
Abstract
In New Zealand, and globally, concerns that living in areas of concentrated social housing will depress the outcomes of its tenants have led to policy directives to limit the proportion of social housing in any one community. This study explores the rationale for these initiatives through the innovative use of administrative linked data for 200,000 New Zealand social housing tenants. We analyse associations between the concentration of social housing (as measured by the proportion of social housing tenants relative to the rest of the area population) and their education and health outcomes seven-to-nine years later. We find that – contrary to policy assumptions – outcomes for social housing tenants are similar or slightly better when they have lived in areas with more concentrated social housing.
Introduction
In countries where social (or public) housing is targeted at the most deprived populations, areas of concentrated social housing have long been viewed with suspicion. Depending on the country, they have been described as ‘sink estates’ or ‘ghettos’ (Gans, 2010; McDonald, 2015; Pagani et al., 2025; Pinkster et al., 2020; Slater, 2018; Wilson, 1987), a view that often contrasts with the perspectives of those that live there (Darcy, 2013; Watt, 2020). Proponents of deconcentrating social housing argue that deprived residents are further disadvantaged because their housing is isolated from people with high socio-economic status, which reduces their access to positive role models, beneficial social networks and superior amenities (Galster, 2012; Gans, 2010). They propose that social housing tenants would be better off housed in areas where social housing makes up a limited proportion of the stock. This idea of area or neighbourhood effects has been highly influential. It has helped to justify the demolition of concentrated social housing and its replacement with mixed-tenure communities, where the proportion of social housing is limited to, for example, between 20% and 30% (Chisholm et al., 2021b; Darcy, 2013; Górczyńska-Angiulli, 2023; Khor et al., 2023). Yet the argument that these policies benefit tenants is challenged by tenants and by researchers (Gans, 2010; Gordon et al., 2017; Slater, 2013; Watt and Smets, 2017).
Our study explores the evidence for social housing deconcentration policies by investigating the association between the concentration of social housing and tenant education and health outcomes in New Zealand. We do this through identifying the degree of social housing concentration in areas across New Zealand in 2013, as measured by social housing tenants as a proportion of the population. We look at the outcomes of these 200,000 tenants in 2021. The time-lag between measuring social housing concentration and investigating tenant outcomes is important because the processes that could affect outcomes are likely to take some time to have an effect (Musterd et al., 2012; van Ham and Manley, 2010). Education and health were selected as outcomes because of their importance in policy and research discussion on this issue (Graham et al., 2009; Kearns and Mason, 2007; Robison et al., 2016; Sautkina et al., 2012; Woods, 2023), and the fact that ‘higher order’ outcomes such as health and education are likely to capture gains in intermediate outcomes (Graham et al., 2009).
To conduct the study, we draw on New Zealand’s integrated administrative data: de-identified linked records of individual’s interactions with government services, as well as Census and survey data (Milne et al., 2019). Linked administrative data has many advantages in evaluating government policies, such as avoiding self-reported outcomes and amassing a large sample (Busch-Geertsema et al., 2016; Hinds et al., 2019). While we cannot determine causality, we find that living in more concentrated social housing was associated with better health and educational outcomes for social housing tenants. Our study is the first to investigate educational outcomes in relation to social housing concentration in New Zealand.
Our paper proceeds as follows. First, we introduce the literature on international social housing deconcentration policies, and the existing evidence on the association between social housing concentration and key social outcomes. Next, we contextualise our own study through outlining New Zealand social housing, the policy preference towards social housing deconcentration, and the limited evidence on its effectiveness. The methods section introduces the administrative data used to conduct the analyses. We next outline our results: our sample, and the associations between social housing concentration and outcomes relating to health and education. The discussion summarises these results and contextualises them within the literature and the New Zealand policy setting. We conclude with policy recommendations.
Literature
It is important to provide evidence on the associations between social housing concentration and tenant outcomes because policymakers’ belief that social housing concentration is harmful has spurred enormous urban restructuring worldwide (Casarin et al., 2023; Levin et al., 2022). As public housing advocates in the United States put it, ‘deconcentration theory fuels current public housing policy’ (Right to the City Alliance, 2010: 15). Ideas about the desirability of residential socio-economic or tenure ‘balance’ or ‘mix’ have periodically resurfaced in countries including the United Kingdom, the United States, Australia and New Zealand since the 1800s (Arthurson, 2008; Chisholm et al., 2022b; McFarlane, 2019; Sarkissian, 1976). However, the last three decades have seen a particular focus on operationalising this ideal through the demolition of social housing estates, buildings and neighbourhoods. The typical target is ageing social housing that has lacked maintenance and investment, and that is located centrally and convenient to amenities (Arthurson et al., 2015; Lees, 2014). Deconcentrating social housing entails replacing it with new ‘mixed tenure’ communities where social housing exists alongside market housing (Casarin et al., 2023; Levin et al., 2022). Whether implemented by the private or the public sector, the optimal proportion of social housing in these developments is typically set at somewhere between 20% and 30% (Chisholm et al., 2021b; Darcy, 2013; Górczyńska-Angiulli, 2023; Khor et al., 2023). This ‘tenure diversification’ strategy has been criticised for displacing social housing tenants, promoting gentrification and subjecting tenants to stigma within the new communities (August, 2016; Chisholm et al., 2024; Corcillo and Watt, 2023; Davidson, 2008).
Those that argue for social housing deconcentration, and for housing social tenants in mixed-tenure communities alongside market residents instead, imagine that this could result in better outcomes (Chisholm et al., 2022a; Sautkina et al., 2012). Researchers have investigated major outcomes thought to be associated with such policies, including health, education, employment and perceived crime or anti-social behaviour (Kim et al., 2022; Kleinhans, 2004; Lindberg et al., 2010; Sautkina et al., 2012; Saville-Smith et al., 2015). Other studies look at the theorised mechanisms through which these outcomes are thought to result: social capital or interaction between tenure groups (Camina and Wood, 2009; Levin et al., 2022; Thurber et al., 2018), neighbourhood reputation/satisfaction (Arthurson, 2013; August, 2014; Kleinhans, 2004), the quality of neighbourhood services/amenities (Arbaci and Rae, 2013; Arthurson, 2010; Atkinson and Kintrea, 2004; Coley et al., 2023; Musterd, 2008). We now turn to studies that, like our own, draw on routinely collected administrative data to examine associations between social housing concentration and these two key outcomes. They are descriptive and cannot attribute causality. We do not discuss studies which examine social housing tenant outcomes when moving to low-poverty areas. As noted by Sautkina et al. (2012), it is not clear that the poverty rate measure (used in the United States) is equivalent to the level of social housing measure, used by policymakers including in New Zealand and the United Kingdom.
