
Abstract
Globally, youth have high rates of unmet mental health needs, especially in Majority World contexts. Youth themselves are well positioned to engage their peer group in mental health provision. The aim of this study was to explore how peer educators could co-produce and deliver mental health promotion in resource-constrained South Africa communities. Six peer educators aged 18 to 24 initially co-facilitated consultation with 209 youth, before designing and delivering three mental health promotion workshops to 179 youth. Peer educators and 21 workshop beneficiaries participated in focus groups on their experiences. Key findings related to involving youth by integrating mental health to community activities, using participatory approaches, applying and transferring knowledge, signposting for further help, and putting support mechanisms in place. In conclusion, youth hold unique expertise in mobilizing their peer group and promoting mental health. Peer educators should be incorporated in service systems, with allocated budgets, training, supervision.
Introduction
It is widely established that youth across different cultural contexts worldwide have high rates of unmet mental health needs, evidenced by policy and epidemiological research (World Health Organization, 2020). These needs increase at least twofold with socioeconomic disadvantage and inequalities, because of the multitude of associated risk factors (Pearce et al., 2019). Identified reasons for not receiving timely and appropriate mental health support include stigma of mental health, adult-centric—thus non-engaging—services, and insufficient resources (Zhou et al., 2020). These factors are compounded in Majority World Countries (MWC), as interventions are often not culturally and contextually informed, and available professional skills are limited further (Patel et al., 2018).
In recent years, mental health concepts have become broader, shifting away from more medicalized notions of disorders or illness, to encompass positive functions and resources to face daily life challenges. A positive outlook toward mental health was found to be endorsed by youth in several MWC (Renwick et al., 2022). Such positive conceptualization is essential for the design of youth mental health promotion programs, and for their inclusion in school curricula. Indeed, several such school or community-based initiatives were shown to improve awareness, problem-solving strategies and help-seeking (Eustache et al., 2017; Leventhal et al., 2022).
Engagement, uptake and implementation to mental health promotion initiatives is enhanced when local stakeholders and communities are actively involved in its co-production and delivery. In relation to mental health, such process facilitates the development of culturally appropriate interventions and services, and the implementation of solutions through locally relevant and contextualized actions (Abayneh et al., 2020). Co-production with youth can create dialogical spaces for power redistribution (Norton, 2021) through creative and youth-friendly approaches (Brooks et al., 2021). Equalizing power dynamics and decision-making between researchers and community members (or experts by experience) can be facilitated through participatory research processes that involve critical reflection, systematized experiences and learning, and collective analysis (Mathias et al., 2020). This is especially important for resource-constrained and rural settings, with limited access to mental health services (Abayneh et al., 2020).
This evidence on potential benefits of mental health promotion in MWC is largely based on delivery by mental health or other professionals such as teachers or community workers. The increasing emphasis on youth as unique holders of knowledge on their own needs, provides opportunities for peer-to-peer mental health promotion and support (Marinucci et al., 2022). When faced with concerns about their mental health, youth are more likely to share those with their informal support networks, especially their peer group (Heerde & Hemphill, 2018). Enabling factors include common lived experience, developmental stage, mutual support, and perceived safety (Lubman et al., 2017). For this reason, there has been value in involving youth in mental health care settings in various roles such as peer educators, mentors, advisers, or support workers. Peer educators usually promote mental health by providing information and psychoeducation to targeted groups, while peer support workers have a more active responsibility of providing advocacy and delivering or co-facilitating first-level response for individual youth (De Beer et al., 2023; King & Simmons, 2022; Simmons et al., 2023).
Indeed, previous research indicates that peer educators can have positive impact on youth recognition and disclosure of mental health problems (Boucher et al., 2022), although findings remain inconclusive on other outcomes. In MWC, peer educator roles have been reported within programs that promoted wellbeing along multiple domains (Rose-Clark et al., 2019), or that targeted health issues such as nutrition and sexual reproductive health (Kitelele et al., 2022; Singhal et al., 2010). These interventions were associated with improved understanding and awareness of recipients, and parallel personal growth reported by peer educators themselves (Singuti et al., 2019). In contrast, there is less knowledge on how youth can promote positive mental health among their peers and communities in MWC.
