
Abstract
Contemporary approaches to counter homelessness push for a housing-led model that is seen as more progressive and less punitive than traditional approaches. Few studies have however investigated its translation on the ground. In this paper we aim to do so by studying the implementation of a housing-led approach in the Netherlands; in a context of housing shortages and health care austerity. By building on qualitative interviews with people (previously) experiencing homelessness and professional stakeholders, we argue that while a regular home is a much-needed improvement to emergency shelters and institutions, housing contracts are often conditional and used as disciplinary instruments restricting what people are allowed to do in their own home. Care and screening services are increasingly executed by housing associations and the local police, further entwining housing, care and punishment. Intersecting with local housing shortages and insufficient health care this becomes a barrier to a more effective and humane approach to homelessness. These findings contribute to theories on urban governance by showing how the management of the poor is extended to the private domain.
Introduction
The housing first approach to counter homelessness prioritises providing permanent independent 1 housing over medical treatment and short-term shelter. Some have described it as a paradigm shift away from traditional responses to homelessness based on the staircase model of conditionality (Busch-Geertsema, 2014; Tsemberis and Eisenberg, 2000). The staircase is supposed to transition homeless people from the streets to permanent housing in steps that include shelters, hostels and transitional housing; better housing conditions are the reward for improved behaviour, while eviction and relocation remain as threats or sanctions for breaking the rules (Sahlin, 2005). Increasingly, the staircase model to housing readiness is criticised for being ineffective, leading to hospitalisation, uncertainty and falling back into homelessness. In contrast, the housing first approach of providing immediate regular housing is now seen as a more humane and effective way to end homelessness (Benjaminsen, 2013; Sylvestre et al., 2017). All over the Global North housing first projects are now being disseminated and praised for their progressive, unconditional and non-punitive character.
Research has, however, revealed significant variation in how housing first approaches are implemented. These do not always adhere to an unconditional right to housing (Clarke et al., 2020; Hennigan, 2017; Wirehag, 2021). As strategies are executed by local actors within existing governance arrangements, we need to carefully examine how the philosophy is ‘translated in a particular context’ (Clarke et al., 2020) especially outside the dominant focus of US urban space (DeVerteuil et al., 2009). In this paper we aim to do so by studying the governance of homelessness in the Netherlands, where housing first approaches have recently gained prominence in public discourse. As most initiatives do not follow all the principles of the housing first approach as developed by Tsemberis and Eisenberg (2000), we speak of ‘housing-led’ responses. This refers to all approaches that provide independent permanent housing as a main response to homelessness.
The framing of homelessness as a housing problem is relatively new in the Netherlands, compared to countries such as England, Scotland (Anderson and Serpa, 2013) and Finland (Tainio and Fredriksson (2009). While the Netherlands has historically approached homelessness as a problem of health care policy (Boesveldt, 2015a), the housing first discourse necessitates coordination between the policy domains of housing and care. It requires the increased availability of social housing and the involvement of housing associations in community care and the prevention of homelessness, especially as homeless and mental health facilities are deinstitutionalised and decentralised at the same time. The housing-led approach is furthermore implemented in context of a severe affordable housing shortage. As such the Netherlands is an interesting case to research how a housing-led approach is operationalised within such a context.
This article builds on longitudinal qualitative data to study how relations between these new actors are forged and how this influences the experience of homelessness and independent housing. Semi-structured interviews with professional stakeholders as well as homeless and rehoused people highlight the ambiguities in the contemporary governance of homelessness.
Inspired by the poverty management literature, we reveal the uneasy co-existence of supportive and caring initiatives that favour independent housing over shelters and institutions with conditional housing contracts that risk continuing and extending the management of the poor to the (newly created) private domain. Strict requirements for independent housing, threats of eviction, and housing solutions in isolated areas further conflict with the right to housing. Our findings thus show that although the Netherlands has adopted a housing-led approach to homelessness, elements of the staircase model persist. Having private permanent accommodation does not protect from conditions, care, control and punishment. This endangers personal freedom and the home as a base for freedom, belonging and security, turning it into an instrument of urban governance.
Urban governance approaches to homelessness
Punitive and management approaches
Scholars have conceptualised urban governance approaches to homelessness in various ways. Punitive/revanchist governance refers to strategies to exclude marginalised populations from inner cities in order for these areas to remain attractive for investment (Smith, 1996; Wacquant, 1999). These approaches limit movement and coerce behaviour in public space by prohibiting sleeping in parks, camping, begging or sitting on the sidewalk. The most important actors are the local police and prosecutors, and the most important instruments, laws and incarceration (Herring et al., 2019). The revanchist approach to homelessness is reflected in the materiality of the city, with planters, spikes and specially designed benches to deter sleeping in urban space (Davis, 2006; Petty, 2016). New York City in the early 1990s – characterised by zero-tolerance, criminalisation, containment and the ‘cleansing’ of the homeless from its streets – is perhaps the best known example of the punitive/revanchist approach to homelessness (Mitchell, 1997; Smith, 1996; Zukin, 1995).
