
Abstract
Adolescent substance use is influenced by social support and social norms, which can be protective or risk-enhancing. This study analyzed survey data at baseline and 6-month follow-up from 919 adolescents attending schools on or near the Cherokee Nation Reservation. Generalized linear mixed-effects models assessed the influence of social support from parents/caregivers, teachers, community adults, and peers on alcohol and cannabis use with tests of moderation by injunctive and descriptive norms. Results revealed significant moderation in four of ten models. Parental support had stronger protective effects on alcohol use when parental disapproval was high, and teacher support had stronger protective effects on cannabis use when adult disapproval was high. Community adult support consistently protected against cannabis use. In low-normative contexts, friend support was a risk factor for alcohol use. Findings show the complex interaction of social support and norms with source- and substance-specific effects alongside implications for theory and prevention.
Introduction
The social environment—family, peer, and school dynamics—shapes adolescent substance use (Trucco, 2020). Social norms are especially powerful. The Theory of Triadic Influence (TTI) and Integrated Behavior Model (IBM) together frame how social norms influence behavior (Flay & Petraitis, 1994; Montano & Kasprzyk, 2015). TTI’s social environment “stream” emphasizes how social bonding (akin to support) and perceived norms may influence substance use via mediators like intentions and decisions (Flay, 1999; Flay & Petraitis, 1994). IBM and norm-focus theory distinguish descriptive norms (perceived prevalence) from injunctive norms (perceived approval/disapproval), both tied to adolescent use (Cialdini et al., 1991; Elek et al., 2006; Montano & Kasprzyk, 2015).
Social support is a consistent protective factor for American Indian (AI) youth, and low support is a risk factor for severe outcomes (Bush & Qeadan, 2020; Hodgson et al., 2022). A study of Anishinaabe/Ojibwe, Dakota/Lakota, and other Tribal youth linked social support from family and community with fewer mental health problems and showed its protective effects against risky behaviors (Ersan & Rodriguez, 2021). The Asdzáán Be’eená intervention for young girls in Navajo communities improved social support and relationships with caregivers along with reducing internalizing symptoms (Chambers et al., 2021). Interviews with Indigenous youth in Canada revealed that supportive relationships serve as an important pillar of coping (Lys, 2018). Positive relationships with family, characterized by support, care, warmth, and communication, have also protected against adverse outcomes for Indigenous youth (Burnette & Figley, 2016; Hodgson et al., 2022).
Though generally protective, social support from distinct sources may function differently for adolescents from rural reservation-based communities like the Cherokee Nation Reservation. For example, among Yup’ik adolescents, connection to adults and Elders associated with community and family protection against suicide and substance use, while connection to peers did not (Philip et al., 2016). Distinct people within an adolescent’s social environment may impart distinct norms and social support as youth grow, develop, face hardship, and resist or succumb to pressures. Social support from peers might manifest as density or strength of support that builds camaraderie through shared experiences (e.g., classrooms, extracurricular activities, peer pressures). Inuit youth identified secure and stable peer relationships as important to resilience (Kral et al., 2014). However, it is possible that if these relationships are with peers who regularly use substances, such social bonds foster increased substance use, especially when support from adults is lacking (Wills & Vaughan, 1989).
Injunctive norms (e.g., perceived parental and peer approval of substance use) and descriptive norms (e.g., parental and peer substance use) have been associated with adolescent substance use (East et al., 2021; Hawkins et al., 1997; Pedersen et al., 2017). Perceived parental or peer approval of youth substance use is a key factor distinguishing adolescents who abstain, experiment, or regularly use substances (McMaster & Wintre, 1996). Both types of norms have predicted later use of alcohol, tobacco, and cannabis among high schoolers, with peer descriptive norms maintaining significant effects over time (Cherry, 1991; Eisenberg et al., 2014). Perceived peer use may more strongly predict substance use than objective measures (Iannotti et al., 1996). In contrast, perceived parental approval may more strongly predict adolescent use than parental use itself (Eiser et al., 1989), a nuance that suggests source-specific variation in effects.
