
Abstract
This study investigated the extent to which adolescent social network positions are associated with the risk of lifetime daily smoking and nicotine dependence (ND), and whether these associations differ by gender. Using data from the National Longitudinal Study of Adolescent to Adult Health (N = 6,267), this study estimated multinomial logistic regression models. An increase in in-degree nominations, out-degree nominations, and Bonacich centrality was associated with a lower relative risk of never smoking daily versus ever smoking daily. By contrast, adolescents with greater in-degree nominations, out-degree nominations, Bonacich centrality, and network reach in three steps were at decreased risk for lifetime ND. Gender-stratified models indicate that the negative association between network position and never smoking daily was driven largely by women, whereas the positive association between network position and lifetime ND was driven largely by men. Incorporating social network structural approaches into adolescent smoking prevention efforts may be beneficial.
Introduction
In 2021, approximately 11 in every 100 middle school students (11.3%) and approximately 1 in every 3 high school students (34.0%) reported having ever used tobacco products in the United States (CDC, 2022). About 4 in every 100 middle school students (4.0%) and about 13 in every 100 high school students (13.4%) reported currently using a tobacco product. Moreover, in the United States in 2020, 8.5% (or approximately 23.6 million people) of people aged 12 or older had nicotine dependence (Substance Abuse and Mental Health Services Administration, 2020). Adolescent smoking is known to have negative effects on a variety of youth outcomes including academic performance (D’Amico et al., 2016; Orpinas et al., 2016) and physical (Bauldry et al., 2012; Griesler et al., 2016) as well as mental health (Moylan et al., 2013). These outcomes hold long-term implications for socioeconomic status attainment and health. Understanding the determinants of adolescent smoking is particularly important because smoking during adolescence is strongly correlated with smoking behavior throughout the course of a person’s lifetime (US Department of Health and Human Services, 2012).
Social networks exert a strong influence on adolescents, especially on smoking behavior (Montgomery et al., 2020). According to previous research, the influence of adolescent social networks on smoking behavior may stem from exposure to the characteristics and behaviors of peers. For example, adolescents with more smoking friends are more likely to begin smoking due to social learning and/or peer pressure from persons in their social networks (Green et al., 2013; Hoffman et al., 2006; Valente et al., 2013). Another line of research has suggested that an adolescent’s structural network position influences his or her smoking behavior (Lakon & Valente, 2012). Popular adolescents (those with more in-degree nominations) are more likely to engage in or initiate smoking behavior in order to maintain or occupy a prominent position in their friendship networks (Alexander et al., 2001; Ennett et al., 2006; Phua, 2011; Valente et al., 2005). In addition, they are more frequently exposed to smoking environments and tend to use smoking as a social activity (Almquist & Östberg, 2013; Niño et al., 2016; Prinstein et al., 2011). In contrast, however, some studies have found that adolescents who are socially isolated (i.e., less popular) are more likely to begin smoking (Seo & Huang, 2012).
Despite existing evidence establishing a link between social network position and smoking behavior, previous studies have been limited by their reliance on self-reported egocentric measurements. From a methodological perspective, egocentric social network analysis is incapable of observing and capturing the structural features of peer relationships because it is based on the ego’s subjective evaluation of his/her own network position (e.g., self-reports of the number of friends one has) (Djomba & Zaletel-Kragelj, 2016). Thus, the use of egocentric social network data may lead to biased estimates due to measurement error (Feld & Carter, 2002). In addition, studies employing egocentric network measures have almost exclusively relied on the characteristics of the ego’s immediate network such as popularity and isolation. This approach ignores the role of social network structure and is unable to capture an individual’s broader structural position within the entire network (e.g., centrality). It is thus critical to objectively and comprehensively measure the network’s attributes in order to delineate the processes of social influence occurring within the social network (Rice et al., 2014).
In addition, prior research on social network positions and smoking behaviors has almost exclusively focused on popularity as a measure of a favorable network position. Although popularity and centrality are often used interchangeably, popularity only considers direct connections (i.e., the number of in-degree nominations), whereas centrality (degree or reach centrality) considers both their own direct connections and their friends’ connections, capturing information about an individual’s structural network position (in terms of connections and distance) (Gest et al., 2001). Therefore, centrality is a more accurate indicator of an individual’s status and social prestige within a whole network structure. Examining network centrality (along with popularity) enables us to gain a better understanding of the relationship between social networks and risk-taking behaviors by providing clarity on which aspect of one’s network position (immediate connections vs. relative position in network structures) is more salient for smoking behavior.
Another limitation of previous research is that few studies on social networks and smoking have considered nicotine dependence (ND) as an outcome. While smoking is a general form of tobacco consumption behavior, ND refers to the underlying level of psychological and physiological addiction or dependence on nicotine (Bainter et al., 2020). Given that smoking behaviors progress through stages based on frequency and intensity of use (Mayhew et al., 2000), ND is crucial to the progression and persistence of smoking behavior over the life course. Previous research has demonstrated that, compared to novice adolescent smokers, adolescents with ND are more likely to engage in smoking behavior in the future and are less likely to stop smoking (Dierker et al., 2015; Selya et al., 2016). Moreover, compared to adults, adolescents are more susceptible to lifetime ND (Wellman et al., 2016). Despite the importance of studying ND, the majority of previous research has focused on the influence of network measures on regular smoking behavior, such as daily smoking (McMillan et al., 2018; Robalino & Macy, 2018). Given the lifelong implications of the development of ND, it is essential to investigate whether and how adolescents’ social network position is related to lifetime ND.