The revanchist/punitive framework has spurred scholarly debate on its relevance for governing homelessness outside the USA. Researchers have found traces of revanchist politics in urban homelessness policies worldwide, for example in Quito and Guayaquil (Swanson, 2007), Seoul (Song, 2011), and various cities in Europe (Doherty et al., 2008; MacLeod, 2002; Uitermark and Duyvendak, 2008). DeVerteuil (2006) and DeVerteuil et al. (2009) nevertheless warn against overextending the framework and argue that not all contemporary responses to homelessness can be categorised as punitive/revanchist. Instead, they propose an alternative framework based on ‘poverty management’. Poverty management entails specific strategies from the state or elites to –spatially – control urban marginalised populations in for example asylums, orphanages or jails (Wolch and DeVerteuil, 2001). This approach to homelessness includes more ambivalent social welfare responses that focus on regulating the homeless population and decreasing their visibility in urban public space (DeVerteuil, 2006).
For DeVerteuil and colleagues, the contemporary governance of homelessness is more complex and heterogeneous than punitive frames suggest. First, punitive responses co-exist with more ambivalent and even supportive approaches, which are not always easy to distinguish, as care often comes together with control (Clarke and Parsell, 2020; DeVerteuil et al., 2009; Dozier, 2019; Hennigan and Speer, 2019). Johnsen et al. (2018) have similar criticisms of revanchist readings and argue that we need to better understand the varied forms and outcomes of specific interventions; simply stating that interventions are punitive fails to acknowledge the diversity of social control measures that can range from force to tolerance. For example, ‘cops think[ing] like social workers’ by threatening with arrest to persuade people into treatment and/or shelters (Hennigan and Speer, 2019), patronising social service programmes (Williams, 1996) and surveillance practices that support street outreach programmes (Clarke and Parsell, 2019). Second, we need to recognise the diversity of actors and institutions involved in the governance of homelessness which, in addition to law enforcement, includes an extensive network of care workers, volunteers and local governance actors. Categories such as ‘the police’ and ‘the state’ need to be unpacked as there are often tensions between their different departments (Carlsson Stylianides et al., 2022), while how policies are interpreted and implemented by individuals on the ground can vary greatly (Johnsen and Fitzpatrick, 2010; Lipsky, 1980). Third, the poverty management approach extends the geography of homelessness beyond public space to shelters, service centres and prisons as ‘strategies translate into specific sites of management that vary over time’ (DeVerteuil et al., 2009: 652). An example of a more ambivalent poverty management response to homelessness is homeless shelters. Shelters provide some basic needs and can be seen as a counterweight to direct punitive measures such as incarceration. At the same time containing homeless people in shelters also regulates social order and reduces the visibility of homelessness without addressing key causes (DeVerteuil, 2006).
Housing-led approaches to homelessness
In contrast to punitive responses that exclude the homeless from public space and managerial approaches that regulate them in shelters, housing-led policies seek to solve homelessness by increasing access to permanent housing in regular neighbourhoods. The housing first model – advanced by Sam Tsemberis and colleagues – departs from the staircase model by asserting that a homeless person first needs a house to overcome other barriers such as addiction or unemployment. This philosophy has inspired many housing-led policy initiatives around the world, for example in Copenhagen, Glasgow (Boesveldt, 2015a), Finland (Tainio and Fredriksson, 2009), Alberta (Anderson-Baron and Collins, 2018) and Brisbane (Clarke and Parsell, 2020). Although housing first programmes are progressive and anti-paternalistic in theory, they have attracted their share of criticism. Hennigan (2017) finds that in Arizona, a paternalistic approach is found in a housing first project. ‘Case management’ is centred around improving individual life skills such as housekeeping, personal hygiene and communication skills. The lease, furthermore, functions as a disciplinary instrument as evictions are used ‘a powerful tool’ to impose (self-)discipline. This can also be seen in Sweden where ‘social contracts’ with special terms are used to house homeless households in a secondary sub-leased housing market (Knutagård et al., 2021). As there is little national state involvement in Sweden, this leads to significant variation in local practice (Carlsson Stylianides et al., 2022). Social services and local landlords can decide who is eligible for housing and whether and when a social contract is continued as a regular lease (Wirehag, 2021), making housing first approaches vulnerable to the moral and normative assumptions of the actors implementing them (Boesveldt et al., 2017; Wirehag, 2021). In addition to such biases, Clarke et al. (2020) emphasise how public housing policies shape the ways in which local service providers adapt housing-led strategies. In Australia, they found that although state policies espouse housing-first approaches, conditionality remains an implicit feature of the government’s response to homelessness, especially for people with complex needs. In Canada authors warn that without addressing structural causes (e.g. unaffordable housing markets, the cost of living, deteriorated health support and precarious jobs) housing first policies frame homelessness as an individual problem by providing individual solutions (Anderson-Baron and Collins, 2018; Katz et al., 2017; Oudshoorn, 2022).
The literature on housing first shows that policies and their implementation vary significantly between cities and countries. These local variations are sometimes in conflict with the characteristics of housing first, although one should note that the original model is also not free of conditions and assumptions (Katz et al., 2017). There is thus an urgent need for more research into the local translation of housing-led approaches over the world. We apply the ‘management of the poor’ framework to investigate the Dutch response to homelessness. This framework allows us to recognise the complexity –punitive and caring elements – and the diversity of actors, instruments and sites that can be part of urban governance. Through studying housing-led approaches we also extend the management of the poor framework that has mainly centred around the American shelter system and the governance of public space to a new site: the private home. Building on housing first critical studies, we argue that housing is used as an urban governance instrument to regulate the behaviour of people formerly experiencing homelessness.
