specialties) is amenable to ambulatory surgery for many eye conditions. Because of a lack of primary care gatekeeping in Taiwan’s health system, patients can access any clinic or hospital for care. The NHI Bureau has defined 17 medical area networks (health care markets) based on geographic contiguity of human settlements and commuting patterns. To calculate the Herfindahl-Hirschman index of market competition in each market, the total of all eye services claims submitted by clinics and hospital outpatient departments in each medical area network served as the denominator, and each clinic’s total claims was the numerator.
Policy changes were identified by reviewing the BNHI Web site for policies applicable to eye services and through interviews with national and regional office-bearers of the ophthalmologists’ association. These officers engage with the BNHI in policy development and enforcement.
Statistical Analyses
Changes in point volumes were analyzed separately for SCF and SCC. The following were used: (1) t test of differences in mean claim points per clinic nationwide, and clinic-level paired t tests of differences in claimed points between 2000, 2005, and 2007; (2) paired t tests of differences in clinic points within each health care market in the above-mentioned 3 years; and (3) multilevel modeling with repeated measures to model SCF and SCC separately, specifying health care market fixed effects. Market fixed effect was used to account for health care market characteristics that may affect a provider behavior.
All clinics with eye care claims in 2000, 2005, and 2007 were included in the study. Annual SCF and SCC points were calculated for each clinic. SCC and SCF claim points were the key dependent variables of interest. Key predictor variables were market competition level Herfindahl-Hirschman Index (HHI), clinic type (solo practice, single-specialty group practice, and multi-specialty group practice), and geographic region (north, south, central, and east). Herfindahl-Hirschman Index (HHI) was calculated as the sum of squared market shares of the clinics out of the total outpatient eye care provided in clinics and hospitals in each health care market. A higher HHI score indicates lower competition or high market concentration, and a lower HHI indicates a highly competitive market.
SAS (Version 9.2) was used. Measures of skewness and linear regression residual analysis showed violations of normality of the dependent variables, SCF and SCC. Natural log and square-root transformations were tested; the latter resulted in a near-normal distribution, suitable for linear regression. Square-root transformations of claim points were subjected to multiple regression analyses that produced randomly distributed residuals across clinics by size or type (without heteroscedasticity) permitting valid inferences.
Results
Table 1 presents the distribution of clinics by type and ownership. Approximately 80% of clinics were solo practices, mostly for-profit. A total of 418 clinics had SCC claims in all 3 study years, and 297 clinics had SCF claims in all 3 years. Figure 1 and Table 2 show that the nationwide mean SCC claim point per clinic in 2005 was higher than in 2000 (paired t test, P < .0001). The 2007 claim volume was similar to that of 2005 (P = .40). The SCC increase in 2005 was driven by significant increases in the highly competitive markers of the major metropolitan cities (Taipei, Taichung, Kaohsiung, Taoyuan, and Changhwa, points A-E in Figure 2). The increase in SCC points followed by stabilization in 2007 at the 2005 level is validated by clinic-level paired t tests within markets, with the highest increases observed in the above-mentioned five markets (table not shown).
Distribution of Clinics With SCF Claims and SCCs in 2000.

Note. SCF = Simple Claim Form; SCC = Special Case Claim.

Mean Special Case Claim points per eye clinic in Taiwan.
Paired t Tests of the Differences in Global Budget Points Claimed by Clinics, Pre-GB, Post-GB but Prior to Service Cap, and Post–Service Cap.
