
Abstract
Different types of environment stimuli (e.g. noise, aesthetics) in urban environments are becoming better understood as determinants of the mental health of urban dwellers. Research on the impacts of urban exposures, especially those related to urban designs, and their potential impacts on the mental health of adolescents specifically, however, is currently lacking. In this study, we examine the relationships between five pedestrian- and transit-oriented design (PTOD) concepts – imageability, enclosure, human scale, transparency and complexity – and adolescent emotional responses to six settings of varied PTOD quality, and discuss potential design-related emotional affordances within Gibson’s Theory of Affordances (ToA). Using an online survey method with videos of each setting, a nationally representative sample of Canadian adolescents viewed the videos and indicated responses to six mental health indicators (positive affect, negative affect, calmness, anxiousness, perceived restorativeness and mental demand). Adjusted linear mixed models (LMMs) were constructed to examine the association between different urban settings and each outcome. Results indicated that, generally, as the quality of five PTOD concepts increased, as reflected in the scores of the different settings, positive emotional responses tended to increase while negative responses decreased (excluding mental demand). Within the frame of the ToA, multiple emotional response outcomes were significantly associated with settings high in aggregate PTOD quality (e.g. Plaza-Positive Affect: β = 0.116, 95% CI: 0.010–0.222, p = 0.033; Bluespace-Mental Demand: β = −1.634, 95% CI: −1.770 to −1.498, p = <0.000), suggesting such spaces may be perceived by adolescents as possessing greater emotional richness with respect to affordances. Future studies should further explore these relationships with other means (e.g. objective methods).
Introduction
Adolescence (10–19 years) is a primary period for social, emotional and cognitive development in an individual’s life. Given that 50% of mental health disorders begin by the age of 14 (Kessler et al., 2005), and that the onset of mental health disorders during this time – and specifically by age 14 – account for 13% of disability-adjusted life years (Vigo et al., 2016), preventing the development of mental disorders and promoting mental health during adolescence is of great significance. Efforts to address the development of adolescent mental disorders are doubly significant when recognising that rapid brain development renders youth particularly vulnerable to the development of chronic health issues (Dahl, 2004). For example, the onset of mental health disorders during this time can contribute to several negative long-term health outcomes, including an increased risk of heart disease and stroke (Scott et al., 2016), long-term disability (Kapungu et al., 2018) and eventually a heightened risk of all causes of early age mortality (Kessler et al., 1995). One important influence relevant to the issue of adolescent mental disorders is external environment exposures. Studies of environmental toxins and mental illness have, for example, previously observed links between toxin exposure levels and antisocial behaviour (Needleman et al., 1996) and neurobehavioural disorders (Weiss and Landrigan, 2000), as well as relationships between high-stress early-life environments and reduced prefrontal cortical grey matter (i.e. matter in the central nervous system involved in the control of memory and emotions) (Gianaros et al., 2007). Increasingly, other exposures such as urban designs are being explored as important factors affecting the mental well-being of young people (Buttazzoni et al., 2022; Sun et al., 2018). However, such study is in its nascent stages and has been critiqued for lacking precision in its investigation of relevant relationships (Fleckney and Bentley, 2021). To address this gap, the present study examines the relationships between specific pedestrian- and transit-oriented design (PTOD) concepts, as reflected in videos of six distinct urban settings, and a range of subjective affective responses among adolescents in Canada.
Impacts of urban environments on adolescent mental health
Previous research has outlined several ways in which urban environments impact adolescent mental health and disorders. Cross-country trends have found that: in India, adolescents in urban areas report higher rates of mental disorders relative to their rural counterparts (Pillai et al., 2008); Bangladeshi youth in urban slums are significantly more likely than other urban and rural dwelling groups to have serious behavioural problems (Mullick and Goodman, 2005); and in a multi-city study across three continents, certain groups of adolescents living in economically distressed areas of their respective city and who reported poor perceived social support had significantly higher odds of depression than those with greater perceived social support (Cheng et al., 2014). More precisely, environments structured to prioritise vehicles produce high levels of noise that induce sleeping issues (Tiesler et al., 2013), while poor pedestrian route directness may increase the risk of depressive symptoms (Duncan et al., 2013). Conversely, preventive effects of urban designs may be accrued through exposure to more natural areas such as greenspaces (e.g. parks) which can, for instance, reduce ADHD symptoms (Amoly et al., 2014). Moreover, built designs that feature higher-quality environmental aesthetics (e.g. more tree shading) (Sun et al., 2018) and sidewalks (Rothman et al., 2018) can promote physical activity, which has been linked to improved mental health such as increased incidences of positive affect. Although these relationships have received more study recently, the impacts of specific exposure concepts (e.g. the quality of spaces) (Vanaken and Danckaerts, 2018) remain unclear.