While general patterns of social norms and substance use are documented, it is crucial to consider context and influences among rural reservation-based youth who experience disproportionately high rates of drug-related harms and have distinct historical, cultural, and social dynamics relating to drugs and alcohol (Frank et al., 2000; Gone et al., 2019; Herman-Stahl et al., 2003). Among AI youth, peer substance use and low family disapproval have been associated with greater opioid misuse, while peer and grandparent disapproval have associated with lower substance use (Martinez et al., 2015; Nalven et al., 2020). Social norms have therefore been targeted by prevention strategies. Commonly, interventions aim to educate and improve the accuracy of normative beliefs and have effectively reduced alcohol and cannabis use among young people (Bewick et al., 2008; Neighbors et al., 2010; Pischke et al., 2021).
However, much of the literature has focused on urban, university, and/or non-Indigenous youth, despite high rates of drug-related harms among rural and AI adolescents. Place and culture are relevant factors to social dynamics and adolescents’ sense of social belonging, especially where Tribal identity and culture are foundational to community and relational worldviews (Gone, 2009; Masotti et al., 2020; Snowshoe et al., 2017). Social support and health-promoting norms could serve as protective factors, offering promising avenues for targeted interventions to improve outcomes (Burnette & Figley, 2016).
Opportunities for intervention at school and family levels could be powerful; school connectedness and family communication have buffered against detrimental effects of adverse childhood experiences and could mitigate adverse effects of risky norms (Clements-Nolle et al., 2022). Given some inconsistent or divergent effects of injunctive and descriptive norms depending on source (e.g., parents vs. peers), it is possible that social support’s effects similarly vary.
As such, the study’s objective is to examine whether effects of social support on substance use vary across levels of social norms among adolescents attending high schools on or near the Cherokee Nation Reservation. Self-reported survey data from adolescents at baseline and 6-month follow-up were analyzed. Hypotheses are:
Although norms and support were both from baseline, we specified norms as moderators based on both theory and measurement considerations. Theoretically, social norms represent broader, more distal influences in the social ecology, whereas support reflects proximal relational dynamics. This framing is consistent with TTI’s emphasis on normative context shaping the impact of proximal influences. Practically, norms were measured categorically, which facilitated moderation tests examining whether the effect of support varied across distinct normative contexts.
Methods
Data, Setting, and Sample
Data come from the Connect trial, a two-arm cluster randomized controlled trial evaluating a combined school- and family-based substance use prevention intervention compared to a delayed-intervention control in rural communities on and near the Cherokee Nation Reservation. The broader study protocol (which includes detailed consent procedures) and this manuscript were approved by the Cherokee Nation IRB (Komro et al., 2022). All students enrolled in the 10th grade across 20 high schools were surveyed using electronic tablets during school hours in the fall of 2021 (baseline) and again 6 months later in the spring of 2022 (follow-up). Out of 1,063 eligible students, 919 provided survey data at baseline, and 929 provided data at follow-up. A total of 836 students provided data at both time points. Non-response was attributable to parent refusals, student refusals, undeliverable parent consent forms, absenteeism, and virtual school attendance.
The complete intervention is described thoroughly elsewhere along with baseline statistics on relevant variables (Komro et al., 2025). The intervention included (1) the Connect Brief Intervention, a motivational-interviewing digital tool delivered semesterly by trained coaches in schools, and (2) Connect Kits for Family Action, mailed to parents/caregivers across 3 years with developmentally appropriate, culturally grounded prevention content. Schools were randomized using constrained randomization to balance community characteristics. Intervention activities began during spring of 2022, after the baseline survey and concurrent with the follow-up survey in a few of the 10 schools. Because little intervention activity had occurred by this early time point, intervention effects were nonsignificant, but trial condition was included as a covariate for rigor. Baseline characteristics and follow-up response rates were comparable across intervention and control groups (Komro et al., 2025).