Considering the more apparent negative symptoms of ND (e.g., impairment of social activities and psychological health problems such as anger, difficulty concentrating, depression, insomnia, anxiety, restlessness, etc.) and the stigma associated with it, the relationship between adolescents’ network positions and ND may differ from that of regular smoking behavior. Those who are socially popular or central may have a strong motivation to avoid developing ND (Post et al., 2010). Popularity and centrality often accompany the emotional, social, and instrumental support that is essential to the avoidance of engagement in risky behaviors (Hershberger et al., 2016; Kandel et al., 2007; Lakon et al., 2010). These supports may prevent individuals from developing ND throughout their lives. Similarly, Valente et al. (2005) argue that popular adolescents engage in risky behaviors to the extent that they do not deviate excessively from the group’s norms.
There may be gender differences in how social networks influence daily smoking and ND. While daily and past 30-day smoking prevalence have decreased among American adolescents in recent years, the decline is more pronounced in boys than in girls (Meza et al., 2020). While many boys tend to begin smoking to imitate their peers’ behavior and/or to cope with anxious feelings, girls often attempt smoking to gain social approval from their peers and others or to appear more socially advanced (Lansford et al., 2009). Furthermore, given that girls are more susceptible to peer influences and pressures regarding smoking than boys are (Santano-Mogena et al., 2022), the role of network position on regular smoking may be more salient for girls than boys. In contrast, considering the potential higher cost of ND for boys (boys’ popularity and centrality are often based on social interactions and activities) (Ahn & Rodkin, 2014), the negative association between network position and ND may be more pronounced for boys than girls.
The present study overcomes some of the data limitations in previous studies and addresses important gaps in the understanding of peer influence on smoking behaviors. Using the National Longitudinal Study of Adolescent to Adult Health (Add Health), this study investigates whether network position in adolescence is associated with lifetime smoking behavior. We consider four network measures including in-degree nominations, out-degree nominations, Bonacich centrality, and network reach in three steps. To quantify the measures of adolescent network position, we use sociometric data on friendship ties, rather than egocentric network measures. Furthermore, in order to build on previous research, we distinguish between regular smoking and ND. In addition, we focus on lifetime smoking behaviors rather than adolescent smoking behaviors. We also estimate gender-stratified models to investigate whether the relationship between adolescent network measures and lifetime smoking behaviors varies by gender.
Based on the aforementioned empirical evidence on peer influences in adolescents’ smoking behaviors, we formulate three main hypotheses. First, a more favorable structural position in adolescence (i.e., higher popularity and higher centrality) increases the chance of ever being a daily smoker. Second, a more favorable structural position in adolescence (i.e., higher popularity and higher centrality) decreases the chance of ever being nicotine dependent. Third, the association between adolescent network position and ever being a daily smoker is more pronounced among girls, whereas the association between adolescent position and ever being nicotine dependent is more pronounced among boys. Given some disagreement in the existing literature regarding the relationship between network positions and smoking behavior and the paucity of empirical evidence on ND, we used our proposed hypotheses primarily to guide the direction of our empirical analyses.
Data and Methods
Data
This study used data from the National Longitudinal Study of Adolescent to Adult Health (Add Health). Add Health is a nationally representative sample of students in grades 7 through 12 in 1994 to 1995 (Wave 1). Follow-up surveys were conducted approximately 1 year (Wave 2), 6 years (Wave 3), 13 years (Wave 4), and 22 years later (Wave 5). Participants of the Add Health provided written informed consent for participation in all aspects of Add Health in accordance with the University of North Carolina School of Public Health Institutional Review Board guidelines, which are based on the Code of Federal Regulations on the Protection of Human Subjects 45CFR46: http://www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.html. Written informed consent was given by participants (or by their next of kin/caregiver). Because this study analyzed secondary data with no personal identifiers, it was exempt from Institutional Review Board approval (KUIRB-2022-0057-01).
A unique feature of Add Health was that the survey was based on a clustered design, making it possible to collect sociometric network data. Sociometric network data are useful because they contain extensive information about how individual students are connected to the social structure in which they are embedded. Taking advantage of sociometric network data, researchers can measure the structure of extended friendship networks among students (e.g., Bonacich centrality and network reach in three steps) that egocentric social network data cannot capture. In this study, data from Wave 1 (both In-School and In-Home surveys) and Wave 4 (In-Home survey) were used. Wave 4 data were used to capture one’s lifetime nicotine dependence because nicotine dependence is an outcome that develops over a long period of time (Dierker et al., 2015; Selya et al., 2016).
