
Abstract
Using a three-wave (mean age 14.4, 17.4, and 20.4 years) longitudinal design (N = 1,834; 55.6% females), we set out to map direct and indirect effects of adolescent peer victimization and mental health on academic achievement in early adulthood, and the buffering effect of positive family relations. Data was collected in Sweden 2012 to 2018. We found concurrent (βs = .13–.28) but no longitudinal transactional effects between peer victimization and symptoms of depression, anxiety, and conduct disorder (CD). Peer victimization, depression, and CD had longitudinal direct effects on poorer academic achievement in early adulthood (βs = .09–.11). Positive family relations did not moderate the effects. The results indicate that prevention and interventions against peer victimization and poor mental health may contribute to a higher proportion of individuals graduating from high school.
Introduction
Adolescence is an important transition period between childhood and adulthood, characterized by increased independence from parents, elevated influences from peers, and increased emotional vulnerability (Sawyer et al., 2012). The transition involves a series of developmental changes and tasks to be accomplished, and experiences during adolescence often have an impact well into adulthood (Schulenberg et al., 2004). One important marker of successful transitioning into early adulthood is to graduate from high school. This is a requisite for entering higher education, and dropping out of school is associated with a wide range of detrimental outcomes including lower income, criminality, health problems, and higher societal costs (Rumberger, 2011; Sörberg Wallin et al., 2019). There are many potential obstacles to efficacious transitioning, such as peer victimization and ill mental health (Agnafors et al., 2021; Rumberger, 2011).
Peer victimization concerns systematic abuse of power and is defined as repeated exposure to verbal and/or physical violence (Olweus, 1994). Peer victimization is common, with a childhood prevalence of 30% and has a negative impact on adult adaptation and physical and mental health (Wolke & Lereya, 2015). Poor mental health may in turn increase the risk of being subject to peer victimization, and there are indices of this for both internalizing (e.g., depression and anxiety) and externalizing symptoms (e.g., conduct problems) (Vaillancourt et al., 2013; van Lier et al., 2012). Depression and conduct problems have been linked to poorer grades, whereas the role for anxiety seems more complex (Agnafors et al., 2021; Duncan et al., 2021; Erskine et al., 2016). A large meta-analysis found that the effect of peer victimization on concurrent academic achievement was significant yet small (Nakamoto & Schwartz, 2010). As for longitudinal effects, a large cohort study found effects of childhood victimization on different aspects of education in early adulthood (Wolke et al., 2013). Especially those who were both exposed to peer victimization and bullied others were at heightened risk for poor academic achievement (Wolke et al., 2013), suggesting that externalizing symptoms may play a role.
The combined long-term effects of peer victimization and mental health problems on academic achievement need further scrutiny. That is, peer victimization may increase symptoms of depression, anxiety, and conduct problems, in accordance with the interpersonal risk model (Davis et al., 2019), which in turn could affect future academic achievement negatively. The opposite effect may also be present. Specifically, poor mental health may increase the risk of exposure to peer victimization, as suggested by symptom-driven models (Davis et al., 2019), which could negatively influence future academic achievement. Presence of both of these effects would suggest a transactional model where peer victimization and poor mental health are reciprocally exacerbating each other across time (Davis et al., 2019), with joint or indirect effects on academic achievement. A transactional model was examined for peer victimization and depression in a 2-year, three-wave longitudinal study in middle childhood and revealed both direct effects of peer victimization on poor academic achievement, and indirect effects through levels of depression (Liu et al., 2018). Similar associations, including also externalizing problems, were found in 6 to 8-year-olds (van Lier et al., 2012) and middle childhood (Totura et al., 2014; Vaillancourt et al., 2013). However, none examined these effects into young adulthood.
As adolescence is a period with increased influences from peers in combination with heightened emotional vulnerability, adolescents may be at elevated risk for negative effects of peer victimization compared to younger children (Troop-Gordon, 2017). To complicate the picture, effects of peer victimization and experiences of poor mental health on academic achievement may be moderated by other factors. For example, having positive family relations may buffer against the negative effects of peer victimization (Hansen et al., 2012), which have been shown in relation to maladjustment (Stadler et al., 2010) and substance use (Vannucci et al., 2021). There are also indications that parental support and school involvement moderate the association between peer victimization and academic achievement during elementary school (Fite et al., 2014) and early adolescence (Rothon et al., 2011). To our knowledge, the direct and indirect effects of adolescent peer victimization and mental health problems into early adulthood and whether positive family relations moderate them have not been examined. Mapping such association may in turn inform our understanding of adolescent development in general. For instance, regarding concurrent and longitudinal effects and what mechanisms may underpin stability and change. Within the design of a prospective research program following a cohort of Swedish adolescents up to young adulthood in three waves, we saw an opportunity to rectify the limitations in previous studies. We set out to:
Map concurrent and longitudinal associations between peer victimization and mental health problems in adolescence and their direct and indirect effects on academic achievement in early adulthood.