Predictors and hypothesized moderators were collected at baseline and included social support (from parents/caregivers, teachers and other adults in school, adults in the community, and friends), injunctive norms (of parents/caregivers, adults in the community, and peers), descriptive norms (of peers), and covariates. Outcomes assessed at follow-up were past 30-day use of alcohol and cannabis. Univariate and bivariate analyses were conducted to check frequencies, distributions, and assess missingness within participants and across waves prior to multiple imputations.
Measures
Social Support
Social support was measured using a 6-item scale about support from different sources in the adolescent’s life. Support was measured separately for each source (parents/caregivers, friends, teachers or other adults at school, and adults in the community) in parallel format. The survey asked, “In my family, there is a parent or caregiver who. . .,” “Among people my age, I have a friend who. . .,” “At my school, there is a teacher or some other adult who. . .,” or “In my community, there is an adult (other than at my school or a parent/caregiver) who. . .,” followed by six items: “really cares about me,” “tells me when I do a good job,” “notices when I’m not there,” “always wants me to do my best,” “listens to me when I have something to say,” and “believes that I will be a success.” Responses were rated on a 4-point scale: 0 = never, 1 = rarely, 2 = sometimes, 3 = often. Social support from parents/caregivers, teachers, adults in the community, and friends were calculated as means of the six items for each source, with possible scores ranging from 0 (minimum) to 3 (maximum). Psychometric testing of the social support scale and subscales in this sample yielded Cronbach’s alpha estimates ranging from .87 to .96, indicating good to excellent internal consistency (Livingston et al., 2023). The overall social support scale showed small but statistically significant criterion and predictive validity with a substance use index based on past 30-day use of alcohol, cannabis, and off-label prescription opioids, with slight variations among subscales by race/ethnicity, which may indicate differences in support among youth across races/ethnicities (Livingston et al., 2023).
Injunctive Norms
Injunctive norms were operationalized as perceived disapproval from different people: parents/caregivers, adults in the community, and peers. Perceived disapproval from parents/caregivers was assessed with a single item asking, “Do your parent(s)/caregiver(s) disapprove of young people doing each of the following? Drinking alcohol?” and “Using marijuana?” For each substance, respondents indicated perceived disapproval on a scale of 1 to 3, where 1 = don’t disapprove, 2 = disapprove, and 3 = strongly disapprove. This format was mirrored to assess perceived disapproval from “adults in your community” and “people your age” (peers). Cronbach’s alphas for injunctive norms related to alcohol use and cannabis were 0.70 and 0.74, respectively, indicating acceptable internal consistency in this sample. Criterion and predictive validities with the aforementioned substance use index were small to moderate in the expected direction with no variation by race/ethnicity (Livingston et al., 2023). For analysis, injunctive norms were modeled separately by relationship type; each was tested in interaction with its corresponding source of support (e.g., parental disapproval with parental support).
Descriptive Norms
Descriptive norms were normative estimates of peer use of alcohol and cannabis. For alcohol use, these were assessed with a single item that asked, “How many people your age in your school have drank alcohol in the past year? Would you say. . .” Respondents indicated their estimates on a 5-point scale: 1 = none or almost none, 2 = less than half, 3 = about half, 4 = more than half, and 5 = almost all or all. For cannabis use, normative estimates were assessed with a similar item: “How many people your age in your school have used marijuana in the past year? Would you say. . .” using identical response options. As descriptive norms data were available only for peer use, the interaction examined peer injunctive norms and peer descriptive norms as moderators in separate models. Cronbach’s alpha for this measure was .73 (acceptable). Criterion and predictive validities were small but statistically significant in the hypothesized direction (Livingston et al., 2023).
Substance Use
Alcohol use was measured with a single item asking, “During the past 30 days, how many days did you drink alcohol?” Cannabis use was measured with a similar item that asked, “During the past 30 days, how many days did you use marijuana?” Respondents indicated their frequency of use on each item as an integer from 0 to 30 days.