Peer education and support have often been conceptually informed by a youth-focused explanatory theory, the Positive Youth Development (PYD) framework. This framework advocates that, when youth engage in reciprocal, constructive relationships with individuals and organizations in their social environment, they are more likely to thrive (Lerner et al., 2005). The PYD framework is particularly important in designing programs for marginalized youth groups in MWC, by providing opportunities for youth voices to be heard (Lerner et al., 2020). Such programs were shown to promote agency, skills-building, confidence, sense of belonging, emotional support and peer relationships, including through role models such as mentors (Olenik, 2019). For example, peer educators facilitated a life skills program with youth in South Africa, and this was found to improve self-efficacy, self-esteem and personal growth (Page et al., 2023).
In summary, there is increasing emphasis of youth facilitating or delivering programs that aim to enhance awareness, knowledge and skills along different wellbeing domains. There is, however, less evidence on which factors enable youth-led mental health promotion in MWC resource-constrained settings. This gap informed the rationale for this study. The aim was to explore the process of youth-led mental health promotion in disadvantaged South African communities. A mental health program was thus co-produced and delivered by youth, to youth from the same communities. In this paper, we address two research questions:
(a) How can youth, as peer educators, promote mental health in disadvantaged South African communities?
(b) What types of support do peer educators need in this process?
Methods
We utilized a qualitative thematic design due to the exploratory nature of the research. Theoretically, the work was underpinned by a macro-social-constructionism epistemology, which centers on language and how social structures shape the social world (Lester & O’Reilly, 2018). This epistemology provides a focus on voice and young people’s personal accounts of their experiences as constructed through social interaction (Fraser et al., 2004) and is consistent with our explanatory theory of PYD that promotes marginalized youth voices being heard (Lerner et al., 2020). Such a theoretical foundation paves way for youth to exercise their agency in research as congruent with a children’s rights framework (Tisdall, 2015), while recognizing that there are broader structural and systemic influences on their generation of experiential meaning.
Context and Participants
This study was conducted in the context of a South Africa National Youth Service Program to provide skills and experience across different domains to unemployed youth aged 18 to 24 years that increase their employability and entrepreneurial skills (National Youth Development Agency, South Africa, 2023). Youth received training on topics such as healthy nutrition, early childhood development and environmental sustainability, and were offered placements to gain experience in community settings like schools and early childhood centers (Seriti Institute, 2023). Approximately 3,000 youth participated nationally and were allocated across provinces and localities. Of those youth participants to the program, a small number were recruited as ‘youth team leads’ to co-ordinate training and placements within each community.
The area of focus for the study was the City of Ekurhuleni, east of Johannesburg, in Gauteng. With a population of 3,774,638, this urban area includes five of the 20 most populated townships in South Africa and is representative of other disadvantaged urban communities (COGTA, 2020). This includes several townships with high concentration of informal settlements. These overcrowded communities have high levels of socioeconomic deprivation, poor sanitation and housing infrastructure, and limited access to health and welfare services (Marutlulle, 2019). Six of these communities participated in the study, Tsakane (population 200,000), Marikana (19,000), Mayfield (16,000), Daveyton (130,000), Windmill Park (30,000) and Wattville (26,000).
The study was hosted by a non-governmental organization (NGO), which provides psychosocial support to youth. One senior practitioner was responsible for peer educator recruitment and a youth care practitioner was responsible for training, supervision and organization of mental health promotion workshops. The youth team leads, who were already operating in the participating communities and had been assigned to the host NGO, were invited to additionally act as mental health peer educators. Of 12 youth team leads who initially agreed to be involved, six completed the training and co-facilitated mental health promotion workshops (four female, two male).
Peer Educator Mental Training and Pilot Youth Discussion Groups
Peer educators went through three stages of training with the local youthcare worker and the research team, during which they co-produced a range of materials and activities on mental health promotion to utilize within their communities. The research team combined psychology and psychiatry skills and helped to contextualize previously developed evidence-based training materials (Vostanis et al., 2019).
(a) Initially, peer educators received training on mental health concepts, risk and protective factors, and first-level mental health responses, which enabled them to co-design pilot mental health promotion workshops. This involved five meetings between the youthcare worker and the research team, and five intermittent weekly meetings with the peer educators, who decided on the delivery approaches for each workshop.
