
Abstract
Daily mobility has been shown to contribute to the wellbeing of older adults, as it promotes healthy and independent living. However, very little is known about how the complex relationships between locations, geographic environments and daily mobility relate to wellbeing. In the current paper, we rely on the concept of ‘motility’– defined as potential mobility– and the concept of ‘movement’– defined as actual mobility– to take a step forwards in disentangling the relationship between mobility and wellbeing. We further examine how both motility and movement relate to two complementary definitions of wellbeing: hedonic wellbeing as a measurement of happiness, and eudaimonic wellbeing as the actualisation of an individual’s human potential. To investigate this relationship, we draw up a conceptual framework stressing pathways linking mobility to wellbeing, which we empirically test using structural equation modelling on a stratified sample of 470 older adults. We first quantitatively confirm that motility is defined by access, competences, appropriation and attitudes to modes of transportation. We then observe that motility has direct effects on eudaimonic wellbeing and, to a lesser extent, on hedonic wellbeing. Part of the motility effects on wellbeing are mediated by movement. Separating mobility into motility and movement stresses the independent and complementary role that potential and realised mobility play in shaping older adults’ wellbeing.
Introduction
Policymakers and academics are increasingly paying attention to linking mobility and the built environment to improve urban sustainability and health (e.g. Diener et al., 2009; Lowe et al., 2015; Rydin et al., 2012). This renewed interest in making cities healthy and pleasant places leads to considering wellbeing and a good quality of life as important outcomes of planning policies (e.g. Cloutier et al., 2014). For example, the Organisation for Economic Cooperation and Development (OECD) recently aimed to redefine the growth narrative to put people’s wellbeing at the centre of governments’ efforts (OECD, 2016). Wellbeing is also core to the notion of health (Diener et al., 1999), since high levels of life satisfaction and a good mood are beneficial to physical health (Diener and Chan, 2011). The Constitution of the World Health Organization (WHO) defines health as ‘a state of complete physical, mental and social wellbeing and not merely the absence of disease or infirmity’ (WHO, 1946). New measurements have emerged, such as the ‘Gross National Happiness’ index, which integrates housing conditions, wealth, social participation, education and health (Kahneman and Krueger, 2006).
Mobility is not directly part of such indicators, though it is recognised as playing a key role in wellbeing (e.g. Banister and Bowling, 2004). Mobility is linked to the ability to conduct activities and participate in society (e.g. van den Berg et al., 2011), maintain physical independence (e.g. Michael et al., 2006), promote social relations (e.g. Ettema et al., 2010) and avoid social exclusion (e.g. Lucas, 2012). Some population categories, such as older adults, can suffer physically and mentally when their mobility is precarious (Hanson, 2009), and since the proportion of older adults is growing in most Western countries, healthy ageing is a major public health concern (Pan et al., 2018). Compared with other population segments, older adults present fewer mobility needs related to employment or childcare, but face growing physical or cognitive obstacles to mobility that can limit their wellbeing. However, very little is known about how wellbeing interacts with geographic environments and daily mobility. Measuring the relationship between daily mobility and wellbeing, as well as the determinants of mobility among older adults, is therefore important for assessing health outcomes and improving the built environment or social services (Haustein and Sirén, 2015).
With the ‘mobility turn’ (Sheller and Urry, 2006), geographers have recognised the importance of the movement of people, things, ideas and information. In particular, several authors have reconsidered the notion of daily mobility by distinguishing two aspects: movement per se and motility, that is, the mobility potential or capital (Kaufmann et al., 2004). While the concept of motility has been refined over the last decade, quantitative measurements remain scarce and incomplete (e.g. Kaufmann et al., 2018). Kaufmann and colleagues conducted a quantitative operationalisation of motility in the case of commuting. They came up with a typology of motility that relates to an aggregate living environment (NUTS2 scale). In the current paper, we investigate how mobility influences wellbeing in the specific case of older adults, while controlling for micro-environmental conditions. We are also theoretically driven, and attempt to separate the notion of mobility into measurements of motility (potential) and movement (actual), and to assess how these two dimensions relate to wellbeing.
