
Abstract
The increasing focus on the urban dimensions of care has brought attention to mobility as a crucial aspect. However, traditional origin–destination and time-use surveys often overlook the nuanced and diverse aspects of care-related mobility. They fail to account for the variety of care tasks, socioeconomic conditions, spatial contexts, and relational dynamics that shape different forms of care-related movement. Our article aims to contribute to filling these gaps by analyzing caregivers’ mobility, caregiving tasks, and sociodemographic characteristics. Using a survey in Chile that compares a pre-pandemic scenario with the first reaction to the pandemic, the article uses hierarchical clustering to find caregiving-related profiles and a joint multivariate model to identify observed and unobserved effects impacting the level of stress, ease of movement, and struggle to engage in paid work from home. Our analysis identifies four distinct caregiving mobility profiles, revealing significant disparities. Caregivers with heavier workloads and limited resources experienced the greatest challenges, including restricted mobility, higher stress, and difficulty managing remote work. Our model shows that gender is a critical factor influencing stress, mobility, and work-from-home struggles, even after accounting for socioeconomic and behavioral factors. Individuals less concerned about COVID-19 mobility restrictions reported lower stress levels. Lower stress levels were reported by those less concerned about COVID-19 restrictions, while stress was notably higher among caregivers for individuals with special needs and young children (0–6 years). Connectivity issues further intensified remote work challenges. These findings underscore the need for urban mobility planning and policies that recognize caregiving as a relational activity shaped by spatial and social dynamics, emphasizing the diverse impacts on caregivers.
Keywords
Introduction
Care activities can be defined as paid and unpaid work performed by people who accompany or perform activities in place of or for children, older people, and the sick, among others, helping the functioning of a household. These care activities, fundamental to urban life, demonstrate that mobility is rarely an exclusively individual activity and requires an inevitable interdependence with other subjects (Jirón and Carrasco, 2020).
To explore care-related inequalities among socioeconomic groups and household members, origin–destination and time-use surveys have provided very useful information. Nonetheless, these surveys usually fail to capture more profound and hidden aspects of mobility (Rojas Quezada et al., 2020), particularly when a more exhaustive study of care tasks is needed. First, caregiving is blurred among other activities such as walking, visiting, leisure, accompanying, or free time, making care-related trips invisible. Second, it is difficult to distinguish between women’s personal or leisure travel compared to care, which is measured under the same category in different contexts, such as Chile and Spain (Sánchez de Madariaga and Zucchini, 2020). Third, most of the analyses using time-use surveys do not focus on people receiving informal care, whether children, older people, or people with disabilities (Stampini et al., 2020), and do not distinguish the forms of mobility associated with different care needs. Thus, instruments that help characterize caregivers’ mobility patterns, care tasks, and sociodemographics are urgently needed.
At the same time, the growing interest in the urban dimensions of care is giving space to mobility as a significant phenomenon. The reciprocal interaction between space and care is the object of works that tackle several spatial dimensions of care, from initiatives taking care of neighborhood spaces and protected areas to policy initiatives and informal networks that take care of specific groups and spaces (see Wiesel et al., 2020, for a review and a special issue devoted to “cities of care”). As a significant cause and consequence of specific care arrangements, mobility has received less attention. On the one hand, gender and sociodemographic features of individuals configure different forms of interdependence between individuals, which also generates specific forms of mobility related to the accomplishment of care-related activities. On the other hand, spatial settings at different scales—from houses to neighborhoods and cities—provide different opportunities to satisfy needs related to caring for oneself and one’s loved ones, conditioning how people can care for someone else and generating significant interpersonal differences. Examining the interplay between mobility patterns, care tasks, and sociodemographic characteristics is fundamental to fully grasping how space conditions care and how care contributes to the reproduction of unequal social and spatial arrangements.
In this article, we aim to contribute to this literature by providing evidence on the organization of care activities, the forms of mobility they generate, and the impact of the COVID-19 pandemic, recognizing that the health emergency increased caregiving responsibilities and has exacerbated several forms of inequality related to them (Ryan and El Ayadi, 2020; Sultana, 2021). Expanding on the existing COVID-19 literature focused on mobility patterns and transport mode shifts, we focus on understanding how the limited personal mobility generated tension between paid work and caregiving activities within the household and affected individuals differently.
More specifically, our article analyzes caregivers’ mobility, caregiving tasks, and sociodemographic characteristics, comparing a pre-pandemic scenario with the first reaction to the pandemic scenario. Using a survey in Chile, a country where several activities started to be performed from home immediately after a health emergency related to COVID-19 was declared, we provide insights into the characteristics and behavior of different caregiver profiles and the main factors that explain stress levels, ease of moving, and struggle to engage in paid work from home.
The article is structured as follows. After this introduction, the previous literature is described in the second section. The third section gives the Chilean context to the different topics of the mobility of care. The survey instrument and corresponding statistical methods are presented in the fourth section. The fifth section presents the main findings of the analysis. Finally, the sixth section concludes and summarizes future work.
Literature review
Care as an object of study
Care refers to activities necessary for the management and maintenance of the life, health, and wellbeing of people in everyday life (d’Argemir, 2017) and occupies an important place in our forms of socialization (Chinchilla, 2020). It involves physical and emotional work executed in multiple dimensions, which include caring and being cared for by others and engaging in work-related areas of care or health. It is not only a transaction, as it can occur within reciprocal relationships in the present and the long term, such as the care cycle between parents and children during the different stages of life (Plyushteva and Schwanen, 2018).
In recent decades, care characteristics and the relationships involved in care activities have been studied in sociology, public policy, and feminist research (Milligan, 2003). The latter have observed that care can be seen as dichotomous social provision systems in multiple dimensions: public/private, paid/unpaid, formal/informal, among others, but also as mixed economies, where the state, families, friends, and neighbors participate as care providers (Daly and Lewis, 2000). As a social and political construction, it is a gendered concept that has fallen disproportionately on women, with significant implications for those who deliver and receive care (Milligan and Power, 2009), for example, unfavorable repercussions for their labor and social trajectories (d’Argemir, 2017) and limitations in access to and choice of jobs, which are usually temporary, flexible, and therefore more precarious (Rico and Segovia, 2017). Similarly, women are more exposed to health issues due to excessive responsibility, overload or isolation, and a lack of time or resources to attend to their health (UN Women, 2020). These issues may cause women to be more prone to suffer from body pain, depression, and sleep disorders, among other conditions (Petrini et al., 2019).
Geographies of care have explored practices and perspectives that reflect culturally specific norms of care provision and needs in both the Global North and South, including changes introduced by women’s increased entry into the paid labor force and the international migration of women care workers (Hanrahan, 2018). Feminist geographies debates have positioned the urgency of investigating the spatialities of care by situating the social and material spaces of care under new scrutiny, where care is an activity and a form of relationship (McEwan and Goodman, 2010). At the cultural level, there are also frequent discourses influenced by the assumption of “traditional” societies. Extended families are responsible for ensuring the care of older people, as opposed to “modernized” societies, which impact the production of public policies associated with care (Hanrahan, 2018) and divert attention to the material and physical conditions of care (Milligan, 2003).