Pedestrian- and -transit-oriented design
PTOD is a relevant planning paradigm that outlines multiple specific built design concepts that may be used to examine more precise linkages between urban environments and adolescent mental health. The PTOD paradigm centrally aims to support accessibility and active travel infrastructure and ultimately improve pedestrian usage of public spaces (Renne, 2016). To achieve these objectives, important PTOD concepts include: imageability, enclosure, human scale, transparency and complexity. Imageability, a design concept thought to contribute to ‘sense of place’ (Ewing, 2013), refers to the distinguishing features of a setting (e.g. landmarks, architectural structures) which can make it particularly memorable (Gehl, 1987). Enclosure, or a space’s potential to cultivate a sense of ‘hereness’ or presence (i.e. identity with surroundings) (Cullen, 1995), describes the vertical nature of a setting and to what extent its relevant features (e.g. buildings, trees) create a ‘room-like quality’ (Ewing, 2013). Human scale centrally outlines the orientation of a setting’s physical qualities (e.g. infrastructure) (Ewing, 2013) towards either pedestrians –‘lower-speed’ designs (e.g. lower speed limits, street furniture) which may improve comfort – or vehicles –‘higher-speed’ designs (e.g. wider roads, higher speed limits) which may be more overwhelming (Kay, 1998). Transparency has been associated with spatial awareness (Arnold, 1993) and denotes the level to which human activity is observable beyond a street or public space as a result of windows, doors, landscaping and other openings (Jacobs, 1993). Finally, complexity encourages engagement with one’s environment (Nelessen, 1994) and captures the visual richness of a setting via the range (i.e. number, styles) of present architecture, buildings, ornamentation and landscape features (Ewing, 2013).
Theoretical frame: Theory of Affordances
The Theory of Affordances (ToA) further contextualises the research described here. A transactional environmental psychology framework, this theory posits that affordances are value-mediated relational processes which drive human–environment interactions, and are the result of both what a person’s intentions and capabilities are as well as what an environment presents the person (e.g. layout of an environment, other people, objects) (Gibson, 1979). Recent evolutions of the ToA suggest that affordances are a form of realism about meaning, and that affordances – meaning – are the result of the real (objective) and perceivable (subjective) rather than a property of either the environment or the individual (Chemero, 2003). Consequently, this contemporary perspective allows for the examination of an environment’s ‘functional significance’, or the ways in which affordances are or aren’t supported in a particular setting. This approach has been employed to explore similar topics like adolescents’ use of space (Clark and Uzzell, 2002) and the needs of young people regarding local parks (Townshend and Roberts, 2013). Clark and Uzzell (2002) applied the Theory to investigate adolescent perspectives of affordances in various urban environments to illuminate this cohort’s understanding of the functional significance of different designs with respect to support for developmental needs, social interaction opportunities and retreat experiences. In this way, functional significance constitutes the social and physical aspects of an environment necessitating that an individual and their context jointly contribute to the meaning and nature of a phenomenon (Heft, 2010). Such framing can help to identify important emotional affordances associated with the PTOD quality of public spaces. Put more precisely, this framing can be used to identify ‘restorative niches’, or “‘stable’ place features that offer opportunities to promote wellbeing” (Roe and Aspinall, 2012: 3229) through reflecting health-supporting links between personal needs and particular environments – in this context, between adolescent mental health and PTOD place quality. Having established this theoretical frame, we use the ToA to investigate the functional significance of affordances outlined as the relationship between the physical PTOD quality of urban areas and subjectively reported adolescent mental health outcomes. Therefore, in the present article we seek to explore the nature of PTOD affordances regarding their impact on six self-reported measures of adolescent mental well-being.
Research justification and questions
Examining the links between urban morphologies and their attendant impacts on the mental health of people is becoming an increasingly popular topic of interest for city designers and urban planners. For instance, concepts like ground-floor setbacks have been noted as a central factor in defining the sense of enclosure associated with a sidewalk or streetscape, or more broadly a street environment’s general visual appeal (Burden et al., 2013), while more transparent facades can increase pedestrian activities and socialisation in a public area (Gehl, 2010). However, how these dynamics affect particular groups like adolescents remains largely unknown at present as young peoples’ and adolescents’ socio-spatial experiences of urban areas have been relatively understudied when compared to other groups (Skelton and Gough, 2013). Consequently, suggestions to improve the study of adolescent mental health and urban environments have noted the potential of exploring the impacts of specific design concepts (Buttazzoni et al., 2022). This article addresses these points by examining different affordances in the form of the quality of distinct design exposures (i.e. PTODs) in different urban settings, and how they are associated with a series of adolescent mental health indicators. To this end, the following research question was posed: What are the relationships between PTOD exposures, as reflected in the six different settings, and adolescent mental health indicators (i.e. positive affect, negative affect, calmness, anxiousness, perceived restorativeness and mental demand)?
We settled on the six specified outcomes of interest listed above as indicators for mental health for three central reasons. First, we selected three sets of distinct dimensions of mental health that are mutually opposite or exclusive; that is to say, for example, it is unclear how one might be both very positively affected and negatively affected at the same time. Second, emotions have previously been used as indicators for emotional development and mental health in demographically similar groups such as children (Guhn et al., 2020), and thus are appropriate for assessing adolescent mental health. And third, the use of emotions as indictors – including internalising symptoms (e.g. negative affect, anxiety) – of overall mental health has been shown to be relevant in predicting early-onset (6–14 years) mental health conditions (Thomson et al., 2019), which is precisely the proxy being inferred in the present study.
Methods
Sample
A nationally representative sample (in terms of region, age and sex) of 1500 Canadian adolescents was recruited through the Canadian market research firm Léger (Montreal, PQ, Canada), who reached out to families via their internal research panels. All participants were screened to ensure representativeness, with specific requirements denoting that each individual needed to: (1) be 9–17 years old, thus old enough to have some level of independent mobility but not old enough to have a full driver’s licence (which would alter environmental interactions); (2) be able to complete a survey in either English or French; (3) have obtained parental/guardian consent; and (4) have internet access via a mobile device or computer. Complete sample characteristics are presented in Table 1.
Sample demographics (n = 1500).
