
Abstract
The purpose of the current study was to explore whether selfcompassion predicted psychological distress over and above childhood maltreatment and attachment orientation in high-risk youths. Fifty-one youths (31 males, 20 females) aged 17 to 24, recruited from a community non-profit organization in St. John’s, Newfoundland and Labrador, Canada, were administered validated measures of childhood maltreatment, attachment orientation, self-compassion, and psychological distress. Results indicated that self-compassion was inversely associated with childhood maltreatment, attachment anxiety, attachment avoidance, and psychological distress. However, results did not support the hypothesis that self-compassion was a significant predictor of psychological distress over and above attachment anxiety and childhood maltreatment in high-risk youths. Our results indicated that self-compassion is not well developed in street-involved youths and may be a vital intervention target to heal negative internalized views of the self, while maintaining vigilance to threats inherent in the street environment.
Keywords
Introduction
Homelessness for children and youths are at crisis levels. In Canada, approximately 40,000 adolescents (ages 13–24) are homeless every year (Gaetz, Dej, et al., 2016; Gaetz, O’Grady, et al., 2016). Homeless youths comprise 20% of the homeless population in Canada, with an estimated 40% under the age of 16 (Gaetz, Dej, et al., 2016). The most common reasons given for street-involvement are poverty, family conflict, and abuse (Embleton et al., 2016). Many of these youths are part of the hidden homeless, frequenting youth shelters, temporarily staying with friends or family (“couch surfing”) or living on the street. Although the street culture is dangerous and unstable, these youths view leaving home as an escape from untenable environments where they may endure emotional, physical, and sexual abuse (Kidd, 2004). In many cases, their primary caregivers are the source of the threat, rather than comfort, and security. Individuals with a history of childhood maltreatment and insecure attachment orientations are at higher risk for mental illness in adolescence and adulthood (Wu et al., 2018). The highest rates of mental illness for street-involved youths include depression, anxiety (Bosmans et al., 2010), post-traumatic stress disorder, psychosis, alcohol, and drug abuse (Whitbeck et al., 2004). Thus, street-involved youth have many obstacles to survival, with high rates of childhood maltreatment, poor bonds with their family of origin, and unstable housing that fosters psychological distress. The severity of these psychological challenges makes it imperative to identify protective factors that mediate the mental health struggles that come with physical and emotional deprivation.
A growing body of evidence is showing that self-compassion is a protective factor for both adolescents and adults (Barry et al., 2015; Marsh et al., 2018). Neff (2003b) operationalizes self-compassion within three components: (1) showing kindness toward the self in times of struggle; (2) an understanding that painful experiences and emotions are a common part of humanity; and (3) mindfulness enables individuals to experience their thoughts and emotions in the moment without over-identification. In clinical and non-clinical adults, self-compassion has been associated with lower levels of psychopathology (MacBeth & Gumley, 2012; Zeller et al., 2015) and higher levels of self-esteem, well-being, and quality of life (Neff, Rude, et al., 2007; Neff & Vonk, 2009; Van Dam et al., 2011; Zessin et al., 2015). Less is known about the role of self-compassion for adolescent clinical populations (Xavier et al., 2016). Recent findings indicate that self-compassion is negatively associated with aggression, narcissism, childhood maltreatment, alcohol abuse, suicide attempts, psychological distress (Barry et al., 2015; Jativa & Cerezo, 2014; Jiang et al., 2017; Tanaka et al., 2011; Vettese et al., 2011), and positively associated with self-esteem (Barry et al., 2015; Marshall et al., 2015). In a recent meta-analysis, Marsh et al. (2018) found that self-compassion was inversely associated with anxiety, depression, and stress, and that lower levels of self-compassion may have a role in maintaining emotional challenges in adolescence. It is noteworthy that of the twenty studies included in the Marsh meta-analysis, only three studies involved adolescent clinical samples, suggesting that the association between self-compassion and psychological distress in adolescent clinical samples is still relatively unknown. More research is necessary to determine if self-compassion is a possible protective factor for high-risk youths.