The mobility of care: Gender and interdependence
Care also influences everyday mobility, intended as the individual capacity or aptitude to move around and solve basic daily needs (Miralles-Guasch and Cebollada, 2009). Individual mobilities between household members, close friendships, work, or neighborhood social networks are inherently linked (Jirón and Gómez, 2018). Thus, mobility should be understood as a relational and interdependent practice with different manifestations and implications regarding gender, which in turn intersect with other characteristics such as age, ethnicity, income, skills, and place of residence (Jirón, 2007; Jirón et al., 2020). In fact, mobility emerges as a gendered practice (Hanson, 2010; Uteng and Cresswell, 2008; Uteng et al., 2019), with significant differences that often lead to inequality and exclusion (Jirón and Gómez, 2018). Considering the existing research, certain dimensions central to the mobility of care emerge: the way in which care responsibilities are distributed among different subjects; the mobility practices related to care; and the mobility constraints that caregivers must face.
The distribution of care responsibilities is often related to gender roles and the expectations attached to them. Depending on gender, a person is expected to perform certain tasks and, as a result, one’s participation in relevant activities changes. Role expectations may lead to a different distribution of care responsibilities between partners, with a balance that depends on the relationship between them. For example, traditional role views within a couple determine a more specialized division of household tasks (Ettema and van der Lippe, 2009). Moreover, significant life course changes—such as the birth of a child—influence care-related mobility (Plyushteva and Schwanen, 2018; Scheiner, 2020; Scheiner and Holz-Rau, 2017). Socioeconomic resources condition how interdependence and care networks are structured; in some cases, these relationships are resolved within the family. For those who do not have this type of support, income conditions enable the possibility of delegating care to one of the family members or hiring domestic services (Jirón and Gómez, 2018). The interdependence approach to mobility makes it possible to account for the importance of care in daily life and the inequalities this generates in women’s lives (Jirón and Gómez, 2018).
Gendered expectations and the distribution of care responsibilities also influence the mobility practices of caregivers, generating what has been defined as the “mobility of care” (Sánchez de Madariaga, 2013; Sánchez de Madariaga and Zucchini, 2020). This involves various purposes, such as accompanying children or dependants to school, recreation, health care, and other extracurricular activities; shopping; errands in public offices; visiting and accompanying sick and elderly relatives; and home maintenance activities. The interest in the mobility of care has grown in recent years and higlights four relevant dimensions with which to understand this phenomenon. The first is the individual activity space: women often have smaller but more complex activity spaces, shaped by several space–time constraints (Kwan, 2000; Schwanen et al., 2008). The second is the modal choices: the need to perform care activities leads women to choose the mode that allows them to be a “good parent,” which in a suburban area means using a car and in a dense, central urban zone allows using active transport modes (Gómez-Varo et al., 2024; Sánchez de Madariaga and Zucchini, 2020; Schwanen, 2011). The third is time allocation: men often have longer travel time and participate in more personal activities, also at night (Fan, 2017; Wang and Yang, 2023); nonetheless, socio-economic status is another feature that, together with gender and age, determines the amount of time devoted to activities (Murillo-Munar et al., 2023). The fourth is mental health and wellbeing: gender differences, travel times and modal choices, together with parental status and the travel time of the partner, differently influence individual wellbeing, with negative effects especially for women (Tao et al., 2023; Wang and Yang, 2023). The roles associated with gender thus determine a set of expectations and activities that determine unequal individual, spatial, and social boundaries for the mobility of women (D’Agostino et al., 2024), greatly influencing not only their everyday practices but also their overall wellbeing.
Care mobilities and the related gendered differences generate barriers that tend to affect the subjects in charge of caregiving, determining specific space–time constraints (Jirón and Mansilla, 2013; Kwan, 2000) that lead to “thick” forms of mobility. For example, women are more likely to have smaller spatial ranges of daily movement than men, mainly staying in the domestic space. Likewise, women make more trips unrelated to paid work, more multiple-stop trips, and more trips accompanied by or accompanying others (Chaves et al., 2017). Women also show differences in the frequency of public transport use and cargo trips (baby trolleys, bags, shopping, etc.), travel times and associated insecurity (Comisin Econmica para Amrica Latina y el Caribe [CEPAL], 2019), and car ownership and driver’s license possession (Loukaitou-Sideris, 2016). All these unique travel patterns are closely interrelated with economic inequalities, where women are among the most vulnerable groups (CEPAL, 2019; Figueroa Martínez and Forray Claps, 2015).
The imbalanced distribution of care responsibilities and the consequent space–time constraints become particularly evident in the case of parenting. Caring for children in fact determines that men and women often spend similar daily amounts of time traveling but women devote a significant part of their time to travel with and for children (Craig and van Tienoven, 2019). Even if social and cultural norms differ across countries, some common expectations are attached to the mobility of parents and their children, such as the need to directly look after children instead of allowing them to travel alone, and to ensure that they arrive on time and that their travel is safe (Carver et al., 2013; Craig and van Tienoven, 2019; Forsberg et al., 2020). As a result, these expectations often discourage active travel (Forsberg et al., 2020; Sersli et al., 2020) and instead determine specific forms of car dependence (Kent, 2025; McLaren, 2018), which often—but not always—have a long-term influence on the mobility preferences of the children once they grow up (Bhosale et al., 2017; Kent, 2025). According to some authors, the efforts associated with planning and performing the mobility practices related to parenting configure this as a specific form of domestic work (Gilow, 2020).
The mobility of care is thus associated with deep gender-related imbalances, which intersect with the differences related to the age and socioeconomic conditions of the caregivers. The growing interest in the mobility of care has already generated intersectional studies in both the Global North and South (Gómez-Varo et al., 2024; Murillo-Munar et al., 2023; Plyushteva and Schwanen, 2018). Nonetheless, these studies tend to consider care arrangements and the related forms of mobility in a specific moment, grasping the differences associated with different moments of the life course. Less attention has been devoted to the impact that critical, exogenous events may have on the (im)balances that characterize care activities and related mobility. Some studies have considered the impact that different dramatic events (such as natural disasters) have on everyday mobility patterns (see e.g. Wang and Taylor, 2016), but without considering the mobility arrangements associated with care and the implications in terms of stress and mobility barriers for caregivers.