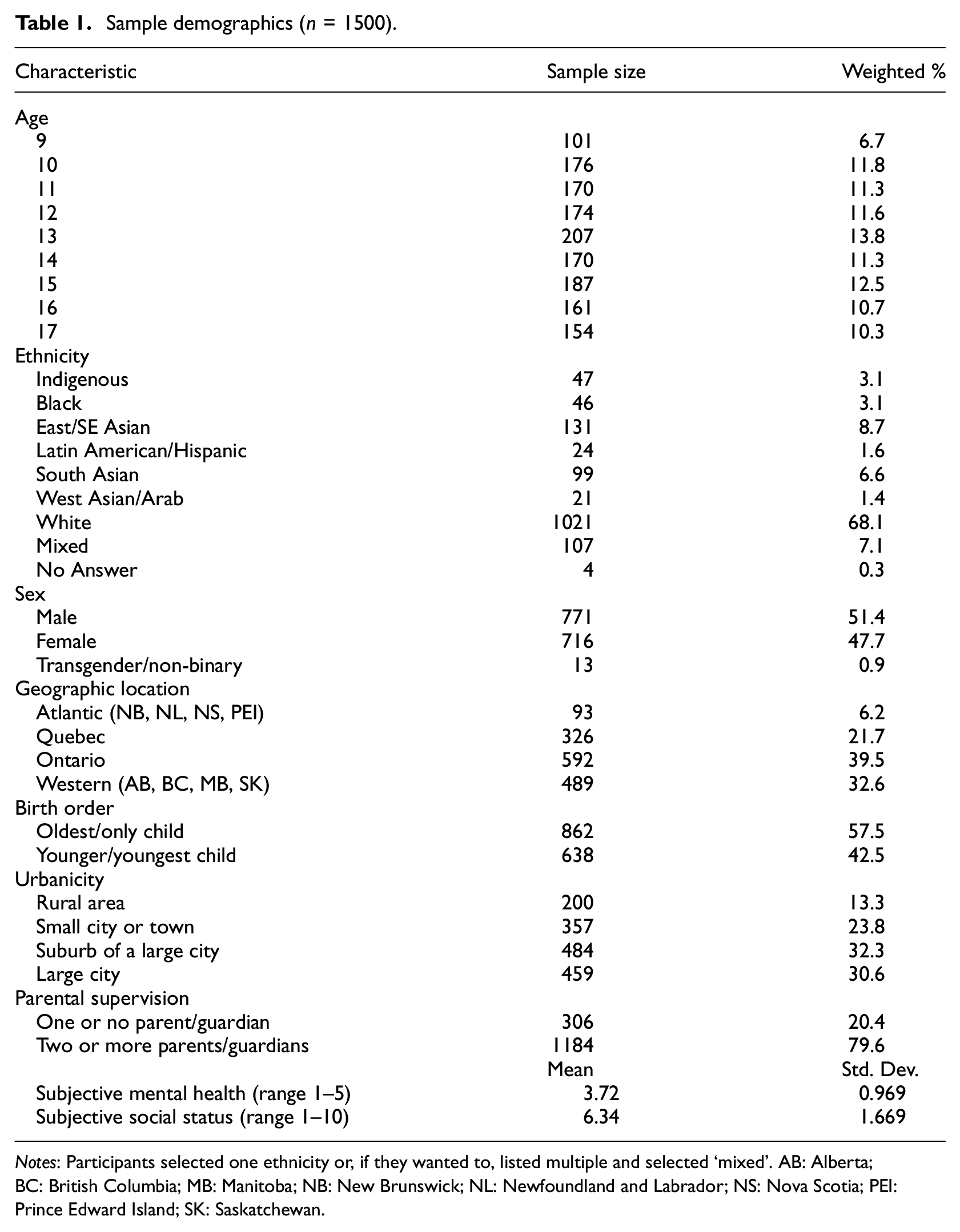
Notes: Participants selected one ethnicity or, if they wanted to, listed multiple and selected ‘mixed’. AB: Alberta; BC: British Columbia; MB: Manitoba; NB: New Brunswick; NL: Newfoundland and Labrador; NS: Nova Scotia; PEI: Prince Edward Island; SK: Saskatchewan.
Survey protocol
An online survey with a single-blind (i.e. participants unaware of research question) format was developed by the authors using Qualtrics, transferred to the Survey Research Centre at the University of Waterloo, Canada to undergo quality control (e.g. testing, Qualtrics programming) and then sent to Léger for distribution to participants for completion via either a mobile device (e.g. phone, tablet) or computer. Recruitment was undertaken by Léger, who identified and contacted participants using reputable Canadian online panels associated with the firm. Parents or guardians were first asked to provide consent for their child who, after providing their assent to participate, then began the survey. The survey featured 10–15-second panoramic videos (with sound, re-watch available) of six different urban areas, with each video being followed by a series of questions about emotional responses to the area in the video. Overall, the survey took participants an average of 20 minutes to complete. It was structured to mitigate different forms of bias. In particular, the survey randomised the presentation order of the videos for each participant to guard against order bias, and ensured anonymity and participant blindness to the research question of the study and true locations of the recorded settings to minimise potential sources of response bias. Concerning the completion rate of the surveys, during data collection Léger identified 74 drop-out or partially completed surveys for which new participants were recruited to the study. For their time in completing the survey, participants were remunerated via the firm’s internal point compensation programme that awards redeemable points to participants based on survey completion.