Relation between social housing concentration and health outcomes
Proponents of social housing deconcentration argue that this could improve social tenant health through their observing and adopting the healthier behaviours of the presumably wealthier market residents, or through accessing superior health-promoting amenities (i.e. green space, safer streets, better medical facilities) associated with middle-class advocacy (Graham et al., 2009; Kearns and Mason, 2007). However, the evidence is sparse (Sautkina et al., 2012; Saville-Smith et al., 2015). We identified five relevant studies. A United States study found no difference in the health characteristics of the social networks of public housing tenant children living in mixed communities as opposed to concentrated public housing (Kennedy-Hendricks et al., 2015). An Australian study showed that the score for median mental wellbeing was the same for social housing tenants living in areas where the proportion of social housing ranged from 1.83% to 41.22% of households; it was better when tenants lived in areas with less than 1.83% social housing (Parkinson et al., 2014: 39). A New Zealand study showed that social housing tenants’ health (as measured by hospitalisations, pharmaceutical dispensing, and mental health outpatient events) was slightly better when they lived in areas with greater proportions of social housing (Chisholm et al., 2022b). Two observational studies carried out in the United Kingdom examined associations between the proportion of social housing in an area and health for the population as a whole, rather than social housing tenants; mixed results meant they concluded that policies to reduce social housing concentration to improve ‘mix’ are unsupported by evidence (Graham et al., 2009; Lawder et al., 2014).
Relation between social housing concentration and educational outcomes
It is theorised that reducing the concentration of social housing (and housing a greater proportion of market residents) could improve social housing tenant education outcomes in two ways. First, provided children from market and social housing households attend local schools together – which is by no means guaranteed (Chisholm et al., 2022a) – social housing tenant children may benefit from superior education at better-resourced schools, due to a greater proportion of parents who are wealthier and may be more likely to advocate and fundraise for their school (Kearns and Mason, 2007; Robison et al., 2016). Second, whether at school or not, social housing tenant children with advantaged neighbours may benefit from role model influence and collective socialisation effects which reinforce a positive attitude to educational attendance and attainment (Kearns and Mason, 2007; Robison et al., 2016). However, the evidence base for associations between social housing concentration and educational attainment is sparse (Sautkina et al., 2012). We identified two relevant studies. Weinhardt (2010, 2014) found that students (age 14) in England who moved earlier to a neighbourhood with more than 80% social housing experienced no negative effect on educational attainment, compared to those who moved later. Another study in England found that living in an area with a ‘high’ (more than 75%) share of social renters did not affect educational attainment; ‘the implication is that – on the educational dimension at least – programmes to promote socio-economic mixing in communities through residential relocation are unlikely to be effective’ (Gibbons et al., 2013: 868).
The New Zealand case
Social housing was built throughout urban New Zealand in large numbers in both small and large concentrations in the years and decades following World War II (Bergstrom et al., 2011; Schrader, 2005). As this housing became increasingly targeted towards disadvantaged people, New Zealand policymakers and social critics became concerned that living in areas where social or public housing is spatially concentrated might adversely impact the outcomes of social housing tenants (Chisholm et al., 2021b, 2022a, 2022b; Ferguson, 1994; Schrader, 2005). Yet, relative to countries such as England, from which it draws policy inspiration, New Zealand has low concentrations of social housing tenants. For example, one study identified 10 areas (when an ‘area’ was a statistical unit averaging 1500 residents) in London with at least 40% social housing (and 40% owner-occupied housing; Arbaci and Rae, 2013). In New Zealand in 2013, drawing on a similarly-sized statistical area unit (median of 1863 people), only about 15% of the social housing tenant population lived in areas where more than 40% of the population is a social housing tenant (Chisholm et al., 2022b).
Despite this, New Zealand has echoed the common international approach described in the previous section over the past 15 years: demolish communities of social housing and replace them with mixed tenure communities where the proportion of social housing ranges from 13% to 40% (Chisholm et al., 2022a). These range from small communities to large suburbs: in Pomare, 89 social homes were replaced by 150 homes, 13% of which were social homes; in Tamaki, 2500 social homes are being replaced by 10,500 homes, 27% of which are social homes (Chisholm et al., 2022a). The state’s housing agency notes that ‘we currently turn down opportunities [to develop housing] due to concerns about the extent of concentration of public housing in the community’ (Kinga Ora (KO), 2021: 9).
Describing the rationale behind a new government development housing private as well as social housing tenants, the Minister of Housing noted that a key benefit was ‘improved life outcomes – employment, health and educational – for public housing tenants’ (Woods, 2023). The belief that limiting the proportion of social housing in a community benefits social housing tenants is widespread in government, community and private organisations involved in social housing delivery (Chisholm et al., 2022a; Fergusson et al., 2016; Simonsen, 2018; Woods, 2023). This is despite reports from social housing tenants in areas targeted for deconcentration about the strength of their communities (Chisholm, 2016; Cole, 2015; Gordon et al., 2017; Waldegrave et al., 2013), and a government-commissioned literature review that noted the weakness of the international evidence base for deconcentrating social housing (Saville-Smith et al., 2015).
Today, social housing makes up about 3.8% of New Zealand’s total housing stock, a drop from a peak of around 7% of the total housing stock in the early 1980s, and below the OECD average of 6.9% (PWC, 2023). Social housing in Aotearoa is provided by the government agency, Kāinga Ora – Homes and Communities (Kāinga Ora), which provides 75,000 homes for 191,000 people, and community housing providers, which provide 26,000 homes for 35,000 people (CHA, 2024; KO, 2024). Social housing is targeted at people with low socio-economic status and health disadvantages that make it difficult for them to secure housing in the private market. Once placed in social housing, tenants pay no more than 25% of their income in rent (Ministry of Housing and Urban Development, 2025). Reflecting the disparities wrought by colonisation, discrimination and institutional racism, Māori and Pacific people are disadvantaged compared to other populations and therefore overrepresented in social housing (KO, 2024; Walker, 2004). Compared to the general population, social housing tenants had significantly lower average incomes (less than half), were more likely to be female, had larger households on average, were less likely to have completed high school (Smith and Davies, 2020) and had poorer health outcomes (Pledger et al., 2019). However, New Zealand research shows that being housed in social housing improves health outcomes (Fasoro et al., 2024) and reduces youth offending (Yu et al., 2025), and that self-reported wellbeing outcomes can be broadly comparable between homeowners and long-term social housing tenants (Grimes et al., 2024). Relative to low-income housing in the private rental sector, social housing tenants benefit from more affordable rent, greater security and a more responsive and sympathetic landlord (Chisholm et al., 2021a; Morris, 2009; Russell et al., 2023).