Examine the potentially buffering effects of positive family relations.
We expected to find longitudinal effects of peer victimization and mental health problems on academic achievement. Due to the lack of studies targeting adolescence, we did not specify whether these effects would be direct or indirect. We expected that positive family relations would buffer against the negative effects of peer victimization and mental health problems.
Material and Methods
Participants and Procedure
Participants include N = 1,834 adolescents (males n = 814, 44.4%) who responded and provided written informed consent at the three data waves included in the current study. Eighty-one percent of the sample were of Scandinavian origin (i.e., one or both parents were born in Scandinavia). Of the fathers, 10.6% were born outside of Europe, as were 10.2% of the mothers. The participants were recruited to a prospective cohort study, the Survey of Adolescent Life in Västmanland (SALVe) (Vadlin et al., 2015). In 2012, all adolescents born 1997 or 1999 and living in Västmanland, Sweden were contacted by mail to request participation in the study. Initial response rate was 40% and 1,834 adolescents participated at wave (W) 1 (mean age = 14.4 years; SD = 1.0). Follow-up was conducted three (W2; response rate n = 1,644; 89.6%; mean age = 17.4 years; SD = 1.0) and six (W3; n = 1,212; response rate 66.1%; mean age = 20.4 years; SD = 1.0) years later.
Dropout analysis using t tests to compare those who had valid data at all three waves to those who did not, showed mostly small but significant differences regarding peer victimization at W1 (m = 5.71 vs. m = 5.95, p = .001); conduct disorder (CD) at W1 (m = 4.77 vs. m = 5.96, p < .001), CD at W2 (m = 6.00 vs. m = 7.66, p < .001); positive family relations (m = 28.49 vs. m = 27.83, p = .016); and socio-economic status (SES; m = 3.92 vs. m = 3.70, p = .006). Those who had non-complete data had higher ratings of peer vitimization and CD and lower ratings of positive family relations and SES. Further, chi-square tests showed that those with valid data at all three waves to a higher degree were females (62.7 vs. 47.5%, p < .001) and had completed high school with approved grades at wave 3 (W3; 85.5 vs. 70.2%, p < .001) compared to those who did not.
The research was conducted in accordance with the Declaration of Helsinki and approved by the regional ethics board in Uppsala, Sweden (Dnr: 2012/187).
Measures
Peer victimization
Participants reported on peer victimization at W1 and W2 through an adapted version of Alsaker and Brunner’s bullying questionnaire (Smith et al., 1999). The constructors added a question about cyber bullying to the original scale, resulting in 5 items concerning victimization during the last school year (Kanders et al., 2022): “being reluctant to go to school due to fear of getting into trouble”; “being exposed to physical violence”; “being teased, accused for things s/he has not done, threatened, or called names”; “being lied to, slandered, or ignored”; or “being cyber bullied”. The items were rated on a scale from 1 (“never”) to 4 (“at least once a week”). Factor analysis (principal components, eigenvalue >1, varimax rotation) suggested one component of peer victimization (Kanders et al., 2022). We used the sum of all items as a measure of peer victimization. Cronbach’s alpha was α = .65 (item correlations r = .25–.60) for W1 and α = .68 (item correlations r = .46–.57) for W2.
Depressive symptoms
We used the Depression Self Rating Scale, Adolescent version (DSRS-A; Sonnby et al., 2022) to assess symptoms of depression at W1 and W2. The DSRS-A consists of 15 questions regarding depressive symptoms corresponding to the DSM-IV criteria A for major depression disorder. The participants responded yes or no to each item. Number of endorsed symptoms (0–9) constituted our measure of depressive symptoms. Cronbach’s alpha was α = .80 for W1 and α = .83 for W2. A score of 5 and above indicates clinical depression (Sonnby et al., 2022).
Symptoms of anxiety
We used the Spence Children’s Anxiety Scale (SCAS; Olofsdotter et al., 2016; Spence, 1998) to assess symptoms of anxiety at W1 and W2. The SCAS consists of 44 items on a scale from 0 (“never”) to 3 (“always”), of which 6 are positive filler items to reduce negative bias and 38 correspond to indices of anxiety. We used the total score (i.e., the sum of the 38 anxiety items) as a measure of symptoms of anxiety. Cronbach’s alpha was α = .91 for W1 and α = .92 for W2.