Methodology
Case description
Between 2007 and 2015 the Dutch system of social support and long-term care, including homelessness services, was substantially reformed. Since then, municipalities have been under the Social Support Act (Wmo) responsible for the provision of social support, emergency shelters and protected living arrangements. Typically, the municipalities work together in regions of five to eight smaller municipalities, in which the largest municipality is responsible. Longer-term and more intensive care is organised through the Long-Term Care Act (Wlz), which is executed on a regional level by health insurance companies. The reforms promote deinstitutionalisation, self-reliance and participation in society; public support is only meant to be temporarily for people deemed incapable of arranging support on their own.
The reforms arguably signify the take-off of a housing-led approach to homelessness. Around the same time the Advisory Committee on the Future of Protected Housing (2015) published the vision report ‘From protected living towards a protected home’. Their advice – that was taken as a guideline by municipalities –‘moves away from the staircase model’ (Advisory Committee on the Future of Protected Housing, 2015: 15) and advocates for a safe and stable independent place to live with flexible care. For people with higher care needs small scale protected living facilities in the neighbourhood are envisioned. In 2020, the Council for Public Health and Society issued another advisory report ‘First a Home’ (Eerst Een Thuis, Council for Public Health and Society, 2020). These reports ultimately informed the launch of a national approach to homelessness that prioritises ‘First a house, then recovery’ (Van Ooijen, 2022: 6). With this the national government hopes to stop homelessness which has experienced a steep increase over the last 10 years (Statistics Netherlands, 2019).
While homelessness was previously the responsibility of the Ministry of Health and Welfare, the latest policy initiatives extend responsibility to the Ministry of Internal Affairs, which is also responsible for housing. This is also evident from the close alignment of the national approach to homelessness and the national housing task. Two hundred and fifty thousand new social housing units are planned to be built before 2030, also addressing the need of low-income people ‘including homeless people’ (Van Ooijen, 2022: 32). Furthermore, municipalities are now required to include a vision for people at the risk of experiencing homelessness into their housing strategies. For these tasks additional funding has been made available from 2023 to 2027 by the Ministry of Health and Welfare (325 million) and Ministry of Internal Affairs (1.5 billion) (Van Ooijen, 2022). These changes signify the new framing of homelessness: from primarily a health issue to one of housing.