(b) Youth mental health discussion groups involved out of school youth aged 16 to 24 years from the participating communities, who were also participated in the National Youth Service Program. These group discussions then served as the pilot to the mental health awareness workshops. Youth were allocated to three discussion groups, each co-facilitated by two peer educators (identified above). Group discussions were approximately 4 hr long and included a number of activities related to mental health and wellbeing. The local youthcare worker and two members of the research team were present as well. They provided support and supervision, whilst also scoping youth responses and interactions, before providing feedback in a learning process.
A brief overview on mental health issues was followed by small group discussions. Youth were asked to define mental health, consider types of mental health difficulties, reasons for their development, strategies of ensuring positive mental health, and ways of engaging and educating communities. Following feedback and discussion, youth re-joined their small groups and co-produced youth mental health promotion concept notes according to a given template on objectives, key messages, target group, desired outcomes, delivery approaches, and logistics (venue, number of participants, duration). The resulting concept notes informed the next phase of peer educators co-designing the substantive workshops for youth in the communities. The numbers of participating youth and venue for the three workshops, respectively were 88 (community hall), 74 (church) and 47 (community hall), or total n = 209.
(c) Peer educators attended four further training sessions to reflect on their pilot experiences, challenges and recommendations; receive feedback and guidance on facilitation and delivery approaches; and delve in more detail into emerging mental health issues, including impact on their own mental health and self-care. Youth-produced concept notes largely focused on social issues facing them in the community, that is, tackling stigma, abusive environments, gender-based violence and drug use, keeping youth off the streets, enhancing gender equality, and instilling hope to parents and caregivers. During the final training phase, peer educators refined the mental health workshops, as described below.
Community Youth Mental Health Workshops
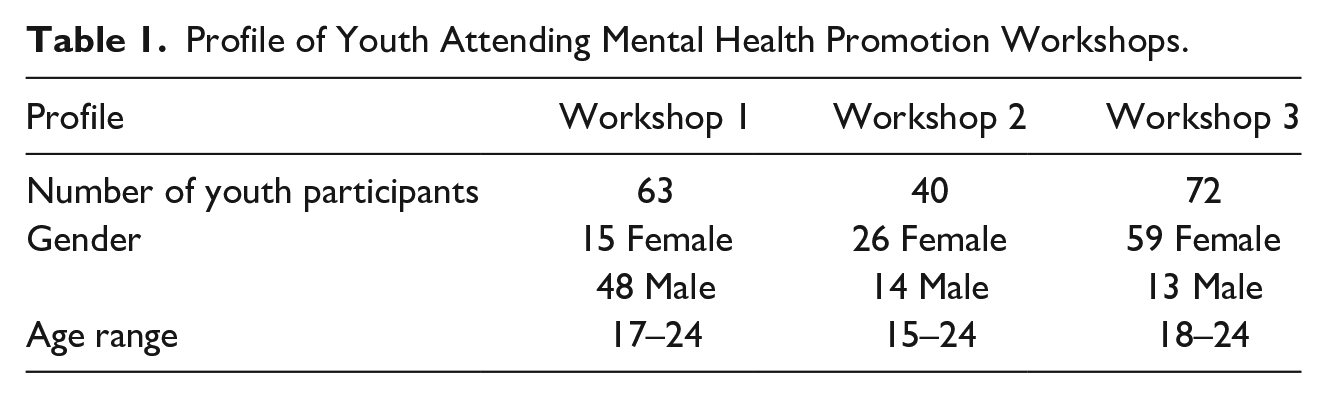
Peer educators met with teachers and community leaders in their preparation of the youth mental health workshops; ensuring that events were supported by these key role-players. Workshops followed a similar structure and duration as the pilot youth group discussions but used sports (football tournament) and creative activities (music, poetry) as mediums of engagement. Based on feedback from the youthcare worker, the local leaders and the research team, the key messages and topics were re-focused to the importance of positive mental health and wellbeing, awareness and recognition of emerging mental health difficulties, sharing and seeking help, and tapping into protective factors to enhance mental health and prevent difficulties. Each workshop involved youth from two communities and was co-facilitated by two peer educators. The supervisor and one more youth care worker from the host NGO were present at each event to answer any questions on service criteria. All workshops were held at community halls. In total, 175 youth attended three workshops. Their profiles are presented in Table 1 below.
Profile of Youth Attending Mental Health Promotion Workshops.