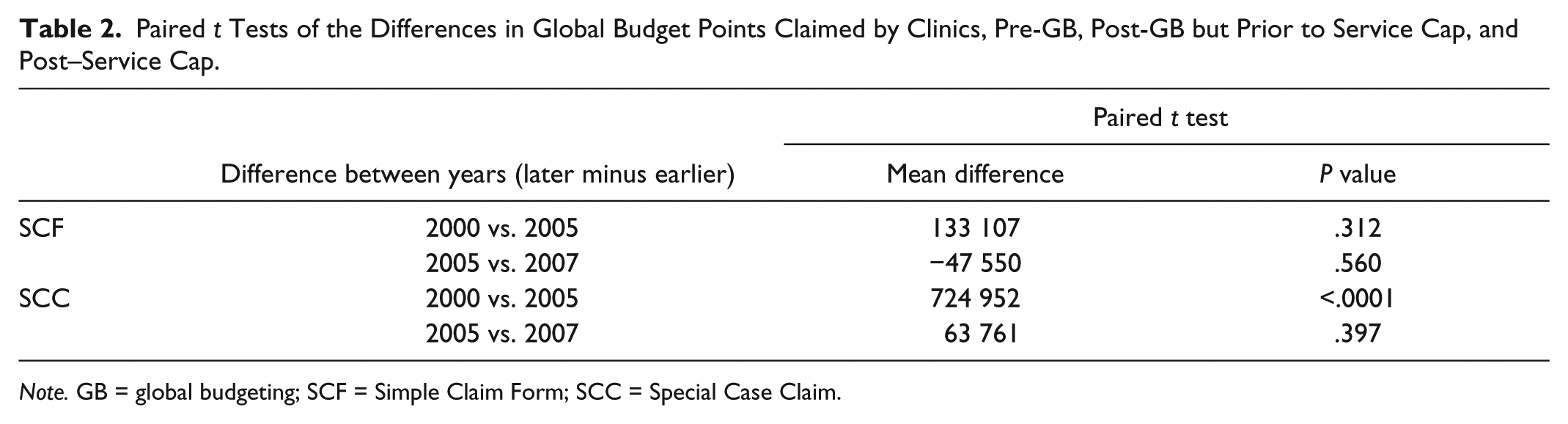
Note. GB = global budgeting; SCF = Simple Claim Form; SCC = Special Case Claim.
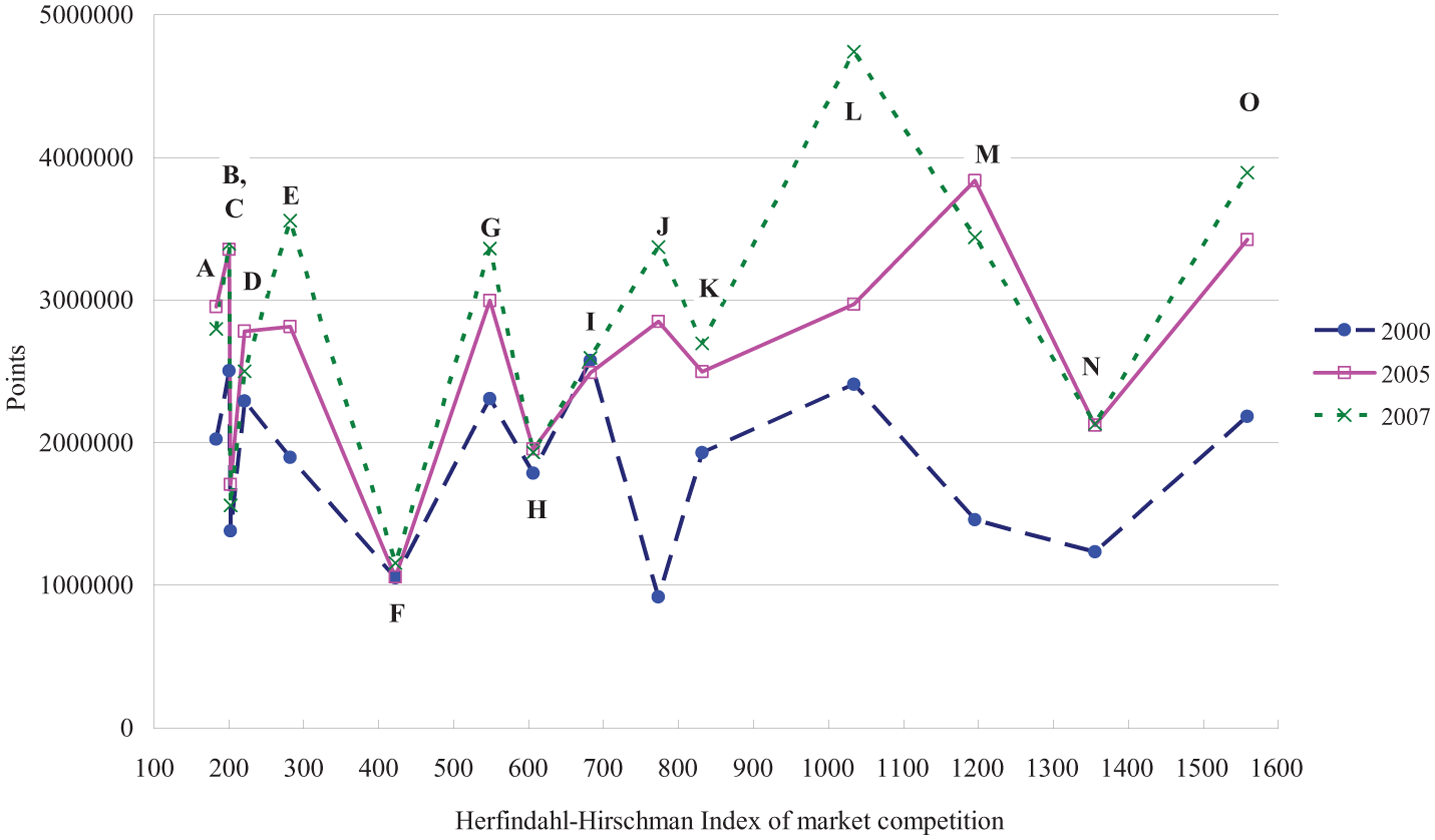
Mean SCC points per clinic in each medical care market represented by the HHI level.
For SCF, Figure 3 shows that the nationwide claims total in 2005 was similar to 2000 and 2007 (health care market-wise paired t tests, P = .31, and P = .56, respectively; see Table 2). The lack of significant difference nationally was sustained in within-market analyses (table not shown). Plots of clinic means grouped by market against HHI show no systematic patterns relative to the intensity of competition (see Figure 4). The observed year-wise changes in the figure are not statistically significant.

Mean Simple Claim Form points per clinic—All clinics in Taiwan.

Mean SCF points per clinic in each medical care market represented by the HHI level.
Multiple regression analysis results are shown in Table 3. The adjusted SCC points were significantly different by study year, with 2005 points being higher than 2000 points (P < .0001). SCC point volume in 2007 was similar to the 2005 volume. Multi-specialty group practices claimed significantly more points than solo and single-specialty group practices (P < .01, and P < .001, respectively). The SCC point volume was not associated with market competition (P = .06). Interactions between year and competition, year and ownership, and competition and ownership were not significant. Health care market effect was not significant but was retained in both SCF and SCC regression models to account for unique market characteristics driving provider behavior.
Adjusted Associations Between Eye Care Volume and GB Policies, Year 2000 (Pre-GB), 2005 (Post-GB but Pre–SCC Service Cap), and 2007 (Post–SCC Service Cap).

Note. Geographic region is collinear with the HHI area and hence removed from the model. GB = global budgeting; SCC = Special Case Claim; SCF = Simple Claim Form.
