
Abstract
Limited emphasis is placed on understanding the gendered pathways that influence mental health, especially long-term cumulative impacts of gender-based inequalities. Exposure to early child marriage (marriage by age 15) may exaggerate exposure to gender-based mental health risk-factors, providing an opportunity to understand the multi-layered gendered pathways that impact mental health overtime. We used nationally representative cross-sectional data from Ethiopia to examine the relationship between early child marriage and psychological well-being and assessed if intimate partner violence mediates this relationship among young women. We implemented three separate multivariate regression models to assess these relationships. Our results suggest that the relationship between early child marriage and psychological well-being is influenced by higher levels of violence experienced by women in early child marriages as compared to their counterparts who married later. Investments in longitudinal data are needed to rigorously parse out the relationship between early child marriage, intimate partner violence, and psychological well-being.
Keywords
Introduction
Overview
Women are more likely than men to be impacted by common mental health disorders such as depression and anxiety, which affects approximately one in three people, contributing significantly to the global burden of disease (WHO, 2018). The reasons for higher prevalence of common psychological problems among women are not well understood and several theoretical pathways have been put forward to explain these differences, but there is limited empirical evidence supporting these pathways (Sachs-Ericsson, 2002). Beyond biological considerations, several theories postulate that the higher rates of common mental illnesses among women, particularly depression, may be spurred by gender-based inequalities that disproportionality impact women (Sachs-Ericsson, 2002). Gender is understood as a multilevel system of difference and inequality, which involves cultural beliefs, distributions of resources, patterns of behavior, organizational practices, and selves and identities (Ridgeway & Correll, 2004). Gender norms, which are accepted attributes and characteristics associated with ones gender, define what are appropriate social roles for women and men, which in turn determine access and control over critical resources such as social status, treatment and earnings in society, agency and ability to make decisions about one’s life – factors known to increase or decrease exposure and susceptibility to common mental illnesses (WHO, 2018). Gender norms also influence attitudes surrounding appropriate age to marry and have children for women and men, ideologies surrounding transitions to adulthood, and the economic value of men versus women (Greene & Stiefvater, 2019). Due to prevailing gender norms, girls are more likely than boys to drop out of school early, and to be married as children (UNICEF, 2012).
Gender Socialization, Gender Roles, and Adolescence
Gender socialization is the process of learning and internalizing the gender norms or rules of society, which are reinforced by social networks (John et al., 2017; Schulenberg, et al., 1997). Although gender socialization starts very early in life, adolescence is understood to be a critical point for gender socialization as the shaping of gender beliefs and attitudes intensifies during this period, in part because of changes experienced during puberty (Hill & Lynch, 1983; John et al., 2017; Kågesten et al., 2016). During adolescence, girls and boys face additional social pressure from family and peers to conform to prescribed gender roles, which reinforce notions of femininity and masculinity (Chandra-Mouli et al., 2017; John et al., 2017). Researchers theorize that socialization of adolescents into gender appropriate roles is often more stressful for girls than for boys because of the need to adhere to narrower roles and idealized feminine traits such as submissiveness, nurturance, and emotional sensitivity (Aubé et al., 2000). Another body of research suggests that gender role conflict or gender role stress results when there is discrepancy between how one believes they should act,—based on gender role expectations learned in childhood - and how one thinks, feels, or behaves (Pinhas et al., 2019). Available evidence suggests that gender role conflict is heightened for females during puberty because of greater social pressures to conform to prescribed gender roles from peers and parents, which makes girls more vulnerable to psychological distress (Gilligan et al., 1990; Hill & Lynch, 1983). Gender-role conflict has been found to play a role in the suicidal behaviour of girls (Pinhas et al., 2019). Others suggest that the socialization process encourages girls as opposed to boys to cope with distress by internalizing it, and this process of internalization is associated with more depression, anxiety, and suicidal ideation among women (Canetto, 1997; Sachs-Ericsson, 2002).