COVID-19 and its impact on systems and mobilities of care
Feminist economics has shown that feminized reproductive work has been fundamental in sustaining the capitalist global economy (Gago, 2019). For this reason, economic crises resulting from disease outbreaks significantly impact social reproduction and women’s lives. As Woskie and Wenham (2021) point out, in previous experiences such as Ebola or Zika fever, it was women who faced the most significant economic and social consequences—quitting their jobs to take care of their (sick) children, assuming the financial and care overload due to their partners’ abandonment, a longer delay in re-entering the salaried labor force, and a more sustained abandonment in schooling by girls. Likewise, due to the high participation of women in health care, in contexts of health crises they are more exposed to contracting diseases, dismissal, and social stigmatization for being seen as vectors of contagion (Leone and Caballero, 2021).
The recession resulting from the COVID-19 pandemic has had disproportionately negative effects on women, particularly mothers, who have mainly taken on additional care work due to school and daycare closures, experiencing penalties and stress in the labor market. The Risks That Matter (RTM) 2020 survey applied in 25 OECD countries indicates that 61.5% of mothers of children under 12 years of age reported having assumed most or all extra care work, almost three times more than the 22.4% reported by fathers. Likewise, mothers of children under 12 were more likely to move into unemployment between 2019 and 2020 (Frey and Alajääskö, 2021). Even in countries that have remained at the top of the gender gap indices, the evidence remains the same. In Iceland, mothers reported greater physical, mental, and emotional work to maintain peace of mind and security in facing economic uncertainty and health risks to their families (Hjálmsdóttir and Bjarnadóttir, 2021). Also, women mostly report concern for their children’s education during quarantines (Frey and Alajääskö, 2021).
Similarly, the COVID-19 pandemic and its effects on population mobility showed new scenarios and reorganizations in the geographies of care while revealing and increasing the multiple gaps to which caregivers and care subjects are exposed. Although overall mobility decreased during the most intense periods of COVID-19 due to government closures and voluntary social distancing, the data show heterogeneous effects across population segments, which show that women are being more affected than men in terms of mobility and care (Caselli et al., 2021; Czymara et al., 2021; Frey and Alajääskö, 2021; Hjálmsdóttir and Bjarnadóttir, 2021; Porter et al., 2021; Woskie and Wenham, 2021).
With the elimination or restriction of care-related outings abroad, the time spent on care and its types has been altered. In Austria, mobility decreased significantly for both men and women, although the latter restricted their movements more than the former. Also, they presented some changes in mobility patterns as self-care strategies. At the same time, women tended to avoid crowded spaces such as shopping malls, while men frequented more commercial, social, and recreational areas. Furthermore, following the lockdown, men “returned to normalcy” more quickly than women (Reisch et al., 2021). Van Tienoven et al. (2023) point out that in the case of Belgium, women cover most of the routine domestic and care work, while men are mainly engaged in non-routine work, involving more sporadic time–distant travel and recreational outings. A lack of mobility also raises concerns with increased time at home and reduced social networks, exacerbating safety issues and violence toward women. Between March and June 2020, 1409 femicides, more than 240,000 reports of violence, and more than 1,250,000 calls to hotlines to report acts of male violence against women were recorded in the Latin American region (Leone and Caballero, 2021).
The Chilean context
Before the pandemic, women in Latin America already spent three times more time than men on caregiving in their homes (CEPAL, 2020). The last national time-use survey in Chile showed that women spend 5.8 hours a day on care work, more than twice as much as men, while spending 2.6 hours less on leisure, social life, paid work, and studies (ENUT, 2015). In the case of long-term caregivers, time-use surveys in countries such as Chile, Colombia, Costa Rica, and Mexico show that women constitute 63–84% of long-term family caregivers and account for 72–88% of the total hours spent in this area. In all these countries, women who provide this type of care are less likely to engage in paid work; those who do so work fewer hours per week and have a double workload (Stampini et al., 2020).
While most studies on care in Chile have focused on burden sharing, little work has been done on the links between care relationships and mobility (Henríquez et al., 2025). Before the pandemic, activities associated with care led to different travel patterns for women: in Santiago, women make just over half of the daily paid work trips (13% compared to 25% for men), while they make twice or three times as many trips related to shopping, health, and accompaniment of various kinds (Sagaris and Tiznado-Aitken, 2020). Due to the complexity of caregiving tasks, multiple strategies have been developed in Chile that involve economic resources, time, and movement, directly impacting people’s daily lives (Jirón and Gómez, 2018), where gender acts as one of the main gaps. For Jirón (2017), some of these strategies correspond to (i) maintaining communication channels between household members and/or support networks to make decisions in real time, (ii) constantly seeking and managing support (paid or voluntary) that allows them to maintain their mobility, (iii) making multipurpose trips, (iv) adapting working hours to accommodate care work, and (v) recognizing better routes and travel paths to optimize times and experiences in transfers.
The COVID-19 pandemic has emphasized these imbalances. Confinement measures constantly varied in Chile, from voluntary recommendations to stay at home to mandatory quarantines with two weekly permits for specific activities (work permits, shopping, medical hours, funerals, and pet walking). However, educational establishments remained closed for two years, a care task assumed by families but more by mothers. The Cuidar study in May 2020 revealed that the educational system was responsible for 65.4% of the care before the pandemic, followed by 16.6% for mothers and 1.9% for fathers. Subsequently, care provided during the morning and afternoon increased dramatically for women, rising to 73.6% and 69.4% versus 12.4% and 17.7% for fathers for both schedules, respectively (Silva Sá and Pérez Cortés, 2021). According to another study published in August 2020, 57% of men did not spend hours on childcare, and 38% did not spend hours on housework (Hiner, 2020). Similarly, recent studies show that while men spend 3.8 hours on unpaid housework in Chile, women spend 5.6 hours on such work (CEAS, 2020).
During the pandemic, children stayed at home for various reasons, mobilizing others to take charge of their care despite a more reduced mobility space (Cortés-Morales et al., 2021). The overload of domestic tasks and childcare activities negatively impacts women from segregated neighborhoods in Santiago, Chile. In a context of segregation and urban deterioration, determined by women’s life cycle, immobility was present before the pandemic. This behavior was exacerbated after the closure of schools, limiting women’s mobility even more and forcing them to adopt new strategies to cope with care activities in a confined space (Carrasco et al., 2021; Luneke et al., 2021).
Research has focused not only on individual or family practices but also on communitarian expressions. Anigstein et al. (2021) point out that one of the aspects that the COVID-19 crisis has revealed in Chile is the importance of collective actions to cope with the pandemic’s physical, social, and economic effects in the absence of governmental solutions. These situated actions in the Latin American context highlight the dynamic interplay between mobility, interdependence, time, and work. Building on existing COVID-19 literature that examines mobility patterns and shifts in transport modes, this article aims to address some of these elements by exploring how restricted personal mobility and the tension between work and caregiving responsibilities within households differently impact individuals.