This requires increased social housing availability. Most social rental stock is owned by housing associations. These are semi-private organisations with the public task of delivering affordable housing for low-income groups. Access to social housing is through a waiting list, although priority access is possible for ‘urgent’ groups, such as people leaving homeless shelters and refugees. The whole country is dealing with a shortage of affordable housing as the social housing market has been restructured severely (van Gent and Hochstenbach, 2020).
Since the 90s the share of social housing has decreased from around 41% (Priemus, 1995) to 34% in 2022 (Statistics Netherlands, 2023). The waiting time is often more than seven years, and in some municipalities even more than 17 years (Kraniotis and De Jong, 2021).
The new housing-led approach pushes the policy domains of housing and care closer together, but at the municipal level these bodies are still divided; social support and housing, for example, come under different municipal departments, executing acts from different national ministries. This makes the governance of homelessness complex and multi-layered.
Methods
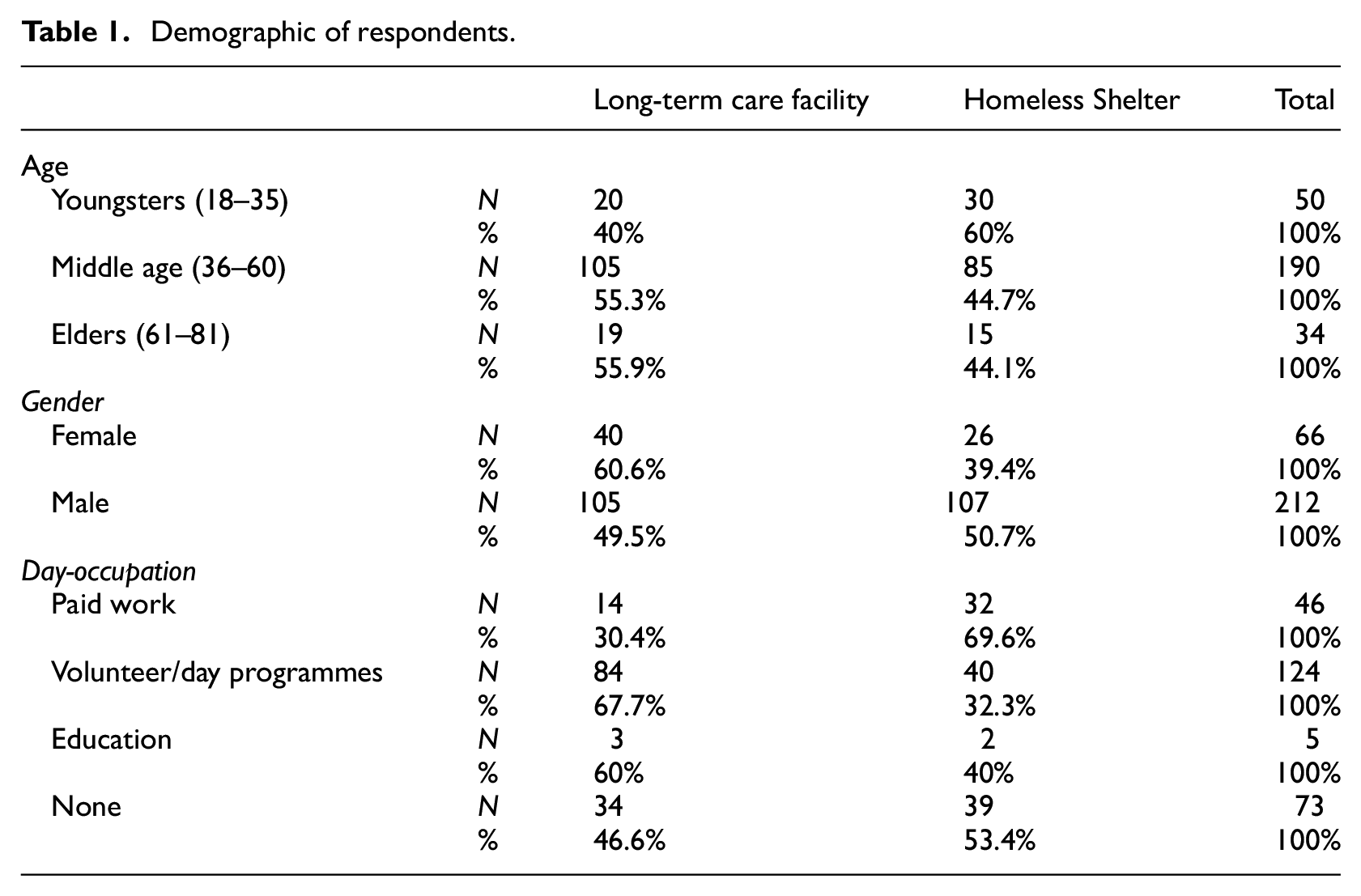
This paper builds on a larger longitudinal research project 2 that studies deinstitutionalisation and decentralisation of homeless and protected housing services, from the perspective of (former) residents of emergency shelters and long-term care facilities (hereafter: resident participants) and professional stakeholders (professional participants). Professional participants included representatives of housing associations, municipal employees responsible for housing, homelessness and social care, insurance companies and police officers. This study took place in in seven Dutch regions, encompassing 34 municipalities. Large cities (the Hague and Utrecht), medium sized cities as well as several smaller municipalities participated in the study. Figure 1 shows a map of municipalities and participants involved in the study. The participants in these regions were followed on a yearly basis between 2018 and 2022. Participants were interviewed two to four times. The longitudinal study was set up in order see how long it takes for people to receive independent housing, and what happens after they have received such an offer, as we know from other studies that relapse into homelessness occurs frequently (McQuistion et al., 2014). This longitudinal approach also enabled us to follow the process of deinstitutionalisation and housing-led policies from the professional perspective. Policy processes take time and intentions and goals are not always met. In total, 1045 interviews with 536 participants took place: 278 resident and 258 professional participants. Of the resident participants 133 (47.8%) resided in a homeless shelter at the first time of an interview, 145 participants (52.1%) resided in long-term care facilities. Table 1 provides an overview of the age, gender and day-occupation of the resident-participants in this study.
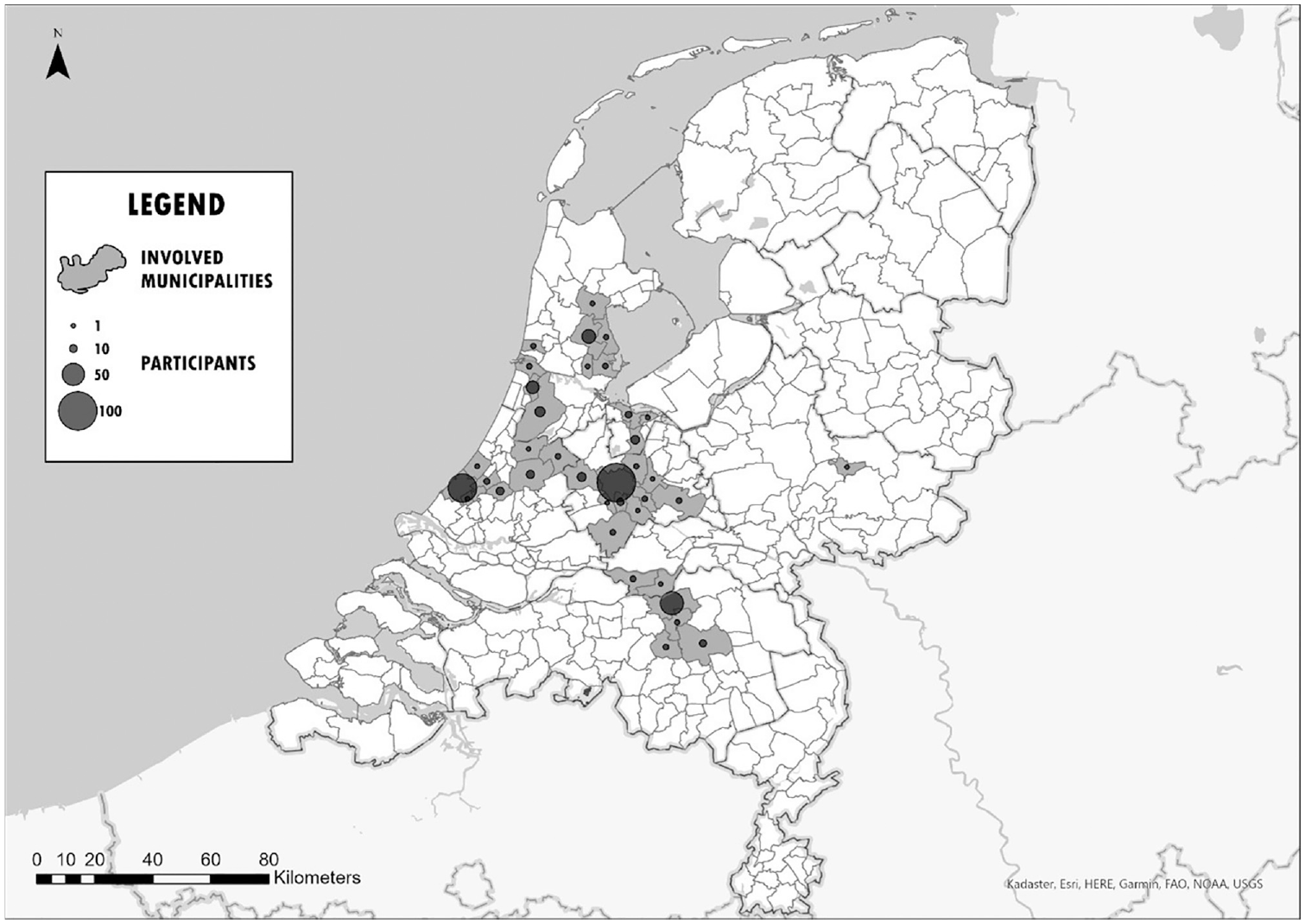
Map of research areas.