A woman’s status within marriage due to their prescribed gender roles and related structural inequalities have also been theorized to reduce psychological well-being. Drawing on structural approaches to stratification and mental health outcomes, theorists argue that groups who are lower in social hierarchies suffer from greater psychological problems (Rosenfield, 2012). These structural approaches posit “double or triple jeopardy” situations, where its hypothesized that groups lower in multiple stratification systems are especially at high risk of mental illnesses (Rosenfield, 2012). Research suggests that married women may have lower levels of psychological well-being as compared to their unmarried counterparts mainly because of their relegation to housework, which may not be very rewarding, or having to multi-task at home and the workplace but without any recognition of their contributions (Lennon & Rosenfield, 1992; Mirowsky & Ross, 2003). Relatedly, due to their prescribed gender roles within marriage, women end up depending on their husbands for socio-economic survival, have limited agency, lower status within their marriages, and increased exposure to gender-based violence; factors hypothesized to increase susceptibility to mental health issues (Kapungu & Petroni, 2017; Landstedt et al., 2009; Rhodes et al., 2014).
Child Marriage and Early Child Marriage
Child marriage, an extreme manifestation of gender inequalities, is defined as any formal marriage or informal union where one or both parties are under 18 years of age (UNICEF, 2014). In this paper, we distinguish early child marriage (marriage by age 15) from child marriage because of its potential to have more severe health impacts. Women married as children may have increased susceptibility to mental illness as they face several inter-linked jeopardy situations like the structural theories postulate. Their vulnerability to mental illnesses may be compounded by the disadvantages they face due to their age and developmental stage, in addition to their gender, marital status, as well as their socio-economic background, and the interlinkages between these factors. Early marriage requires transitioning abruptly into gendered adult roles and responsibilities, and a young girl may not be developmentally ready to tackle these responsibilities (Mathur et al., 2003). Girls who marry early are also more likely to come from poorer households, live in rural areas, and have limited opportunities for schooling and labor force participation (Erulkar, 2013; Parsons et al., 2015; UNICEF, 2014). This increases the likelihood of economic dependence on their spouse, and limits their bargaining power within their marriage (Nguyen et al., 2014). Additionally, unequal power dynamics is often heightened in these marriages due to significant age disparities between spouses, which further reduces the ability of the woman to negotiate and exercise agency within the marriage (Choi & Ha, 2011; Singh, 1998). Women in these marriages also tend to experience higher levels of intimate partner violence than their older married counterparts (Kidman, 2017). Due to their compromised agency, young brides are more likely to believe that their husbands are justified in beating them, which increases their susceptibility to tolerate violence, and reduces their likelihood of leaving abusive partners (Nasrullah et al., 2017). Ultimately, their developmental stage, loss of adolescence, factors associated with early marriage such as curtailment of personal freedom and agency, forced sexual relations, and elevated exposure to intimate partner violence may increase the propensity of these women to experience mental illnesses and reduced well-being. Furthermore, evidence suggests that those who experience early child marriage are particularly vulnerable to these negative outcomes. Multiple studies demonstrate that child marriage increases risk for intimate partner violence and reduces decision-making ability, particularly among those who have experienced early child marriage (Erulkar, 2013; Heise et al., 2002; Klugman, et al., 2014; Raj et al., 2010; Santhya et al., 2010; Speizer & Pearson, 2011; Yount et al., 2016). Clearly, several gender and age-related risk factors intersect with child marriage and elevate the risk of psychological distress, and these risk factors are heightened among those who have experienced early child marriage. Early child marriage, therefore, provides a unique opportunity to understand the cumulative impacts of a gender-based discriminatory practice with co-occurring risk factors on mental health but it remains understudied.