To date, the developmental origins of self-compassion lack theoretical depth. Neff and McGehee (2010) hypothesize that self-compassion emerges from early attachment relationships and the development of internal working models that frame self-perceptions of others’ ability to provide security in times of threat, as well as one’s self-worth. Bartholomew and Horowitz (1991) were the first to propose defining attachment orientation in adolescence and adulthood within two independent dimensions of anxiety and avoidance. Thus, one’s place on these dimensions will characterize their sense of security, worthiness, view of others and the strategies they use to manage stress, threats, and emotional intimacy. Those high on avoidance and low on anxiety are classified as having an avoidant attachment orientation that is characterized by difficulties with intimacy, a rigid focus on self-reliance, and utilizing deactivating strategies (Kobak et al., 2015) that involve disengagement from emotions and cognitions associated with the threat. On the other hand, individuals that are high on anxiety and low on avoidance engage in hyperactivating strategies leading to extreme emotional efforts to sustain close contact with their attachment figure.
Attachment theory is vital to integrate when exploring self-compassion in high-risk youths because attachment orientation is the foundation of how individuals view themselves and others. Neff and McGehee (2010) suggested that people with secure attachments (low anxiety, low avoidance) find it easier to be compassionate toward the self because they have received early messages from caregivers that they are worthy of love and comfort. Whereas those with insecure attachment orientations have experienced inconsistent responses of comfort and support, leading to a more critical internal voice that makes comforting themselves more challenging. Research has shown that lower levels of self-compassion are associated with dysfunctional families, childhood maltreatment (Tanaka et al., 2011), and insecure attachment styles (Neff & McGehee, 2010; Wei et al., 2011). Research has shown that adolescents with secure attachments report higher levels of self-compassion. In contrast, fearful (high anxiety, high avoidance) or preoccupied (high anxiety, low avoidance) attachment styles report lower levels of self-compassion (Neff & McGehee, 2010). In addition, low levels of self-compassion are associated with anxious and avoidant attachment and low maternal warmth (Pepping et al., 2015; Raque-Bogdan et al., 2011).
These preliminary results suggest that the relationship between self-compassion, child maltreatment and attachment orientation may shed light on how high-risk youths frame their view of themselves and their future. Living and surviving in the harsh environments of their family of origin and the streets demonstrate that this population possesses a great deal of resilience. If self-compassion is a protective factor in high-risk youths, treatment interventions targeting this self-construct could shift the individual’s self-perceptions toward healthier developmental trajectories. The purpose of the current study was to explore whether self-compassion is a protective factor for high-risk youths. Specifically, does self-compassion predict psychological distress over and above childhood maltreatment and attachment orientation in high-risk youths? It is hypothesized that self-compassion will be inversely associated with childhood maltreatment, insecure attachment orientations, and psychological distress. Furthermore, self-compassion will not be a better predictor of psychological distress over and above attachment orientation and childhood maltreatment in high-risk youths.
Method
Participants
Fifty-two youths, between the ages of 17-to-24 years (M = 20.86, SD = 2.44, 58.8% males), were recruited from a community non-profit organization that provides resources to high-risk youths, in St. John’s Newfoundland and Labrador. Although a larger sample size would have been preferred, the pool of available participants of high-risk youths were limited because they are a small subgroup of the general population, not all high-risk youths were accessing services at the non-profit organization, and their overall tendency to be suspicious of outsiders may have limited their comfort in participating in research.
Procedure
Ethics approval was obtained through the Interdisciplinary Committee on Ethics in Human Research (ICEHR) at a Canadian University. Youths were eligible for the study if they were between the ages of 16-to-24 years, and ineligible if they had a significant cognitive impairment, were not fluent in English, or were currently experiencing a psychotic episode.