Demographic of respondents.
All participants gave their written informed consent prior to participation. The researchers explained the content of the consent form and emphasised the anonymous and voluntary nature of participation, and that participants could decline to answer any questions or stop their participation at any time.
Interviews were done by research assistants, university researchers and the authors of this paper. We used different semi-structured interview-questionnaires depending on the role of the respondent. Resident participants were interviewed about their housing/homelessness pathways, their care networks, needs and experiences. These interviews were conducted together with trained peer-support workers to ensure a comfortable environment. Professional stakeholders were asked about policy development and implementation. Specific questions addressed the drivers of policy, the instruments used to implement them, and any barriers to achieving the policy goals.
All interviews were audiotaped and transcribed. Content analysis of the interview transcripts proceeded in two steps: (1) deductive analysis using predetermined codes (see Boesveldt, 2015b for the theoretical model behind the coding) and (2) inductive analysis to generate new codes and to reduce the complexity of the data (Thomas, 2006). Conditionality was one of the themes that emerged from the inductive part of the analysis. This then led us to go back to the interviews, specifically the parts that addressed independent housing, and analyse these again through the theoretical lens of the management of the poor.
Results: Risks of extending the management of the poor to the (new) private domain
We observed the growing popularity of housing-led approaches to homelessness in all studied regions. In six of these seven regions, additional agreements have recently addressed the number of social rental units available with priority to persons leaving short-term shelters and care institutions; the seventh region is currently drafting such agreements. Different municipalities have also started their own pilot projects with housing-led initiatives. In the regions we studied, all parties agreed that municipal housing departments, housing associations, the police, the care department and care and homelessness institutions need to work together to facilitate deinstitutionalisation. In what follows, we present our findings concerning the conditions homeless persons must fulfil to be eligible for independent housing, the conditions they must fulfil to keep their homes, and the punitive side of current policy instruments. Together these themes show chronologically, from receiving housing to (after) eviction, how the management of the poor is extended to the private realm.
Conditionality in the decision-making process: Who deserves a home?
Agreements on housing for prioritised groups, together with the severe housing shortage, lead to long waiting lists and strict conditions for who can apply for priority housing. In many of the regions we studied, the agreements between housing associations, municipalities and care institutions concern individuals who are deemed unable to take care of themselves but whose cases are not ‘too complex’. This is in line with the Dutch Social Support Act which seeks to limit help to those who are unable to arrange their own affairs.
The lack of regular affordable housing means that people without additional care needs often fall through the cracks. Misha, a middle-aged woman, residing in a homeless shelter at the time of the interview represents such a case. She has a paid job but became homeless after her relationship ended as she was not registered in the municipality for long enough to access regular social housing. As Misha wished to stay close to her children, she did not want to go to a region with more accessible housing, as was suggested by the municipality. Initially, she was deemed too self-reliant to meet the emergency shelter threshold. Only by lying about her situation did she receive a place in the emergency shelter and, eventually, priority access to permanent housing: ‘I indicated that I could not clean, that I had difficulty opening mail. That I’m a little cuckoo. Anything to make sure I would get a home’. Misha received a social housing offer with a care-priority only after she had spent five months in the shelter. In the meantime, she experienced severe stress and began smoking too much weed to cope. She told us, ironically, that her time in the shelter made her less self-reliant. But now that she has a place of her own and is able to take care of her family again, things are better. She told us: ‘That man from the social support team who was here yesterday already said: “You are one of the few who have everything in order, I see no reason why I should come here”’. Misha will receive mandatory guidance from the social support team for at least two more years.
While people like Misha are deemed ‘too independent’, other conditions stipulate that clients are not ‘too complex’. The criteria vary between regions and municipalities. One region requires clients to stay within the intramural setting for over three months to see what kind of support or house would fit best. Another municipality requires participation in meaningful day-to-day activities, remaining sober for a certain period, and a background check by the police. In another region people were required to apply to regular social housing offers on a weekly basis for over a year to ‘prove their motivation’– a requirement that conflicts with the national guideline that people should not stay in the homelessness service for more than three months (Valente, 2020). The residents we interviewed in emergency shelters and intramural care institutions were rarely well informed about this requirement and computers were not always available.