Covariates
Covariates were drawn from baseline survey data. These included age, gender, enrollment in a free or reduced-price lunch program (an indicator of socioeconomic status), race/ethnicity, baseline alcohol or cannabis use, and prevention trial group assignment. Trial condition was included to conservatively account for early implementation in a few schools. The peer injunctive norms model further adjusted for descriptive norms (normative estimates of peer use) and vice versa to distill the effects of the focal norms moderator for the relevant model. Covariates were selected based on theory and evidence showing that both social support and substance use vary by age, race/ethnicity, gender, and socioeconomic status, and that substance use at different time points is strongly correlated (Elek et al., 2006; Livingston et al., 2023; Runarsdottir & Vilhjalmsson, 2015; Smith et al., 2017; Swaim & Stanley, 2020; Vaux, 1985).
Analytic Approach
Generalized linear mixed-effects models were used to examine interactions between social support and social norms on substance use outcomes. Poisson regressions were used to predict past 30-day alcohol use and cannabis use, as these outcomes are count data skewed toward zero. Multiple imputations (m = 30) were used to address missingness, chosen for its flexibility for handling different types of missingness mechanisms (Li et al., 2015). Each model included a distinct source of social support (parent/caregivers, teachers, adults in the community, or friends), as well as its paired injunctive norms moderator (when applicable; e.g., parental support by parental disapproval). Peer descriptive norms and peer injunctive norms were modeled separately and tested as moderators of friend support. Because support and norms were measured concurrently, moderation tests should be interpreted as theory-informed conditional associations rather than evidence of causal ordering. Regression models to test