Decisions for the six urban areas used in this study were based on the research team’s intention to develop a cross-section of settings varying in PTOD score quality, urbanicity and setting type (i.e. natural vs built). In addition, areas were selected to reflect settings in which adolescents typically have daily interactions (i.e. commercial and residential spaces, not industrial areas), and to reflect both pedestrian- and auto-centric infrastructure systems. This approach was also implemented to minimise the potential influence of inter-rater grading variances that may emerge pertaining to the PTOD quality of different settings that were scored, and instead ensure that those spaces featured in the survey were genuinely disparate in their PTOD quality (i.e. not different as a result of a tool-scoring artefact). Ultimately, the six selected locations featured: two natural urban areas, two built urban areas higher in PTOD quality and two built suburban areas lower in PTOD quality (see Table 2).
Video settings’ design feature scores.
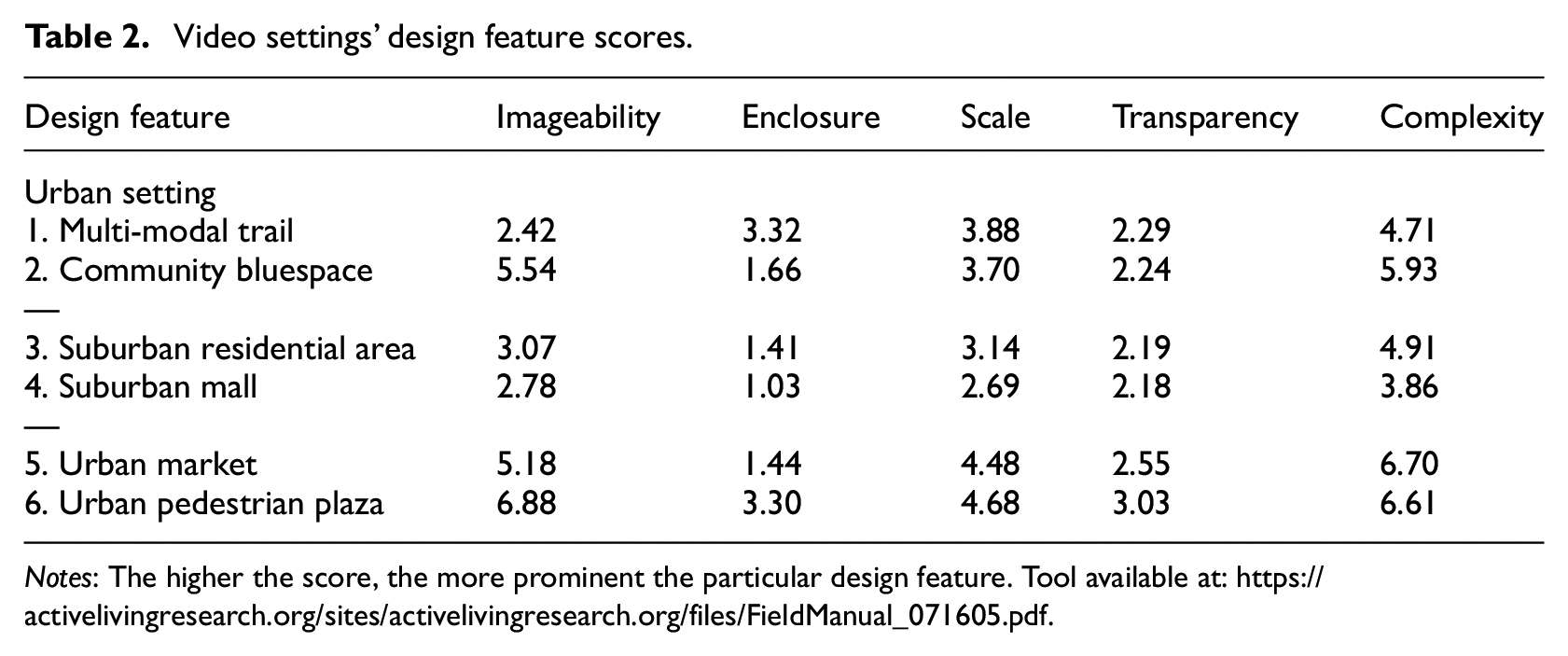
Notes: The higher the score, the more prominent the particular design feature. Tool available at: https://activelivingresearch.org/sites/activelivingresearch.org/files/FieldManual_071605.pdf.
Scoring of the locations filmed and presented in the survey was based on Ewing and Handy’s (2009) guide, and conducted using a validated tool (Clemente et al., 2005). Using the tool, the lead author and a trained PhD-level research assistant visited the six sites and, first, independently scored each of the five PTOD concepts. Next, the two raters compared their separate grades, which were not overly disparate and rather relatively consistent across the different designs, to develop a final set of mutually agreed-upon PTOD scores for each design across the six settings (full scoring tool available in Clemente et al., 2005). Recorded PTOD scores in this study ranged from approximately 1 to 7, with higher scores a greater prominence of a design concept in a given setting, and were similar to other studies investigating neighbourhood walkability (Hooi and Pojani, 2020), suggesting good tool reliability and true variability in urban design concepts. Locations featured existed in either Kitchener or Toronto, Ontario and comprised a multi-modal urban trail, urban bluespace (i.e. lake area), suburban residential street, suburban mall, urban pedestrian plaza and urban market area (see Supplemental Materials). This study was approved by the University of Waterloo’s Office of Research Ethics (study #43603).
Independent variable
The six different urban settings scored for PTOD quality in Table 2 were the independent variables in the analyses, and a dummy variable was created to indicate the presence of each setting in the mixed models.