Participants were recruited through an advertisement at a non-profit youth community center. To avoid any perception of coercion, recruitment was by advertisement invitation, and only those youths interested in the study were given appointment times to meet with the researcher. To address possible literacy issues, all measures and the consent form were presented orally to participants. To ensure privacy of responses and reduce social desirability, each participant endorsed items on a separate form, outside of the researcher’s field of vision. All participants received a $10 gift certificate for a local coffee shop for their time.
Measures
Sociodemographic information
Demographic information was collected through the Youth Participant Profile, a semi-structured interview developed by the non-profit agency. The interview was comprised of both opened and closed ended questions exploring sociodemographic information (i.e., gender, age, housing and employment history, family history, involvement in the criminal justice system). The average completion time for this measure was 20 to 30 minutes.
Attachment orientation
The Experiences in Close Relationships Scale-Revised (ECR-R; Fraley et al., 2000) is a 36-item measure of the two attachment dimensions of anxiety and avoidance. Each ECR-R item has a 7-point Likert scale (7 = strongly agree, 1 = strongly disagree) with half of the statements assessing discomfort with closeness and attachment avoidance (e.g., “I prefer not to be too close to others”); while the other half assesses fear of abandonment and need for contact, hallmarks of attachment anxiety (e.g., “My desire to be very close sometimes scares people away”). The ECR-R has been shown to have both high test-retest reliability (r = .86) (Sibley et al., 2005) and internal consistency (α = .94 for avoidance scale, α = .90 for anxiety scale) (Brennan et al., 1998).
Maltreatment
The Childhood Trauma Questionnaire Short Form (CTQSF; Bernstein et al., 2003) is a 28-item retrospective self-report questionnaire that is scaled across the five abuse domains of physical abuse, physical neglect, emotional abuse, emotional neglect, and sexual abuse. Participants rate each item on a five-point Likert scale from “never true” to “very often true.” The CTQSF has good test-retest reliability (Bernstein et al., 1994, 2003; Lipschitz, 1999) and excellent internal consistency (α = .91).
Self-compassion
The Self-Compassion Scale (SCS; Neff, 2003a) is a 26-item measure of self-compassion. The SCS includes six subscales: Self-kindness, self-judgment, common humanity, isolation, mindfulness, and over-identification. The SCS has good test-retest reliability (r = .93) (Neff, 2003a; Neff, Kirkpatrick, et al., 2007) and good internal consistency (α = .90–.95 for overall scores and .75–.86 for subscale scores). Neff and McGehee (2010) found no significant differences between adult and adolescent scores on the SCS, or between internal consistency coefficients (α = .90 for adolescents and α = .93 for adults). In the present study, the internal consistency of the SCS was high (α = .91).
Psychological distress
The Brief Symptom Inventory (BSI; Derogatis, 1993) is a 53-item measure of psychological distress indexing the degree to which the participant has experienced a specific symptom during the past week. Responses are measured on a five-point scale from “not at all” to “extremely.” The measure contains nine symptom scales: somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism, in addition to three global indices: global severity index (GSI); positive symptom distress index (PSDI), and positive symptom total (PST). In the current study, the GSI was used to measure psychological distress. The BSI has been shown to have good internal consistency (α = .71–.85). In the current study, the internal consistency of the BSI total score was high (α = .90).
Statistical Analysis
SPSS 25 was used to conduct the analysis. Data screening involved examining missing values, outliers, normality, skewness, and kurtosis. Data was checked for linearity, collinearity, multi-collinearity, homoscedasity, and non-zero variances. Due to the constraints on sample size inherent to this small study population, a sensitivity power analysis (as opposed to an a priori power analysis) was conducted using G*Power 3.1.9.4 (Faul et al., 2007). Given an alpha of .05, a power of .8, and the achieved sample size of 51, the minimum detectable effect (MDE) size for this study using Cohen’s (1992) criteria is a medium one (f2 = .16). Marsh et al. (2018) in their meta-analysis of studies using mostly non-clinical adolescent populations, consistently found a large effect size for the inverse relationship between self-compassion and psychological distress. Given these findings for a large effect in the extant literature on non-clinical adolescent populations, a medium MDE was deemed acceptable for the purposes of this study.