Three major sample restriction criteria were applied to construct our analytic sample. First, from our baseline sample of 15,322 adolescents who were interviewed for both the Wave 1 and Wave 4 In-Home surveys, we dropped 4,541 participants with missingness in Add Health network measures. During the In-School survey, students were asked to nominate up to five male and five female friends. Based on these nominations, Add Health created measures capturing the within-school network structure among students. To improve the reliability of the information, these measures were constructed only for students in schools in which more than half the student body completed the questionnaire (Carolina Population Center, 2001). Second, we dropped 4,151 participants who reported in the In-School survey that they smoked during the past 12 months. This sample restriction rules out the possibility that smoking behaviors determine adolescent social networks and not vice versa. Third, we dropped 363 participants without valid data on smoking behaviors (including ND) in Wave 4. This leaves an analytical sample of 6,267. Ten multiple imputations were implemented using the chain equations (ICE) procedure in Stata 16.1 to handle missing values of control variables (mostly family income and maternal education measured at Wave 1).
In supplementary analyses, we compared the sociodemographic characteristics of the final analytic and the excluded sample. Specifically, we ran regression models of an indicator of sample inclusion on sociodemographic characteristics (Table S1 in the Supplemental Material). We found that those who are younger, Black (vs. White), foreign-born, have a better-educated mother, and live with both biological parents are more likely to be included in the analytic sample.
Measures
Dependent Variables
Two lifetime smoking behaviors were used as dependent variables (measured in Wave 4). “Ever smoked daily” was measured by students’ response to the following questions (No/Yes): “Have you ever smoked cigarettes regularly—that is, at least one cigarette every day for 30 days?” “Lifetime ND” was measured using responses to the six questions drawn from Fagerstrom test for ND (Heatherton et al., 1991). Respondents were asked about their current smoking behavior (Cronbach’s alpha for current ND = .69); for those reporting no current symptoms, the questions were asked about the period when they smoked the most (Cronbach’s alpha for lifetime ND = .72). The following questions were asked: (1) How soon after you wake up do you have your first cigarette (within 5 min, within 6–30 min, within 31–60 min, after 60 min; coded 3, 2, 1, and 0, respectively)?; (2) Do you find it difficult not to smoke in places where it is forbidden, for example, in church, at the library, or in theaters (No/Yes; coded 0/1)?; (3) Which cigarette would you hate most to give up (any other in the day or evening/the first in the morning; coded 0/1)?; (4) How many cigarettes a day do you smoke (31 or more cigarettes, 21–30 cigarettes, 11–20 cigarettes, 10 or fewer cigarettes; coded 3, 2, 1, and 0, respectively)?; (5) Do you smoke more frequently during the first hours after waking than during the rest of the day (No/Yes; coded 0/1)?; and (6) Do you still smoke even if you are so ill that you are in bed most of the day (No/Yes; coded 0/1)? Following Breslau and Johnson (2000), all the responses were summed, and a score of 4 or more was defined as ND. Using information about past and current smoking behaviors, three mutually exclusive categories were created: never smoked daily (Ever smoked daily = No); ever smoked daily (Ever smoked daily = Yes & Lifetime ND = No); and lifetime ND (Ever smoked daily = Yes & Lifetime ND = Yes). Wave 4 data were used to create a lifetime smoking behavior variable because only Wave 4 includes both current smoking behavior and lifetime nicotine dependence behavior (Wave 3 includes only current behavior and Wave 5 has no data on nicotine dependence).
Independent Variables
The independent variables included four measures of adolescent network position (measured in Wave 1) (Bryan, 2017; Kim & Park, 2022): (1) the number of friend nominations received from other students in school (in-degree nominations); (2) the number of friend nominations sent to other students in school (out-degree nominations); (3) respondent’s centrality within a school social network (Bonacich centrality); and (4) the total number of students respondent could reach in three steps (i.e., friends of friends’ friends) (network reach in three steps). Bonacich centrality (degree centrality) captures a respondent’s prominence or importance in one’s social network (Bonacich, 1987), whereas network reach in three steps (closeness centrality) captures a respondent’s extended social network size (i.e., the extent to which the respondent and his/her friends are socially isolated). All network measures were standardized to ease interpretation of coefficients.
Control Variables
In regression models, we included a large array of individual- and family-level covariates (measured in Wave 1). Given that there are well-established demographic differences in both one’s social network position and health behaviors (Smith & Christakis, 2008), we adjusted for age, gender, race/ethnicity, foreign-born status, and grade-level. Familial/parental characteristics may also be potential confounders because they tend to shape children’s social networks (Bryan, 2017) and health behaviors (Haas, 2008). Familial/parental characteristics included maternal education, family income, co-residence with both biological parents, number of siblings, and rural status.
Several adolescent characteristics may also confound the relationship between adolescent social networks and lifetime smoking behaviors. Given that latent cognitive and noncognitive skills predict peer network/relationships (van Aken & Asendorpf, 2018) as well as health behaviors (Kim, 2022), we controlled for standardized Peabody Picture Vocabulary Test (PVT) score, Wave 1 personality (extraversion, neuroticism, and conscientiousness), and low self-control. Other adolescent characteristics and experiences that may be confounders include sports participation, disability status, and physical appearance (Strauss & Pollack, 2003). As such, we controlled for the following covariates: participation in sports activities, physical attractiveness (rated by interviewer), body mass index (BMI), and disability status.