New Zealand has insufficient social housing to meet needs. At the time of the 2023 Census, 112,496 people or 2.3% of the population, were severely housing deprived (Statistics New Zealand, 2024). There were 19,000 applicants for social housing registered as of March 2025 (Ministry of Social Development, 2025). Efforts to limit the concentration of social housing risk limiting the social housing stock available. Therefore, the idea that social housing concentration is harmful should be subject to scrutiny. In the next section, we explain how we do this.
Methods
Data
The research drew on the Integrated Data Infrastructure (IDI), through which we gained access to the number and proportion of social housing tenants versus the total population in different areas, and the health and education outcomes of those tenants. The IDI is a collection of linked individual records for the whole New Zealand population from routinely collected administrative data sources including government agencies, surveys and the census. All data are de-identified and linked by Statistics NZ, allowing us to combine data from all available sources without breaking any individual’s privacy. Access to these data is only available to approved researchers in a restricted data-lab environment. The output relating to this project was externally assessed by Statistics NZ to ensure confidentiality for all individuals is maintained. We reconciled Census data and Housing New Zealand (HNZ; now Kāinga Ora – Homes and Communities) data to establish the proportion of HNZ residents (henceforth ‘social housing tenants’) compared to the total population in each statistical area on Census Day in 2013. We describe this as ‘social housing concentration’. We retrieved information on social housing tenancy from the HNZ dataset. We drew on the Statistical Area 2 (SA2) unit, which housed 2000–4000 residents in city council areas and 1000–3000 residents in district council areas (Statistics New Zealand, 2022).
Demographic and outcome measures
We retrieved the demographic information of the tenants and their household members from the personal detail dataset. Using the administrative population census time series dataset, we identified the SA2 where the cohort lived in 2013. We retrieved the deprivation index of the SA2 the cohort lived in by reconciling the meshblocks in each SA2 with the meshblocks in the 2013 deprivation index metadata. The health outcome analysed is the hospitalisation rate; while being hospitalised represents the extreme end of the spectrum, it serves as a proxy for general health. The hospitalisation data was retrieved from the Ministry of Health Minimum Dataset which contains publicly funded hospital discharge and event records. The education outcomes analysed are participation in and results pertaining to the National Certificate of Educational Achievement (NCEA) which were sourced from the Ministry of Education. The NCEA is New Zealand’s national qualification for secondary school students. It comprises three levels; since it is optional for schools to offer level 1, we only considered levels 2 (year 12, age 16–17) and level 3 (year 13, the final year of school: age 17–18). School attendance is compulsory until age 16. Participation in NCEA signifies attendance at school and includes both those who achieved and those who failed to achieve the NCEA level. We assessed the proportion of students who participated in the NCEA levels. We also present the data in bar charts as a sensitivity check (Appendices 3–5).
Analysis
We included 200,910 tenants who lived in social housing from 2012 to 2014 in our final analysis (Table 1). Of this sample, 18,723 were deceased in 2021 and were excluded from the analysis. We analysed the proportion of social housing tenants in the population in the statistical areas where social housing tenants lived in 2012–2014. We then analysed health and education outcomes for those individuals in 2021. This allowed us to estimate how the concentration of social housing relates to outcomes seven-to-nine years later. This period of observation is important because the processes that could affect outcomes are likely to take some time to have an effect (Musterd et al., 2012; van Ham and Manley, 2010). This period is slightly less than van Ham and Manley’s (2015) choice of 10 years because of the availability of Census data. We also analysed the difference in hospitalisations and education between different groups within social housing in the regression models.
Demographics of social housing tenants and general population in 2013.
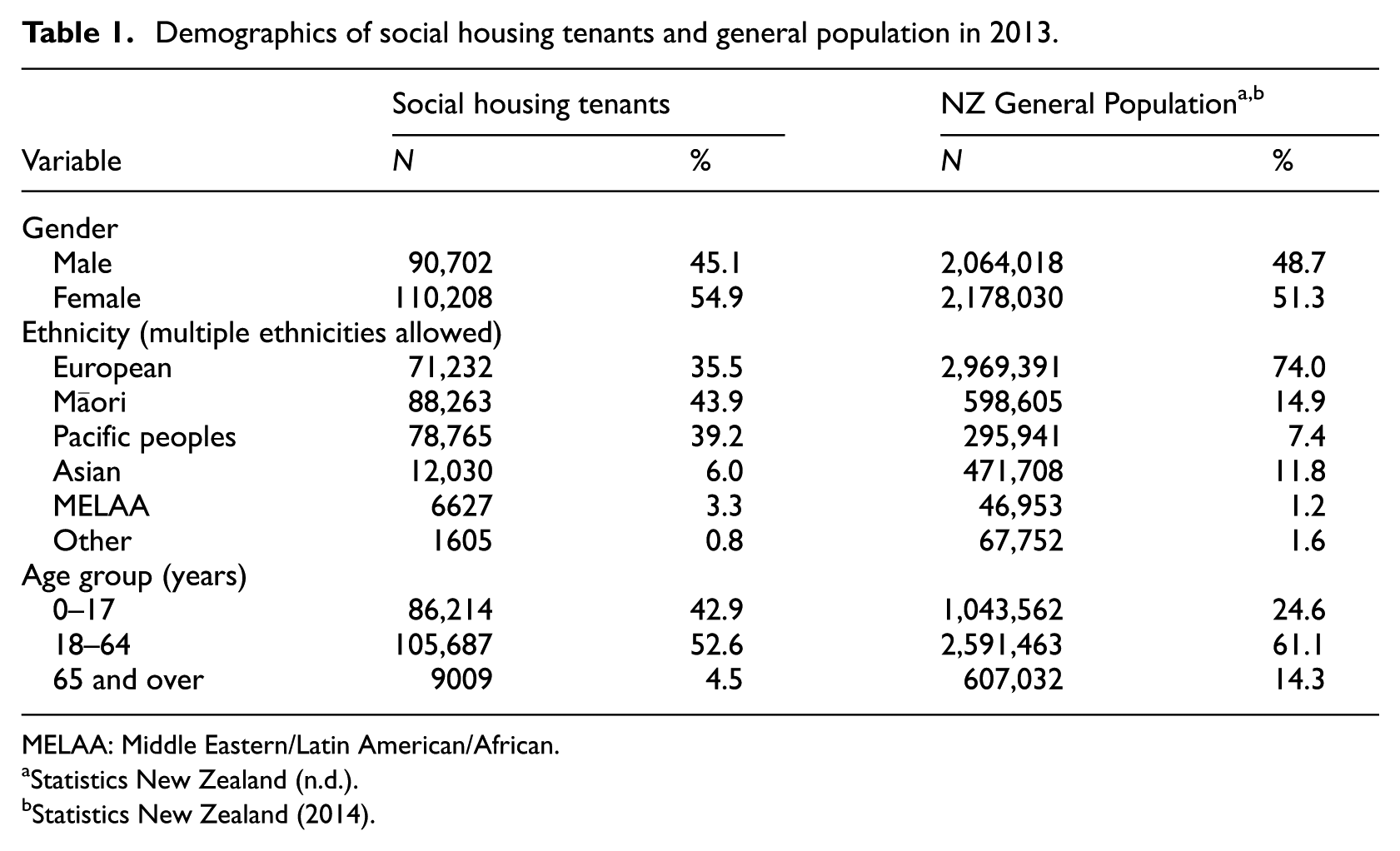
MELAA: Middle Eastern/Latin American/African.