where log(Y) represents the outcome with a log() link function, β0 is the intercept, β1 and β2 are the coefficients for the exposure variables social support (X1) and social norms (X2), β3 is the coefficient for the interaction term between social norms and social support, and βp represents the coefficients for other covariates included in the model. Where interactions were significant, we probed simple slopes of support at each level of the dichotomous norms variable and graphed these conditional estimates in Figure 1. Interaction tests are reported in text. Interaction terms were removed when found to be non-significant to obtain main effects estimates of social support and norms (
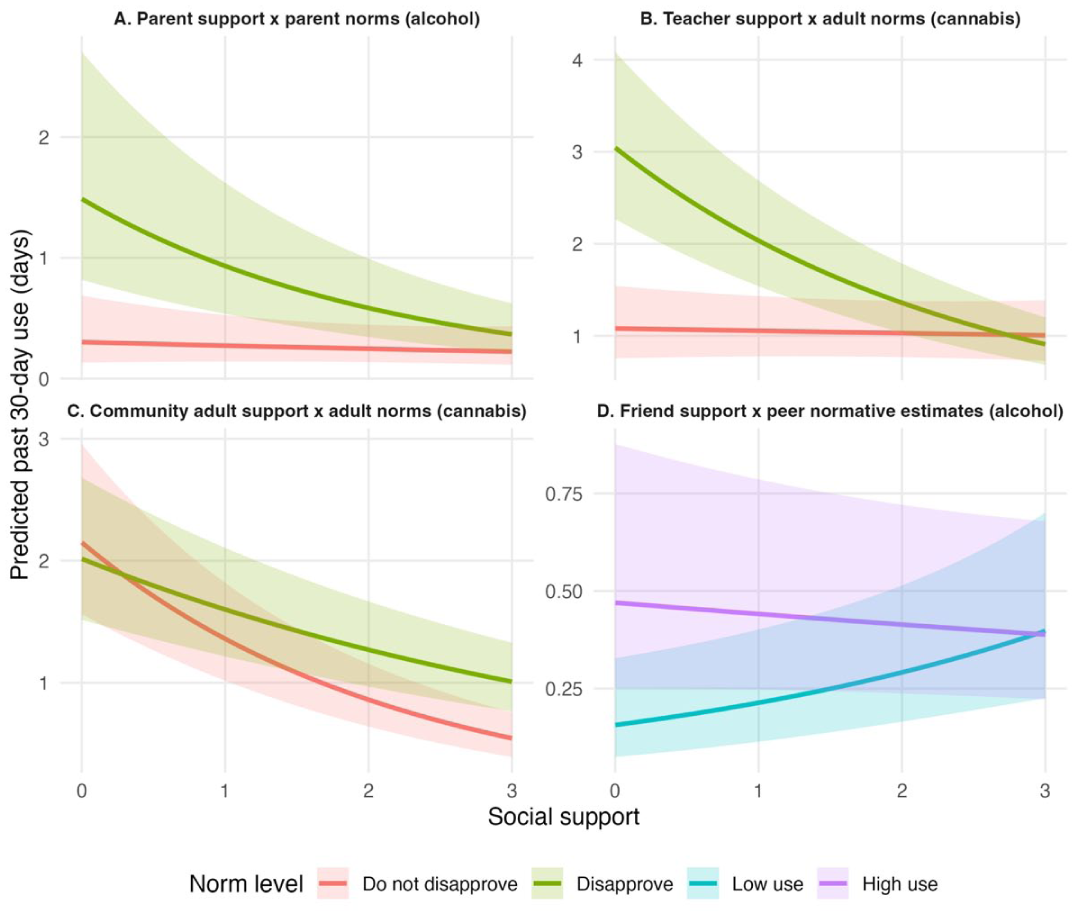
Predicted past 30-day alcohol and cannabis use by social support and norms. Notes: Panels show significant interactions of (A) parent support x parent disapproval on alcohol use, (B) teacher support x adult disapproval on cannabis use, (C) community adult support x adult disapproval on cannabis use, and (D) friend support x peer descriptive norms on alcohol use. Lines depict fitted values with 95% confidence bands. Estimates are conditional simple slopes derived from interaction models, visualized on a representative imputed dataset (imputation 1).
Adjusted Regressions of Main Effects on Alcohol and Cannabis Use in Models Without Significant Interactions (n = 919).
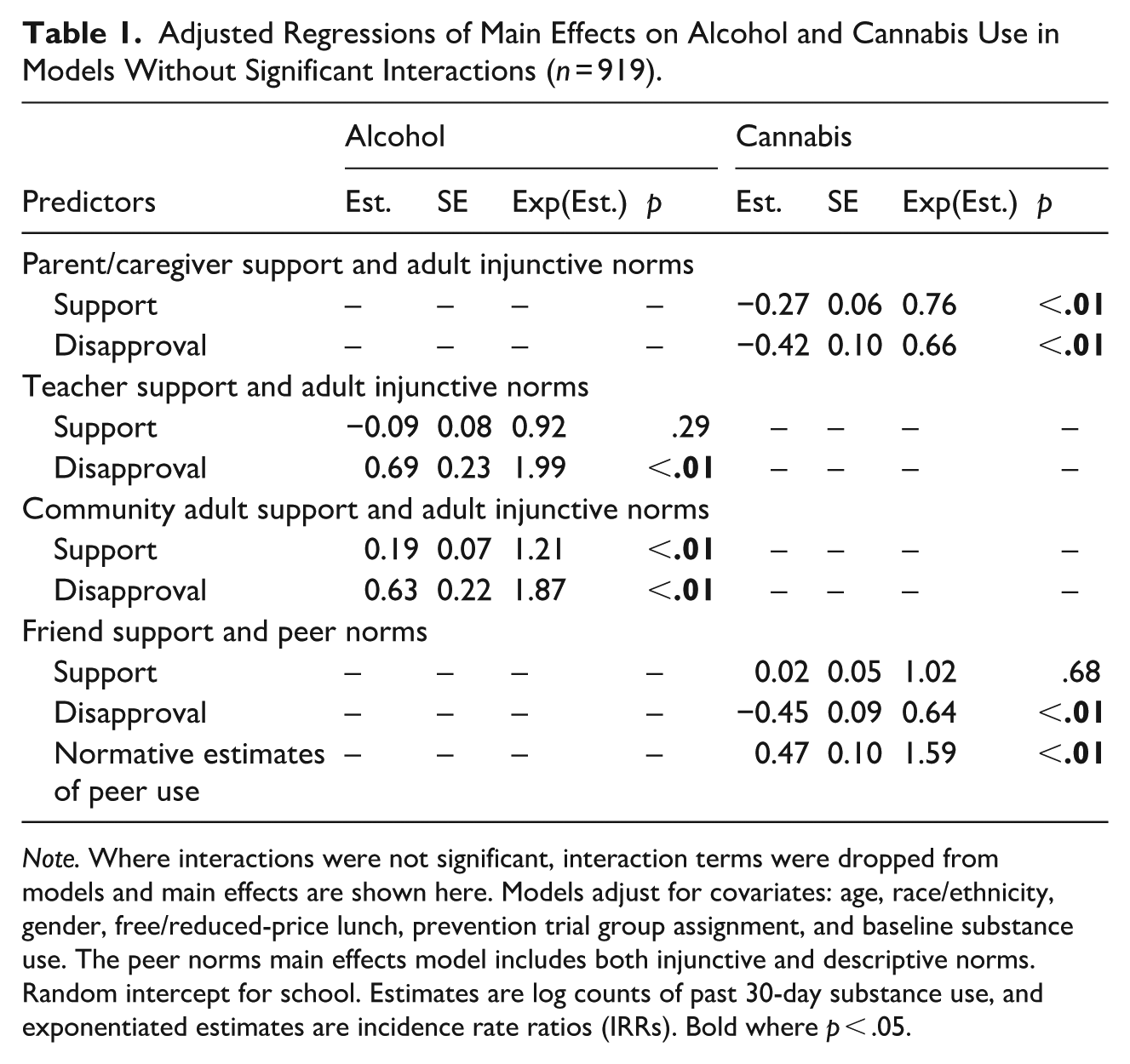
Note. Where interactions were not significant, interaction terms were dropped from models and main effects are shown here. Models adjust for covariates: age, race/ethnicity, gender, free/reduced-price lunch, prevention trial group assignment, and baseline substance use. The peer norms main effects model includes both injunctive and descriptive norms. Random intercept for school. Estimates are log counts of past 30-day substance use, and exponentiated estimates are incidence rate ratios (IRRs). Bold where p < .05.
Results
Descriptive Statistics
At baseline, 95% of respondents were 15 or 16 years old, nearly half identified as female, and 74% reported receiving free or reduced-price lunch at school. On race/ethnicity, 29% identified as AI only, 35% as White only, 27% as AI and one or more additional races/ethnicities, and 9% as another race/ethnicity. Mean social support scores ranged from 2.16 (SD = 0.94) to 2.53 (SD = 0.59) across different sources. Injunctive