Symptoms of conduct disorder
To assess symptoms of CD at W1 and W2, we used a delinquency scale (Andershed et al., 2002) adapted for the current study (Åslund et al., 2011; Isaksson et al., 2020), to correspond to the DSM-IV criteria for CD, including aggressive behavior, vandalism, deceitfulness or theft, and norm-breaking behavior. The participants rated 26 items (e.g., “Have you broken the rules in school?” and “Have you taken money at home, that weren’t yours?”) on a scale from 0 (“never”) to 4 (“more than 10 times”). We used the sum of all items as a measure of conduct symptoms. Cronbach’s alpha was α = .79 for W1 and α = .81 for W2.
Positive family relations
We used the subscales Warmth, Structure, and Autonomy support from the Parents as Social Context Questionnaire (PASCQ; Skinner et al., 2005) to assess positive family relations at W2. The three subscales consist of 12 items in total on a scale from 1 (“does not apply at all”) to 4 (“definitely applies”), such as “my parents let me know they love me” (Warmth), “when I want to do something, my parents show me how” (Structure), and “my parents trust me” (Autonomy support). We used the sum across all items as an index of positive family relations. Cronbach’s alpha was α = .84.
Academic achievement
Academic achievement at W3 was assessed by having the participants indicate whether they had finished high school with complete grades or not (1 = yes; 2 = no).
Covariates
Academic achievement W1
The adolescents reported on academic achievement at W1 by indicating number of failed marks (1 = none, 2 = 1–2, 3 = 3–4, and 4 = 5 or more).
Socio-economic status
Parents reported on highest levels of maternal and paternal education at W1 (1 = elementary school, 2 = vocational high school, 3 = high school, 4 = non-university post-high school education, 5 = university < 3 years, and 6 = university degree). If available, we used the mean of both parents’ highest education as a proxy for SES.
Analytic Strategy
IBM SPSS Statistics 26 was used for preliminary analyses and the lavaan package in R was used for the path and moderation analyses (Rosseel, 2012). Multiple imputation, using predictive mean matching (PMM; Kleinke, 2017) with the mice package in R, was used to account for missing data. In a first step, we conducted bivariate correlations on non-imputed data for descriptive purposes and to confirm the theoretical associations between the constructs of interest. After that, structural associations between the constructs (see Figure 1) were examined using path analysis (Streiner, 2005). Chi-square, the root mean square error of approximation (RMSEA), comparative fit index (CFI), and Tucker–Lewis index (TLI) were used as model fit indices. A non-significant chi-square, CFI > 0.90, TLI > 0.95, and RMSEA < 0.08 indicate good model fit. Sex, age, academic achievement at W1, and SES were included as covariates. We present regression parameters and R2 to depict explained variance. In a separate multi-moderation regression model, positive family relations were explored as moderator in relation to academic achievement at W3. Interaction terms between positive family relations and all predictors (peer victimization at W1, peer victimization at W2, depression at W2, anxiety at W2, and CD at W2) were included, controlling for the other constructs and the covariates. The interaction terms were then excluded in a stepwise procedure in which we step-by-step excluded the least significant interaction term (Holmbeck, 2002). p Values <.05 were regarded as significant.
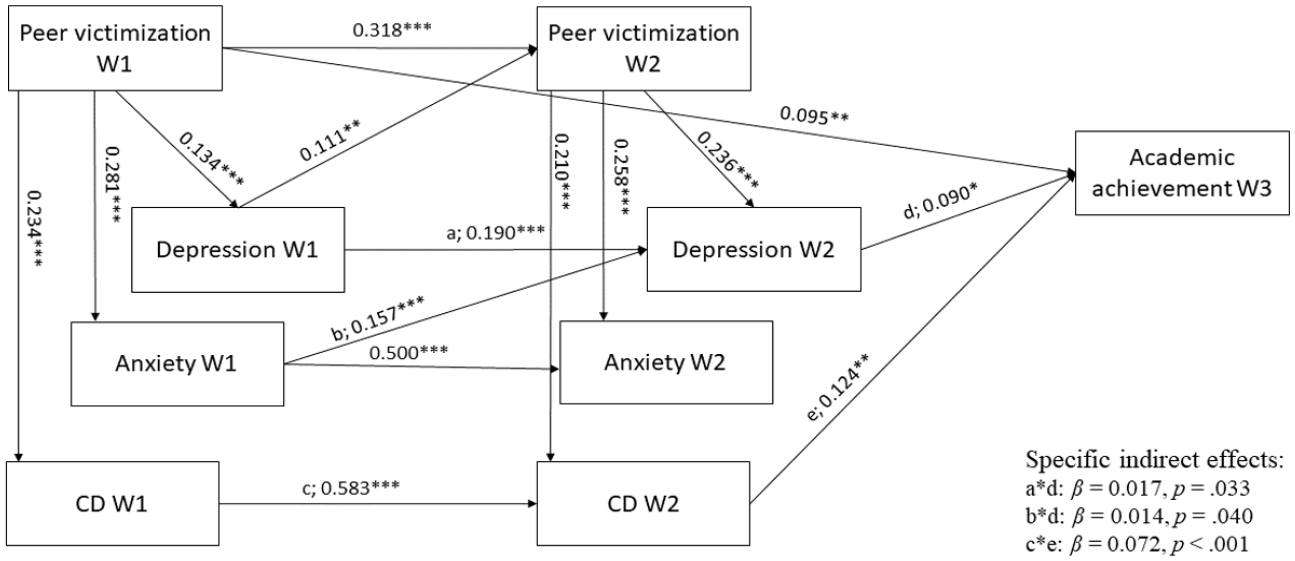
Path diagram with depiction of statistically significant standardized estimates for direct and indirect effects.