Data Collection Procedure
Five peer educators (four female, one male) and, through purposive sampling, a sub-sample of 21 youth (15 female, six male) who attended the three workshops (eight, seven and six youth respectively), were invited to attend focus groups to assess the perceived process and efficacy of the workshops. Focus groups engage participants in “collective conversations” in relation to their experiences, insights, and perspectives (Adler et al., 2019). These take the form of guided conversations that encourage self-disclosure and collaborative discussion in a safe shared space (Freeman, 2006). This is particularly important when involving marginalized groups such as youth from resource-constrained settings, whose voices are rarely heard (Onwuegbuzie et al., 2009), as focus groups can promote the empowerment of youth by confronting stereotypes and stigma, deepening our understanding of the contextual conditions facilitating empowerment, and promoting shared learning and collaboration (Hall et al., 2023).
The topic guide explored youth perspectives on ideas or challenges from the workshops, whether they shared any of these ideas with family or peers, whether they could lead mental health promotion events in the future and, if so, what support they might need. Peer educators considered aspects of the training they received, challenges in designing and delivering the workshops, process of learning, and recommendations for future scaling-up to enhance reach and impact. Each focus group was held at a community venue and was facilitated by an independent researcher. Discussions were in isiZulu and were audio-recorded. Ethics approval was granted by the Sociology Research Ethics Committee of the University of Leicester in the UK. All participants were aged 16 years and over and provided written informed consent.
Data Analysis
Transcribed data were translated from isiZulu to English. We utilized thematic analysis (Braun & Clarke, 2006), and particularly engaged with its codebook form. This allowed for conflation of inductive and deductive coding processes and ensured analyst collaboration and dialogue through a multiple coding process (Braun & Clarke, 2022). In practice, this meant that the initial coding framework was informed by an a priori engagement with the literature and initial codes were created. The inductive coding process followed the steps of Braun and Clarke (2019) and involved familiarization and coding using the words of participants, thematizing of clusters of codes, and a final mapping exercise to generate the codebook. Data were initially coded by one researcher and were revisited by a second coder to ascertain transparency and rigor in the process. One further independent researcher helped resolve any discrepancies through a dialogic reflexive process which facilitated the quality of the analysis and the promotion of transferability. This was an appropriate form of analysis, as thematic analysis centralizes the voices of participants, identifies patterns within and across data, and allows a synthesis of core messages for translation and interpretation.
Results
Participants reflected how learning from the workshops could be applied to promote youth mental health in similar communities. Key messages involved better understanding and recognition of mental health signs and underpinning factors, a more positive stance toward mental health, and relating mental health across their socioecology (self, family and community). They concluded with recommendations on how mental health promotion could be sustained by actively involving youth and mobilizing communities. The established themes and subthemes are summarized in Table 2. These are described in more detail, with representative supporting quotes.
Established Themes and Subthemes.

Theme 1: Awareness Process
Participants initially considered what enabled them to develop a different approach to mental health, so that they could transfer such learning to others. Some concepts were new, especially viewing mental health on a spectrum, rather than only focusing on disorders or illness. The universality of mental health need applying to all societal groups came as a surprise to some youth.
What I remember is that mental health affects all age groups. Yes, and it can be in a positive way or in a negative way, but generally, mental health affects everybody. (FG1, Youth 2) That mental health affects all age groups. . .also, that it doesn’t matter whether you are rich or poor, or white or black because, with most black people, you will think a person is sick, but they have mental issues. (FG3, Youth 1)
They did, however, acknowledge the influence on mental health of stressors from life circumstances, especially within their communities. Socioeconomic disadvantage and unemployment, which were the main criteria for joining the wider program, were major stressors for youth, including the peer educators. Such stressors are thus important to acknowledge in mental health promotion initiatives.
I think on my side, it’s the pressure because when they talk about unemployment, there’s also the pressure that comes with it. Because you’ll see something somewhere, the pressure starts after a while. It’s all about the environment around you. (FG4, Peer educator 1)
In contrast with stigmatizing attitudes, an improved understanding of mental health on a spectrum and underpinning psychosocial mechanisms that can threaten positive mental health can lead to acceptance and tolerance of people in their family or community. This can be achieved through emotional literacy and by giving a different meaning to behaviors such as anger or drug use.