P < .05. **P < .01. ***P < .001.
For SCF, the 2005 and 2007 volumes were similar to 2000 after accounting for clinic type and ownership. Multi-specialty group practices claimed significantly more points than solo and single-specialty groups. In addition, for-profit status was associated with higher SCF points (both P < .001). Market competition was significant, and lower competition was associated with higher SCF points. None of the interaction terms was significant.
To facilitate conclusions on provider behavior across the two service types, Table 4 presents an integrative summary of findings and the associated conclusions regarding provider behavior. Low-revenue, fixed-rate SCF services remained constant from pre-GB to early post-GB and late post-GB, but SCC increased in 2005 over pre-GB, and was sustained at the 2005 level in 2007.
Summary of Eye Care Provider Behavior Under Global Budgets.

Note. SCF = Simple Claim Form; SCC = Special Case Claim; GB = global budgeting.
Discussion
Our study documents evidence of increased provision of discretionary billable, care-intensive services with no change in low-revenue services under GB. These findings support that providers attempt to maximize their individual share of the global budget to maintain a target level of income. The BNHI responded by co-opting the experts (specialist associations) to come up with a realistic cap on discretionary billable services using historic data, and enlisted physician cooperation for the policy by relying on professional self-regulation to enforce the caps. Concurrently, the BNHI promoted awareness of the collective long-term interest of providers served by limiting health care costs to NHI premium revenues. The strategy was effective, as shown by sustained SCC volumes in 2007 at the 2005 level with no further increase.