norms measures showed that the vast majority of adolescents perceived adults as disapproving of substance use (89%–91%), while a minority perceived their peers as disapproving (40%–41%). For peer descriptive norms, 62% and 54% of respondents estimated that at least half or more of their peers had used alcohol and cannabis respectively in the past year.
Regressions
Results from the regression analyses showed that effects of support on substance use varied by social norms in four of the ten models: parents/caregivers (alcohol), teachers (cannabis), adults in the community (cannabis), and peers—descriptive norms (alcohol).
Parents/caregivers
In the adjusted parent/caregiver alcohol model, we observed a significant interaction effect between parent support and parent disapproval on alcohol use that aligned with our hypothesis (
Teachers
In the adjusted teacher model, we observed a significant interaction between teacher support and adult disapproval on cannabis use, consistent with our hypothesis (
Adults in the Community
In the adjusted community adult model, we observed a significant interaction between community adult support and disapproval on cannabis use that did not align with our hypothesis (
Peers
In the adjusted peer alcohol model, we observed a significant interaction between friend support and normative estimates of peer alcohol use that contradicted our hypothesis (
Main Effects
Table 1 presents the main effect estimates where interaction terms were dropped due to non-significance. Significant main effects on cannabis use outcomes aligned with our hypothesis (
Significant main effects on alcohol use outcomes were contrary to our hypothesis (
Discussion
This study explored interactions between social support and social norms on substance use among adolescents attending high schools on or near the Cherokee Nation Reservation. Results partially supported our hypotheses and added nuance to understanding social influences on alcohol and cannabis use in this population. Findings indicate areas for further research and theory development and provide contextually grounded evidence that may inform prevention efforts via positive social influence.