You can tell by their behaviour and their actions. . .they fail to keep their emotions in check. (FG3, Youth 3) So, OK, this person is not talking to us, and then after two or three days, she won’t talk to us. She can go for two-three days, not talking to any of us. So, we understood. (FG3, Youth 3)
Sharing experiences could make mental health difficulties and threats to positive mental health more real. Nevertheless, it was acknowledged that opening up during mental health promotion events is difficult, particularly among young males, because of the fear of being judged by peers or adults, hence has to be anticipated and managed carefully.
The testimonies from other people. . .because you got to see, it's okay. I’m not going through this alone. (FG1, Youth 2) The hardest idea from the event today was when they told us you can talk to somebody. . .I think it was the hardest because most people, they were like, no, it's hard talking to somebody, because they will judge you. (FG1, Youth 6)
Youth thus sought reassurance of being in a safe space and having a degree of trust toward the mental health promotion facilitators and their peers. Peer educators tried to create a safe space, highlight the importance of confidentiality, and avoid discussing personal information beyond broad mental health issues, instead directing those participants to seek external help.
This is the story I wasn’t happy that she was sharing because it’s personal, but now I see that it is actually helping her. These events are helping us. The information we receive because they inform us and then we go and inform others. . .the communication, you see. (FG3, Youth 1) As long as I feel safe around you, I’m not worried about you judging me. . .obviously, I can’t just cry in front of anyone. There are those friends that you trust and that you feel safe around. (FG3, Youth 4)
Participants identified enablers in processing knowledge from the mental health promotion workshops. These included communication and interpersonal skills such as non-judgmental listening, empathy, and reflection.
I think it changed in a good way because I’ve learned to be more considerate about other people’s feelings and not to judge at first instance. I must get to understand their problem first before you judge. (FG1, Youth 2) I personally don’t reflect on myself, I reflect on others. (FG2, Youth 3)
Other perceived outcomes involved being more active and problem-solving, especially jointly with their peers.
On my side, I think that the event that we had helped me to realize that teamwork is important. After the presentation, we started playing soccer. So, you cannot play soccer alone, and you cannot score alone. So, at the same time, you need to depend on someone because you cannot succeed alone. And then with the discussions I learnt that maybe my idea is important, and your idea is important but together the two ideas when you combine them, they are better. (FG2, Youth 7)
Peer educators described needing to feel empowered, self-reflect, have a positive mindset and grow in confidence before feeling ready to facilitate mental health promotion workshops. They worked as a team in supporting each other throughout this learning.
You know, there are some things that can make you angry, yeah, like it forces you to show a side of you that you don’t want to show, but as I got training, I realized that I didn’t know how to control myself. (FG4, Peer educator 4)
Theme 2: Application of Knowledge
Youth participants reported how they had applied new knowledge from the mental health promotion workshops in their everyday lives. To this effect, they applied lessons to protect and improve their own wellbeing, shared learning with peers and family, and considered informal and structural types of support.
So, it shows me how my positive side leads to my mind and how my negative side leads also to my mind. So, the training has helped me, because I can see a difference on my positive side and my negative side. (FG4, Peer educator 5) It doesn’t mean that change was good. Some of it may have been negative, you know, you didn’t like it. It’s really important to understand differently. (FG1, Youth 7)
The most common application of new knowledge was in developing more adaptive coping strategies in dealing with everyday stressors. Peer pressure was widely mentioned in the youth context of the mental health promotion workshops.
I think about that point when they spoke about peer pressure, because I used to have a lot of peer pressure, and then when I got there, I got to learn about ways of dealing with it. Like you shouldn’t allow people to pressurize you about things that you are not comfortable doing, so that point really stood out for me. So, now I don’t feel like I am pressurized or I’m facing peer pressure. I feel like I am on the right track. (FG3, Youth 2)
Several participants felt confident enough to share new knowledge with family and friends. This related to looking differently at mental health issues and trying to understand reasons behind their development and generating strategies when faced with stressors.
What I share with my family is that, if you feel that you are over-stressed, you have to try to calm down and to relax, so that the stress that you have cannot lead to depression. . .when you see that you are stressed, you have to exercise, try to do something that will help you de-stress. (FG1, Youth 2) I shared with my friends and my family that someone with a mental health problem may not always display it, because people have different ways of dealing with stress. . .so, you find that some people drink a lot, but it might not be because of that. It could be because they have problems that they are not able to talk about at the time. (FG1, Youth 6)
Despite the positive perceptions of acquiring new knowledge, youth still faced negative attitudes in the community following the workshops. Another challenge was that awareness was not sufficient for those requiring more active mental health support.