Statistical Analysis
In this study, we jointly examined whether adolescent social networks are associated with different lifetime smoking behaviors. We estimated multinomial logistic regression models to predict the odds of having “Ever smoked daily = No” and having “Ever smoked daily = Yes & Lifetime ND = Yes,” compared to having “Ever smoked daily = Yes & Lifetime ND = No” (reference category). We presented relative risk ratios (RRRs). A RRR greater than one represents an increased risk and less than one represents decreased risk. We conducted a sequence of nested models to assess the extent to which covariates confound observed associations and yield spurious results. The first model estimated bivariate associations between social network position and lifetime smoking behaviors. In the second model, we adjusted for a wide array of sociodemographic, familial/parental, and adolescent characteristics that are likely to predict both network position during adolescence and lifetime smoking behaviors.
All models controlled for school fixed effects. School fixed effects likely capture important environmental and contextual confounding factors (at both the school- and neighborhood-levels) that may affect both students’ network position in adolescence and lifetime smoking behaviors (Leventhal & Brooks-Gunn, 2000). School fixed effects models mechanically yield the average differences in lifetime smoking behaviors within schools for students with different network positions by controlling for all contextual variables correlated with adolescent networks and adult health. Robust standard errors were clustered at the school level.
Results
Table 1 presents summary statistics for the analytic sample (N = 6,267). The mean respondent age was 16 years old in Wave 1. Approximately 55% were women. Regarding race/ethnicity, 51%, 26%, 14%, and 8% were white, Black, Hispanic, and other, respectively. Among the sample (those who did not smoke by the In-School survey in Wave 1), about 14% reported ever being a daily smoker, and 12% reported ever being nicotine dependent (4.4% for current ND and 7.4% for lifetime ND). Among those who had ever smoked daily, about 45% were nicotine dependent. On average, respondents received about 4.37 nominations from and sent about 4.52 nominations to friends attending the same school. The mean Bonacich centrality scale score was 0.85, and the mean network reach in three steps was 58.17. There are significant gender differences in smoking behaviors as well as social network position. Men are more likely than women to ever smoke daily and develop ND over the course of their lives. Women also tend to have an advantage in network measures over men, with higher popularity (in-degree and out-degree nominations) and centrality (Bonacich centrality and network reach in three steps).
Summary Statistics, Add Health Sample (N = 6,267).
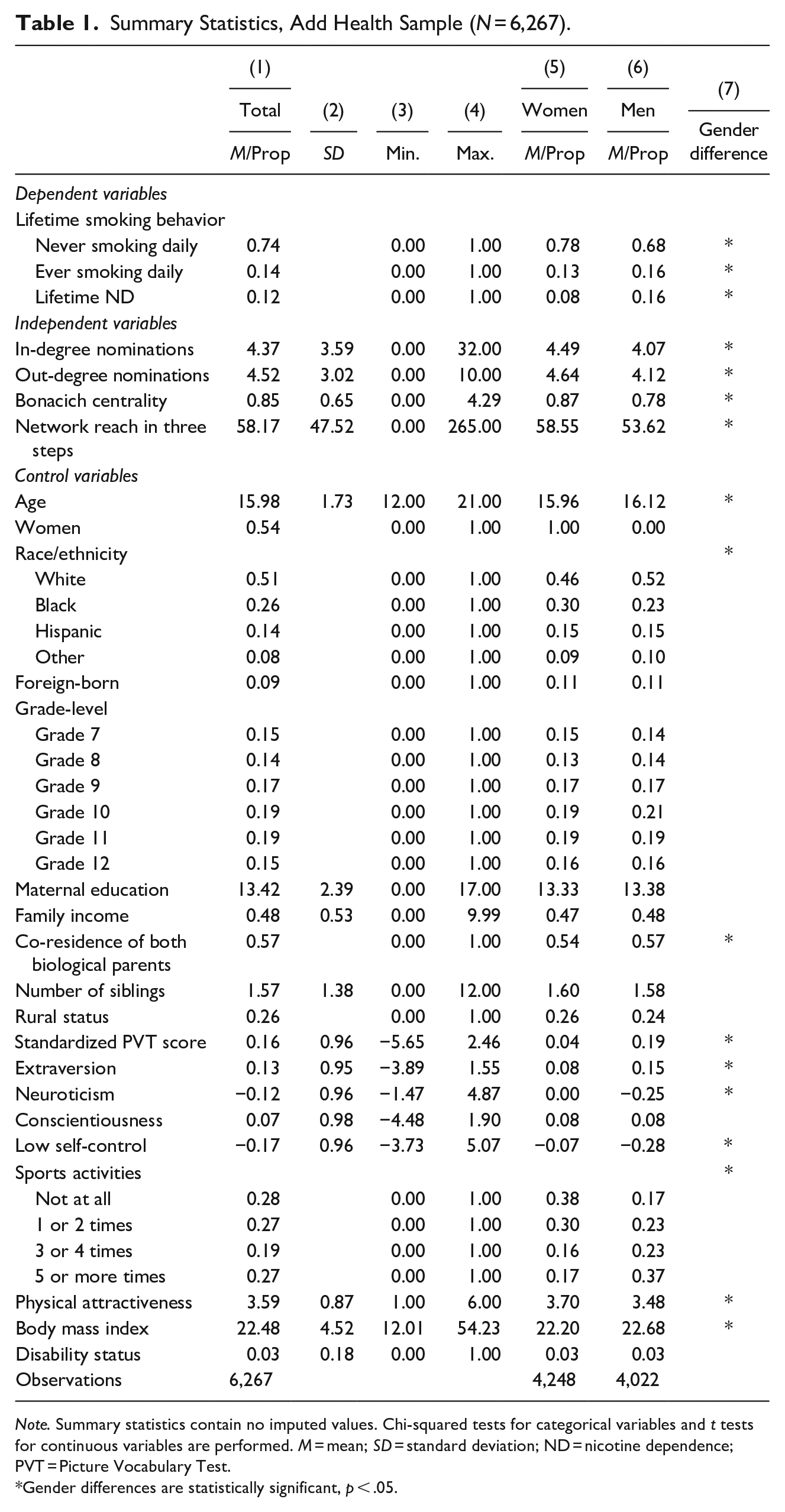
Note. Summary statistics contain no imputed values. Chi-squared tests for categorical variables and t tests for continuous variables are performed. M = mean; SD = standard deviation; ND = nicotine dependence; PVT = Picture Vocabulary Test.