Early Marriage in Ethiopia
While the proportion of girls marrying as children is declining globally, there has been faster progress in Ethiopia in recent decades. Nonetheless, as many as 20 % of Ethiopian women 15-24 years old continue to be married very early (by age 15) (Central Statistical Agency (CSA) [Ethiopia] and ICF, 2016). Moreover, polygamous unions continue to prevail (7.4%), and the share of women who marry early tends to be higher in polygamous as compared to monogamous households (Central Statistical Agency (CSA) [Ethiopia] and ICF, 2016). Studies from Ethiopia also suggest that girls who marry very early are particularly vulnerable to adverse outcomes. A population-based study conducted in Ethiopia’s seven regions found that girls who married before age 15 had limited decision-making ability and were more likely to have experienced forced sex (Sachs-Ericsson, 2002). Another nationally representative study found compromised communication, trust, intimacy and reduced equality in early child marriage with violence contributing to the situation (John, Edmeades, Murithi et al., 2019). The association between CM and mental health is understudied in Low and Middle Income Countries. We are aware of one published study conducted in Ethiopia among a sample of girls aged 10 to 17 years in the Amhara region, which found increased odds of suicidality among girls who were ever married, or were promised in marriage, or had received marriage requests as opposed to girls who had never been in the marriage process (Gage, 2013).
Given these gaps, we used nationally representative cross-sectional data from Ethiopia to examine the relationship between early child marriage, intimate partner violence, and psychological well-being. In a previous paper, we examined the association of child marriage and psychological well-being among Ethiopian women 18 to 45 years old using data from the same study and found that early child marriage is associated with reduced psychological well-being (John, Edmeades, & Murithi 2019). In this paper, we try to disentangle the relationship between early child marriage, intimate partner violence, and psychological well-being among young Ethiopian women (18–24 years). Figure 1 outlines the conceptualized relationship between the three variables. The model hypothesizes a temporal sequence in which early child marriage affects psychological well-being through the mediating variable intimate partner violence, which is the indirect effect. The model also allows a direct relationship between early child marriage and psychological well-being. We restricted the analysis to women aged 18 to 24 years so that findings reflect lived realities of the current cohort of Ethiopian women. Given the focus on intimate partner violence, we limit the analysis to currently partnered women.
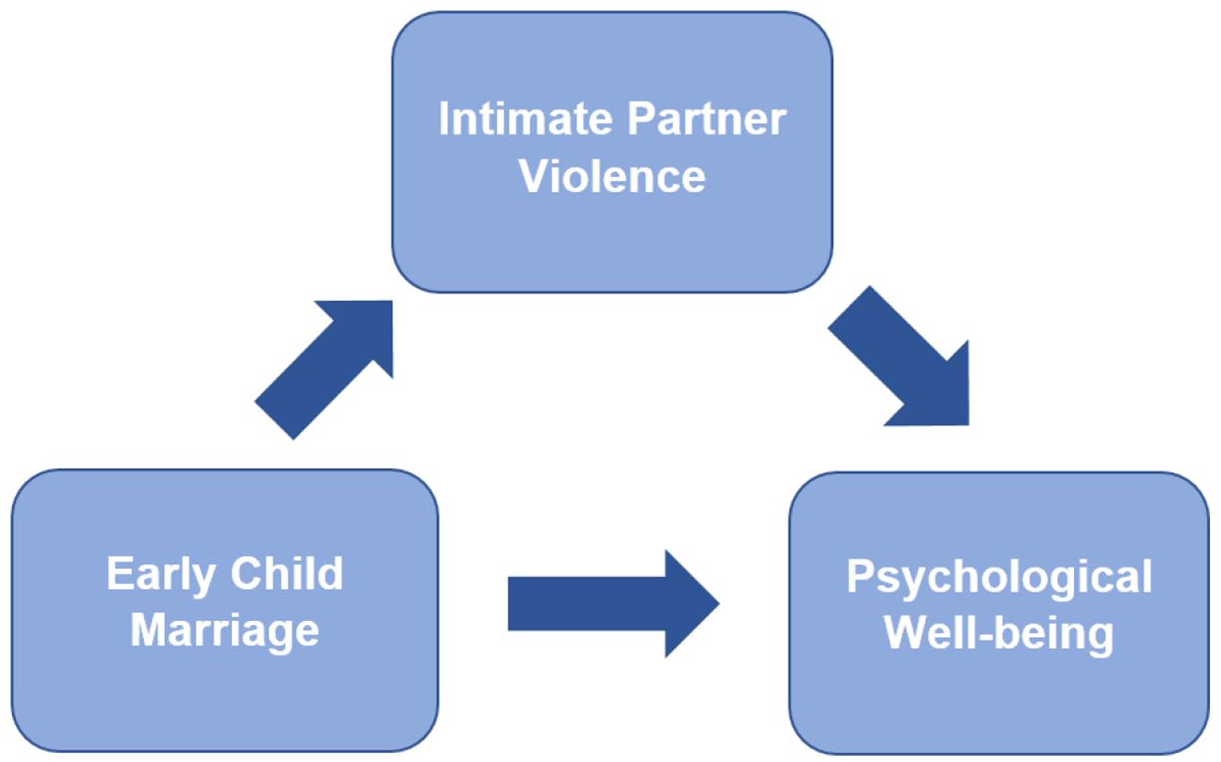
Pathways framework for analysis.