Dependent variable
Six mental health outcomes reflecting different emotional responses were the dependent variables: positive affect, negative affect, calmness, anxiousness, perceived restorativeness and mental demand. In order to ensure the completion of the survey and to not exhaust participants, the number of items for each outcome variable scale was reduced from the original scales based on results from cognitive interviews and pilot testing of the survey instrument with three adolescents between the ages of 11 and 15. Positive and negative affect were measured using the five-point (1: very slightly or not at all; 5: extremely) Positive and Negative Affect Schedule for Children (PANAS-C) questionnaire (Ebesutani et al., 2012), which was adapted to present two positive affect items (e.g. ‘joyful’) and three negative affect items (e.g. ‘sad’). Calmness and anxiousness were measured using the five-point (1: not at all; 5: extremely) Profile of Mood States (POMS) (Grove and Prapavessis, 1992) ‘tension’ (e.g. ‘nervous’) subscale and an adapted ‘calmness’ (e.g. ‘peaceful’) subscale, which were adapted to two items each. Perceived restorativeness and mental demand were measured using the five-point (1: not at all; 5: extremely) Perceived Restorativeness Scale (PRS) Being Away subscale and Coherence subscale (Hartig et al., 1997), respectively. Both measures were adapted to contain three items each related to restorativeness (e.g. ‘it is a place to get away from it all’) and mental demand/fatigue (e.g. ‘there is too much going on’). Total outcome scores for measure were then aggregated to develop final score ranges between 2 and 10 for positive affect, calmness and anxiousness, and 3–15 for negative affect, perceived restorativeness and mental demand.
Covariates
Individual-level covariates included demographic data such as age (9–17 years old) and sex (male, female, non-binary) to account for the documented differences across these factors (Connolly et al., 2016; Patel et al., 2007), as well as self-identified ethnic identity (Aboriginal/Indigenous, Black, East/Southeast Asian, Latin America/Hispanic, South Asian, West Asian/Arab, White, Mixed, Other) (Fox et al., 2020). Overall subjective mental health well-being assessments were gathered using the five-point (1: poor; 5: excellent) single-item measure of self-rated mental health from the Canadian Community Health Survey (Government of Canada, 2015). Family and household factors were also compiled. Socioeconomic status (SES) information was collected using a subjective social status (SSS) measure (Amir et al., 2019) based on the MacArthur Scale of SSS, a validated cross-culture measure of social status (Goodman et al., 2001). As a part of the question, the measure presented an illustration of a ladder and asked participants to compare their family’s money, education and jobs to Canadian society by ranking their standing on the ladder between 1 and 10 for each category; these scores were later summed to create an aggregate SSS score. Parental supervision (one or no parent/guardian, two or more parents/guardians) was collected to account for parental controls which can impact an adolescent’s interactions with their local environments (Alparone and Pacilli, 2012; Foster et al., 2014). There is some evidence of associations between birth order and individual social attitudes (Salmon, 2003), and social behaviours (Courtiol et al., 2009), thus to control for parental resource devotion across these groups (Booth and Kee, 2009) we included a birth order (oldest/only child, younger sibling) variable. Broader environment-level covariates included region (Maritimes [Newfoundland and Labrador, Prince Edward Island, Nova Scotia, New Brunswick], Quebec, Ontario and Western Canada [Manitoba, Saskatchewan, Alberta, British Columbia]). Finally, urbanicity was gathered using an adapted and abbreviated version of a PEW Research Center measure (Miller et al., 2012) which asked ‘What type of community do you live in?’ (rural area, small city or town, suburb of a large city, large city).
Analyses
Analyses of the impacts of the six urban settings on the six emotional response outcomes of adolescents were conducted via a series of linear mixed models (LMMs). LMMs were selected due to their appropriateness for analysing data that are nested, thus not assumed to be independent, as is the case for the outcome variables of this study (since each participant reported their mental health responses for each setting). Clustered responses like this potentially introduce additional correlation and consequently cause the standard errors to be underestimated if not accounted for in the analysis (increases probability of Type 1 error). Mixed models correct for clustered data by accounting for both fixed and random effects. Fixed effects are assumed to remain constant across clusters and have a fixed effect on the outcome of interest, while random effects vary in effect on the outcome across clusters and are not assumed to be constant. In the present study, LMMs allowed the analysis to account for repeated measures on the same individual, which are not independent, by specifying the random effect (unique participant ID) and fixed effects (covariates) at the individual level. Overall, 36 LMMs were run: one for each combination of setting and affective response outcomes. Both unadjusted models and adjusted models controlling for the theoretically relevant covariates noted above were run for each set of analyses. All analyses were run in SPSS Statistics version 25 (IBM Canada Ltd., Markham, Ontario, Canada).
Results
Full results of the unadjusted and adjusted LMMs for the six different urban settings and the six mental health outcomes are shown in Table 3. Findings from the unadjusted models outline significant positive associations between the natural settings (i.e. trail, bluespace) and all three salubrious mental health outcomes, the most exceptional being perceived restorativeness (trail: β = 3.106, 95% CI: 2.934, 3.278; bluespace: β = 3.498, 95% CI: 3.330, 3.666). The suburban mall setting (the lowest scored PTOD area) was consistently associated with the most significant deleterious mental health responses across all six outcomes. Notably, the setting was associated with significant decreases in calmness (β =−1.954, 95% CI: −2.066, −1.842), almost a full point lower than the setting with the next lowest score (urban market), and perceived restorativeness (β =−2.848, 95% CI: −3.022, −2.674), also roughly a full point lower than the setting with the next lowest score (suburban street). Contrarily, the highest scored built setting (i.e. a setting that is not the trail or bluespace), the urban plaza, was the only built setting to be significantly associated with an increase in positive affect (β = 0.116, 95% CI: 0.010, 0.222), and featured a relatively minimal (but significant) decrease in perceived restorativeness (β =−0.358, 95% CI: −0.544, −0.173), and a nonsignificant decrease in negative affect (β =−0.040, 95% CI: −0.113, 0.032).