We use graphs to show the relationship between the percentage of social housing tenants in the statistical area where social housing tenants lived in 2012–2014, and their outcomes in 2021 (Figures 1 and 2). The different levels of the proportion of social housing tenants in the population are grouped together in percentile groups. The area of the dot represents the size of the population. The x coordinate represents the mean social housing concentration. The y coordinate represents the outcome measure. We used linear regression lines to visualise the relationship between variables and the trends in the data using the ggplot2 package in R studio (R Core Team, 2023; Wickham, 2016). There was evidence of overdispersion, so we fitted a quasi-Poisson regression model to hospitalisation counts (Table 2). We used binary logistic regression models to examine the association between participation in the NCEA levels and the independent variables (Tables 3 and 4). NCEA participation was dichotomised: 1 signifies participation in that NCEA level, and 0 signifies no participation. We used a stepwise selection method to identify variables to be included in the final model. Prior to fitting the final model, we assessed multicollinearity among the predictor variables using the Variance Inflation Factor (VIF). All the VIF values shown in Tables 2–4 suggest that there were no high correlations among the variables, and multicollinearity was not a significant issue in the models.
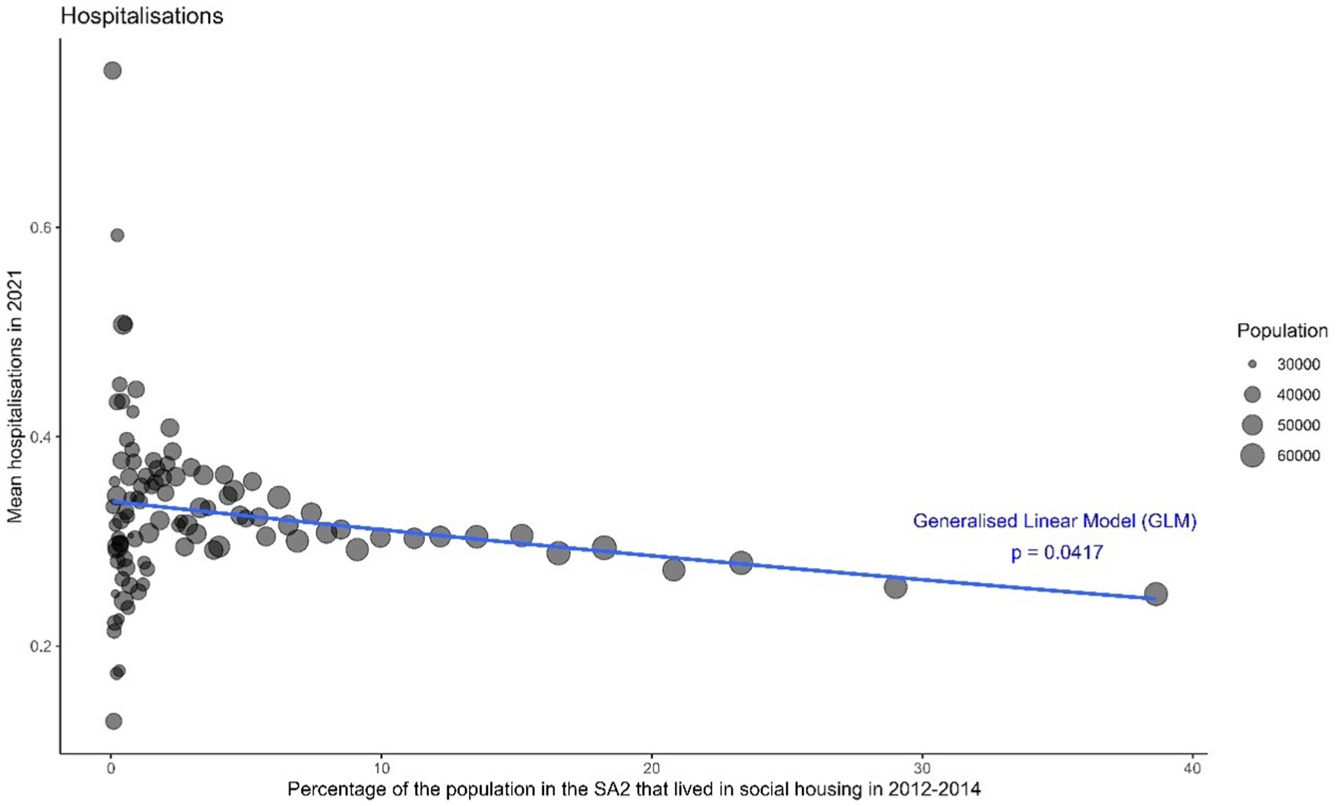
Relationship between social housing concentration where social housing tenants lived in2012–2014 and their mean rates of hospitalisation in 2021.