Data and methods
Survey data
The study used a survey for Chilean individuals to capture (i) how paid and care work is shared among household members and their networks, (ii) differences between pre- and post-COVID-19 mobility and care activities, and (iii) the overall experience and most stressful elements of quarantine care tasks (see the full questionnaire in the Supplemental Material). Given the pandemic restrictions, we applied the survey to 871 individuals using stratified social media recruitment via Facebook (Zhang et al., 2020), with initial stratification designed to focus only on the Chilean context. However, we acknowledge that this sampling method introduces potential biases, such as platform-specific and self-selection biases, and limits the generalizability of our findings. As the sample is non-random, we interpret our results cautiously and primarily use descriptive and exploratory analyses to highlight trends rather than making definitive inferential claims.
The recruitment took two weeks between late March and mid-April 2020, allowing the research to capture before and after the health emergency was declared in Chile in March 2020. At that time, the main limitation was the closure of schools, and labor was still mixed, with some companies working from home and others still requiring in-person work. It is important to note that this survey captured the first reaction to the emergency and does not reflect the full pandemic-related panorama.
Methods
After conducting a descriptive analysis of our sample, we employed hierarchical clustering to identify caregiving-related profiles. This unsupervised learning method was used to uncover similarities and patterns among the variables without any predefined labels. Hierarchical clustering allows for the detection of subgroups within the caregiving population, providing a more nuanced understanding of the diversity in caregiving experiences. Given that caregiving is a complex and multifaceted role that varies significantly across individuals, analyzing caregiver profiles helps to explore how mobility patterns, care tasks, and sociodemographic characteristics intersect. This approach highlights that caregivers do not experience or engage with their roles in the same way and can reveal groups that may be more vulnerable to the negative impacts of the pandemic, such as those facing mobility challenges, limited access to resources, or increased care burdens.
The segmentation was based on three variables related to caregiving: (i) the distribution of the caregiving burden, (ii) with whom the caregiving tasks are shared, and (iii) the person who receives care. The database included the 16 dichotomous variables presented in Table 1. Each one takes the value 1 when representing that category and 0 otherwise.
Variables used for our segmentation.
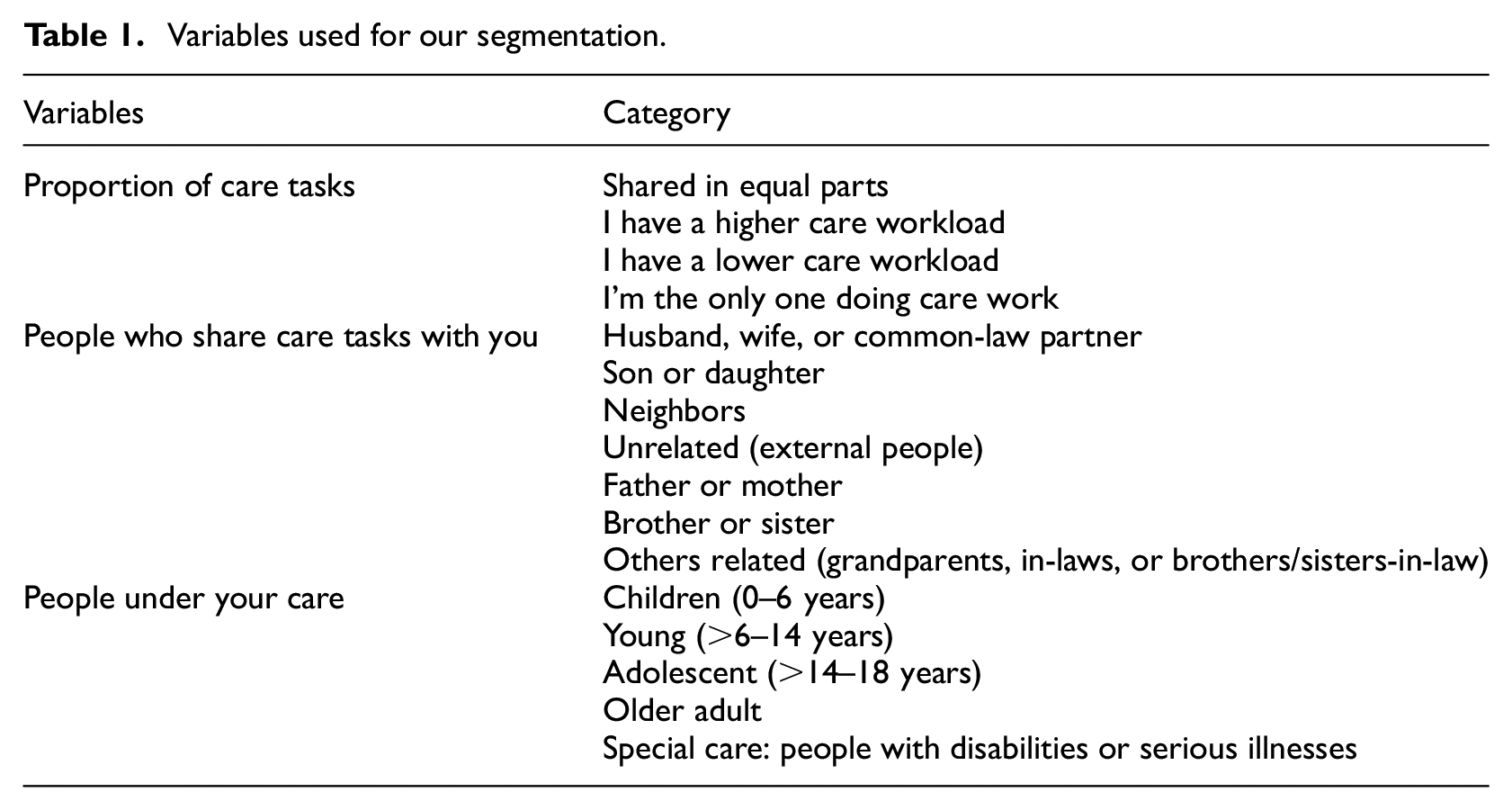
The data-clustering process involved using Gower distance, recommended for categorical and binary variables (Dos Santos and Zárate, 2015), and average linkage as the measure and method of association, respectively. As alternatives, we tested single linkage, complete linkage, the centroid method, and Ward’s method for the linkage criteria, selecting the one that provided the most distinguishable clusters.
Finally, we use a joint multivariate ordered probit model to explore which characteristics and care-related tasks are related to higher stress levels, lower ease of movement, and higher struggle with paid work-related activities from home, both before and during the first weeks of the pandemic. This multivariate framework considered five ordinal five-level Likert-scale endogenous variables jointly estimated: mobility ease before March 16, mobility ease after March 16, stress level before March 16, stress level after March 16, and difficulty performing paid work tasks from home. We estimated the effects of different exogenous variables used in the joint model, and common unobserved factors are considered by allowing correlation between the error terms of the relations describing each endogenous variable (Ferdous et al., 2010). Details of the modeling framework, including estimation method and identification conditions, can be found in Ferdous et al. (2010).