Consistent with
In the community adult/cannabis model, support was protective across disapproval strata, though stronger when disapproval was low. We caution against overinterpretion, as the discrepancy may be minimal in practice.
In contrast, the peer model of descriptive norms on alcohol use revealed a significant interaction that contradicted
Other unmeasured factors, such as network characteristics, personality traits, coping, or socialization patterns might also affect relationships between support and substance use (Brechting & Giancola, 2007; Ennett et al., 2006; Gunnarsson et al., 2008; Lyness & Koehler, 2016; Shin & Miller-Day, 2017; Wills, 1987). Family dynamics, neighborhood characteristics, and exposure to substance advertising might also play a role (Cambron et al., 2020; Shih et al., 2019; Trucco, 2020). Relationships are likely complex and multifaceted, involving nonlinearities, mediating or moderating effects of unmeasured variables, or differential effects across subgroups (Flay, 1999; Flay & Petraitis, 1994). Future research could explore further by incorporating network factors, such as centrality, density, size, homophily, strength of social ties, and cliques—all of which have been linked to youth substance use and targeted in network-based interventions (D’Amico et al., 2023; Ennett et al., 2006; Hussong et al., 2018).
Limitations
Limitations should be considered in light of findings. First, measures of social support and norms were designed to monitor risk and protective factors of substance use—not to examine their interaction or test causal hypotheses. Peer norms measures may have captured collective norms at a broader level than within a person’s immediate social group, which could misalign with the source of friend support, as discussed. Because both support and norms were measured at the same time, we cannot determine their causal ordering in moderation analyses. Second, users and non-users might be qualitatively different; mixture models might be more appropriate to handle zero-inflated outcome distributions. However, given the trial design for primary prevention, all adolescents in this study were considered qualitatively similar. Additionally, the survey captured perceptions but did not manipulate or test how salience of norms might alter perceptions or behaviors, a key component of Cialdini’s focus theory of normative conduct (1991). Experimental or quasi-experimental approaches could provide insights into causality and mechanisms by which norm salience amplifies protective effects. Finally, a larger sample would be needed for subgroup analyses. For example, the majority of students perceived adult disapproval, while only 9% to 11% perceived adults as “not disapproving,” which may limit power to detect interaction effects in some models.
Theory Development and Prevention for Reservation-Based Youth
One of the strengths of TTI and IBM is their applicability to understanding substance use behavior across contexts (Flay & Petraitis, 1994; Montano & Kasprzyk, 2015; Nyambe et al., 2016; Talip et al., 2016). However, the social, cultural, and environmental factors that influence youth living in rural or reservation-based settings suggest areas where theoretical refinement may be valuable. TTI’s social environment “stream,” which describes the role of social norms and bonds/support, was useful framing for this study but could be adapted to better capture the distinct cultural norms and multigenerational influences present in Indigenous communities. For instance, Elder influence and traditional cultural norms are underexplored in the extant literature but have been identified in emerging research as prevention targets for mental health and substance use among AI youth. Connection to Elders and cultural values play significant roles in shaping behavior, reinforcing norms, and providing social support (Brockie et al., 2022; Masotti et al., 2020; Woods et al., 2022; Yamane & Helm, 2022).