Viewing SCF and SCC changes concurrently, we observe that a constant level of SCF throughout the study period was observed, concurrent with an increase in SCC during the unregulated post-GB period until 2005. This finding is consistent with the hypothesis that providers seek to maintain a target level of income, and, in the context of global budgets, respond by increasing discretionary billable SCC procedures to maximize their individual share of the region’s budget. Moreover, in 2007, providers limited SCC volumes to the 2005 level, consistent with the goals of the policy-enforced caps.
One could question why SCF volumes remained at pre-GB levels in the post-GB years despite the incentive to provide more services. Unlike industrial production, capacity for producing medical services is limited by the specialist’s fixed time resource. The observed increase in SCC with no changes in SCF is consistent with providers using available additional time (and patients) to produce higher revenue yielding services. Subsequently, the stagnation of SCC service volumes in 2007 without concurrent increases in SCF may attest to near saturation of providers’ time resource, and the poor incentive to invest extra effort in more SCF services given its low reimbursement rate. Consistent with our conceptual framework, SCC volume increases were particularly high in highly competitive markets. Another important finding consistent with a conclusion of incentive-driven provider behavior is that for-profit entities show higher volumes relative to public and non-profit clinics. This is especially notable with SCF claims. In addition, confounding between clinic type and ownership may be allowing clinic type to capture some of the ownership effect in respect of SCC claims. Higher SCF claim volume by for-profit clinics suggests some unnecessary services provided, reflecting possible social welfare loss, as well as the limitations of public policy in improving market efficiency beyond a point.
One potential confounding factor could be changing demographic composition over time, particularly population aging, and differential changes across markets. Mitigating this concern is the policy of the NHI Bureau, to allocate the national global budget cap among the six NHI administrative regions by adjusting for regional demographic composition, using a complex, historic utilization-based algorithm. 13 Thus, all clinics within a region face the same cap and the same demographic distribution, the demand-side variable. We used the HHI index of market competition to adjust for the role of supply-demand dynamics within a market. Data on demographic distributions within each HHI region are not available, and HHI regions are not contiguous with the NHI administrative regions. Inability to adjust for demographic composition is a study limitation. However, a review of the overall population change in Taiwan during the study period reveals patterns that support our conclusions.
The appendix table shows the age-sex distribution of Taiwan’s population in the 3 study years. The population aged above 50 years has the highest risk of eye disease and degenerative conditions, accounting for the most demand for eye care services worldwide.19,20 This age group increased from 20.7% of the 2000 population to 24.9% of a slightly larger 2005 population, and 26.7% of the 2007 population. This represents a 20% increase between the pre-GB and post-GB, pre–SCC cap periods, and further by 7.3% between the pre–SCC cap and the post–SCC cap years. These increases were accompanied by a 2.5% increase in 2005 SCF claims over the 2000 level (133 107 mean points increase in 2005 over the 2000 mean clinic points of ~5 360 000, see Table 2 and Figure 3) and a 37.1% increase in SCC claims (724 952 increase over the 2000 mean clinic total of 1 950 000 points, see Table 2 and Figure 1). The observed changes in service volumes relative to at-risk population volumes reflect that clinics disproportionately increased the high-revenue SCC services relative to the increase in at-risk population. Concurrently, there was a disproportionately low (statistically negligible) change in SCF claims. These findings support our conclusions.
In summary, provider behavior is found to be consistent with the predictions of the tragedy of the commons theory under global budget constraints concurrent with a fee-for-service reimbursement system. First, SCC volume increased while SCF volume remained constant from 2000 to 2005. Then, following the imposition of volume controls on SCC as a percentage of a clinic’s total claimed points in 2005 and 2006, the growth in SCC service volumes stopped between 2005 and 2007.
Our findings suggest that in global budget environments, payers should monitor all the relevant service categories with potential for substitution. For example, a study in Germany showed that the apparent savings from implementing a pharmaceutical sector GB were actually transferred to other service areas (patient referral to specialists or hospitals that had no such caps), resulting in higher total costs to the health system. 21
The current study also shows that combating service distortions resulting from perverse economic incentives under global budgets remains a difficult challenge for insurance administrators. To expect physicians to self-regulate and constrain services to the level of the population’s need is unrealistic when economic incentives promote a game-theoretic tragedy of the commons outcome. Future studies should address whether payers can permit the floating point value to fall as service volume rises without endangering the population’s health status. To meet these diverse goals, payers need to regulate specific types of service in partnership with medical experts and professional associations.