Professional respondents often mentioned Skaeve Huse 3 as a solution for people seen as too difficult or not ready for regular independent housing. This originally Danish model houses people, sometimes in containers, on the outskirts of the city to avoid neighbourhood nuisance. Skaeve Huse initiatives are currently sprouting like mushrooms throughout the Netherlands. Although hard to implement and routinely met by Not-In-My-Backyard sentiments, most of the professional stakeholders we interviewed were enthusiastic about these projects. In 2010, only five such projects had been realised in the Netherlands, but by 2022, we discovered at least fifteen that were built and five more that were planned. There has been scant research on these housing arrangements, although we do know that the level of support provided varies greatly (Singelenberg, 2010). While it can be a good solution for people who prefer to live in an isolated environment with minimal triggers, we observed that Skaeve Huse is often presented as the only alternative for people deemed unfit for regular individual residency. Other more intensive arrangements were not tried or properly implemented. Such arrangements could include housing first or other structural solutions to homelessness such as permanent housing in a more protected setting with adequate intensive support.
The move towards housing-led approaches and deinstitutionalisation were thus accompanied by strict requirements on eligibility. People deemed too independent, ‘too complex’, or not willing or ready enough were excluded. We observed significant variation in both the conditions stipulated in rental contracts and in how they were enforced. In some cases it was left to the care institutions; in other cases, housing associations, the police, the municipality or a combination of these parties were involved. The lack of clear guidelines put a premium on subjective judgement by the responsible party. A municipal worker warned us of the potential for cherry picking clients deemed deserving:
What I hear is … that there is a lot of cherry picking. Like ‘yes he is doing so good, we will give him one [an apartment]’, even if it is a person who would have gotten an apartment based on his waiting time anyway. But the ones who misbehave, yes, we don’t trust them, so they don’t get one.
The emphasis on housing readiness and conditionality shows that the staircase model persists. As we will see in the following section, conditionality is not only present in decisions around eligibility; it continues after people have left emergency shelters and institutions and have been rehoused.
Conditionality after receiving independent housing
People offered independent housing mostly described this as a very positive development; a place of one’s own was often a huge improvement compared to the homeless shelter or institution. Nevertheless, we saw how housing-led initiatives often went hand-in-glove with more conditional and punitive approaches. Although municipal policies in the majority of the studied regions state that all persons living in homeless shelters and supported housing have a priority right to independent housing, it invariably entailed a three-party contract or a conditional lease. The conditions often included mandatory care, abstinence from drugs (including alcohol and otherwise legal weed), mandatory debt management and ‘good tenant behaviour’. Housing corporations set these additional requirements for a minimum of six months, although two years was more common. In some cases, the conditional period was extended. If the resident did not comply, the lease could be terminated. A professional stakeholder from a regional housing department described the growing use of this type of rental agreement:
If you get a renter who gives you a fishy feeling, maybe when someone arrives unwashed and smelly at the housing association, and you think ‘I can’t entrust you to this neighbourhood’, you can now choose for it [a conditional rental agreement].
The use of conditional housing contracts was seen by most parties as an effective strategy. The residents we interviewed were rarely critical of their contracts. Some believed they would not break the conditions and did not take issue with them. Damian, a middle-aged man with no day-occupation who was homeless until recently, now lives in a project where previously homeless persons mix with regular renters, explained:
Yes [it is a conditional lease], but that doesn’t matter for me … for me it does not make a difference. I just live here, it’s my house. Those conditions are for people who are not ready to live on their own. I actually think it’s a very good rule: you have to stick to the conditions, otherwise you lose your house. But for me, that’s not a problem.
Others indicated they appreciated the idea of having a ‘transition’ time as they feared not receiving adequate support if care providers were not party to the rental agreement. Especially people who have experienced street homelessness for a long time and/or have a specialised mental health care need, tend to appreciate or not mind the conditionality. People with lower care needs, who can manage their own finances and/or have a paid job more often object to the conditions.
Mees, a middle-aged man with no day-occupation rented an apartment with a conditional lease when we first interviewed him. At our last (fourth) interview, he continues to rent under a conditional lease, which is his wish. He is satisfied with the specialised ambulatory support he receives – part of his conditional lease which would end if he were to change to a regular lease. Mees explains why he prefers his current situation:
Because I like the way things are going now. … It turned out that I was allowed to keep [the conditional lease] for the first few years. I’m happy about that. … I’ve had three or four [care workers] before, and they were all there for a period of one and a half years. Now I’ve had it for a long time. That really does make a difference.
However, we often observed that the agreements were not clear for the new residents. Some did not even know they had signed a conditional contract; others were not fully aware of the conditions and consequences should they be unfulfilled. There were cases where support was missing in the first, often crucial, weeks. John, a middle-aged man and participating in voluntary work, whom we spoke three times over the past three years, is an example. Between the first and second interview, John transitioned from the psychiatric and addiction department to an independent home. He did not receive a regular housing contract but was offered a three-party contract that included himself, the care provider and the housing association. The contract had an appendix stating that he was not allowed to use alcohol or other drugs. When John moved to his own home, there was no organised support, even though the first days of independent living are known to be full of stress and highly triggering. His former caregivers were no longer responsible while the new team to offer care at home would only start next month. In the intervening period, John relapsed into alcohol and drug use. Failing to meet the conditions in his rental agreement, he immediately lost his home.
That [living independently] lasted five weeks because the outpatient care just didn’t work that well. I lay on a mattress on the floor for three weeks and then they thought it was crazy that I relapsed into drug use and alcohol use. … The first two, three weeks nobody came. … Before the assistance started, I had already relapsed.