They told me that it’s not true [that mental health is real]. (FG1, Youth 5) So, my friend realized that they might have a mental disorder, so then we went back home and discussed where she can get help from, and then we decided that she should speak to a social worker. (FG2, Youth 6)
Information on seeking further help is central to mental health promotion. However, this was beyond the remit of peer educators, at least during this time-limited project. For this reason, two youth care workers attended the workshops to signpost any youth expressing more serious mental health concerns.
I used to think that when you are going through a situation, you need money to get help, but then I learnt that no, there are places that can help you for free. (FG3, Youth 5) . . .who should we refer them to if there is someone who needs some help? (FG4, Peer educator 4)
Theme 3: Sustainability
Feedback from participants suggested that the mental health promotion initiative was positively received but not considered sufficient to enhance reach and sustain benefits. Participants explored what systems should be put in place to make this possible. Their recommendations included ways of engaging youth and communities, integrating mental health to physical and social activities, and extending and supporting the peer educator role. Youth were viewed as being central to this process, although they suggested that mental health promotion should also be extended to all age groups.
I think we need to make sure that we get the youth for the events because, as the youth, we are going through a lot of things, and we don’t open up. So, I think as the youth, it is important that we do something and make sure that we attract the youth to attend the event, and then it will help change things a lot. (FG1, Youth 3) So, I will need flyers, the venue, and I think that’s all, but the challenge that I might have is to gather people because some of people wouldn’t understand the reason for this event and how it will impact their lives. So, it will be a challenge to gather people as much as I can, but it’s better to try. (FG1, Youth 4)
Ways of making mental health promotion more engaging included the careful use of language and running events in busy public spaces. They indicated that these events should be regular, so that communities could get used to them, as indicated by reports of “word-of-mouth” following the workshops. Previous health promotion initiatives such as on HIV and sexual and reproductive health had taken some time before being established and accepted.
Maybe if we want to make this thing viral, maybe we can do it like those that make awareness about HIV and all that stuff. Maybe we could go to the mall with our stuff, we can organize a few people and ask them if we can have a bit of their time to talk about mental health. (FG4, Peer educator 4)
Above all, youth valued the involvement of peers with lived experience. They also felt motivated if their peers demonstrated confidence and openness in talking about mental health.
It’s better if someone is going through this thing and can tell you how they overcame it this way and that way. So, I think it’s better that way, because then people will know that they can take the necessary steps. (FG3, Youth 2) [Name], the first time when we were doing the groups and talking about the topics like he wasn’t talking, but I think him going to the front and representing the group. I think he was more open than when he was in the group because he didn’t talk at all. To say that this is how it is, but when he went to the front, he was able to express it in a way that people can understand what he is talking about. (FG4, Peer educator 5)
Participants largely stated a preference for mental health promotion to be incorporated in activities rather than through stand-alone presentations or discussions. They made the link between mind and body, hence related mental health promotion to meeting basic needs or exercising, albeit within their peer group rather than individually.
You can’t educate an empty stomach. If somebody is worried about what they’re going to eat at the next meal, you can’t help those kind of people, because that thing is going to come in and go out simply because they are hungry. (FG1, Youth 7)
Youth were innovative in their thinking, working around stigma by finding subtle ways to promote mental health. Sports (football, netball) and creative activities (dance, music, indigenous games) were viewed as more acceptable, enabling engagement through fun, entertainment and social participation while sharing important messages.
We tried to think about everything, and then we found what would be entertaining for the guys. There was football, there was music, and then the others watched the football, so what we thought was a challenge wasn’t really a challenge. (FG4, Peer educator 5)
Youth felt they could contribute to future mental health promotion by sharing what they already learnt and because they could engage their peer group. They also expressed doubts though on whether they would be taken seriously, because of their age, coming from the same communities, and lack of professional status.
I think I could do it by sharing my experiences and the things that I have been through. It has changed us. (FG3, Youth 4) I think I could help those that are the same age as me, because older people will just see me as a young person and might not feel comfortable sharing their feelings with me. So, they would need someone who is older and has more experience. (FG1, Youth 8)
Peer educators shared their own experience of going through similar ambiguity in delivering mental health promotion. Their training and supervision helped them focus on their remit without delving into professional roles, whilst understanding and being proud of their unique strengths.