Unadjusted and adjusted linear mixed models of urban environments and adolescent mental health outcomes.
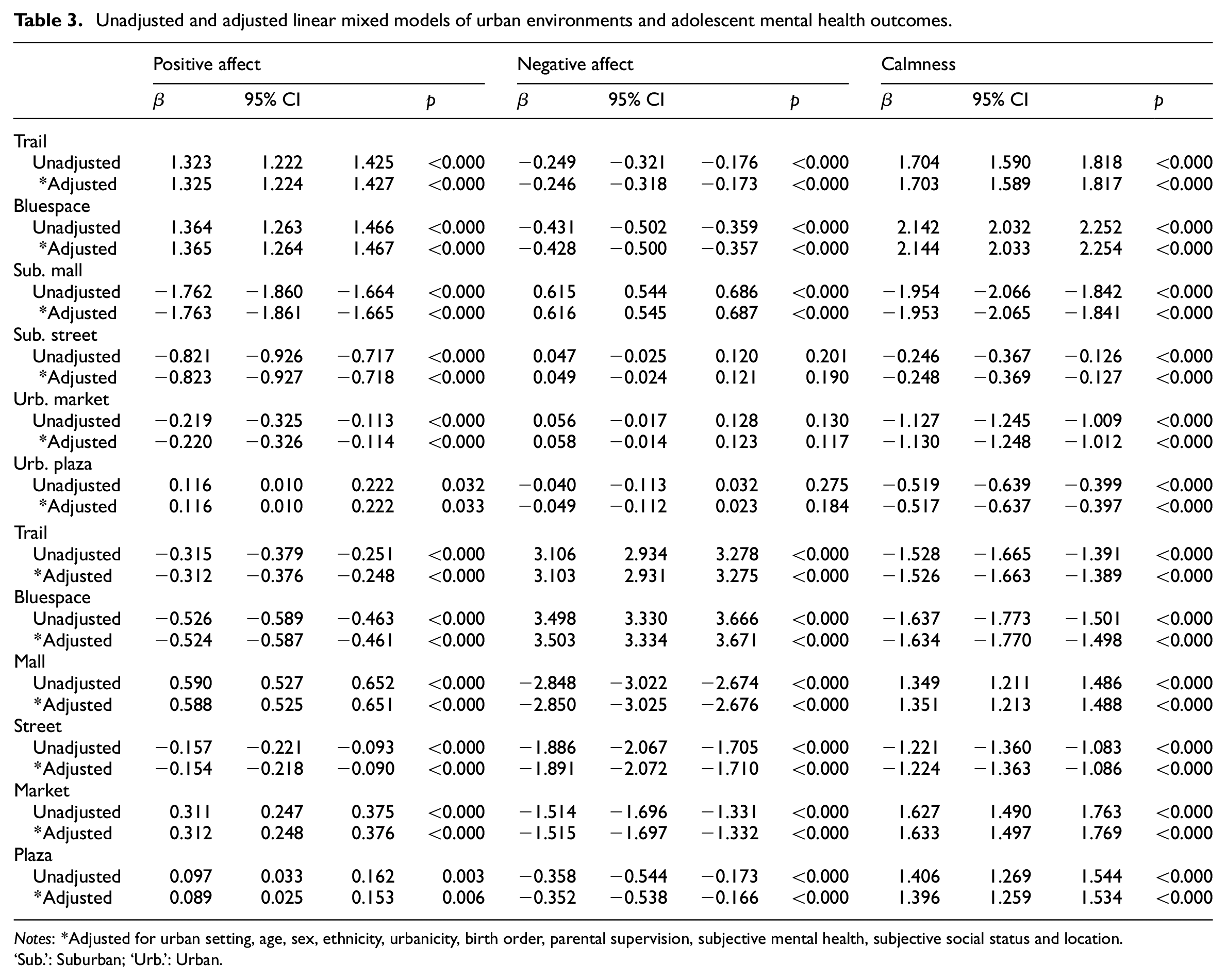
Notes: *Adjusted for urban setting, age, sex, ethnicity, urbanicity, birth order, parental supervision, subjective mental health, subjective social status and location. ‘Sub.’: Suburban; ‘Urb.’: Urban.
Trends observed in the unadjusted models were essentially the same even after including the covariates in the adjusted models. Noteworthy results include all four built settings remaining significantly linked to reductions in calmness, including the comparatively highly PTOD-scored urban plaza (β =−0.517, 95% CI: −0.637, −0.397), and the suburban mall area staying as the only setting linked to a significant increase in reported negative affect (β = 0.616, 95% CI: 0.545, 0.687). Even after being adjusted for several covariates, the relatively low-scored suburban residential street area was significantly associated, albeit modestly, with reductions in anxiousness (β =−0.154, 95% CI: −0.221, −0.093), as well as mental demand (β =−1.351, 95% CI: −1.213, −1.488), representing the only built setting to feature these directional relationships. Between the two natural urban areas, noticeable differences in reported increases of calmness (trail: β = 1.703, 95% CI: 1.598, 1.817; bluespace: β = 2.144, 95% CI: 2.033, 2.254), and decreases in negative affect (trail: β =−0.246, 95% CI: −0.318, −0.173; bluespace: β =−0.428, 95% CI: −0.500, −0.357) and anxiousness (trail: β =−0.312, 95% CI: −0.376, −0.248; bluespace: β =−0.524, 95% CI: −0.587, −0.461) also remained in the adjusted models.