Gender differences are statistically significant, p < .05.
Table 2 presents RRRs from multinomial logistic regressions predicting the relative risk of never smoking daily and lifetime ND to ever smoking daily. Columns 1 and 2 show bivariate results, and Columns 3 and 4 show results from models adjusting for both sociodemographic and adolescent characteristics. As shown in Columns 1 and 2, results were generally similar across different network measures: an increase in network measures was associated with decreased relative odds of never being a daily smoker (Column 1) and being nicotine dependent (Column 2) than ever being a daily smoker. It should however be noted that the associations between out-degree nominations and network reach in three steps and never being a daily smoker were not statistically significant at conventional levels.
Multinomial Logistic Regression of Lifetime Smoking Behaviors in Adulthood on Adolescent Social Networks.
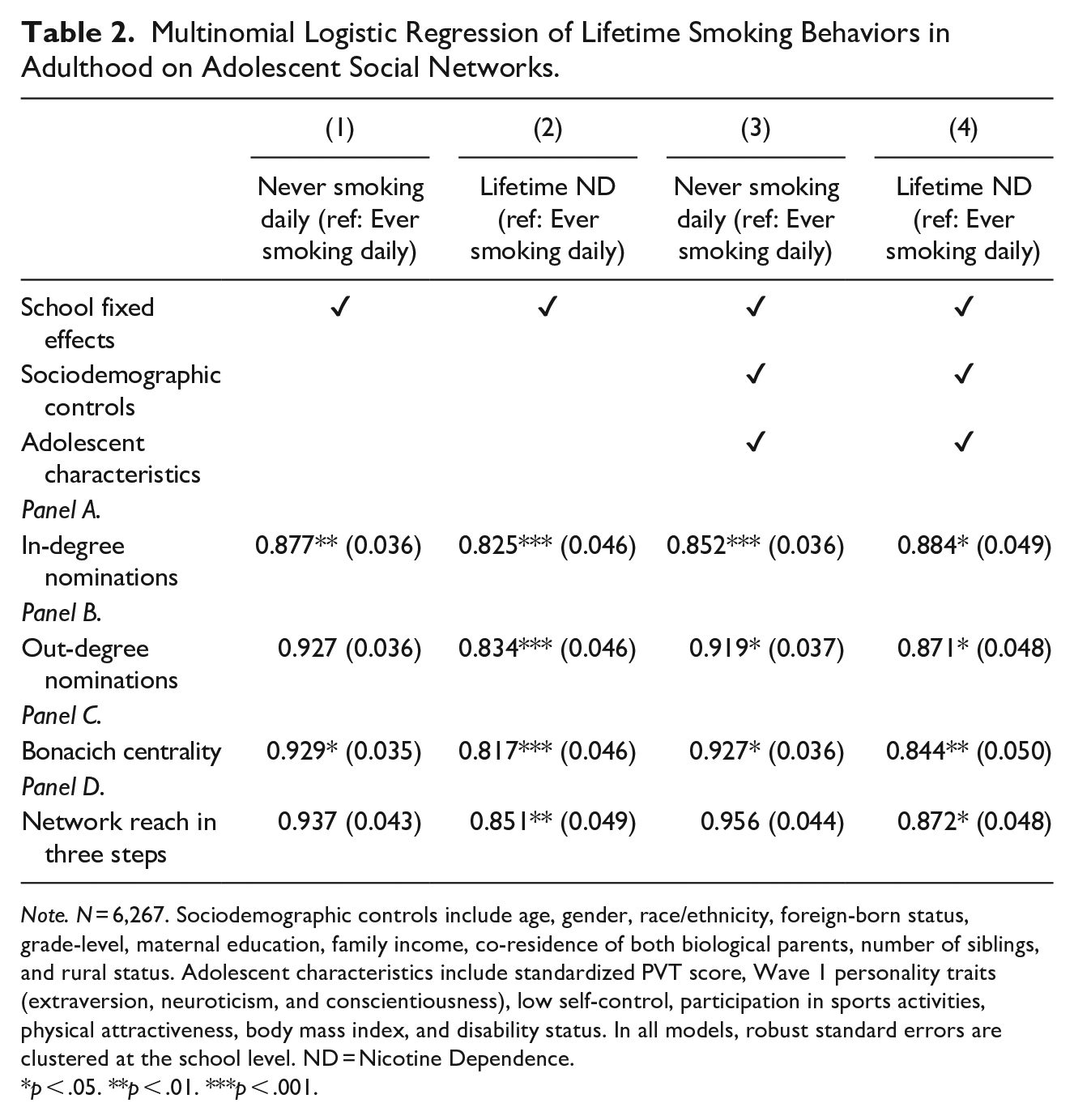
Note. N = 6,267. Sociodemographic controls include age, gender, race/ethnicity, foreign-born status, grade-level, maternal education, family income, co-residence of both biological parents, number of siblings, and rural status. Adolescent characteristics include standardized PVT score, Wave 1 personality traits (extraversion, neuroticism, and conscientiousness), low self-control, participation in sports activities, physical attractiveness, body mass index, and disability status. In all models, robust standard errors are clustered at the school level. ND = Nicotine Dependence.