In summary, our study offers a methodological approach complementing hierarchical clustering and a joint multivariate ordered probit model to examine caregivers’ mobility patterns, care tasks, and stress levels during different phases of the pandemic. Most studies applying cluster or latent class analyses associated with caregiving tend to focus on health-related issues (e.g. Ali et al., 2022; Janssen et al., 2017; Tischendorf et al., 2024), while similar modeling frameworks to the one proposed here have been used mostly in travel behavior research (e.g. Gkartzonikas and Dimitriou, 2023; Ma et al., 2018; Nair et al., 2018). Whereas previous research typically isolates aspects of caregiving—such as burden, mobility, or stress—or relies on qualitative methods, this study provides a more comprehensive analysis by examining these dimensions together and exploring their intersections through a robust quantitative approach.
Results and discussion
Descriptive analysis: A high-level summary
The sample consists of 871 participants (see full description in Table 2, column “Total”), primarily female (76.6%) and middle-aged, with 64.2% aged 31–50 years and an average age of 40.1. All respondents live in urban areas, mostly in Santiago (61.9%), followed by Bío-Bío (22.0%), Valparaíso (7.2%), and other regions (8.9%).
Caregiver profile characteristics.
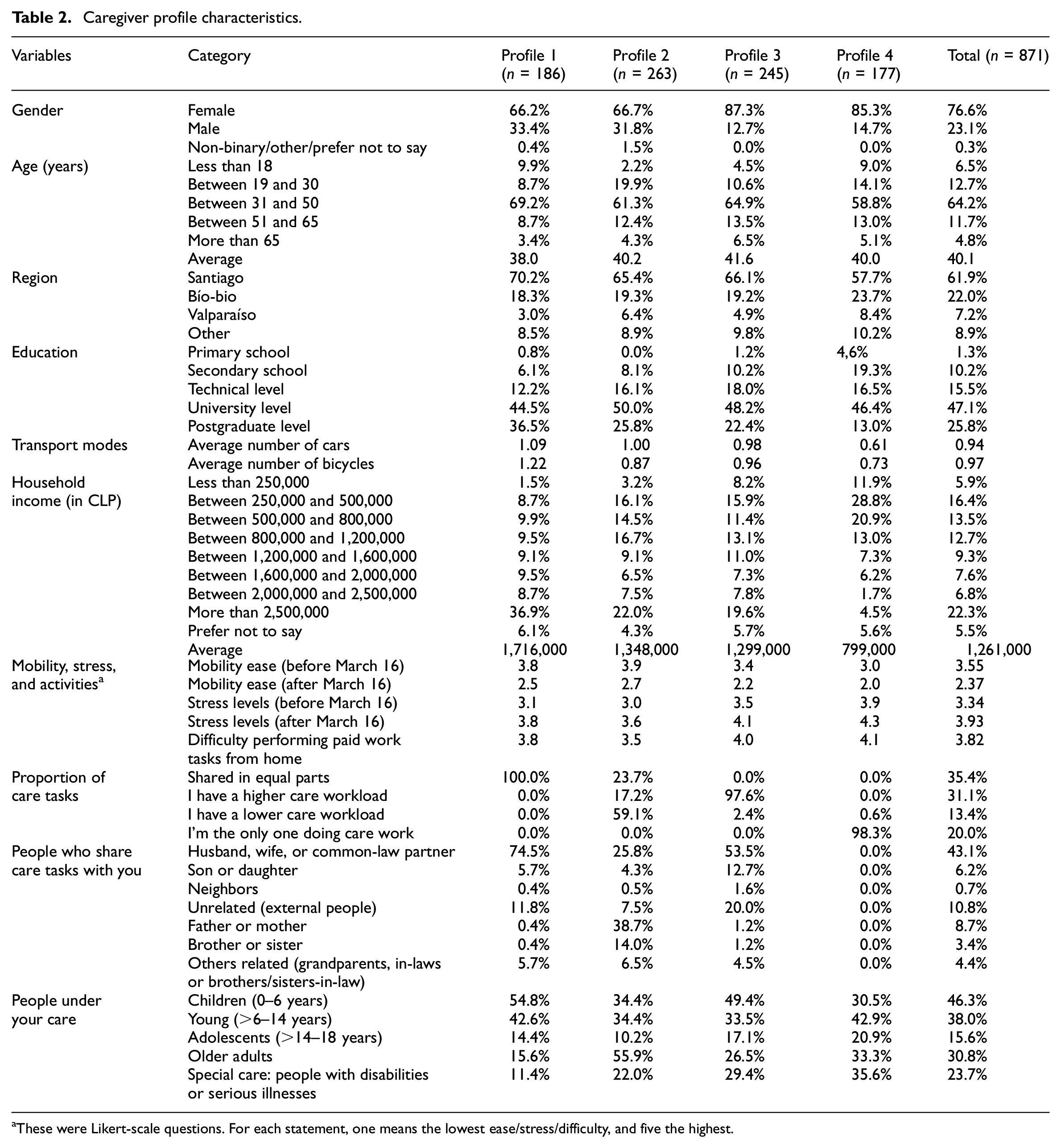
These were Likert-scale questions. For each statement, one means the lowest ease/stress/difficulty, and five the highest.
In terms of education, the sample is highly educated, with 47.1% holding university degrees and 25.8% having completed postgraduate studies. A smaller proportion reported technical-level education (15.5%), secondary school (10.2%), or primary school education (1.3%). Average household income is CLP 1,261,000, but disparities exist, with 22.3% earning over CLP 2,500,000 and 22.3% earning CLP 500,000 or less. Households report moderate car and bicycle ownership (on average, 0.94 cars and 0.97 bicycles per household).
The data highlight significant differences in care responsibilities. While 35.4% share caregiving tasks equally, 20.0% report being the sole caregiver, and 31.1% have a higher caregiving workload compared to others in their household. Most care tasks are shared with a spouse or partner (43.1%), though a notable proportion depend on external help (10.8%) or family members such as parents (8.7%) and siblings (3.4%). Care recipients include children aged 0–6 years (46.3%), older adults (30.8%), and individuals requiring special care (23.7%). Among those who live with older adults or caregivers, different care strategies for dealing with the pandemic can be observed: carrying out check-ups and vaccinations as soon as possible (34.5%), suspending them (29.7%), or stocking up on necessary medications (42.4%). The interdependence of this type of relationship is evident, given that two out of three respondents stated that they do not expose themselves to risks for fear of infecting the people who depend on their care.
Mobility, stress, and work challenges vary. Before March 16, mobility ease averaged 3.55, dropping to 2.37 afterward. Stress levels increased significantly during the same period, from an average of 3.34 to 3.93. Difficulty in performing paid work tasks from home also rose, with an average rating of 3.82, reflecting the broader challenges faced by participants during the pandemic. This aspect translates to 69% feeling tired or very tired performing caregiving. These findings underscore the interconnected nature of caregiving, stress, and mobility challenges, which are further explored in the following subsections.