Pearson product moment correlations were conducted to determine the association between key demographic variables and the primary study variables. A hierarchical multiple regression was used to determine whether self-compassion uniquely contributed to the variance of psychological distress over and above attachment orientation and childhood maltreatment. Psychological distress was the criterion variable and attachment orientation, childhood maltreatment and self-compassion were the predictor variables. Entry into the hierarchical multiple regression was as follows: Block 1 sex (Male coded as 1, Female coded as 2); Block 2 attachment orientation (ECR-R anxiety and avoidance scores) and childhood maltreatment (CTQSF total score); and Block 3 self-compassion (SCS).
Results
Fifty-two youths participated in the current study. One youth identified as transgender and was not included in the final sample because the sample size would be too small to detect statistical differences. The final sample consisted of fifty-one youths.
The sociodemographic findings indicated that the ethnicity of the sample consisted of Caucasian (88.2%) and aboriginal (11.8%) groups. Although the participants were primarily Caucasian, which is unusual in published samples of high-risk youth, the limited ethnic diversity is consistent with the sociocultural dynamics of St. John’s. Approximately two-thirds of the sample (58.8%) reported dropping out of school due to learning disabilities, lack of interest, substance abuse, and mental health challenges. Over a third of participants reported difficulty with reading (33.3%) and writing (31.4%), with the majority of the sample not having completed high school (68.6%). Most of the youths reported symptoms of anxiety and depression (78.4%) with a substantial number reporting suicidal ideation (62.7%) and previous suicide attempts (49%) as well as the majority of participants (60.8%) self-reporting substance abuse. Finally, 27.4% of the sample were homeless at the time of the study, and 45.1% of the sample reported living on the street at some point in their lives.
Predicting Psychological Distress