IBM’s contribution of descriptive and injunctive norms is relevant to AI youth given that community-level norms may reflect broader cultural and historical experiences of collective trauma, resilience, and identity (Skewes & Blume, 2019; Walters et al., 2011). It is possible that AI youth may be more responsive to community-level injunctive norms related to substance use when these norms align with cultural teachings about wellbeing (Halsall et al., 2022; Komro et al., 2023). Incorporating cultural dimensions into IBM’s framework could enhance its predictive power and relevance for AI populations. Understanding how traditional norms are transmitted and reinforced through cultural practices (e.g., ceremonies, language, and intergenerational knowledge sharing) could provide richer insights into mechanisms through which reservation-based youth resist or engage in substance misuse (Heid et al., 2022).
Given our findings, we present considerations for enhancing the relevance of TTI and IBM to AI youth. The social/normative stream of TTI aligns well with the community and family dynamics core to many Native cultures, where “the family unit” extends beyond a nuclear family to include Elders, extended family, and the wider community (Robbins et al., 2013; Woods et al., 2022). For AI youth, social norms are not only shaped by peers and parents but also by cultural leaders and practices (Robbins et al., 2013; Wexler et al., 2024; Woods et al., 2022). This study revealed strong protective effects of perceived parental disapproval, which could be expanded in future work to explore grandparental and community Elder disapproval, given their central role in AI youth upbringing and education (Gone, 2022; Momper et al., 2017; Wexler et al., 2024). Likewise, IBM’s norms could be developed to integrate how Tribal customs and community teachings function as a subtype of injunctive norms. For example, cultural prohibitions against alcohol and drug use that are grounded in spirituality could serve as powerful motivators for Native youth and offer additional protection. This would align with findings from other studies that have shown the protective role of cultural engagement and identity against substance misuse in AI adolescents (Brockie et al., 2022). On the other hand, cultural acceptance of plant-based and holistic medicine might attenuate perceived risks associated with cannabis use (Cates, 2024).
Additional directions for future research include testing moderation effects over longer time periods to assess the durability of these findings. Subgroup analyses might also reveal insights into moderated moderation, as substance use and its social determinants can vary by race/ethnicity, gender, and other factors. With a larger sample, future studies could test for effects among subgroups, which would be important for optimizing universal prevention strategies versus tailored interventions.
Conclusion
This study explored the interactions between social support and social norms on adolescent substance use within rural reservation-based communities. Using survey data from adolescents attending school on or near the Cherokee Nation Reservation, we tested for moderation of social support on alcohol and cannabis use by social norms. Our findings partially supported hypotheses to reveal a more nuanced picture of social influence: the protective effects of social support on substance use can significantly vary by social norms, with distinct patterns across sources of support and types of norms. This study advances our understanding of the social determinants of adolescent substance use in a reservation-based context. Findings indicate opportunities for prevention efforts to support the wellbeing of reservation-based youth.
Footnotes
Acknowledgements
Thanks to the students, families, and schools who engaged with us in research to inform prevention efforts for community health.
Ethical Considerations
This study was approved by the Cherokee Nation Institutional Review Board (IRB), with protocol number #334. Emory University and Cherokee Nation signed a Reliance Agreement, designating Cherokee Nation as the IRB of record for the project.
Consent to Participate
Parent/guardian consent was obtained using a passive consent process, whereby parents/guardians received mailed consent letters describing the study and were given the option to opt out by returning a prepaid postcard or contacting the research team via a toll-free number. Students provided written assent before participation, and participation was voluntary, with the option to withdraw at any time. The Cherokee Nation IRB also reviewed and approved this manuscript for publication. A model consent form is available upon request.
Consent for Publication
Not applicable. This manuscript does not include any data from individual persons that requires consent for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute on Drug Abuse (NIDA) of the National Institutes of Health (NIH) through the NIH HEAL Initiative (UH3DA050234) and training grant T32DA050552. Revisions were completed after Dr. Barry moved to Dartmouth College with support from training grant T32DA037202. The results and opinions expressed therein represent those of the authors and do not necessarily reflect those of NIH or NIDA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated and analyzed during this study are not publicly available due to restrictions from the Cherokee Nation IRB, which prohibits public sharing of Tribal data. However, de-identified datasets may be made available upon reasonable request to the corresponding author, contingent on approval from the Cherokee Nation IRB.