The paper is organised as follows: the following section reviews theories and definitions of wellbeing and mobility, and derives a conceptual framework of their relationships. In the next section, this conceptual framework is tested using Structural Equation Modelling (SEM). Results are presented in the penultimate section, and methodological implications for future research are discussed in the final section.
Framing mobility and wellbeing
Mobility and wellbeing are large and fuzzy concepts that are difficult to synthesise (Nordbakke and Schwanen, 2015). Here we focus only on the components of mobility and wellbeing that relate to urban dimensions, which planners can potentially activate to improve healthy ageing.
Mobility: Movement and motility
Mobility refers to the physical movement of individuals to experience the world in time and space. Cresswell (2006) suggests separating the representations and experiences from the material corporeality of mobility. Kaufmann (2001) was the first to distinguish explicitly movement (i.e. the observed mobility) from motility (i.e. the potential for mobility).
The concept of movement is defined temporally (start time, end time and duration), spatially (point of origin, geographical path and point of destination) and with complementary descriptors such as the mode of transportation. This is in line with traditional trip-based approaches in transport. Departing from trip-based views, time geography (e.g. Hägerstrand, 1970) emphasises the role of the activity space (Golledge and Stimson, 1987), that is, the set of places experienced by an individual over a certain period of time. A movement is then the result of the need to link two consecutive activities, separated in space and time (Enaux, 2009). Ellipses are traditionally used to represent activity spaces, after weighting locations by the time spent or the frequency of visits (e.g. Perchoux et al., 2014).
The concept of motility is rooted in biology, and describes the capability of living organisms to move. Kaufmann (2001) and colleagues imported the concept into sociology, and consider that each individual has a potential for mobility, which can be converted into movement depending on wishes and circumstances. In short, motility can be described as the capability of someone to be mobile across space, either physically or virtually (information exchange) (Kellerman, 2012). This capability is thus the key factor determining mobility. Kaufmann and colleagues (2004) define motility using three notions: access, competences and appropriation. First, access is formed by the geographical context and the accessibility to means of transportation. It includes transport and communications to reach services and equipment in a specific amount of time, as well as the attributes of these transportation means (e.g. public transport schedules, cost, disabled access, etc.). Second, competences refer to acquired skills (e.g. driving licence, using the internet to quickly access information about transport available at specific locations and destinations), organisational capabilities (e.g. scheduling of activities and trips) and experiences. Third, appropriation refers to habits, preferences (e.g. Kaufmann et al., 2003), perceptions, representations, values and strategies thereof (Schwanen and Lucas, 2011). There is no consensus regarding the role of attitudes towards different transport modes and motility. While Kaufmann and colleagues (2004) discuss and implicitly integrate attitudes and appropriation under a larger terminology related to perception, Kjaerulff (2011) further suggests that attitudes are explicitly part of appropriation. Attitudes are proven to be useful to predict mode choice (e.g. Kroesen et al., 2017). For example, Steg and colleagues (2001) show that people, and more specifically older adults, evaluate the car as attractive because of the comfort, safety, flexibility, availability and independence provided.
While calls have been made to construct quantitative measurements of motility (e.g. De Witte et al., 2013), very few studies to date have attempted to measure its three constituents (Kaufmann et al., 2010, 2018; Viry, 2011; Witter, 2012). Here, we propose a quantitative assessment of motility within a broader model linking mobility and wellbeing. In addition, we examine the role of attitudes within the motility concept, in order to see whether it complements these three main constituents.
Wellbeing: The eudaimonic and hedonic dimensions
Wellbeing is a relative and dynamic notion, socially and culturally constructed, that takes different meanings depending on disciplines. Physicians, epidemiologists, psychologists, economists, sociologists and geographers have used different interpretations of wellbeing, often complementary, yet sometimes contradictory (Nordbakke and Schwanen, 2015). From a geographic perspective, wellbeing emerges from the interactions between individuals and space, and is thus continuously refined along social interactions (e.g. Fleuret and Atkinson, 2007).