Methods
Data
The data used for these analyses were derived from a study estimating the economic costs of child marriage in Ethiopia conducted in 2016. Ethical approval was obtained both at the global and local levels. At the global level, review was provided by the Institutional Review Board from the International Center for Research on Women, while in Ethiopia review was provided by the National Research Ethics Review Committee. Quantitative survey data were collected from 4,149 ever married women in the age range of 18 to 45 years in the nine regions and the city of Dire Dawa using a multi-stage cluster design to generate representative data for the country barring the city of Addis Ababa. A three-stage stratified sampling approach was followed to develop the sample. First, within each region, districts were selected probability proportional to size, followed by random selection of kebeles and villages. Household census was conducted in the villages for the random selection of 25 eligible households. An eligible woman was randomly selected from the household roster. If a woman did not consent to participate, the field team randomly selected another eligible woman from the same household or an adjacent household. Local researchers who collected data in the relevant local language of the region attended a week-long training to understand the goals of the study and related ethical considerations. The local Principal Investigator conducted periodic spot checks to ensure data quality and adherence to research protocol.
Measures
Dependent variable
Psychological well-being: Measures of well-being were obtained from the Psychological General Well-being Index, a widely used scale to measure the psychological quality of life of general populations as well as people with chronic diseases (Chassany et al., 2004). The scale has been validated and used in several countries including South Africa and India (Chassany et al., 2004). The index consists of 22 items, which are rated on a 6-point scale and assess psychological well-being in 6 health related quality of life domains: Anxiety, Depressed Mood, Positive Well-being, Self-Control, General Health, and Vitality. The respondents are asked to report on these measures for the month preceding the survey. Internal consistency of the items was assessed using Cronbach’s Alpha, followed by principal components factor analysis. The items had high internal reliability with an alpha over .70. The predicted scores were normalized to range from 0 to 100, where a higher score indicates more well-being.
Independent variable
Early child marriage: A dummy variable was created that differentiated women who were married by age 15 from those who married later.
Mediating variable
Intimate partner violence: The measures were drawn from the 2004 World Health Organization’s Multi-Country Study on Women’s Health and Domestic Violence (García Moreno et al., 2005). The survey includes measures of physical, sexual, and emotional violence. The respondents were asked to report any intimate partner violence experienced in the 12 months preceding the survey. A binary variable that captured any experience of physical and sexual violence was created.
Other variables
A range of standard socio-demographic, household, and couple-level variables known to influence psychological well-being, early child marriage, and interpersonal violence were included in the analysis such as the respondents’ age, education, employment status, number of children, household wealth, spousal age-difference, polygamous marriage, urban residence, and region. Respondent’s age was measured as a binary variable differentiating women aged 18-19 from those over 20 years old. Education was measured as a categorical variable differentiating those with no education, primary and secondary, or higher education. Employment distinguished women in formal work from those not working. Polygamous marriage was measured as a dummy variable. Household wealth was constructed through a principal component analysis of household assets and characteristics such as ownership of consumer items and type of dwelling. The index score was used to divide the households into quintiles that indicates poorest, poor, middle, rich and richest households. A categorical variable was created to differentiate the regions of Ethiopia, while a dummy variable distinguished living in urban and rural communities.