Care profiles
The cluster dendrogram using Ward’s method (Ferreira and Hitchcock, 2009) resulted in four care profiles with a relatively even representation in the sample, ranging from 20% to 30%. The analysis focused on the differences between sociodemographic characteristics and care-related variables among groups (Table 2).
Profile 1 represents 21.4% of participants and is defined by equal sharing of caregiving tasks (100%). Most members rely on their spouse or partner (74.5%), external help (11.8%), or children (5.7%) to share these responsibilities. This group is notable for its focus on young children, with more than half caring for children aged 0–6 (54.8%) and 6–14 (42.6%). Members of Profile 1 are the youngest on average (38 years old), include the highest proportion of men (33.4%), and live predominantly in the capital region of Santiago. They also have the highest education levels, with the largest percentage of postgraduate degree holders, and enjoy the highest household incomes (around CLP 1,716,000) and the greatest access to cars and bicycles.
Profile 2 (30.2%) stands out for its diverse caregiving dynamics, with a mix of equal caregiving (23.7%), lower caregiving workloads (59.1%), and higher caregiving workloads (17.2%). This group relies heavily on support from parents (38.7%) to manage caregiving responsibilities. Profile 3, comprising 28.1% of participants, includes caregivers with a significantly higher burden (97.6%). When caregiving tasks are shared, it is mostly with partners and involves the care of young children or older adults. This profile has the highest average age (42.2 years), the largest proportion of women, and a notable focus on caregiving for older adults and individuals needing special care.
Profile 4 (20.3%) is almost entirely composed of sole caregivers (98.3%) and has the second-highest percentage of women (85.3%). This group is unique for its focus on individuals requiring special care (35.6%) and its geographic distribution, with many members living in the Bío-Bío and Valparaíso regions. Profile 4 also faces the most challenging circumstances: the lowest household income (around CLP 799,000), the fewest cars and bicycles, and the hardest conditions during the pandemic, including low mobility ease, high-stress levels, and significant difficulties working from home.
The pandemic universally reduced mobility ease and increased stress and fatigue due to travel bans and quarantines. Caregiving responsibilities varied significantly, from equal sharing in Profile 1 to exclusive caregiving in Profile 4, with Profiles 2 and 3 in between. Caregivers in Profiles 3 and 4 faced the most challenges during the pandemic, including limited mobility, elevated stress, and difficulties managing remote work, likely due to heavier caregiving workloads and fewer resources. In contrast, Profiles 1 and 2, with shared responsibilities, higher incomes, and better transportation access, encountered fewer pandemic-related difficulties, likely due to their stronger support networks and resource availability.
The findings reveal a connection between caregiving intensity, resource availability, sociodemographic factors, and the challenges posed by the pandemic. Economically and socially vulnerable caregivers faced amplified negative impacts, underscoring the need for targeted support and policy interventions. This relationship warrants further exploration, as discussed in the following section.
Joint multivariate model
The log-composite likelihood value for the joint model is −228,769.62. Using the composite likelihood ratio test (CLRT) statistic proposed by Ferdous et al. (2010), we test our joint model against the independent version, that is, without any correlation between endogenous variables. The estimated p-value for the test is 0.0235, rejecting the null hypothesis and highlighting the need for joint estimation of the five endogenous variables.
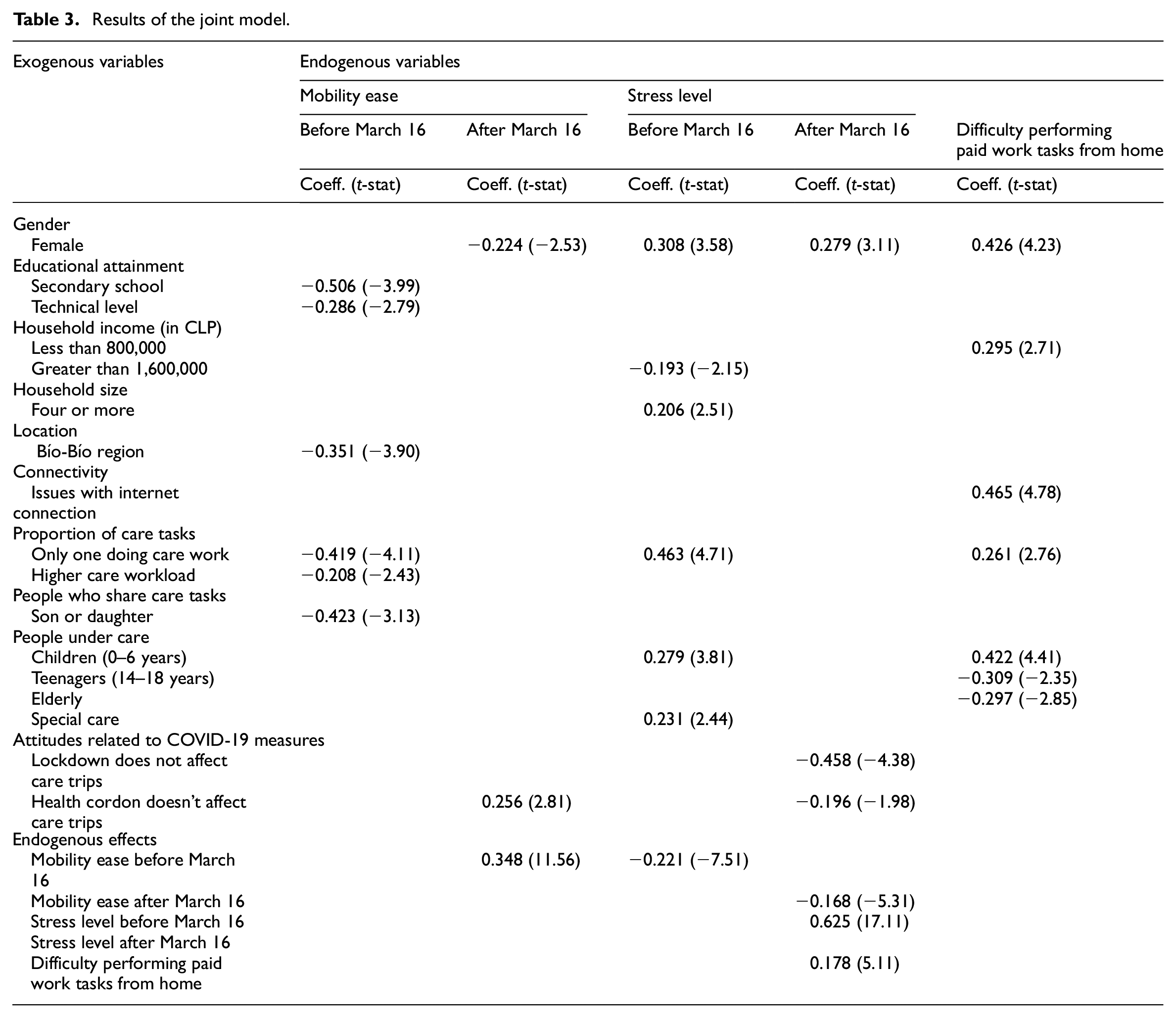
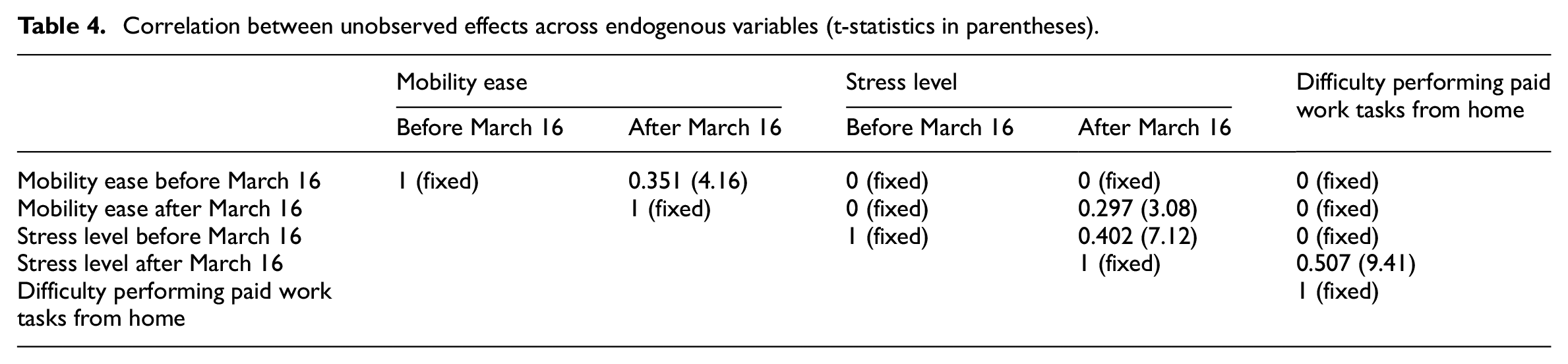
Table 3 describes the estimated effects of different exogenous variables used in the joint model and the five endogenous variables jointly estimated: mobility ease before March 16, mobility ease after March 16, stress level before March 16, stress level after March 16, and difficulty performing paid work tasks from home. Since the endogenous variables are ordinal (on a five-level Likert scale), four threshold parameters should be estimated for each variable. These threshold parameters do not have behavioral interpretations and are not presented in Table 3 (but are available on request from the authors). Common unobserved factors are considered by allowing correlation between the error terms of the relations describing each endogenous variable (Ferdous et al., 2010). The correlation estimates are shown in Table 4.