Results
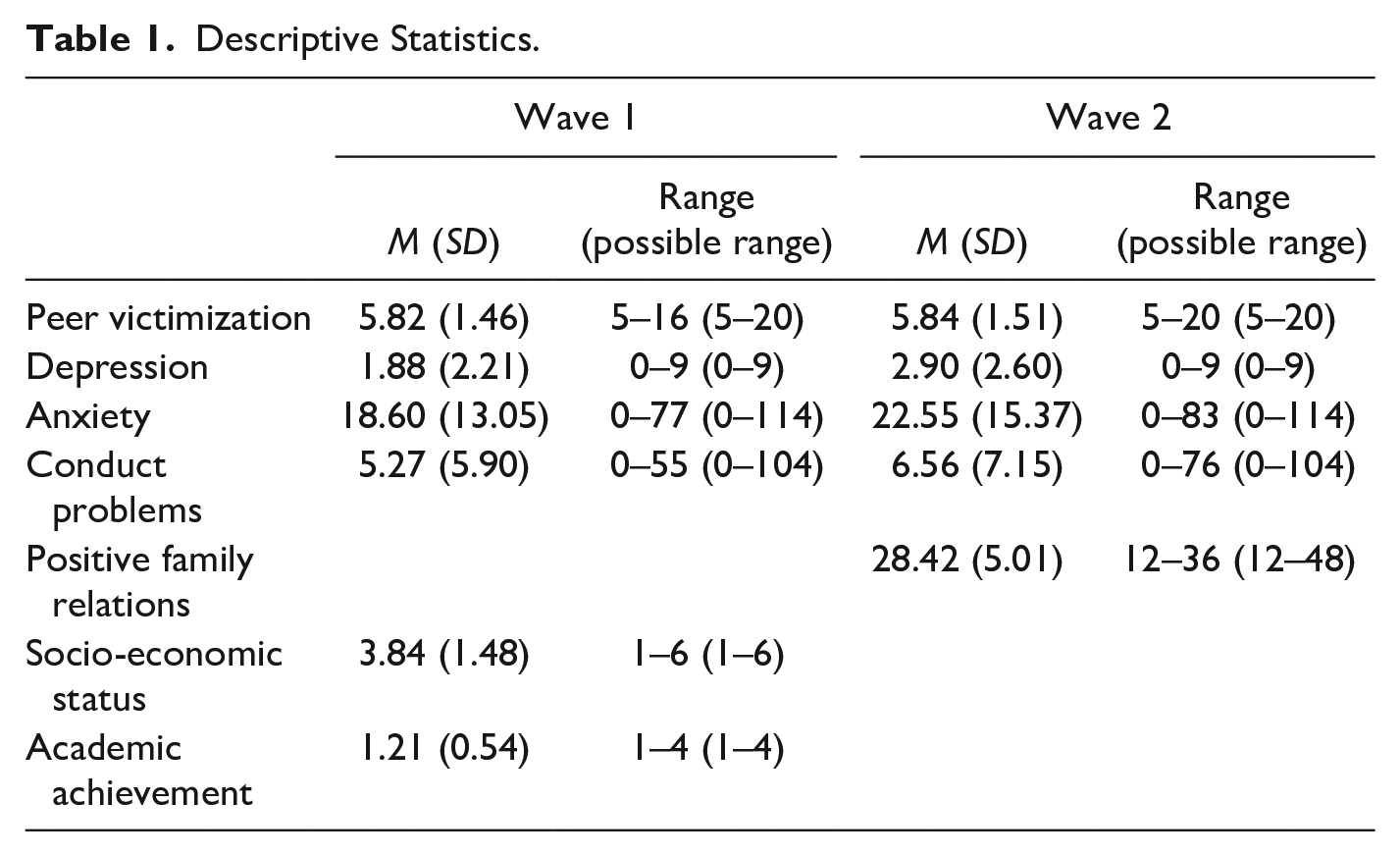
Missing values constituted 11.02%. Little’s MCAR test was significant (χ2 = 265.70, p < .001), indicating that data was not missing at random. To account for this, we imputed five sets of imputed data using PMM, which is deemed appropriate under the current circumstances (Kleinke, 2017). Table 1 displays descriptive statistics and Table 2 correlations between all study variables. As can be expected with a community sample, peer victimization and symptom levels were low at the group level. n = 195 (16.1%) had not graduated from high school. Higher levels of peer victimization were significantly correlated with higher levels of depression, anxiety, and CD, concurrently and longitudinally. Higher levels of peer victimization and poor mental health were also weakly but significantly associated with worse academic achievement.