Statistical Analysis
Mediator variables are variables that sit between independent variable and dependent variable and mediate the effect of the IV on the DV. Mediation analysis provides a way of understanding the mechanisms relating an exposure variable to a specific outcome by identifying influential mediator variables (Imai et al., 2010). A series of regression models can be estimated to compute the effects of the intermediate variable. Mediation analysis traditionally involves three steps (Baron & Kenny, 1986). First, testing if the independent variable (early child marriage) is associated with the dependent variable (psychological well-being) after controlling for other variables. Second, testing if the independent variable (early child marriage) and the mediating variable (intimate partner violence) are associated after controlling for other variables. Thirdly, relating the mediating variable to the dependent variable after controlling for the independent variable and other variables. The first regression model provides the direct effect of the independent variable on the dependent variable. In mediation analysis with continuous predictors, the product of the estimates from steps 2 and 3 provide the indirect effect of the independent variable on the dependent variable, also known as the amount of mediation, provided by the mediator in the relationship between the independent variable and the dependent variable. The direct effect plus the indirect effect produces the total effect. The proportion mediated can then be obtained by dividing the indirect effect by the total effect. However, in our analyses, since the independent and mediating variable are binary, resulting in two different estimation scales, this decomposition of effects does not accurately estimate the effect sizes (Mackinnon & Dwyer, 1993). Instead, the estimated coefficients must be scaled to make them comparable across equations (Mackinnon & Dwyer, 1993). To overcome this challenge, we estimated simultaneous multivariable regression models (i.e., seemingly unrelated regressions) (Zellner, 1962). These estimates provide the coefficients and standard errors needed to compute direct and indirect effects and are useful when the outcome and predictor variables are not continuous. All analyses were performed in Stata 14. Data were weighted for complex survey design, including clustering of data.
Results
The sample consisted of 1109 ever married women 18 to 24 years old, out of which 60 were separated/divorced or widowed. After accounting for missing variables, the final analytical sample consisted of 969 currently married women.