p < .05. **p < .01. ***p < .001.
As shown in Columns 3 and 4, observed associations were robust to adjustment for a wide array of covariates. As shown in Column 3, an increase in in-degree nominations, out-degree nominations, and Bonacich centrality was associated with a decreased risk of never being a daily smoker than ever being a daily smoker (RRRs = 0.852, 0.919, and 0.927, respectively). A one-standard-deviation increase in network measures was associated with a decreased risk of lifetime ND relative to ever being a daily smoker. The decrease was about 12% ([1–0.884] × 100) for in-degree nominations, 13% ([1–0.871] × 100) for out-degree nominations, and 16% ([1–0.844] × 100) for Bonacich centrality (Column 4). Network reach in three steps was only associated with the risk of lifetime ND versus ever smoking daily (RRR = 0.872). In supplementary analyses, when current and lifetime ND were separated, all network measures except in-degree nominations were associated with decreased risk for both lifetime and current ND (Table S2 in the Supplemental Material). On the other hand, in-degree nominations were only negatively associated with lifetime ND, not current ND.
Table 3 presents results separately for women (Columns 1 and 2) and men (Columns 3 and 4). Gender-stratified models suggest that the negative associations between network measures and never smoking daily (vs. ever smoking daily) are more pronounced among women (Column 1 vs. Column 3). In-degree nominations were associated with decreased risk of never being a daily smoker for both women (RRR = 0.810, Column 1) and men (RRR = 0.868, Column 3). In contrast, the association for Bonacich centrality was significant only for women (RRR = 0.874), not men. Among women, a one-standard-deviation increase in network measures leads to about 11% to 19% lower relative odds of not being a daily smoker than being a daily smoker. In contrast, all network measures were negatively associated with the risk of lifetime ND (vs. ever smoking daily) for men but not women (except for Bonacich centrality, Panel C). A one-standard-deviation increase in network measures leads to about 17% to 19% lower relative odds of being nicotine dependent among men (Column 4). Among women, only Bonacich centrality was associated with lifetime ND (RRR = 0.845, Column 2).
Multinomial Logistic Regression of Lifetime Smoking Behaviors in Adulthood on Adolescent Social Networks, by Gender.
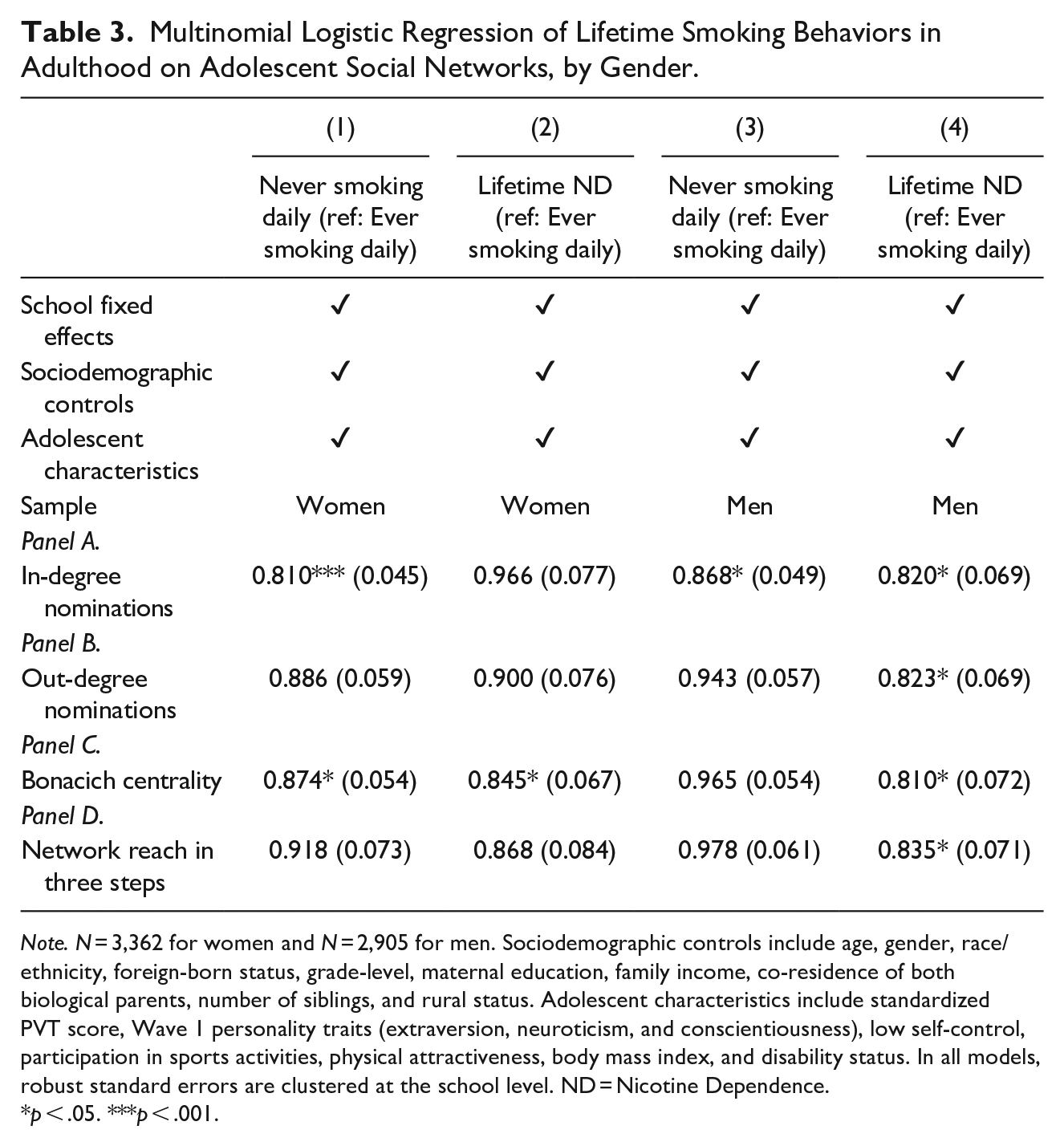
Note. N = 3,362 for women and N = 2,905 for men. Sociodemographic controls include age, gender, race/ethnicity, foreign-born status, grade-level, maternal education, family income, co-residence of both biological parents, number of siblings, and rural status. Adolescent characteristics include standardized PVT score, Wave 1 personality traits (extraversion, neuroticism, and conscientiousness), low self-control, participation in sports activities, physical attractiveness, body mass index, and disability status. In all models, robust standard errors are clustered at the school level. ND = Nicotine Dependence.
p < .05. ***p < .001.
Discussion