Results of the joint model.
Correlation between unobserved effects across endogenous variables (t-statistics in parentheses).
Gender plays a vital role for all the endogenous variables (except mobility ease before March 16), even when controlling for other sociodemographics and pre-pandemic behavior. Being a sole caregiver implies that all tasks, both care and domestic work, are carried out by a single person, which means that the person in charge has very little time for personal care, automatically increasing stress. Being a woman generates more significant pressure since the social perception of this gender shows that they have fewer job opportunities and must stay at home taking care of everyone else. Individuals from lower-income households have more difficulty performing paid work tasks from home, which is expected since low-skilled jobs were related to unemployment during the first months of COVID-19 in Chile (Rivera and Castro, 2021).
Stress was notably higher among caregivers of individuals with special needs and young children (0–6 years), while lower stress levels after March 16 were reported by those less concerned about COVID-19 restrictions. These groups believed that the lockdown and health cordons did not significantly impact their care-related trips. Health cordons were implemented to isolate specific areas and prevent the spread of COVID-19. This measure prohibited individuals from entering or leaving a commune, except in limited cases, such as attending a funeral or receiving medical treatment in another city. This finding aligns with Kaplan et al. (2022), who observed that skepticism toward pandemic restrictions was associated with reduced fear of infection when using public transport. While respondents did not underestimate the potential consequences of the pandemic, they believed they could mitigate infection risks through personal actions, such as maintaining a healthy lifestyle. Similarly, caregivers less concerned about mobility restrictions may have felt more confident in managing their risk of exposure, which likely contributed to their lower stress levels during this period.
Our joint multivariate model demonstrated the impact of connectivity issues on the difficulty of performing paid remote work. This finding aligns with Valenzuela-Levi (2021), who highlighted how digital exclusion, particularly in peripheral and low-income areas, affects access to essential online services, including purchasing products and maintaining connectivity. Similarly, research in Washington state has shown that faster internet connections are associated with increased telecommuting opportunities (McArthur and Hong, 2023). These patterns emphasize how the digital divide can restrict choices and opportunities for certain regions or population groups, potentially exacerbating inequalities in the future.
Our findings indicate that the age group of individuals under care has a differential impact on the difficulty of performing paid work tasks from home. Caring for children aged 0–6 years significantly increases this difficulty, while caring for teenagers (14–18 years) or elderly individuals is associated with lower difficulty levels. A possible interpretation of this result is that young children require constant attention, supervision, and hands-on care, which can disrupt focus and reduce the time available for work-related activities. In contrast, teenagers are generally more independent and require less-intensive caregiving, allowing caregivers to allocate more time and attention to work tasks. Similarly, elderly individuals, depending on their level of autonomy, may require caregiving that is less immediate or labor intensive, potentially causing less disruption to paid work responsibilities. However, other research has shown that nearly a quarter of employed older adult caregivers experience reduced work productivity due to caregiving responsibilities, with an average productivity loss of approximately one-third (Keita Fakeye et al., 2023).
The mobility ease before March 16 is introduced in the mobility ease after March 16 specification as a way to control for pre-pandemic behavior. The effect is significant and positive, as expected. Similarly, the stress level before March 16 impacts the stress level after March 16. The ease of mobility after March 16 negatively impacts the stress level in that period, which can indicate that people with more effortless mobility have less stress during the pandemic. This highlights the role of transportation and accessibility in the mental health of individuals (Liu et al., 2022). Finally, the difficulty of performing paid work tasks from home also impacts the stress level during the pandemic, which is one possible disadvantage of the accelerated adaptation of working from home (Birimoglu Okuyan and Begen, 2022).