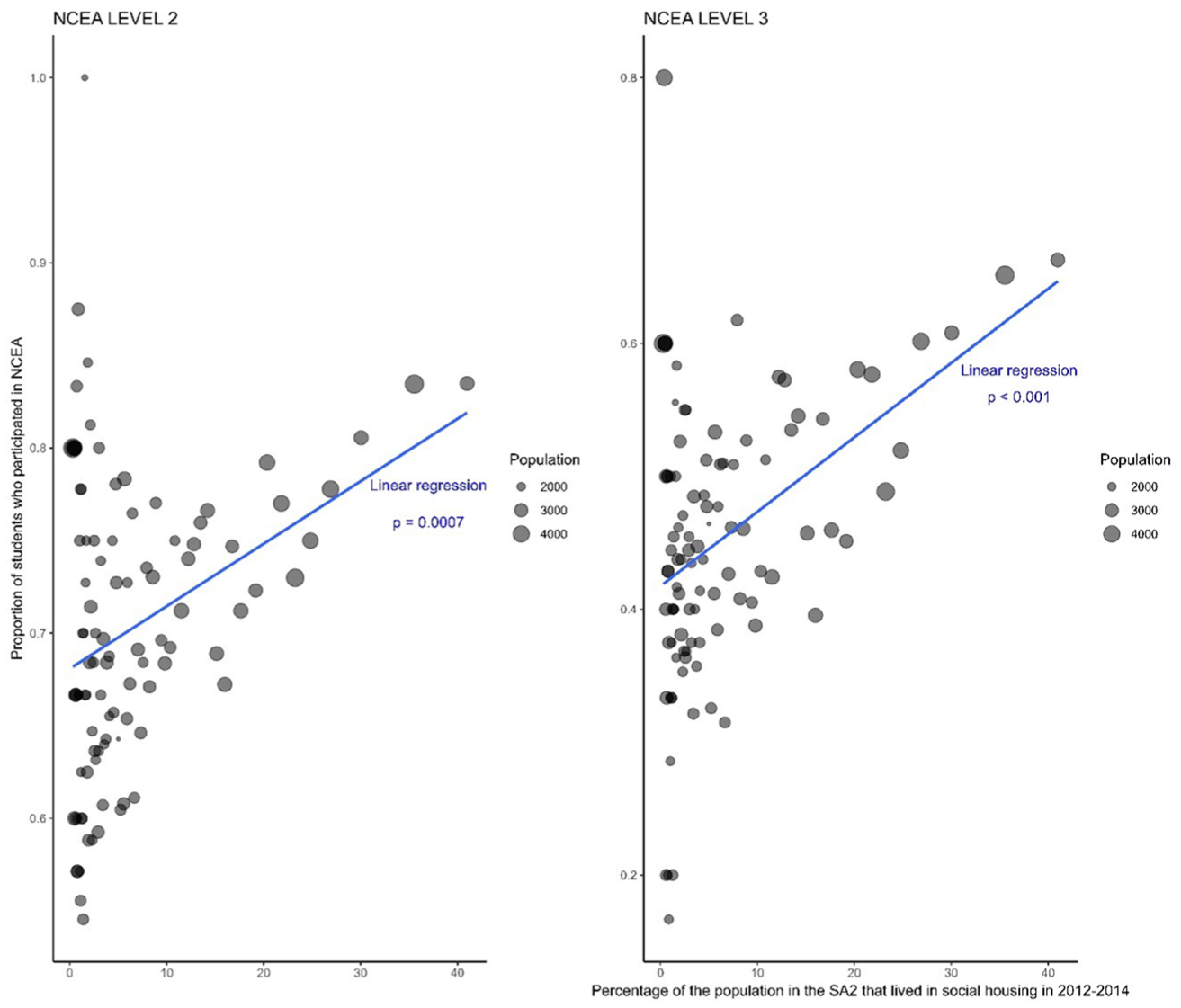
Relationship between social housing concentration where social housing tenants lived in2012–2014 and their NCEA levels 2 and 3 participation rates by 2021.
Poisson regression results for a model of hospitalisations for people living in social housing between 2012 and 2014.
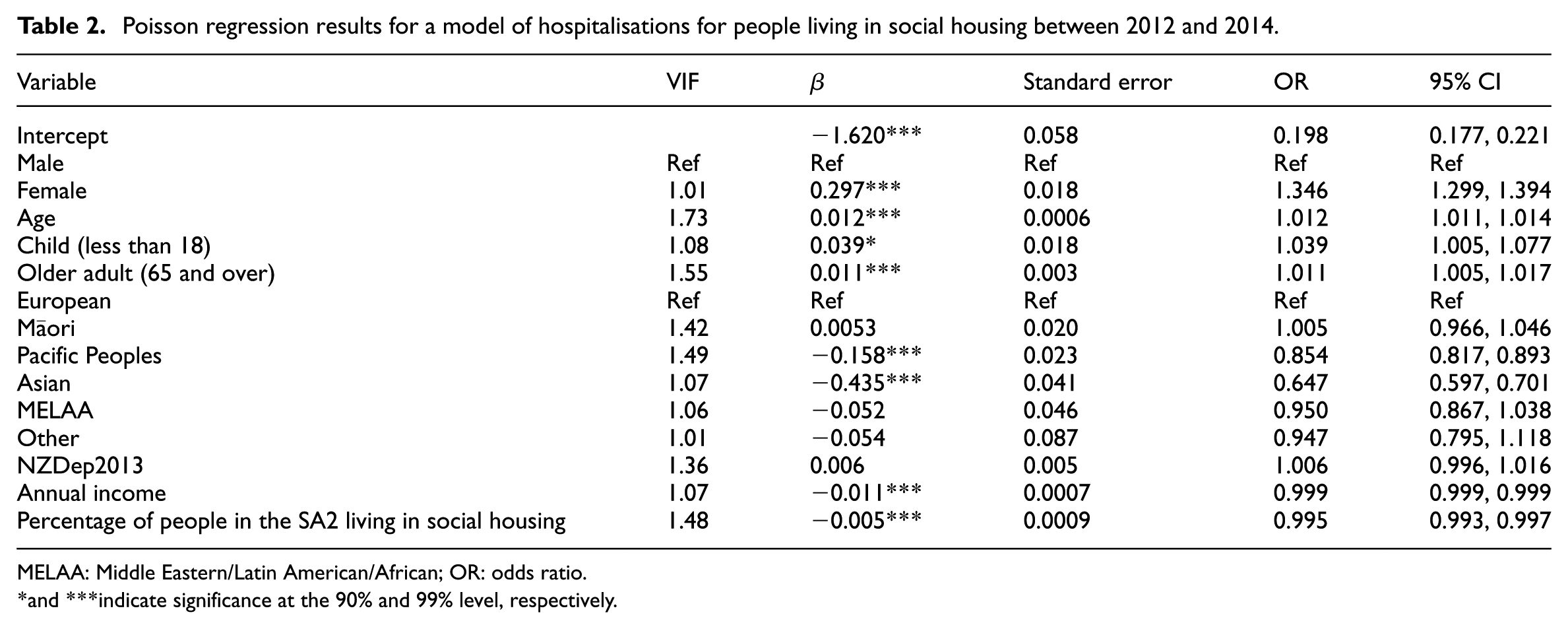
MELAA: Middle Eastern/Latin American/African; OR: odds ratio.
and ***indicate significance at the 90% and 99% level, respectively.