Nordbakke and Schwanen (2015) suggest that wellbeing can be described using three distinctive pairs of approaches. First, an objective and a subjective approach to wellbeing can be distinguished. Accordingly, ‘the subjective stance holds that an individual’s perceptions and experiences are the foundation for evaluations of how well s/he lives’ while, in the objective stance, ‘wellbeing is established from the evaluation of the objective circumstances in which people live’ (Nordbakke and Schwanen, 2015: 107). The two approaches are complementary, and defined irrespective of the type of metrics they use: subjective/objective wellbeing can be measured with objective/subjective criteria and vice versa.
Second, universalists conceptualise wellbeing as independent of time and place, while contextualists stress the dependence of wellbeing on culture and geographical context (Schwanen and Atkinson, 2015).
Third, and most importantly for the present study, one distinguishes hedonic wellbeing (HWB) from eudaimonic wellbeing (EWB). In the hedonic perspective, wellbeing is based on the concept of utility as a measurement of pleasure, satisfaction or happiness; that is the so-called subjective (hedonic) wellbeing (Kahneman et al., 1999). More specifically, HWB is made up of cognitive components (e.g. life satisfaction) and affective components (positive or negative emotions) (e.g. Friman et al., 2017). In the eudaimonic perspective, what matters is the actualisation by an individual of her or his human potential (i.e., self-actualisation). It is reached through self-realisation and acting in accordance with one’s own objectives (Waterman, 1993). Unlike the first two pairs of definitions, the hedonic and eudaimonic views of wellbeing are not strictly opposed. The two stances may overlap and share common attributes, such as depressive status (Ryan and Deci, 2001).
We rely on the complementarity of subjective and eudaimonic approaches (e.g. Henderson et al., 2014), and take the standpoint of contextualists, especially because we consider the geographical context explicitly – at a micro scale – in the analysis. In line with most recent empirical studies, we aim to simultaneously assess the hedonic and eudaimonic dimensions of wellbeing.
Linking mobility and wellbeing for older adults
Our aim is to assess how mobility – and more particularly motility and movement – influences the hedonic and eudaimonic components of wellbeing among older adults. Mokhtarian and colleagues (2015) and De Vos and colleagues (2013) show that travel behaviour, and more specifically movement, affect wellbeing in a number of ways.
Experiences during destination-oriented travel
The time spent on the move is filled with positive or negative experiences and feelings, for example related to comfort (or discomfort), which, in the case of older adults, is related to health conditions.
Activities enabled by travel
Mobility is fundamental to engaging in activities that satisfy social and physical needs. Schwanen and Wang (2014) also show that leisure activities conducted outside the home induce more wellbeing than mandatory activities or those carried out at home. In that respect, while older adults may have more time opportunities for leisure, they may also be more constrained to home activities depending on their physical capacities.
Activities during destination-oriented travel
Planned and unplanned activities during travel affect the travel experience. Being accompanied, for instance, allows older adults to engage in small talk, turning travel into social interactions.
Where travel is the activity
Travelling is not always a derived demand; going outside to enjoy nature, recreational walking or cycling contribute to wellbeing by generating positive emotions (Gatrell, 2011). Recreational travel can partially be limited by ageing.
While reduced movement is generally associated with reduced wellbeing, engaging in few trips or having a restricted activity space do not necessarily mean isolation, confinement or loneliness (Lord et al., 2009). An activity space can be voluntarily limited to the residential neighbourhood while judged sufficient to keep a certain level of physical activity or meet commercial needs (Vallée et al., 2015).
In addition to these four links between movement and wellbeing, we can also assume that motility influences wellbeing.
Motility as a precondition to movement
Motility predicts happiness, self-realisation and wellbeing directly, and indirectly through movement.
Motility as a trigger to rewarding activities
Greater access, and shorter travel or waiting times result in more opportunities to engage in rewarding activities (De Vos et al., 2013).
Motility as a vector of independency
Motility allows people to have more independent living by providing them with increased control over the places and times in which activities can be carried out (Ziegler and Schwanen, 2011).