The findings of the present study are consistent with the experimental results of an earlier study. The impact of expenditure caps and expenditure targets on hypothetical service volumes were tested in a college classroom game. 22 Under both mechanisms, the objective was to keep the total expenditure equal to the total premiums collected during the current year. In the expenditure target experiment, each student (hypothetically a physician) was assigned to perform at fixed fee rates a fixed quota of services. If their actual services deviated from the quota, their individual fees were proportionately adjusted. Under the alternative mechanism of the expenditure cap, a total monetary budget was established across all players for a given period, without individual quotas. Each player was reimbursed at a common unit price determined by the total budget divided by the aggregate points accumulated by all players. Students responded to the collective expenditure cap (similar to Taiwan’s GB) with higher service volumes than under an expenditure target. Thus, players maximized income under an individual expenditure target by controlling service production. However, under a collective expenditure cap, each player has no control over other players’ response, and they respond by maximizing market share by over-providing services, even if doing so reduces the marginal income for each item of service provided.
Conclusions
Our study extends the findings of earlier studies from Taiwan that showed increases in overall service volumes with GB (increased inpatient volumes following hospital GB,5,15 and increased outpatient volumes following clinic sector GB 16 ). We explored service volume and composition changes within a single specialty, and found evidence of displacement of provider efforts to more profitable services. Furthermore, our study finds that co-option of professional associations is effective for regulating medical services. The study does not, however, establish whether the observed increases are welfare enhancing (increasing patient utility) or socially harmful (iatrogenic harm from unnecessary services). Future studies should focus on the health outcome impact of Taiwan’s global budgets.
Footnotes
Appendix
Population Distribution by Age and Gender in Taiwan, 2000, 2005, 2007 (% of Total).

| Age (years) | Gender | 2000 Pre-GB | 2005 Post-GB and pre–service cap | 2007 Post–service cap |
|---|---|---|---|---|
| 0-10 | Male | 7.27 | 6.07 | 5.49 |
| Female | 6.67 | 5.56 | 5.02 | |
| 10-20 | Male | 8.06 | 7.31 | 7.34 |
| Female | 7.53 | 6.75 | 6.76 | |
| 20-30 | Male | 8.66 | 8.67 | 8.20 |
| Female | 8.31 | 8.31 | 7.88 | |
| 30-40 | Male | 8.74 | 8.10 | 8.12 |
| Female | 8.45 | 7.94 | 8.05 | |
| 40-50 | Male | 7.90 | 8.26 | 8.25 |
| Female | 7.74 | 8.13 | 8.15 | |
| 50-60 | Male | 4.29 | 5.84 | 6.49 |
| Female | 4.30 | 5.89 | 6.59 | |
| 60-70 | Male | 3.17 | 3.16 | 3.22 |
| Female | 3.24 | 3.41 | 3.47 | |
| 70-80 | Male | 2.39 | 2.41 | 2.34 |
| Female | 1.92 | 2.27 | 2.41 | |
| >80 | Male | 0.65 | 0.95 | 1.10 |
| Female | 0.70 | 0.95 | 1.09 | |
| Total % | 100.00 | 100.00 | 100.00 | |
| Population | 22 276 672 | 22 770 383 | 22 958 360 |
Note. GB = global budgeting.
Acknowledgements
The authors are grateful to National Health Research Institutes and Bureau of National Health Insurance of Taiwan for preparing and providing the de-identified data set.
Author Contributions
Dr Chang conceived the study and conducted it as part of his doctoral dissertation research, as well as drafting the manuscript. Dr Sudha Xirasagar directed the research to develop the study design, conduct analyses, interpret the finding, and revise the manuscript drafts. Dr Hussey provided statistical direction and support in addressing the study hypotheses. Dr Wang acquired the data set from the National Health Insurance and participated in study design. Mr Chen conducted statistical analyses and Dr Ie-bin Lian was involved in the writing and revising of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.