Binomial regression results for a model of NCEA Level 2 participation for children living in social housing between 2012 and 2014.
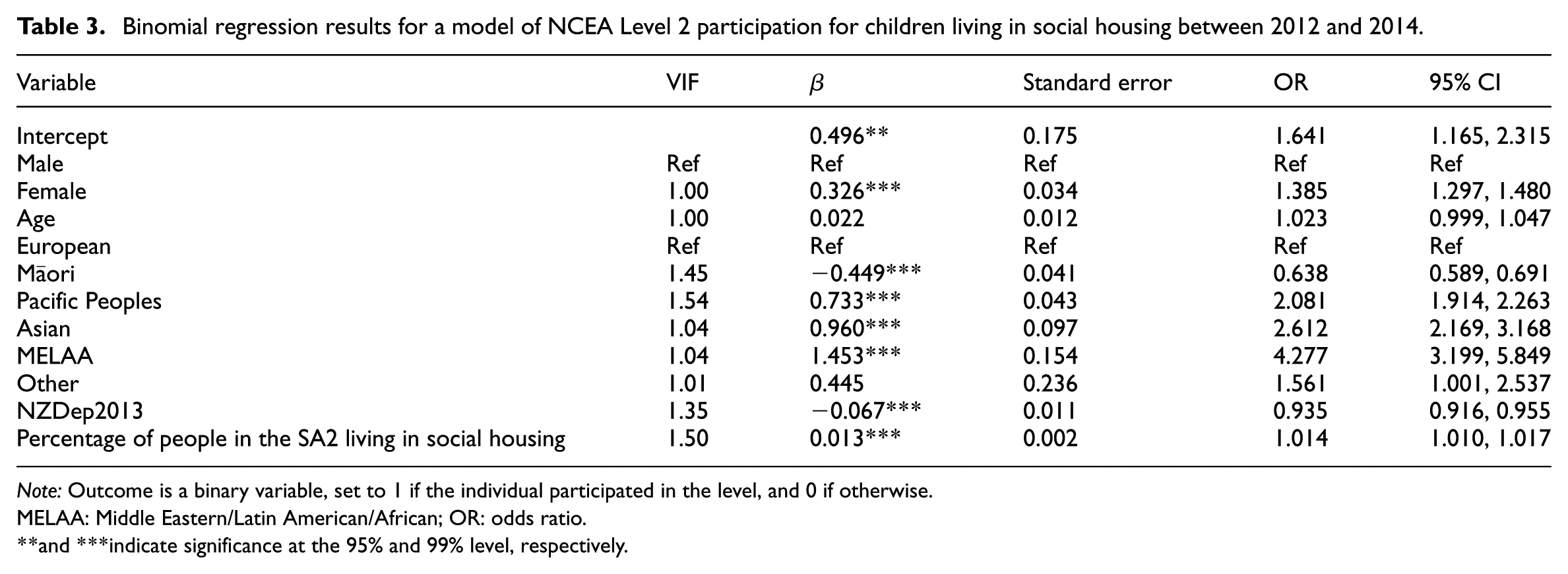
Note: Outcome is a binary variable, set to 1 if the individual participated in the level, and 0 if otherwise.
MELAA: Middle Eastern/Latin American/African; OR: odds ratio.
and ***indicate significance at the 95% and 99% level, respectively.
Binomial regression results for a model of NCEA Level 3 participation for children living in social housing between 2012 and 2014.
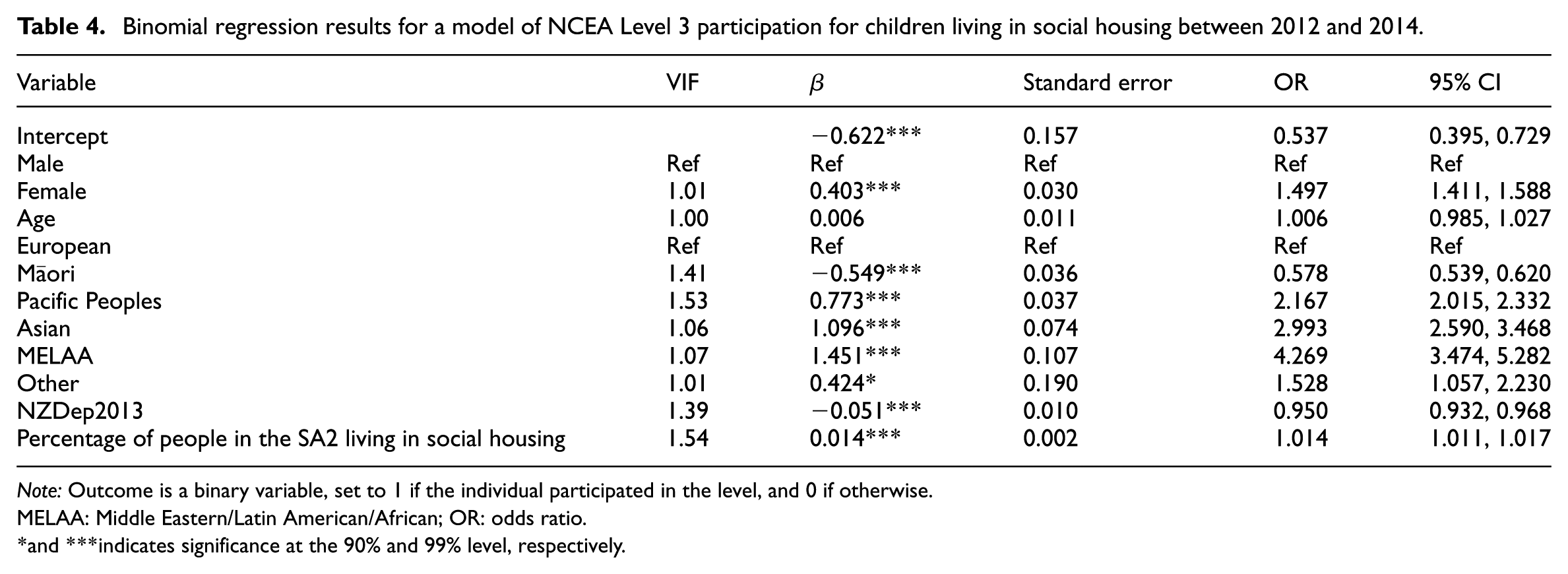
Note: Outcome is a binary variable, set to 1 if the individual participated in the level, and 0 if otherwise.