Descriptive Statistics.
Correlations Between Study Variables.
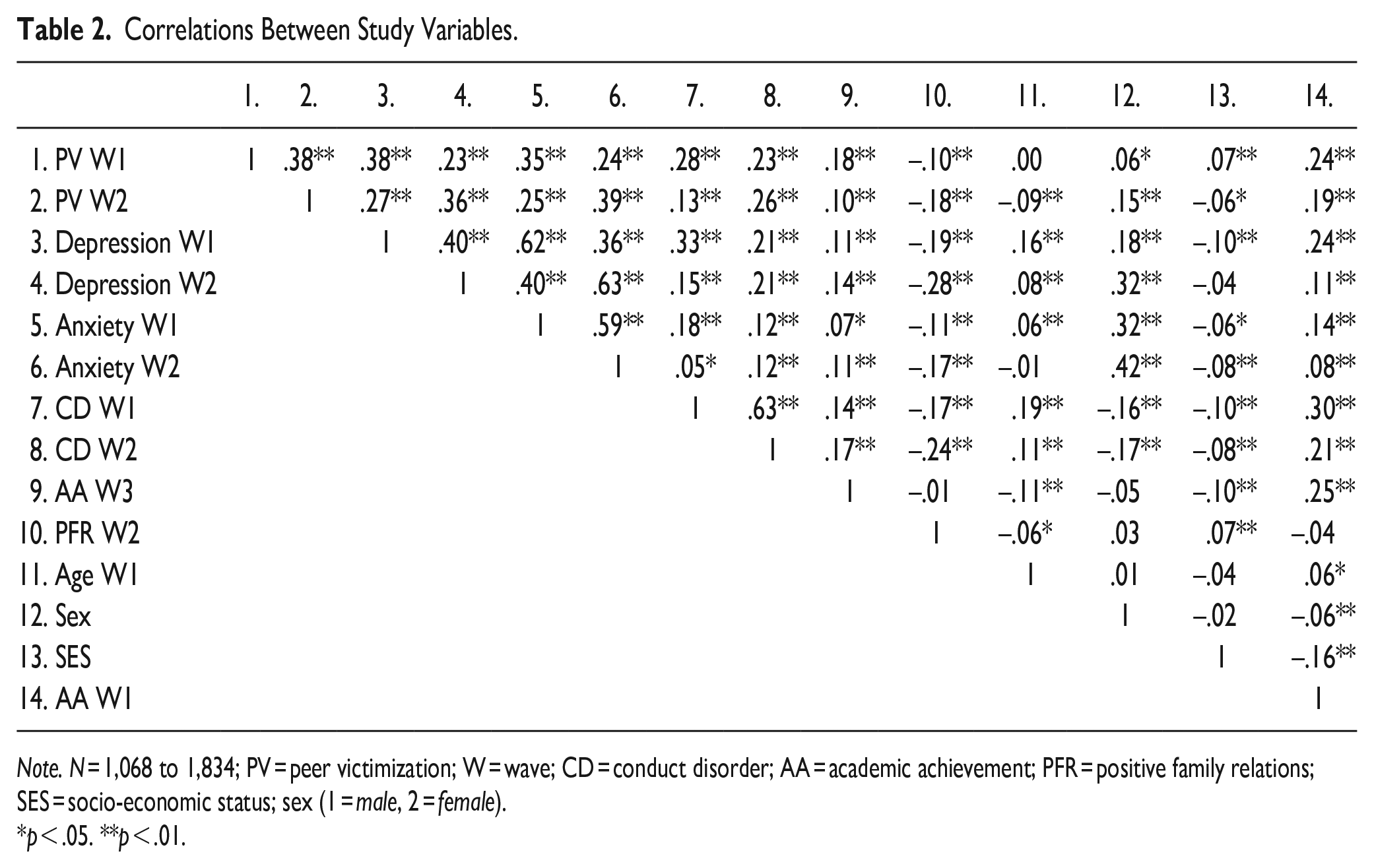
Note. N = 1,068 to 1,834; PV = peer victimization; W = wave; CD = conduct disorder; AA = academic achievement; PFR = positive family relations; SES = socio-economic status; sex (1 = male, 2 = female).
p < .05. **p < .01.