As presented in Table 4, the correlation between the unobserved effects impacting mobility ease before March 16 and after March 16 is significant. This implies that common unobserved factors, such as accessibility measures or lifestyle variables, impact mobility ease in both periods. Similarly, the correlation between the unobserved effects impacting stress levels before and after March 16 is also significant. Finally, the correlations between the unobserved effects in mobility ease after March 16 and stress level after March 16 and between stress level after March 16 and difficulty performing paid work tasks from home are also significant, implying that other pandemic-related factors are latent in our analysis (such as financial crisis or health status).
Conclusions
Although the mobility and paid work inequalities have been analyzed for different socioeconomic groups during the pandemic in Chile (Astroza et al., 2020), the care perspective has been less explored, despite its relevant implications for public action, the organization of the city, and its mobility. The results presented here confirm once more that care activities are primarily the responsibility of women and also show that this burden configures different types of mobility of care, thus requiring consideration of the various factors that contribute to such differences and imbalances.
The survey results allow a first approximation of the inequalities associated with care and its spatial dimension. Of the four profiles identified, two of them are opposites. The first one belongs to the household profile where high-income and well-educated partners share their responsibilities equally, and therefore less stress and struggles are experienced in daily life. The second one may reflect a group with little saving capabilities and less access to resources. These characteristics suggest a high emotional workload, considering the group’s care role, low income, and low resources. This group indicates having more emotional wear and tear since it must do all the care tasks by itself and also does not have the necessary tools to emerge as the other groups. Also, the subjects that are cared for differently impact the caregiver’s wellbeing, considering that children from 0 to 6 years old and people with special needs are associated with higher reported stress levels. These findings align with similar research conducted in other regions. For instance, in the Netherlands, it is more common for highly educated parents who work full time to share child-escorting responsibilities equally, while in most cases traditional gender roles persist, with women primarily responsible for caregiving (Han et al., 2019). Likewise, in the UK, flexible paid work arrangements affect women differently. When combined with the presence of children, these arrangements tend to place heavier caregiving and escorting burdens on women (Viana Cerqueira and Motte-Baumvol, 2022).
The results also have important implications from an urban equity perspective. The survey was developed in a country where almost nine out of 10 inhabitants live in urban areas, but the mobility of care profiles are associated with different settings: the affluent profile 1 lives mainly in the capital city of Santiago; profiles 2 and 3 show a higher presence of people from Central Chile, where intermediate cities prevail; finally, profile 4 has a significant share of respondents from the regions headed by Concepción and Valparaíso, the two main metropolitan areas of the country outside Santiago. While the analysis did not directly consider housing or urban features, it can be expected that the four profiles deal with care in different spatial settings. In an unequal country such as Chile, and especially in unequal cities like Santiago, the amount and the quality of locally available opportunities are different. As a result, the possibility to access services locally and avoid long trips was and is unequally distributed among different neighborhoods of the same city (Link et al., 2021).
The same applies to access to the internet due to forms of digital exclusion that hit especially peripheral, low-income areas (Valenzuela-Levi, 2021), as well as the possibility of buying essential products online. Our joint multivariate model demonstrated the impact of connectivity issues on the difficulty of remote paid work. These findings are consistent with those reported in Washington state, where faster internet connections and increased telecommuting were associated. This digital divide might prevent or limit the choices for some places or population groups in the future (McArthur and Hong, 2023). Additionally, housing issues such as overcrowding and doubling up, which in Chile are chronically present, became even more pressing during the pandemic. While these inequalities related to housing and the urban environment are widely recognized in the Chilean academic and policy debate, it is relevant to consider how they interact with different care profiles, conditioning the forms of mobility we examined and being additional stress factors.
Estimating the joint multivariate model allows the analysis to identify observed and unobserved effects impacting the level of stress, ease of movement, and struggle with caregivers’ remote paid work. Results show that gender significantly affected stress levels, ease of movement, and work-related activities at home during the pandemic (women are more stressed and have more spatial difficulties and paid work-related issues at home), even after controlling for other socioeconomic characteristics, pre-pandemic behavior, and unobserved factors. These findings align with research from France, which indicated that women made fewer daily trips and covered shorter distances during the lockdown imposed due to the pandemic. A noticeable increase in women’s trip frequency was found once schools and childcare services reopened as part of a recovery process (Bulteau et al., 2023).
Overall, the methods applied in this article complement each other by noting important differences among the population between caring-sharing responsibility profiles and their relationship with sociodemographic characteristics, capturing the COVID-19 context in terms of concerns and mobility patterns, and how age had an impact. While our analysis focused on the first moment of the pandemic and did not capture its long-term effects on different forms of the mobility of care, it suggests the existence of significant differences that urban and social policy measures should consider highlighting and supports the importance of care activities for urban life and their role in urban equity.
Finally, we acknowledge that the sampling method used in this work introduces potential biases. Specifically, platform-specific biases (e.g. limited access to Facebook) and self-selection biases (e.g. respondents who are more likely to participate due to interest or availability) may influence the representativeness of the sample. In particular, our sample underrepresents lower-income individuals, as 22.3% of respondents reported earning up to CLP 500,000, compared to 55% of the national population according to CASEN (2022). Additionally, older adults are also underrepresented, with only 4.8% of our sample aged 65 and over, whereas the 2017 census indicates that this group comprises 11.8% of the population. Similarly, the reliance on Facebook as a recruitment platform raises additional considerations. While Facebook is widely used in Chile, it may not adequately capture the experiences of certain groups, particularly caregivers who face “time poverty” or individuals affected by the “digital divide.” These groups, which are often already at a disadvantage in terms of mobility and transportation access, may be underrepresented in the data. Consequently, the study may not fully address the transportation disadvantages faced by these populations, and this is an important limitation of our approach.
Given these factors, we interpret our findings with caution. As the sample is non-random and not fully representative of the population, the results primarily serve to highlight trends and generate insights rather than provide definitive conclusions. We acknowledge the need for further research incorporating more inclusive and representative sampling approaches, such as combining online recruitment with alternative methods to reach disadvantaged individuals. These additional strategies could help capture the perspectives of caregivers and other underserved groups more effectively. Likewise, developing a more comprehensive questionnaire could provide deeper insights by incorporating questions about breadwinner status, exploring its gendered differences and examining its influence on stress levels. This would allow for a broader understanding of stress factors, not solely tied to caregiving responsibilities but also linked to external aspects such as employment security.
Supplemental Material
sj-docx-1-usj-10.1177_00420980251361626 – Supplemental material for Profiling caregivers: Caregiving workload, mobility, stress, and remote work difficulties
Supplemental material, sj-docx-1-usj-10.1177_00420980251361626 for Profiling caregivers: Caregiving workload, mobility, stress, and remote work difficulties by Ignacio Tiznado-Aitken, Giovanni Vecchio, Sebastian Astroza, Juan Antonio Carrasco and María Consuelo Smith Piel in Urban Studies
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge the research support provided by CEDEUS, ANID FONDAP 1522A0002. The third and fourth authors also acknowledge the support from FONDECYT 1201362.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.