Then there are those that don’t really want to listen to us because we are not professionals, and we are not fully those types of people. . .undermining you. (FG4, Peer educator 4) In terms of being professional during that event, there was a time where the boys were trying to understand more about me. . .so, mentally, I already have training. So, I don’t have to explain myself to them, so long as they accept me the way I am. So, I have to live with that. So, for me, in terms of my mental, it is important that I don’t take it personally. I have to be professional while I am still working on gaining more knowledge. (FG4, Peer educator 8)
This led to several suggestions on the types of support peer educators would require ensuring they could extend and sustain their role in mental health promotion. Input from professionals was the main requirement for ongoing training supervision, mentorship and information on local services. Observing professionals whilst delivering mental health promotion would help peer educators anticipate challenges.
Maybe if we could have some professionals or maybe people that are more educated about mental health, so that they could give more information to the community. (FG3, Youth 3) Can he [supervising professional] just tell us what challenges he gets and how he solves them, so that when we have a future event, we can know how to solve it? (FG4, Peer educator 5)
Youth also mentioned resource issues to enable future mental health promotion in the community. An easily accessible and safe venue, support materials like posters or fliers, promotion resources like t-shirts (such as those worn by peer educators during this project) and sponsorship were a few of these suggestions. Overall, youth and peer educators wished to be given tools and support that showed that they were valued by professionals and communities.
We need someone who is going to motivate us, “we know you can do it”. So, someone who is going to give us that thing. We also need to be reminded that we are important. (FG4, Peer educator 5)
Discussion
This study explored how youth mental health could be promoted through a peer-to-peer model in disadvantaged South African communities, by eliciting both peer educator and participant experiences and perspectives. Co-production with peer educators and including youth in the design and delivery of mental health promotion was central to this approach that addressed previously elicited gaps in youth mental health promotion programs that were often adult-led and top-down. Key findings reported in this paper related to youth engagement and mobilization in mental health promotion and sharing messages such as tackling stigma with communities. The need to put supports in place for youth-led mental health promotion to be sustained through integration with service systems was also discussed.
This youth-led approach to mental health promotion addresses current global priorities by international organizations for developing and strengthening youth-for-youth psychosocial support systems through collaborative efforts (UNICEF, 2022). Co-production is particularly important in resource-constrained MWC settings and with marginalized groups (Abayneh et al., 2020). It is also aligned with a decolonizing mental health care framework of empowering youth, alleviating stigma, contextualizing the understanding of mental health and mental health problems, serving the needs of local communities, and opening new avenues for low-cost mental health care and prevention (Alemu et al., 2023).
Youth are uniquely equipped to understand stigmatizing attitudes toward mental health, underpinning reasons for these beliefs, how mental health needs are related to social adversity, the context of youth and communities, and how their generation are more likely to seek help (Leventhal et al., 2022). To this effect, participants spoke of the need to acquire more knowledge and skills, and of the value of connecting with their peers through mutual understanding and shared beliefs. Such a youth-led model of mental health promotion in MWC resource-constrained settings is also consistent with the Positive Youth Development Framework (PYD), in particular with its five central tenets of competence (managing one’s life), confidence (positive sense of self and self-efficacy), connection (positive relationships), character (values that guide one’s behavior), and caring (empathy and desire to help others in need; Lerner et al., 2005). Positive outlooks to mental health and wellbeing can be integrated with wider health, welfare and life skills promotion programs, as demonstrated in the PYD literature (e.g., Page et al., 2023).
Youth established key ingredients of mental health promotion in recognizing, processing, managing (self-care), and seeking help for mental health problems across socioecological systems (Bronfenbrenner, 1979). To this effect, several youth applied new knowledge to generating individual coping strategies, and shared learning with their family, peer and community networks, which were still characterized by stigmatizing and adult-centric views. Indeed, evidence indicates that mental health promotion and prevention should aim to build resilience across systems, as these are inter-linked, especially in MWC resource-constrained settings, where it is difficult to disentangle youth mental health from basic and social care needs (Ungar & Theron, 2020).