Sample Characteristics
The women on average were 21 years old and 44 percent had never attended school (Table 1). The prevalence of early child marriage was 27%. As many as 37% of the women in the early child marriage sample had experienced intimate partner violence as compared to 24% of the non-early child marriage sample, while the mean psychological well-being scores among the early child marriage sample was 66.88 (SD: 22.88) points as compared to 72.88 (SD: 20.39) points among the non-early child marriage sample.
Descriptive Statistics on Study Variables (n = 969).
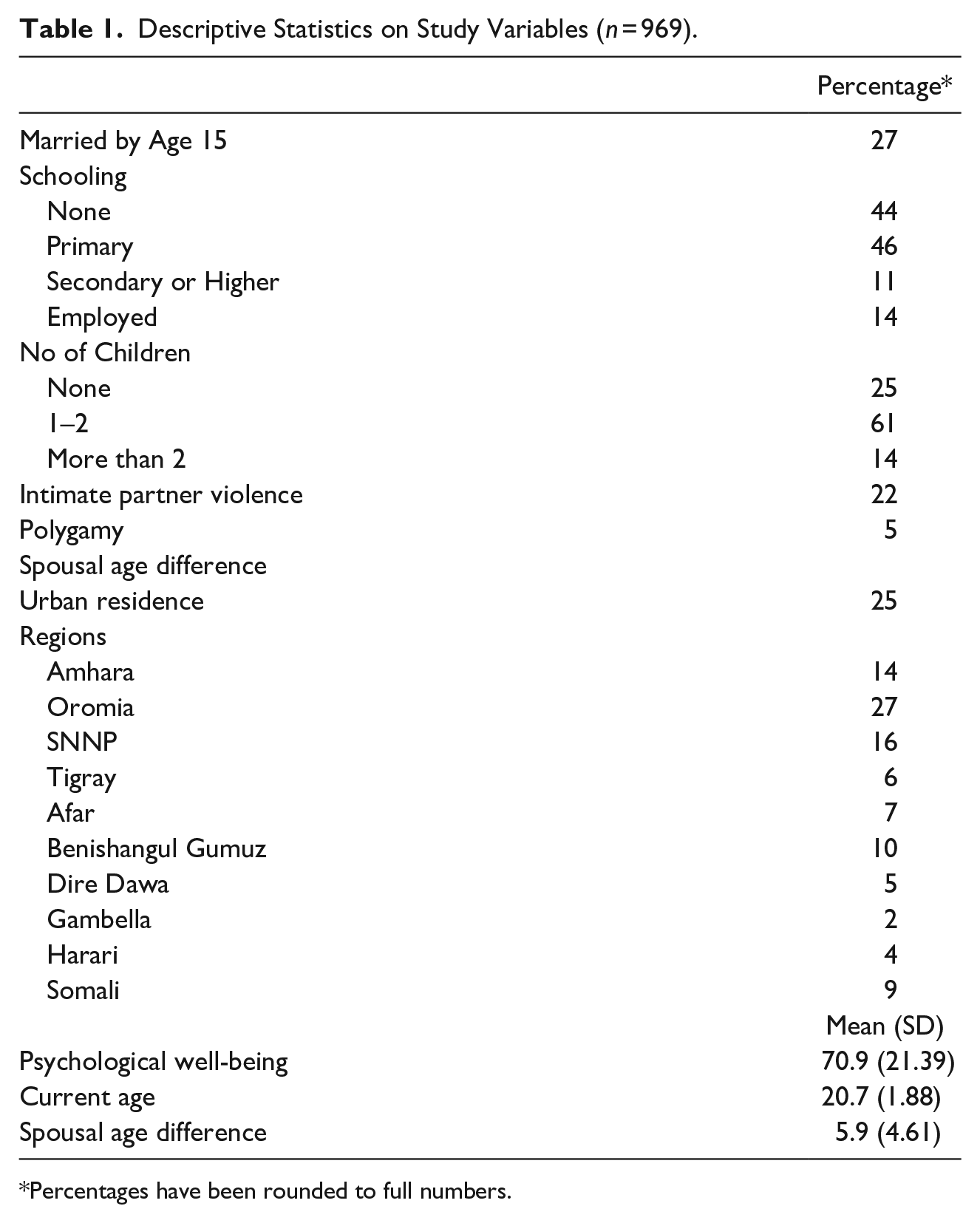
Percentages have been rounded to full numbers.
Mediation Analysis
To assess mediation, we first assessed the association between early child marriage (independent variable) and psychological well-being (dependent variable). Regression 1 (Table 2) found a negative association between early child marriage and psychological well-being. On average early child marriage significantly reduced psychological well-being by 3.12 (β: −3.12; SE: 1.60) percentage points for the early child marriage sample as compared to their counterparts after controlling for other factors associated with early child marriage or psychological well-being (Table 2). As the second step, we assessed if early child marriage was associated with higher levels of intimate partner violence in last 12 months (mediating variable). Estimates from regression 2 (Table 2) confirmed that early child marriage sample had increased odds of experiencing intimate partner as compared to women who were married later after controlling for other variables. Finally, when the intimate partner violence measures were included in regression 1 (regression 3), Early child marriage was no longer significant, but intimate partner violence was significantly negatively associated with psychological well-being, suggesting that the influence of early child marriage on psychological well-being is mainly mediated through increased exposure to intimate partner violence (Table 2). Given that early child marriage was no longer significant after we included intimate partner violence in the final model, we did not estimate direct and indirect effects.
Multivariate Regression Models Examining the Association between Early Child Marriage (ECM), Intimate Partner Violence (IPV) and Psychological Well-being (PWB) Among Young Ethiopian Women (18–24 years old).