Correlations between study variables (see Table 1), and key demographic variables, were calculated using the Pearson product moment correlation. As can be seen in Table 1, psychological distress was significantly correlated with sex (r = .338, p = .015), but not with age (r = −.084, p = .556). As expected, self-compassion was inversely associated with childhood maltreatment (r = −.418, p < .01), attachment anxiety (r = −.551, p < .001), attachment avoidance (r = −.487, p < .001), and psychological distress (r = −.332, p = .017).
Pearson Correlations between Primary Study Variables and Psychological Distress. a
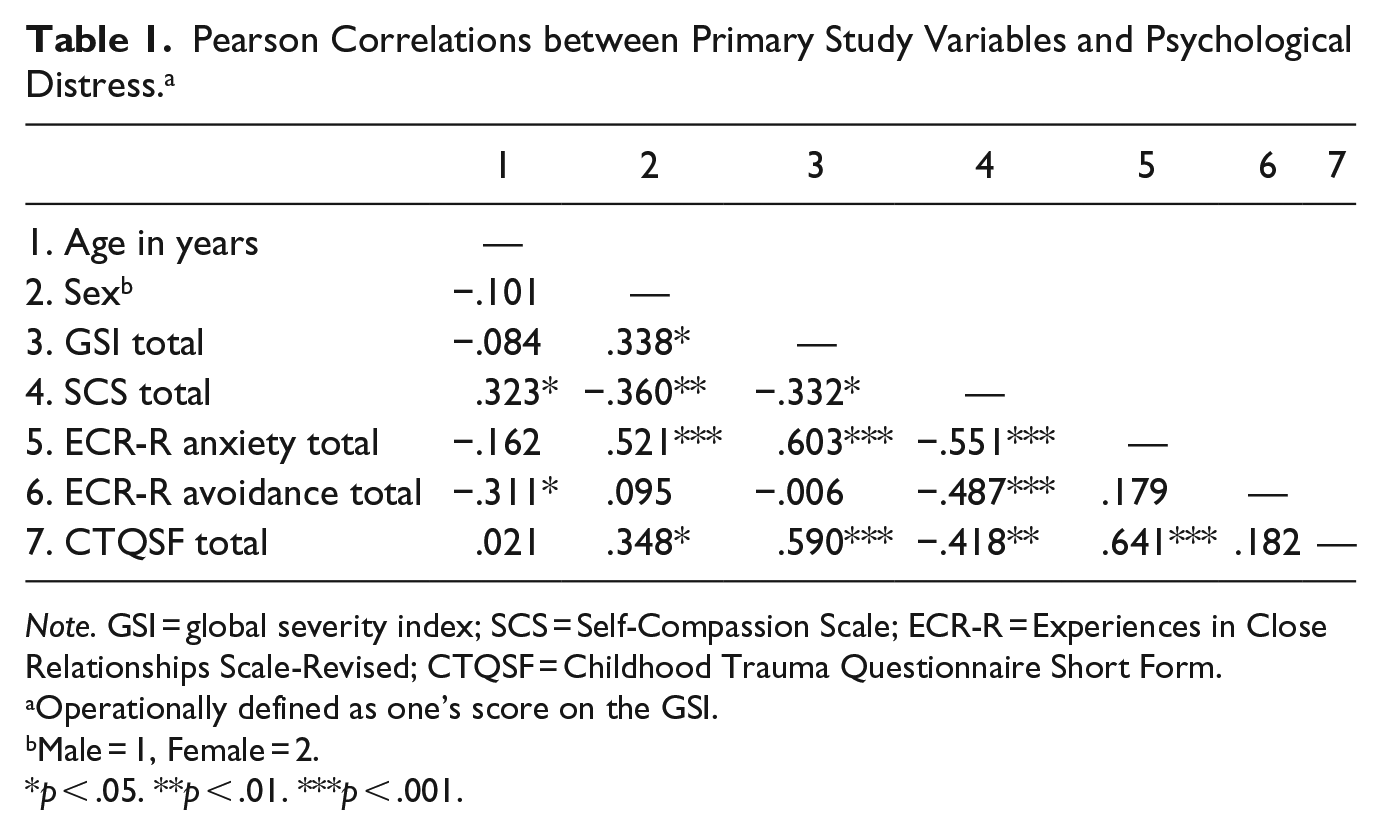
Note. GSI = global severity index; SCS = Self-Compassion Scale; ECR-R = Experiences in Close Relationships Scale-Revised; CTQSF = Childhood Trauma Questionnaire Short Form.
Operationally defined as one’s score on the GSI.
Male = 1, Female = 2.
p < .05. **p < .01. ***p < .001.
A hierarchical multiple regression was conducted to determine if the addition of self-compassion improved the prediction of psychological distress over and above attachment orientation (anxiety and avoidance [ECR-R] and childhood maltreatment [CTQSF total score]), after controlling for the sex of participant. Results (see Table 2) indicated that the full model of sex, attachment anxiety and avoidance, childhood maltreatment, and self-compassion to predict psychological distress was statistically significant, R2 = .456, F(5, 45) = 7.549, p < .001; adjusted R2 = .396. The addition of attachment orientation (anxiety and avoidance) and childhood maltreatment to the prediction of psychological distress (Model 2), led to a statistically significant increase in R2 of .340, F(3, 46) = 9.568, p < .001. However, the addition of self-compassion did not lead to a statistically significant increase in R2, R2 = .002, F(1, 45) = 0.139, p = .711. In the final model, sex of the participant (β = .041, t = 0.156, p = .876) and attachment avoidance (β = −.165, t = –1.300, p = .200) were no longer significant. The significant predictor variables that contributed to the variance of psychological distress were attachment anxiety (β = .362, t = 2.152, p = .037) and childhood maltreatment (β = .357, t = 2.480, p = .017). These results indicated that self-compassion, attachment avoidance, and sex did not significantly contribute to the variance of reported psychological distress, over and above attachment anxiety and childhood maltreatment.