Discussion
Using an online survey with a nationally representative sample of Canadian adolescents, this study investigated the relationships between the aggregate PTOD quality of public spaces and adolescent mental health by examining how distinctly scored urban settings affected self-reports of positive affect, negative affect, calmness, anxiousness, perceived restorativeness and mental demand. Overall, the findings delineate clear trends across the differently scored PTOD settings with respect to their impacts on the self-reported emotional responses of adolescents. Taken together, these results suggest that the PTOD quality of public urban areas may have significant impacts on the mental health of this demographic, and that certain urban design–context combinations may represent ‘restorative niches’ relevant to adolescent mental health. To further contextualise these results and identify potential emotional affordances related to high-quality PTOD public places, we turn to the ToA and the PTOD scores outlined in Table 2 to interpret the findings.
Trends across the four built urban environments generally suggest that as the aggregate PTOD quality worsens, reports of positive emotional responses become lower while reports of negative responses become more common. Such results support broader notions that pedestrian features in urban areas are beneficial for adolescents. For example, several studies have observed that increased levels of physical activity (e.g., active travel) are associated with sidewalk presence (Rothman et al., 2018), narrower street width (Nasar et al., 2015) and street connectivity (Giles-Corti et al., 2011). The trends observed in our results appear more marked, however, when comparing the two lowest scored PTOD areas (suburban mall, suburban street) to the two other built areas (urban market, urban plaza). In particular, the former are associated with considerably larger decreases in positive affect (as seen in the coefficients presented in Table 3: −1.7, −0.8 vs −0.2, 0.1) and perceived restorativeness (Table 3 coefficients: −2.8, −1.9 vs −1.5, −0.4), while the suburban mall is also the only area significantly associated with an increase in negative affect. Situating these results within our theoretical frame, it may be that higher PTOD presents adolescents with a greater number of environmental features (e.g. places to sit/socialise, active uses) that they can make use of, and/or which encourage more cheerful (positive affect) and less-demanding (restorativeness) and upsetting (negative affect) experiences. Alternatively, poor overall PTOD quality may be an indicator of fewer social and emotional affordances (i.e. opportunities to socially or emotionally engage with a space) which can motivate place usage (Knöll and Roe, 2017), consequently resulting in reports of more negative emotions. Given the exploratory nature of these findings, however, future research should seek to replicate similar protocols in real-world settings to triangulate results or use objective methods (e.g. Buttazzoni et al., 2021) to further explore these relationships.
Expanding the theoretical discussion above, insights into the relative importance of PTOD quality in built spaces may be gleaned by further examining differences in potential design-related affordances across the two poorest-scored (suburban mall, suburban street) and highest-scored (urban plaza, urban market) built environments as these affordances relate to the considerable gap in scores regarding scale, imageability and complexity (Table 2). Noting the emotional response trends observed in the findings, it may be that the combination of these designs in a public setting potentially reflects spaces that contain more emotional richness (i.e. variety, density of affordances), consequently indicating such design quality is, in effect, perceived by adolescents as possessing greater environmental extent (i.e. sense of connectedness to a larger whole) and compatibility (i.e. good fit between an environment and one’s intentions, needs) (Knöll and Roe, 2017). More pointedly, this potential relationship may be a result of the more ‘pedestrianised’ urban spaces in this study affording, for example, greater visual distinctiveness and aesthetic appeal (complexity, imageability) via designs that incorporate contours or curvature (Vartanian et al., 2013) and other naturalistic patterns (e.g. tree-like structures) (Coburn et al., 2019). Another potential explanation is that the increased presence of streetscape features like street trees (scale) has been associated with the potential to reduce annoyance (Sarajevs, 2011), while sidewalk features like the presence of vegetated ground (scale) have been linked with more comfortable pedestrian area conditions (Kim et al., 2018). To better understand how specific PTOD features relate to youth mental health, future research could seek to conduct online studies featuring graduated photomontage techniques that use photo manipulation to increase the presence of specific designs or design combinations while simultaneously holding the larger setting constant (e.g. Wang et al., 2019).
Natural urban environments in this study (trail, bluespace), although scoring lower in certain PTOD categories relative to some of the built settings, were associated with the most substantial positive mental health outcomes and minimal negative mental health experiences. Taking the significant associations between the aggregate PTOD quality of these spaces and the perceived restorativeness responses among adolescents in the present study along with similar findings between older people and urban green environments (Neale et al., 2020), these similar trends together might suggest that exposure and/or interaction with more ‘pedestrianised’ natural urban spaces could have mental health benefits across the lifespan. It might be that such aggregate environmental quality combined with naturalistic elements in design has some level of universality as positive design-related emotional affordances. More specifically, while natural environments have previously been linked to a variety of mental and cognitive benefits (e.g. Amoly et al., 2014; Dadvand et al., 2015), a comparison of the two natural settings examined here illuminates some potentially noteworthy design-related emotional affordances or ‘restorative niches’ for adolescents. Contextualising these findings with respect to Table 2, the combination of comparatively higher imageability and complexity quality in the bluespace, relative to the trail, may be central to the roughly half-point (∼0.40) increase observed in calmness and restorativeness.