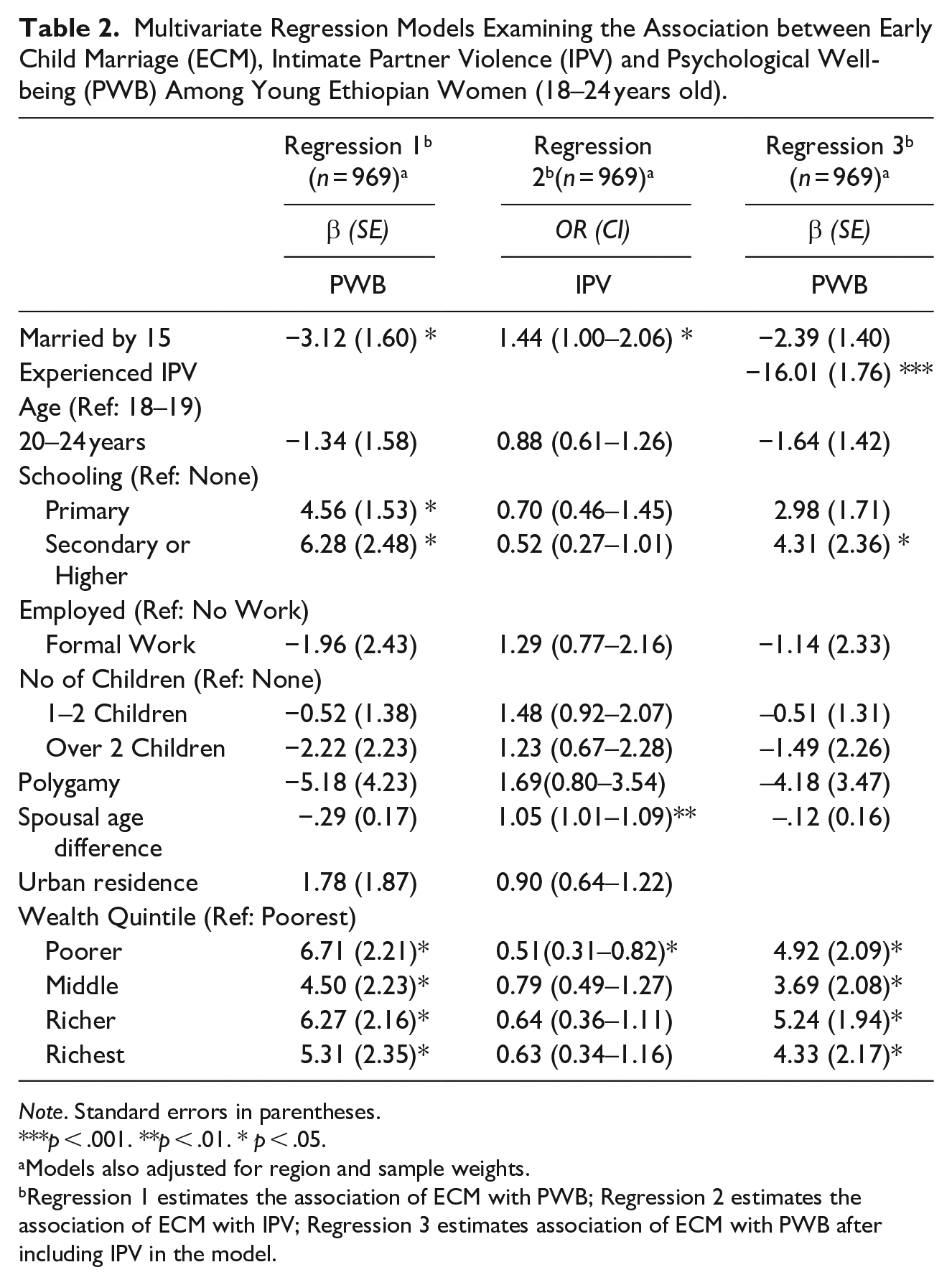
Note. Standard errors in parentheses.
p < .001. **p < .01. * p < .05.
Models also adjusted for region and sample weights.
Regression 1 estimates the association of ECM with PWB; Regression 2 estimates the association of ECM with IPV; Regression 3 estimates association of ECM with PWB after including IPV in the model.