Another objective of mental health promotion is to initiate help-seeking for those youth with more complex mental health needs. Globally, studies consistently found that youth are more likely to initially seek information and help from informal youth-centric (peers, web-based) rather than structural adult-centric sources (professionals, services; Heerde & Hemphill, 2018; Van Breda & Theron, 2018). In previous studies in several MWC resource-constrained settings, including South Africa, we found that children and youth relied on individual and relational psychosocial support, but had limited information on structural support (Haffejee et al., 2023; Vostanis et al., 2022). As indicated by our youth participants, understanding of mental health issues, recognition and help-seeking are closely related. Peer educators are thus more likely to initiate, facilitate and guide care pathways, whilst operating as links between informal and structural support. As insiders, youth can foster peer relationships and trust more readily than ‘authoritative’ adult professionals.
Nevertheless, youth voices need to be centered but also to be supported, to be heard and make sustainable impact. Peer educator posts should not be short-term or provided in silo from psychosocial services. These should be embedded within comprehensive (rather than the currently fragmented) systems, resourced and adequately supported with spaces, supervision and training. As reported by peer educators in this study, they went through a parallel process of learning and personal growth with youth community participants, albeit during a short period, of challenging their own beliefs, and assimilating a large body of knowledge and skills, before cascading to their peer group (Simmons et al., 2020). Their remit should be delineated from providing safeguarding or psychological interventions, but with seamless access to social work or mental health professional skills respectively. These boundaries from providing individual help and maintaining confidentiality, can be particularly challenging when peer educators and end-users live in the same communities. Peer educators raised the importance of feeling valued, and this highlights the need for professionalization of their role by policy and services, without losing their unique strengths (Viking et al., 2022).
The findings should be interpreted within the limitations of this study. The sample of communities and youth participants were not necessarily representative of other South African, indeed MWC, contexts. However, the six participating communities were characterized by multiple and inter-linked socioeconomic risk factors reported in most MWC resource-constrained inner-city settings (COGTA, 2020). In this study, peer educators were selected from an existing pool of youth team leads as part of a national youth unemployment initiative (National Youth Development Agency, South Africa, 2023), hence we could not apply mental health experience criteria, for ethical and logistical purposes. Involvement of youth with mental health lived experience as peer educators would have provided a powerful perspective for the workshops. The peer educators’ training and facilitation of mental health promotion workshops was time-limited, as this was part of research project rather than a statutory initiative. A longer period may have enabled peer educators to embed lessons from their peers in updating content and delivery approaches and may have provided the opportunity to integrate mental health promotion within local services. These issues could be addressed by future research, for example by in including rural communities, cross-cultural MWC settings, and at least a sub-sample of peer educators with lived experience. Future studies could measure changes in attitudes, knowledge and service activities such as the number and reasons for youth seeking help following the mental health promotion workshops. They could also tackle systemic issues by incorporating youth-led mental health promotion within a comprehensive service model, and thus develop a Theory of Change that could be generated to other contexts.
In summary, youth have an invaluable and unique role in promoting and supporting mental health within their peer group and community, and in preventing the development of mental health difficulties. This role is even more pertinent in MWC, where mental health resources maybe often limited, but informal psychosocial support networks are central to youth wellbeing and help-seeking. Youth-led mental health promotion approaches need to be implemented in different settings and over longer periods. Peer educators should be integral to comprehensive psychosocial service systems, with designated support mechanisms.
Such integration can be resource-effective within public health and welfare policy, rather than as random response to emerging needs, thus more engaging to youth and communities. Uptake can be enhanced if individual and collective realities, including those of peer educators, are taken into consideration, for example by linking mental health promotion with the policy initiative to tackle youth unemployment in this study. Youth-informed and participatory delivery approaches are more likely to meaningfully engage youth, as experienced by our participants. Furthermore, the active engagement of youth leading mental health promotion can lead to innovative ways to reach out to communities, through creative techniques and sometimes subtle initiatives.
Footnotes
Acknowledgements
We are grateful to all young people who participated in the study, especially to the peer educators. We thank Kids Haven NGO in South Africa and John Twishime for facilitating this project.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was funded by an Economic and Social Research Council Partnership Grant.
Author Biographies
![]() ), which provides capacity-building, service transformation and evaluation for children in contexts of conflict and disadvantage.
), which provides capacity-building, service transformation and evaluation for children in contexts of conflict and disadvantage.