Summary of Hierarchical Regression Analysis for Variables Predicting Psychological Distress a (N = 51).
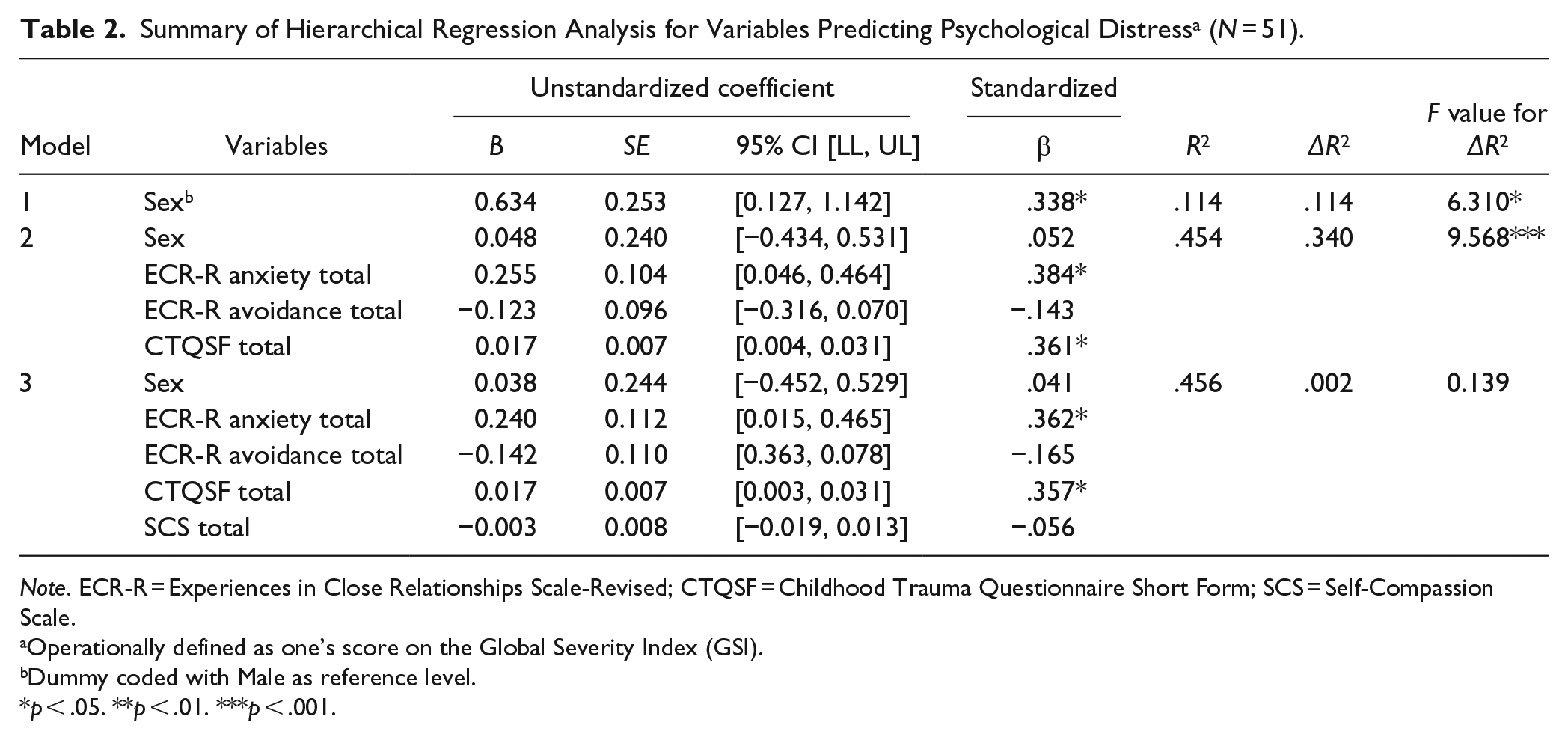
Note. ECR-R = Experiences in Close Relationships Scale-Revised; CTQSF = Childhood Trauma Questionnaire Short Form; SCS = Self-Compassion Scale.