Figure 1 displays an overview of significant direct and indirect effects. Table 3 displays all direct effects in relation to the endogenous variables at W2 and W3 (all enodogenous variables at W1 are depicted in Figure 1 and are as such not included in Table 3). All non-significant indirect effects had p-values > .171. The model had good fit according to all indices: χ2 = 1.863 (df = 3), p = .601; CFI = 1.000; TLI = 1.006; RMSEA = 0.000 [CI 0.000, 0.032]; and SRMR = 0.005. Peer victimization at W1 and W2 had concurrent direct effects on mental health, in that higher levels of peer victimization were associated with higher symptom levels of depression, anxiety, and CD. Longitudinally, all constructs at W1 had direct effects on the same constructs at W2, indicating stability of all constructs. There were no longitudinal direct effects of peer victimization on mental health. Depression at W1 had a direct effect on peer victimization at W2. Peer victimization at W1, depressive symptoms at W2, and CD at W2 had direct effects on academic achievement at W3, in that higher levels contributed to poorer academic achievement. As for indirect effects, depressive symptoms at W2 mediated the effects of depression and anxiety at W1 on academic achievement at W3 whereas CD at W2 mediated the effect of CD at W1 on acdemic achievement at W3. Positive family relations did not moderate the associations between the predictors and academic achievement at W3. Specifically, no interation term was significant in the initial multi-moderation model (all ps > .334) and the stepwise exclusion of interaction terms revealed no remaining significant moderations (all ps > .208).
Depiction of all Effects in the Model.
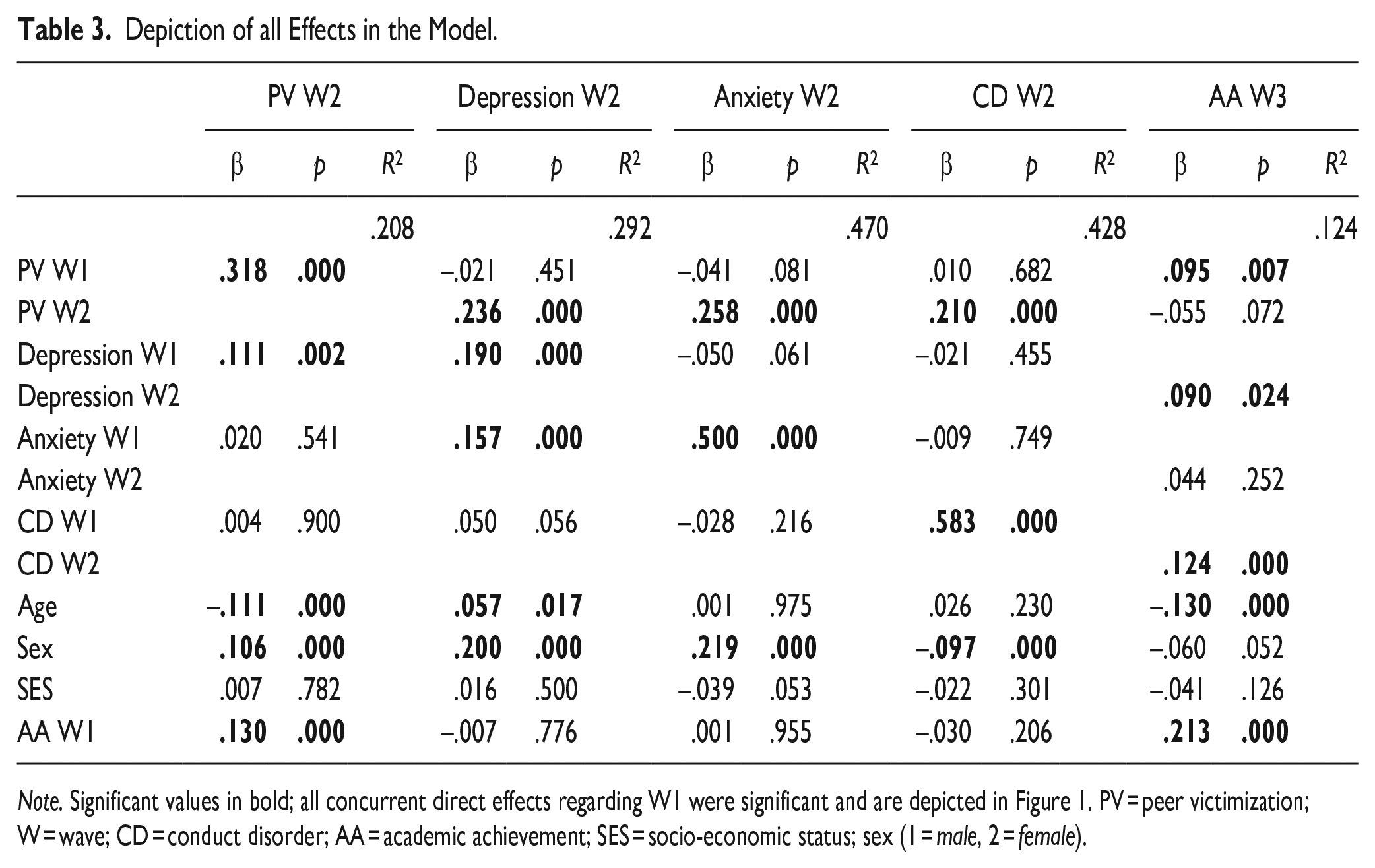
Note. Significant values in bold; all concurrent direct effects regarding W1 were significant and are depicted in Figure 1. PV = peer victimization; W = wave; CD = conduct disorder; AA = academic achievement; SES = socio-economic status; sex (1 = male, 2 = female).
Discussion
An essential marker of efficacious transition from adolescence to adulthood is to graduate from high school. This transition can be obstructed by peer victimization and ill mental health. In a three-wave longitudinal study, we mapped direct and indirect effects of adolescent peer victimization and mental health problems on academic achievement in early adulthood and examined positive family relations as a potential moderator. We found concurrent rather than longitudinal transactional effects between experience of peer victimization and poor mental health. In line with our hypothesis, we found longitudinal direct effects of peer victimization and mental health problems on academic achievement. Specifically, higher levels of adolescent peer victimization and symptoms of depression and CD had direct effects on poorer academic achievement in early adulthood. Depressive symptoms at W2 mediated the effects of symptoms of depression and anxiety at W1 and CD at W2 mediated the effect of CD at W1 on academic achievement. Effects tended to be small and were, in contrast to our hypothesis, not moderated by positive family relations.