While numerous studies have established that adolescent social networks are important for smoking behavior, significant research gaps remain. To address these gaps, this study used a large scale, nationally representative longitudinal dataset to examine the association between various measures of social network position during adolescence and lifetime smoking behavior. We differentiated between regular and ND smoking when measuring lifetime smoking behavior. We found that a person with greater popularity and centrality is at higher risk of ever being a daily smoker but a lower risk of developing ND. These associations remained when we controlled for a wide variety of sociodemographic and adolescent characteristics. In addition, we found gender differences in this relationship: the association between popularity/centrality and an increased risk of ever smoking daily was significant only for girls, whereas the association between popularity/centrality and a decreased risk of ND was significant only for boys.
In general, our findings are consistent with prior research demonstrating a positive association between popularity and smoking behavior during adolescence (Montgomery et al., 2020; Prinstein et al., 2011; Valente et al., 2013). This study also clarified that the relationship was stronger for in-degree nominations (often interpreted as a form of popularity) than out-degree nominations (often interpreted as gregariousness). Similarly, greater centrality (Bonacich centrality, but not network reach in three steps) was also associated with an increased risk of ever being a daily smoker. This suggests that ego’s structural network position, determined by both ego’s and alters’ prominence, also affects how peers influence each other’s smoking behavior. Those who are central in the network may be more likely to begin smoking because they are connected socially to a larger number of students and thus may have a need to embrace the norms of their network in order to remain central (Valente et al., 2005).
By contrast, greater popularity and centrality were found to be protective against ND. This suggests that different features of adolescent network position may have varying pathways through which they affect various behaviors such as daily smoking and ND. Popularity and centrality often accompany social support, which is essential to health (Lakon et al., 2010) and which may act as a protective factor preventing persons from developing ND throughout their lives. For example, the risk of becoming addicted to nicotine may be reduced in popular and central individuals because they may be better informed about health-promoting behaviors and receive more instrumental support (Hershberger et al., 2016). Given that psychiatric disorders such as depressive symptoms, anxiety, and personality disorders are associated with increased risk of lifetime ND, emotional and social support enjoyed by popular and central individuals may help reduce the risk of ND (Kandel et al., 2007). Furthermore, our findings that adolescent school social networks are related to ND into young adulthood are consistent with life course perspectives that argue that early exposure to physical, environmental, and psychosocial factors shape health and health behaviors later in life (Jones et al., 2019; Park & Kim, 2022).