Operationally defined as one’s score on the Global Severity Index (GSI).
Dummy coded with Male as reference level.
p < .05. **p < .01. ***p < .001.
Discussion
The purpose of the current study was to explore the role of self-compassion in high-risk youths as a possible protective factor. Our first objective was to examine whether self-compassion was inversely associated with insecure attachment orientations, severity of childhood maltreatment, and psychological distress. Our second objective was to determine whether self-compassion predicted psychological distress over and above attachment orientation and childhood maltreatment.
As expected, self-compassion was inversely related to attachment orientation (anxiety and avoidance), childhood maltreatment, and psychological distress. This result is consistent with previous research that found higher levels of self-compassion are associated with lower levels of maltreatment in high-risk youths (Tanaka et al., 2011; Vettese et al., 2011). Our findings were also consistent with Marsh et al. (2018) that found a large effect size for the negative association between self-compassion and psychological distress. The current study extends knowledge in the field of self-compassion by examining this self-construct in economically disadvantaged youths, many of whom were homeless at the time of data collection and were struggling to meet their basic needs. Low socioeconomic status (SES) has been shown to be an important factor associated with increasing rates of mental health problems in children and adolescents living in poor economic conditions (Reiss, 2013).
The current study found that self-compassion did not significantly predict psychological distress over and above childhood maltreatment and attachment anxiety. Attachment anxiety and childhood maltreatment accounted for almost half of the variance in psychological distress, while self-compassion and attachment avoidance were not included in the final model. This finding is consistent with previous research (Marsh et al., 2018) with high-risk youth samples with challenges such as substance abuse (Vettese et al., 2011), alcohol abuse, aggression, narcissism, serious suicide attempts, and high psychological distress (Kobak et al., 2015; Neff & McGehee, 2010; Neff, Rude, et al., 2007; Neff & Vonk, 2009; Van Dam et al., 2011) as well as developmental research findings (Cicchetti et al., 1993; Kessler et al., 2010; Lyons-Ruth & Jacobvitz, 2008; Zeanah et al., 2003). Although previous research has supported the effect of self-compassion for increased wellness (Neff, Rude, et al., 2007; Zessin et al., 2015), the preponderance of these studies involved nonclinical samples of high school and college students (Jativa & Cerezo, 2014; Neff & McGehee, 2010; Raque-Bogdan et al., 2011; Wei et al., 2011). In contrast, the youths in the current study were a community sample of high-risk and street-involved youths, most of whom prematurely left high school and were economically disadvantaged. The degree of adversity experienced by participants in the current sample was severe both in childhood and in their current life. To our knowledge, the current study is the first to examine whether self-compassion adds additional predictive value to psychological distress, over and above both attachment orientation and childhood maltreatment. Given the scarcity of research examining the role of self-compassion for high-risk youths, our finding suggested that this self-construct is less evident in high-risk youths.
Although attachment anxiety was a key construct in predicting psychological distress, attachment avoidance was not associated with psychological distress. This is not surprising given that previous research has shown that individuals with high scores in attachment avoidance commonly under report symptoms of distress when dealing with stressful environments (O’Loughlin et al., 2018). Under reporting of psychological distress has been associated with secondary strategies of deactivation, which involve suppression of distressing cognitions and emotions, as well as a rigid need for autonomy. Therefore, the lack of statistical relationship between attachment avoidance and psychological distress does not necessarily reflect a lack of distress, but rather suggests a type of self-protective behavior displayed by individuals higher on the attachment avoidance dimension (Fraley & Shaver, 1997; Neff & McGehee, 2010; Wei et al., 2011).