Peer Victimization and Mental Health
Peer victimization and poor mental health were moderately associated, with only one cascading longitudinal effect, in that depression at W1 affected peer victimization at W2. This effect is in line with the symptom-driven model, and suggests that experience of depressive symptoms is a risk-factor for being exposed to peer victimization 3 years later. As peer victimization did not affect mental health across time, our results do not support the interpersonal model. In conclusion, this means that the transactional model is not supported by our data. This corroborates parts of the findings by Davis and colleagues who found that adolescents who reported higher depressive symptoms also reported higher future peer victimization (Davis et al., 2019). However, they also found interpersonal effects, and as such evidence of transactional effects. Our findings contrast previous studies in middle childhood that found effects of peer victimization on later internalizing (Liu et al., 2018; van Lier et al., 2012) and externalizing symptoms (van Lier et al., 2012), in line with the interpersonal model. Rather, we found concurrent effects, indicating that exposure to peer victimization was simultaneously associated with heightened risk for both internalizing and externalizing symptoms, which in turn had direct effects on future symptom levels.
The contrasting effects may be due to the timespan between assessments. Previous studies had 6 to 12 months between assessments (Davis et al., 2019; Liu et al., 2018; van Lier et al., 2012), whereas we had 3 years. This may indicate that transactional effects may not be that long-lasting and that the present situation overrides previous experiences. Further, the assessment method may play a role. For instance, Liu et al. (2018) used peer nominations and van Lier et al. (2012) had teachers reporting on child symptoms.
All constructs were moderately stable across W1 and W2, indicating continuous exposure to peer victimization and experience of poor mental health, in line with previous findings (e.g., Liu et al., 2018). Interestingly, anxiety at W1 contributed to both depression and anxiety at W2 and its effect on academic achievement was mediated by depression. This indicates that anxiety is a heterogenous dimension: When it feeds into depression (e.g., displays of inactivity and inability to focus), it can be detrimental for academic achievement. However, anxiety with no associated depressive symptoms may not have a negative effect on academic achievement, which in turn strengthens the idea that depression and anxiety should be treated as different constructs (Duncan et al., 2021).