Considering the nature of this combined design exposure with respect to the ToA and potential social and emotional affordances, the findings of the present study might indicate that more natural pedestrianised urban spaces (e.g. via high levels of imageability – presence of a local lake, community gardens; complexity – more colours or designs, public art) represent therapeutic or calming design-oriented restorative niches. More precisely, as these designs ostensibly elicit calmness, they may be indicative of urban designs which function as emotional affordances that support experiences of bottom-up attention – which is associated with involuntary attention (Itti, 2006) as opposed to demanding top-down directed attention associated with excitement (Martínez-Soto et al., 2013) – for adolescents. Whether these relationships are principally due to perceptual (e.g. design or colour attraction) or physical (e.g. a greater number of environmental features to engage with) factors is beyond the scope of this analysis; however, such lines of inquiry are warranted in future study. Irrespective of the source, these theoretical relationships appear to be consistent with related research that has noted that higher-quality environmental aesthetics can positively impact active travel (Sun et al., 2018), while vegetation richness can increase aesthetic preference (Zhuang et al., 2021), and imageability features (e.g. flowers, water sources) can enhance a setting’s restorative potential (Wang et al., 2019).
Implications for practitioners
The results of this study illustrate several connections between the level of PTOD quality in an urban setting and the emotional responses of adolescents, and consequently have implications for professional practice. They suggest that natural spaces that exemplify PTOD features, specifically in the form of imageability (i.e. more distinctiveness) and complexity (i.e. more visual richness), may be key design concepts for planners and urban designers to consider. Examples of such designs include, but are not limited to, gardens/flower arrangements or building facades with more diverse colour palettes, distinctive public art displays, notable built landmarks or buildings with rounded edges (i.e. non-rectangular buildings) and detailed building/structure ornamentation. Alternatively, granted that restorative opportunities among young people have previously been suggested to be linked to an age-specific developmental need for exploration and adventure (Roe and Aspinall, 2012), urban planners may also seek to apply these ideas (e.g. higher aggregate levels of imageability, complexity or scale) when designing parks, trails or other recreational spaces to support experiences of bottom-up attention. More broadly, the results of this study would advise planning practitioners and other urban designers to consider scale in their community’s relevant design guidelines. For instance, practitioners could evaluate relevant policies to assess their potential to implement street trees, sidewalk barriers or street/plaza planters next to thoroughfares or arterial roads; to evaluate the extent to which local policies allow for the pairing of active travel infrastructure (e.g. bicycle racks, benches, wayfinding signs) with other public transit networks and infrastructure (e.g. bus/LRT stops); or, more broadly, to examine how their residential development codes specifically protect individuals from traffic and its attendant impacts.
Limitations
When interpreting the results of this study, there are several limitations to be aware of. Most notably, the development of the survey required reducing the number of items from the validated scales we used to develop outcome variables for feasibility considerations. Consequently, this may have resulted in smaller variation in outcome variables, which would logically lead to smaller coefficients in our results and an increased chance of a type II error (failure to reject a null hypothesis that is actually false). However, the majority of our models found statistically significant associations between various PTOD concepts and survey outcomes. Therefore, while type II errors do not seem to have been a major problem, it is still possible that this limitation resulted in smaller effect sizes than would have been found with a larger variation in outcome variables. The delivery method of the survey – an online format – may have also contributed to an underestimation of the true effects of the urban settings on adolescent mental health. While the videos that participants watched were 360° and included audio of the settings, participants were not physically exposed to environmental conditions such as wind, nor were they able to accurately consider vestibular (i.e. balance and movement in reference to space) or kinesthetic (i.e. bodily sense) inputs with respect to the different settings. Moreover, the videos shown of the different settings also featured, to varying extents, the presence of pedestrians (e.g. urban plaza compared to the residential street); this phenomenon may have resulted in confounding the perceptions of area safety and accessibility (Burden et al., 2013) among participants. This survey also exclusively used video examples of urban settings from the Canadian context, and any generalisations of these results to other contexts with distinctly different urban environments should be made cautiously. Survey questions were also structured to inquire about the present-moment emotions of adolescents in response to the different videos; however, certain potential confounds may have affected responses, namely latent place preferences (e.g. preferences for natural areas relative to built areas). Finally, the research conducted here is cross-sectional in nature, thus it is not possible to speculate about causality. That said, the study design (observations nested within individuals), the large sample size (n = 1500) and the representativeness of the sample in terms of region, sex and age were all strengths of the research, and appropriate considering the lack of extant research on this topic.
Conclusion
To examine the impact of specific urban designs on adolescent mental health, we scored and videotaped six different settings and conducted an online survey with 1500 Canadian adolescents. Findings suggest that the PTOD quality of urban areas are significantly associated with emotional responses of adolescents, positively in the case of higher-quality areas and negatively in poorer-quality areas. Future study should look to conduct similar studies in real-world settings with objective measures to compare results, as well as further examine the role and impacts of imageability and complexity in natural urban areas.
Footnotes
Acknowledgements
First, we would like to thank Beth McLay and Arianne Manary of the University of Waterloo Survey Research Centre for all of their assistance in the development and programming of the online survey. Second, we would also like to thank the Canadian Institutes of Health Research for funding this study (CIHR Grant #175348). Likewise, we would like to thank all of our community partners in the City of Kitchener, Park People, 8 80 Cities and Student Transportation Services of Waterloo Region for their collaboration on this research. AB would also like to thank Bridget Irwin of the Windsor-Essex County Health Unit for her assistance with the analysis of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Canadian Institutes of Health Research provided funding for this study (CIHR Grant #175348).