Our findings regarding gender differences corroborate previous research indicating that girls’ smoking initiation is more susceptible to peer influence and/or pressure (Santano-Mogena et al., 2022). Many girls begin smoking to gain popularity and attention from their peers (Abel et al., 2002). The fact that girls’ peers tend to be more behaviorally homogeneous than boys’ peers also is aligned with our finding that the association between network position and becoming a daily smoker is stronger among girls than boys (Lansford et al., 2009). In the case of ND, the aforementioned mediating role of social support may be more relevant for boys who smoke. Boys may be more resistant to the psychological illness and social rejection caused by ND because they see social gatherings and activities as a way to maintain their social status (i.e., greater popularity and centrality) (Giordano, 2003). Furthermore, despite the lower prevalence, the significantly more severe symptoms of ND in females suggest that network position may play a limited role in lowering the risk of developing ND in females (Colby et al., 2000). For example, girls are more likely to report increased stress and depression, weight gain, increased appetite, and smoking to relieve such symptoms during nicotine withdrawal (Stanton et al., 1996). In this regard, rather than peer support, girls may require more professional treatment from health providers, such as counseling, therapy, and medication, to prevent the development of ND.
This study has a few limitations. First, due to the lack of data regarding adulthood social networks and the timing of ND, this study was unable to examine trajectories of post-school network positions and smoking behaviors and how they are longitudinally associated with adolescent social network positions. Relatedly, this study did not investigate specific pathways that mediate the relationship between social network structure and smoking behavior (e.g., social support from peers, peer group norms regarding smoking, etc.). More research is required to investigate the mechanisms underlying the effect of adolescent social network position on smoking behaviors. Second, despite the fact that we accounted for a wide variety of sociodemographic and adolescent characteristics, as well as school fixed effects, we were unable to fully address unobserved heterogeneity that could confound the relationship between adolescent network position and lifetime smoking behavior. Unobserved family background factors such as genetics, personality (e.g., sociability), parenting styles, and family instability may be potential confounders. Therefore, the study’s findings should be interpreted as correlational rather than causal. More evidence is needed to establish the causal effects of adolescent network measures on lifetime smoking behavior, particularly the development of ND. Third, the sample selection likely limits the generalizability of the findings of this study. Readers should keep in mind that those who are younger, Black (vs. White), foreign-born, have a better-educated mother, and live with both biological parents are more likely to be included in the analytic sample. Given that adolescents from higher socioeconomic families have a lower risk of lifetime daily smoking and nicotine dependence and enjoy more advantageous network positions, the effects found in this study are likely to be underestimated.
The findings of this study hold policy implications and can inform interventions that promote life-long health and well-being. Our findings suggest that incorporating social network structural approaches into adolescent smoking prevention efforts may be beneficial. Schools’ efforts to prevent lifetime smoking initiation may be more effective when targeting students who are positioned near the center of their peer networks (Kim, 2021). For them, social acceptance and prestige may be important enough to justify engaging in health-threatening behaviors like smoking. Moreover, given our finding that those on the periphery of social networks (i.e., social isolates) are relatively more vulnerable to the risk of ND than their central and popular counterparts, interventions aimed at preventing ND may specifically target them (East et al., 2021). Because they often lack a source of social support, it may be beneficial to mitigate the psychological effects of social isolation and marginalization and to provide them with necessary information about ND prevention. Finally, it is necessary to develop school-based smoking prevention programs that are tailored to student gender as our study finds that how network position influences one’s lifetime smoking behavior differently varies by gender. In resource-constrained settings, a gender-specific approach may be considered. For example, interventions targeting girls with greater popularity and centrality may be particularly effective in preventing cigarette smoking, whereas interventions targeting boys with greater popularity and centrality may be particularly effective in preventing the development of ND.
Supplemental Material
sj-docx-1-yas-10.1177_0044118X231164742 – Supplemental material for A Longitudinal Cohort Study of Adolescent Social Network Positions and Lifetime Daily Smoking and Nicotine Dependence
Supplemental material, sj-docx-1-yas-10.1177_0044118X231164742 for A Longitudinal Cohort Study of Adolescent Social Network Positions and Lifetime Daily Smoking and Nicotine Dependence by Minsung Sohn, Daseul Moon and Jinho Kim in Youth & Society
Footnotes
Acknowledgements
All authors contributed equally to the research. This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (![]() ). No direct support was received from grant P01-HD31921 for this analysis.
). No direct support was received from grant P01-HD31921 for this analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Participants of the Add Health provided written informed consent for participation in all aspects of Add Health in accordance with the University of North Carolina School of Public Health Institutional Review Board guidelines, which are based on the Code of Federal Regulations on the Protection of Human Subjects 45CFR46: ![]() . Written informed consent was given by participants (or by their next of kin/caregiver). Because this study analyzed secondary data with no personal identifiers, it was exempt from Institutional Review Board approval (KUIRB-2022-0057-01).
. Written informed consent was given by participants (or by their next of kin/caregiver). Because this study analyzed secondary data with no personal identifiers, it was exempt from Institutional Review Board approval (KUIRB-2022-0057-01).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.