John is now back in the psychiatric department, although he and his caregivers do not feel he belongs there. A long waiting list prevents him from moving out again. Even if he could, John told us he has lost faith and is unsure whether he will be able to ever live independently again.
Conditional leases dictate what people are allowed to do in their private homes and can be used by professionals to discipline formerly homeless people. Some housing and care organisations explained how they plan an eviction, without the intention to evict, as a way to motivate tenants to change their behaviour. A housing association employee spoke of how they used the threat of eviction to force a resident to make an appointment with the psychiatrist:
What we often do is that we really plan the eviction. You have to be very hard towards the people: ‘Yes nice if you do nothing, [but] then you will be evicted that day, so you must have your appointment for that day’. Once the process has been started, we will postpone it.
Although some tenants are happy with this as it ensures the involvement of care parties, relapse into substance use or problems with the rent or neighbours will result in eviction, making them homeless or institutionalised again and undermining their recovery. Moreover, decisions to evict are often highly subjective and up to housing associations or caregivers. In one region, a person was evicted because he behaved ‘differently’. Neighbours complained that he frequently flapped his arms on the balcony which eventually led to the lease being terminated. A professional stakeholder working in this region expressed her worries:
It is distressing. Especially for the people with whom we try independent living, and for whom it doesn’t work. After the conditional period of two years their rental agreement is not continued and then they become homeless again. They have to go back to a protected living facility, but these have long waiting lists.
This is especially problematic as preparation is often minimal and care and support are not always well organised in the initial period after receiving a house. Institutional teams did not always offer continued support outside the protected living facility or emergency shelter, while home-based support services in the neighbourhood had waiting lists, or were not actively involved by the institutional teams preparing residents to transfer to their own home. Many residents transitioning from shelters or protected housing found that the home-based support services in the neighbourhood did not sufficiently reach out to them; others were unconvinced that they would receive the support they needed. The same problem was also mentioned by various social support stakeholders.
Due to the lack of available support, the police participants we interviewed reported increased work pressure in residential areas. With the lack of effective aftercare, the police are often seen as the first point of contact in the neighbourhood. Police participants often felt they were on their own and wished to see care parties taking more responsibility for clients leaving homeless shelters and protected living facilities. We observed that the police eventually intervene when social workers or doctors are unavailable or when persons in distress do not accept their interventions. But police professionals indicated they are not always equipped to perform specific care tasks. In at least two regions, we observed the police transporting mental health clients in crisis when the mental health services were unavailable. In a context of insufficient health care, a housing-led approach thus does not necessarily lead to unconditionality. Housing associations and care providers are reluctant to provide regular independent housing as they are afraid that the residents are ‘not ready’ and will become a nuisance to the neighbourhood. Whenever this happens, people are increasingly helped by a punitive police system, rather than a specialised social health care system.
The conditional agreements illustrate weak tenant rights and the lack of separation between the rights to housing and care. This hinders their freedom and can influence the feeling of home among residents. We spoke to Marie (middle-aged, working, studying and living independent in a housing-first project) who had just heard that after two years of conditional renting her lease was not transitioned into a permanent lease. Even though she did not break any of the conditions, her finances are well (self)organised and her mentor thinks she is doing well, the conditionality was extended for another two years. Marie was very disappointed and told us that ‘it does not feel like a home, as you’re under constant surveillance’.
Punitive practices following eviction
Punitive measures do not end with eviction. Multiple housing associations indicated the use of denial-of-service lists for renters with a history of payment arrears or eviction. The practices varied; some housing associations took a case-by-case approach while others did not accept listed renters for a period of five years. In some cases, names were shared with other housing associations in the region. While most housing associations were vague about the precise workings of such lists, others were forthright about the practice and described the ‘direct exclusion trajectory’ on their websites:
Persons who previously had problems with their housing association or a court decision, for example due to rent arrears or nuisance and who have been evicted due to a court ruling, are no longer allowed to rent a home from housing associations in the entire regional housing market for five years after the judge’s ruling. (Rijnmond, 2022)
Housing association participants told us that they need to consider both the privacy of the home seeker and the social responsibility of housing associations to accommodate people with limited resources. ‘We do our utmost to accommodate problem cases, either in our homes or in the homes of a colleague corporation, so to speak’. Still, they were clear about cases ‘where it will really stop’, usually mentioning hemp cultivation and very high rent arrears. While housing associations admit that it matters ‘whether the person acts like this due to a limitation or to wilfulness’, they acknowledge that they are not care professionals and often find it hard to distinguish.
Denial-of-service lists effectively penalise people twice: through the courts and by taking away their right to housing in the subsidised social sector. We interviewed multiple people who had been listed and became ineligible for priority housing. Their remaining choices were the expensive private rental sector, homeless shelters or care institutions. André, a middle-aged man with paid work, residing in a homeless shelter, told us the first time he was interviewed that he was blocked from accessing the social housing market of his region for five years after being evicted for cultivating weed in his attic. He had struggled for years with a cocaine addiction and had been clean for several months when he was evicted. Afraid that he would return to his cocaine habit at the shelter, André spent a long time ‘wandering around’, unable to start his recovery. As he could not find other affordable housing options, he slept rough for over five years.
Discussion and conclusion
Housing-led policy interventions to combat homelessness, prioritising housing rather than treatment, have gained prominence internationally (Busch-Geertsema, 2014; Tsemberis and Eisenberg, 2000). Based on a qualitative longitudinal study of the experiences of people (formerly) experiencing homelessness and professional stakeholders in the Netherlands this paper makes several contributions.