MELAA: Middle Eastern/Latin American/African; OR: odds ratio.
and ***indicates significance at the 90% and 99% level, respectively.
Results
Of our sample of 200,910 individuals who lived in social housing from 2012 to 2014, the majority were females (54.9%) and adults aged 18–64 years, while a significant proportion were Māori (43.9%) and Pacific (39.2%) (Table 1).
The association between social housing concentration and health outcomes
We looked at hospital admissions among social housing tenants in 2021. The mean number of hospital admissions was 0.3 in 2021 (Appendix 1). This is higher compared to the hospitalisation rate (0.21) reported in the general population in the same year (Health New Zealand, 2024). The regression model shows that female social housing tenants are 1.35 times more likely to be hospitalised compared to their male counterparts (Table 2).
We examined the relationship between hospital admissions for social housing tenants and the concentration of social housing in the statistical areas where they lived seven-to-nine years earlier. Figure 1 shows there was a steady decrease in the rate of hospitalisations as the proportion of social housing tenants increased in the statistical areas. 1 Each percentage increase in social housing concentration is associated with a 0.5% reduction in the odds of being hospitalised. For example, tenants who had lived in areas where social housing tenants were 2.2% of the population had a mean hospitalisation rate of 0.41. This reduced to 0.26 in the same year for people who had lived in areas with 29% social housing tenants. Therefore, the hospitalisation rate of those who lived in areas with low concentration of social housing (e.g. where 2% of the population are social housing tenants) was about 58% greater than those who lived in areas of high concentration (e.g. where 29% of population are social housing tenants).
The association between social housing concentration and educational outcomes
We found that the number of children aged 10–14 living in social housing in 2012–2014 was 20,133. We looked at their participation rates in NCEA levels 2 and 3 by 2021. Figure 2 shows a significant relationship between participation in NCEA levels 2 and 3 and the concentration of social housing. Social housing tenants’ children who lived in areas with higher proportions of social housing tenants participated in NCEA levels 2 and 3 more than those who lived in areas with low proportions of social housing.
We also conducted analyses to see which other factors, besides social housing concentration, were associated with children being more likely to participate in NCEA levels 2 and 3. Female and non-Māori children were more likely to participate in NCEA levels 2 and 3 than the general population of social housing tenants (Tables 3 and 4).
Discussion
Our analyses showed that, contrary to current policy assumptions, living in areas with greater proportions of social housing does not harm tenant outcomes. We found that education and health outcomes were slightly better for tenants who had lived in more concentrated social housing seven-to-nine years earlier. Our study is the first to explore associations between social housing concentration and educational outcomes in New Zealand. Our findings agree with the majority of the international literature that shows that living in more concentrated social housing does not have adverse effects (Chisholm et al., 2022b; Gibbons et al., 2013; Graham et al., 2009; Lawder et al., 2014; Parkinson et al., 2014; van Ham and Manley, 2010; Weinhardt, 2010).
Our study distinguishes itself from the extant literature in showing that, in the case of health and education, there was a slight advantage for social housing tenants living in more concentrated social housing. It supports a previous study (Chisholm et al., 2022b) on the health advantages for New Zealand social housing tenants of living in more concentrated social housing, with an enriched dataset. Our study drew on a large area unit (2000–4000 people). We note that a New Zealand study which drew on similarly sized area unit, as well as a small area unit (median 78 people), found similar results in both area units (Chisholm et al., 2022b).
The advantages of living in more concentrated social housing may be explained by the additional resources that may be more available to tenants in these areas. First, a number of studies have reported that social housing tenants provide mutual support that results in positive social outcomes, for example, through providing lifts to medical treatment, childcare, and access to food (Chisholm et al., 2024; Keene and Geronimus, 2011; Russell et al., 2023). Second, social housing tenants in areas of greater social housing concentration may benefit from services that are offered only in deprived areas (recognising that these align with areas of high-social housing concentration, as per Appendix 2). Such services include subsidised doctor’s visits under the Very Low Cost Access scheme, available to medical practices that have more than 50% of patients living in high-poverty areas (Whitehead et al., 2020), or free school lunches under the Ka Ora, Ka Ako programme, available in schools that have high proportions of children from low-socio-economic households enrolled (Garton et al., 2023). Finally, in New Zealand, socio-economically deprived areas (which include areas with high social housing concentration as per Appendix 2) have superior access to community resources (including supermarkets, and education, health and recreational facilities; Pearce et al., 2007). This points to the fact that these resources, which are likely to support health and education outcomes, are more available to tenants in areas of higher social housing concentrations.
Our study has several strengths. It draws on a large sample – over 200,000 people – and is based on individualised rather than aggregated data. The seven-to-nine-year gap between the initial observation of tenure mix and the measurement of outcomes enables us to take into account that context is likely to take some time to influence outcomes (van Ham and Manley, 2015). Unlike many of the studies we reviewed, our study specifically reports on outcomes for social housing tenants, rather than for residents in general. However, there are some limitations in our study design. First, although duration of exposure to a neighbourhood may influence outcomes (Musterd et al., 2012), our study does not investigate how long tenants remained living at that level of social housing concentration. However, the fact that mean time spent in social housing for our sample was about nine years (Appendix 1) means it is likely that most of them remained in the same home in 2021 (when outcomes were measured) as in 2012–14 (when social housing concentration was measured). We do not investigate the effects of area deprivation; however, we note that neighbourhoods with high concentrations of social housing are the most deprived neighbourhoods in New Zealand (see Appendix 2): as noted earlier in the paper, people enter social housing under strict criteria, which means that they are a highly deprived population relative to the New Zealand population.
Given that our study implies that reducing social housing concentrations would not improve tenant outcomes, what then could? There is a wealth of evidence, from New Zealand and beyond, about what does improve the outcomes of social housing tenants: affordable energy and rent, well maintained and high quality housing and tenure security (Garnham et al., 2022; Grimes et al., 2024; Moore et al., 2018; Rolfe et al., 2020; Thomson et al., 2013). There is also strong evidence that social housing itself supports education and health outcomes, due in part to the security, quality and affordability it offers relative to alternatives in the private rental market in many countries including New Zealand (Dunn et al., 2024; Fasoro et al., 2024; Grimes et al., 2024; Han and Schwartz, 2024; Hinds et al., 2019; Pierse et al., 2022; Pollakwoski et al., 2022). This underlines the importance of challenging the sale of social properties and limits to social housing concentration. Social housing deconcentration often leads to less social housing, when it is greatly needed. By limiting social housing supply, such policies to engineer communities have been identified as ‘fixes that fail’: not a solution to housing problems, but a contributing factor (Pagani et al., 2025: 17 citing Senge, 1990).