Self-compassion has been theorized to develop from the internalized voice and the modeling of caregivers (Neff & McGehee, 2010; Wei et al., 2011). Pepping et al. (2015) found that attachment anxiety predicted low self-compassion and suggested that the origins of self-compassion may stem from attachment orientation. Consistent with previous research, insecure attachment orientation in the current study was associated with lower levels of self-compassion (Neff & McGehee, 2010; Wei et al., 2011). The participants experience with caregivers were characterized as inconsistent, critical, rejecting, and abusive, which are all factors contributing to attachment insecurity. Any or all of these attributes could hinder the development of a secure attachment orientation (Pietromonaco & Barrett, 2000; Shaver & Mikulincer, 2009) and a self-compassionate voice. Therefore, participants likely had less opportunity to develop a self-compassionate voice within the environments they grew up in (Pepping et al., 2015). Another important factor for street-involved youths’ is the uncertain access to basic life needs (e.g., food, shelter, etc.), increasing anxiety that may contribute to challenges in developing a compassionate internal dialog. Given the barriers and threats that high-risk youths face daily, developing the self-construct of self-compassion may be more complex in this population.
Although the current study offers new insights into the association between self-compassion, attachment orientation, childhood maltreatment and psychological distress in high-risk youths, there are several limitations to the current study. First, the current study was a cross-sectional design in which the inferences about the direction of observed relationship and causality are unknown. For example, it is possible that self-compassion does not change the level of psychological distress, rather the level of psychological distress changes the way individuals speak to themselves. Second, the sample was small, restricting power and limiting the ability to detect less than a medium population effect size of self-compassion as a significant predictor of psychological distress over and above attachment orientation and child maltreatment. It is possible that a theoretically meaningful effect exists in the population of high-risk youths that could have been found with a larger sample size. Given that results were found in the current study with a small effect size for the addition of self-compassion further examination of this question is warranted. Although the current sample was small, high-risk youths are a challenging sample to enlist in research and the current study provided an important step in understanding the role of self-compassion for these youths. Finally, the psychological measures used in the current study did not include validity scales to determine the participants’ response style. A validity index would help clarify, for example, whether youths that were higher in attachment avoidance were under reporting their symptoms associated with psychological distress.
The current study results must be considered exploratory and in need of further investigation. Future research should take into consideration contemporary theories of attachment that recognize that attachment orientation is a dynamic construct, involving different attachment patterns within different relationships (Simpson & Karantzas, 2019). For example, some of the participants identified their relationships as secure and supportive. It is possible for youths to have a close friend that has been with them through difficult times, as a secure attachment relationship, whereas other relationships such as family members could remain insecurely attached. Contemporary attachment theory recognizes that an individual has multiple significant relationships in their life and based on the quality of these relationships different attachment orientations could develop with different people (Simpson & Karantzas, 2019). The dynamic view of attachment is also important for understanding how attachment orientation changes over time, dispelling the deterministic view that the child’s attachment relationship with their primary caregiver determines all future relationships.
In conclusion, self-compassion did not provide a protective effect to buffer the impact of attachment orientation and experiences of childhood maltreatment for psychologically distressed high-risk youths. However, self-compassion was negatively associated with attachment orientation, childhood maltreatment and psychological distress, suggesting that it may be a self-construct that is worthwhile targeting in treatment. The mindfulness underpinning of self-compassion may help dissipate the catastrophizing internal dialog associated with attachment anxiety, specifically issues associated with feelings of unworthiness, and fears of abandonment. Furthermore, mindfulness may help soften the deactivating strategies of youths high on attachment avoidance, allowing them to experience previously suppressed negative emotions and foster healthier ways of experiencing and processing those emotions.
Footnotes
Acknowledgements
The authors would like to thank the youths who participated in the research and their willingness to share their experiences. Ethics approval was obtained through the Interdisciplinary Committee on Ethics in Human Research (ICEHR) at a Canadian University.
Authors’ Note
Dataset used is not available to access as ethics approval is based on the dataset remaining confidential and any release, though de-identified, could potentially still be used to identify participants due to the small patient population in the province of study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.