First, by paying particular attention to the Dutch context, we show how the implementation of the housing-led approach is hampered by health-care cuts, decentralisation and an affordable housing shortage. Not all people experiencing homelessness are given the chance to live independently. While conditions varied greatly, the national and local policy discourse on self-reliance dictates that people without additional needs are ineligible for priority housing. The lack of affordable housing in the Netherlands renders the insistence on self-reliance unrealistic and a barrier to solving homelessness.
On the other hand, persons experiencing homelessness cannot be ‘too complex’ either and must demonstrate deservingness for priority housing. For those deemed ‘unmanageable’, Skaeve Huse – housing on the outskirts of society – is gaining popularity as a solution. Professional stakeholders justify this approach by indicating that these people otherwise would become a nuisance to the neighbourhood, but this is something that primarily happens because the appropriate care is not available.
The Dutch housing-led approach to homelessness requires the involvement of new actors including housing associations and municipal housing departments. Together with the local police, they are increasingly responsible for care tasks as well as determining eligibility for priority housing. But as the governance of homelessness was previously the responsibility of the social and municipal health services, these new actors lack experience and expertise. Regulations and outcomes vary both between and within municipalities as local actors bring their own values and prejudices. Without specialised NGOs and clear national guidelines, the entanglement of housing and care leads to blurred responsibilities, the cherry picking of eligible clients and the crumbling of rental and human rights.
In this context people accept conditional leases. Specialised ambulatory care (at the home) is not easily arranged but is secured when signing a conditional lease. Other care providers have long waiting lists or staff shortages or lack the needed expertise. Priority housing with conditional leases further circumvents regular waiting times for social housing. Some people thus appreciate the conditional contracts, not because they are conditional, but because they mean access to specialised care and housing.
Therefore, whereas a housing-led approach to homelessness is more effective than the stair case model (Busch-Geertsema, 2014; Tsemberis and Eisenberg, 2000) our study shows that it is indeed important to investigate how this is ‘translated in a particular context’ (Clarke et al., 2020). In the Netherlands policy doctrines relying on self-sufficiency, health-care cuts and the affordable housing shortage undermine both the human right to housing and a more humane and effective approach to homelessness. This aligns with previous studies cautioning that housing-led and housing-first approaches are not free of conditions (Hennigan, 2017) nor are they a ‘silver bullet’ (Katz et al., 2017). To be truly effective, they should come in together with policies that address systemic poverty (Oudshoorn, 2022).
As this study was part of a broader research project on homelessness, independent housing was just one of the topics in the interview guides. We therefore do not have in-depth accounts of how people experience punitive, controlling and conditional practices. As the housing-led approach is relatively new in the Netherlands, most of the respondents have not been living under conditional leases for longer than three to four years. Future research could take a more ethnographic approach, to study the even longer-term experiences of housing-led approaches. Furthermore, we focus only on the broader trends across the Netherlands, although significant differences between municipalities are present. A further study could compare housing-led approaches across municipalities.
This paper also revealed the often ambivalent and complex nature of urban governance (DeVerteuil et al., 2009) by positioning the housing-led approach in a ‘poverty management’ framework. Through dictating who gains access to specialised health care and independent housing and who is removed to the outskirts of society, as well as adding conditions to the lease, government actors can select ‘appropriate’ tenants and regulate behaviour in private space. Conditional contracts prohibit certain behaviours deemed acceptable for other residents. Transgression of the rules can lead to eviction and banning from the regional social rental sector. This underlines that housing has become an instrument in the urban governance of marginalised populations such as homeless people.
Our findings extend the poverty management perspective on homelessness. While traditional poverty management practices controlled the movement of homeless persons in public space and shelters (DeVerteuil et al., 2009; Hennigan and Speer, 2019), housing-led responses have added the private home to the sites of governing homelessness, leading to multifaceted arrangements and ambivalent outcomes. While housing is arguably the most important and immediate solution to homelessness, this does not necessarily entail the end of control. Alongside the supportive response of providing housing, more punitive practices – often entwined with care – continue in the housing domain, now executed by the providers of social housing.
The incorporation of the private realm in the governance of the poor ties into a wider development of crumbling housing security for, in particular, marginalised populations (Alam et al., 2022; Power, 2023). A home can be the site where people (re-)establish a sense of security in the world; a refuge where one feels in control and free to be themselves in absence of surveillance (Dupuis and Thorns, 1998; Power, 2023). The current Dutch housing-led approach to homelessness provides a home to a select group of people, but at the same time threatens this sense of ontological security. Housing is not a right, nor a safe space, but a conditional instrument that can be taken away.
Footnotes
Acknowledgements
Data-collection for this study has also been carried out with the help of students and researchers in our team (Tommaso Amy, Marte Kuipers, Juul Mulder, Merel Otto, Marieke van der Star and Charlotte van der Veen) and experts with lived experience have acted as peers in interviewing clients (Robbert Brouwer, Thijs Kuiling, Peggy DeMilt, Wim Eickholt and Stan Coldewijn). Also, we want to thank all participants for their genuine and honest stories. We furthermore thank Jan Willem Duyvendak and Harry Pettit for commenting on an earlier version of this article. Finally, the comments of the anonymous reviewers provided valuable feedback for finalising this manuscript, and we appreciate their time and attention.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of financial support for the collection of the research data from several Dutch municipalities and NGOs active in the field of long-term care facilities and homeless shelters between 2018 and 2022. The findings and views reported in this article, however, are those of the authors and should not be attributed to these municipalities and NGOs.