Our research agrees with previous research that there is no clearly negative effect for social housing tenants of living in concentrated social housing. Reducing disparities requires addressing poverty, not deconcentrating social housing (Casarin et al., 2023; Cheshire et al., 2014). However, it diverges in that there may be some positive effect, at least regarding education and health outcomes. We have noted some ways that the New Zealand health and education systems may serve social housing tenants better when they live in areas with more social housing. However, these are only suggestions. There is more work to do on what is it about living in areas of more concentrated public housing that may lead to slightly better education and health outcomes for social housing tenants. Ongoing research on wellbeing, including neighbourhood experiences and access to amenities, in social housing in New Zealand may help provide insights (NZ Centre for Sustainable Cities, 2024).
Conclusion
In New Zealand, living in an area with a high proportion of social housing does not adversely affect education or health for social housing tenants. In fact, the more social housing there is in the area where public housing tenants live, the less likely they were to be hospitalised, and the more likely they were to participate in education. Our findings support the international evidence base that exposing social housing tenants to market residents does not improve their outcomes. They suggest that deconcentrating social housing areas through privatisation will harm social housing tenants. Improving people’s outcomes relies on providing sufficient social housing to meet need, increasing people’s wages, benefits and access to employment and investing in education, health and social support.
Footnotes
Appendix
Mean age, hospitalisations, income and time spent in social housing.
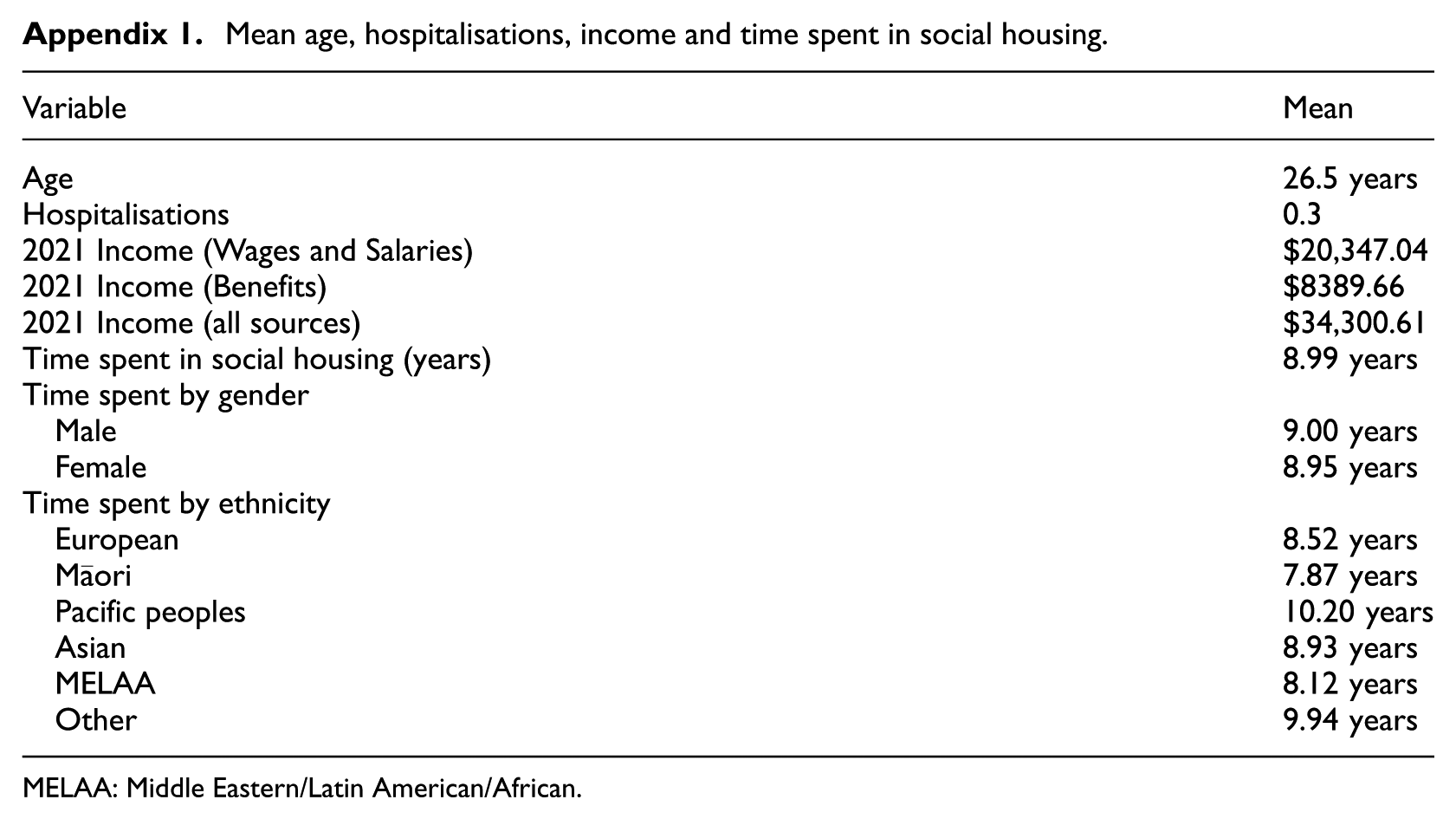
| Variable | Mean |
|---|---|
| Age | 26.5 years |
| Hospitalisations | 0.3 |
| 2021 Income (Wages and Salaries) | $20,347.04 |
| 2021 Income (Benefits) | $8389.66 |
| 2021 Income (all sources) | $34,300.61 |
| Time spent in social housing (years) | 8.99 years |
| Time spent by gender | |
| Male | 9.00 years |
| Female | 8.95 years |
| Time spent by ethnicity | |
| European | 8.52 years |
| Māori | 7.87 years |
| Pacific peoples | 10.20 years |
| Asian | 8.93 years |
| MELAA | 8.12 years |
| Other | 9.94 years |
MELAA: Middle Eastern/Latin American/African.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was carried out as part of the Public Housing and Urban Regeneration: Maximising Wellbeing research programme (2020–2025), which was funded by a New Zealand Ministry for Business, Innovation and Employment (MBIE) Endeavour programme grant (Grant ID: 20476 UOOX2003).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.