Longitudinal Effects on Academic Achievement
The model proposed direct albeit small (12.4% explained variance) effects of peer victimization, depression, and CD on poorer academic achievement in early adulthood controlling for sex, age, SES, and early academic achievement. Interestingly, peer victimization in early rather than later adolescence influenced academic achievement, suggesting long-lasting effects and that early peer victimization overrides the effects of later peer victimization. Possible mechanisms may be that peer victimization leads to school disengagement through distress, psychosocial adjustment problems, absenteeism, and/or a diluted sense of worthiness (Hong et al., 2014; Nakamoto & Schwartz, 2010). Our results are in line with Wolke and colleagues who found an increased risk of not earning a high school diploma for individuals who had experienced childhood peer victimization (Wolke et al., 2013). However, they found that only the group who had both experienced peer victimization and bullied others were at risk for later academic failure.
Results from the current study do not suggest that the effect of peer victimization on academic achievement is mediated by mental health symptoms, but rather that both individual and contextual factors contribute to worse academic achievement. We found direct effects of symptoms of depression and CD at W2 and that symptoms at W2 mediated the effects of all three symptom domains at W1. This finding again indicates stability of symptoms during adolescence, and that the continuity of symptoms at least partly explains the associations between mental health and academic achievement. Mechanistically, depressive symptoms may influence academic achievement through difficulties sustaining attention, poor self-reliance regarding school performance, and perceiving in-classroom and home work as too demanding (Fröjd et al., 2008). Symptoms of CD may in turn affect academic achievement through a range of mechanisms, such as school withdrawal due to delinquent behavior or through comorbid symptoms of inattention (Barriga et al., 2002).
Positive Family Relations
In contrast to our hypothesis, we did not find that positive family relations buffered against the negative effects of peer victimization and poor mental health. Previous studies that found moderating effects of parental support examined samples of younger children and early adolescents (Fite et al., 2014; Rothon et al., 2011). This effect may wane in late adolescence due to the increased autonomy from parents during adolescence, which is considered a salient aspect of psychosocial development (Schulenberg et al., 2004). Instead, other forms of support, such as from peers or teachers, may be important, which calls for further scrutiny. Of note, interventions directed at strengthening family relations may still be beneficial. The current study can only show that no such buffering effect seems to be present naturalistically in relation to academic achievement.
Limitations
Strengths of the current study include a relatively large community-based sample, using a three-wave longitudinal design. There are however a few limitations that need to be noted. First, drop out analyses suggest that there were significant differences between responders and non-responders. Examination of the mean differences suggests that most of these were small in magnitude, although non-responders tended to have heightened levels of CD, be male, and have poorer academic status at W3. To account for this, we conducted the main analyses on imputed data. Results on imputed and non-imputed data were however highly similar. Further, we made no distinction between victims of peer victimization and individuals who were both victims and bullied others. As prior research suggests that bully/victims may be particularly vulnerable, we may lack some specificity in the results. Self-ratings have advantages in that it captures the individuals’ experiences. However, objective measures of exposure to peer victimization could reduce social desirability. Finally, we used a broad measure of academic achievement. Fine-grained measures could provide a more nuanced picture of the associations.
Implications and Conclusions
Systematic reviews suggest that prevention and intervention programs directed against peer victimization and poor mental health are at least somewhat effective (Das et al., 2016; Zych et al., 2015). Although commonly not addressed directly, such interventions may also contribute to a higher degree of individuals graduating from high school, which in turn may prevent alienation and social exclusion due to less income, crime, and health problems. Our results propose that many factors influence the essential step of graduating from high school, and as such interventions may therefore need to be multi-faceted and tailored to address the individual’s cultural, contextual, and personal needs (Malti et al., 2016). Depending on context and individual factors, interventions can be directed at reducing peer victimization (Zych et al., 2015), increasing mental well-being (Das et al., 2016), support academic achievement and involve the school, peers, family, and/or the individual adolescent (Stadler et al., 2010). Of note, we found that positive family relations did not moderate the effects of peer victimization and poor mental health. This may indicate that efficient interventions should preferably target the individual (and perhaps his/her peers) rather than the family system. Taken together, results from this study suggest that exposure to peer victimization and internalizing and externalizing symptoms all contribute to poorer academic achievement although they may not be interrelated through mediation processes. Finally, symptom-driven rather than transactional processes seem to be present in the current sample.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Swedish Research Council for Health, Working Life and Welfare (FORTE) dnr 2018-01127; Svenska Spel Research Council (fo2021-0003); Regional Research Council Mid Sweden-939665 to Sofia Vadlin. Matilda A. Frick was supported by a postdoc grant from the Sasakawa Young Leader’s Fellowship Fund.