Discussion
Our study expands knowledge on an understudied topic by examining how gender-based pathways influence psychological well-being over time. Our findings indicate that current levels of psychological well-being were lower among young Ethiopian women who experienced early child marriage as compared to their counterparts who married later. The mediation analysis suggests that increased exposure to intimate partner violence among those married early is likely an important gender-based driver of the association between early child marriage and psychological well-being. However, it is important to note here that our study was unable to sufficiently adjust for other drivers of intimate partner violence such as husband’s alcohol abuse and broader structural factors that are known to increase exposure to intimate partner violence, and future studies should explore how these factors may differentially affect those married very early (Jewkes, 2002). Our findings align with the different theoretical approaches that have contributed towards the conceptualization of the relationship between gender-based drivers and mental illness. In alignment with gendered structural theories, and theories that highlight gender role conflict that girls are more likely to experience due to the intensification of gender socialization during adolescence, our findings indicate that the multiple jeopardy situations associated with early child marriage such as age, developmental stage, limited opportunities to build capacity and exercise agency, may increase exposure to intimate partner violence, and decrease overall sense of psychological well-being among these women, and these affects remain over time. Our findings are critical and emphasize how gender-based discriminatory systems are multi-layered and exposure to one increases the level of exposure to other related systems of discrimination and abuse, which ultimately reduces overall psychological well-being and potentially increases the likelihood of suffering from a mental illness later in life.
From a programmatic and policy perspective, these findings highlight that in addition to efforts to prevent child marriage from taking place in the first place, supporting the current cohort of child brides, particularly those married very early, is critical to improve their mental health outcomes later in life. To this end, programs should recognize that child marriage is part of a larger gender-based discriminatory system and its successful elimination as well as alleviating its negative impact will need a multi-pronged approach. Here we can learn from HIV and violence prevention programming, where prevention models have been developed with the explicit recognition that gender inequality and violence underpin women’s vulnerability to HIV and violence (Ellsberg et al., 2015; Pulerwitz et al., 2012). These approaches, therefore, try to address the underlying and multiple vulnerabilities that women face simultaneously such as legal structures that favor men, unequal gender norms, increased care burden, reduced agency, poverty, lower levels of education, and economic dependence on men. More recently, these programs have started involving men and other stakeholders to shift gender norms and power dynamics within couples and in communities using different modalities such as group-based training and community mobilization (Ellsberg et al., 2015; Olaolorun & John, 2021). While in its early stages, there is emerging evidence that these programs that engage numerous stakeholders and use multiple approaches to tackle the underlying gender-based risk factors and promote healthy relationship behaviors among women and men can prove effective for reducing violence and fostering a healthier and more equitable relationship (Ellsberg et al., 2015). Similar approaches can also prove beneficial for shifting marital dynamics and levels of violence among those who have experienced child marriage and improve their health outcomes and mental well-being.
This study has several limitations that need to be considered when interpreting the results. Both the age at marriage and psychological well-being measures were self-reported and subject to recall and social desirability bias. Several procedures were adopted to minimize these errors such as helping respondents remember their exact age at marriage by citing historical events and ensuring interviews were conducted in privacy. Moreover, these problems were more likely among the older respondents and not among the 18 to 24-year-old respondents, the focus of this analysis. The cross-sectional nature of our study is a major limitation, and the estimates can only be interpreted as associations. However, we used the temporality of events to establish the logical sequence of key measures (early child marriage, intimate partner violence and psychological well-being) and adjusted for many factors to ensure robust findings. Despite these limitations, our study provides a unique contribution to the literature by examining the relationship between early child marriage, intimate partner violence and psychological well-being and expands the evidence base on how multi-layered gender systems reinforce their negative impacts and may have long-term consequences. To our knowledge, no other study has investigated this relationship using large scale population-based data in sub-Saharan Africa. Furthermore, our survey collected detailed measures on psychological well-being and intimate partner violence which are not routinely collected at national levels.
Footnotes
Authors’ Note
However, views expressed and information contained within do not necessarily reflect the UK government’s official policies and are not endorsed by the UK government, which accepts no responsibility for such views or information or for any reliance placed on them.’
Meroji Sebany is now affiliated to Save the Children U.S., Washington, DC, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ‘This article was funded by a grant from the Responsive Research and Evaluation Fund of the Gender and Adolescence: Global Evidence (GAGE) programme which is funded by UK aid.