Conceptual framework
From the aforementioned assumptions, we built the theoretical framework of Figure 1 to disentangle the relationships between mobility, wellbeing and their respective components for older adults. While previous research has analysed the link between mobility and wellbeing (Figure 1, grey box), our framework identifies potential pathways between motility (i.e. mobility potential), movement (i.e. observed mobility) and wellbeing. We particularly assume that motility influences wellbeing directly and/or via movement. Movement has been broken down into ‘time movement’ and ‘space movement’, assuming ceteris paribus that a larger activity space increases wellbeing, while a greater amount of time spent on travel decreases wellbeing (Stutzer and Frey, 2008). We also examine the role of attitudes towards transport, especially whether attitudes should be integrated into one of the three other components of motility or be separated as a fourth component. Lastly, we test the existence of motility and wellbeing as separate and second-order constructs (bold circles in Figure 1). These hypotheses are tested with a Structural Equation Model (SEM) for a case study in Luxembourg.
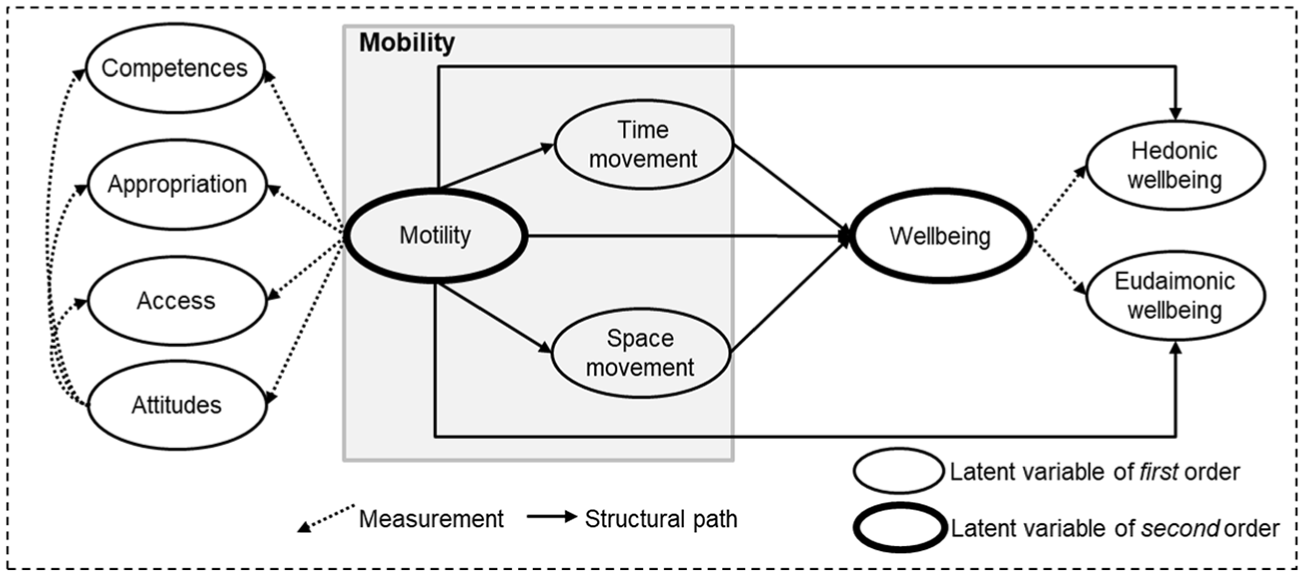
Conceptual framework.
Material and methods
Methodological framework
Our conceptual framework (Figure 1) has a large number of formal links to be explored. Hence, we opted for a Confirmatory Factory Analysis (CFA) followed by the estimation of a covariance-based Structural Equation Model (SEM) where direct and indirect pathways are estimated. The SEM comprises two parts: a measurement model and a structural model. First, the measurement model relates a set of measured and observable variables to an unobservable (latent) variable. The choice of indicators was prompted by theory and empirical literature. We created the latent variables using CFA and the Cronbach’s alpha coefficient for congruence of the indicators (Hoyle, 2014). The structural model then draws explicit links between the various latent variables, thus testing our hypotheses. This combination of methods is frequently used to test if a set of indicators reflects a theoretical construct (e.g. Anderson and Gerbing, 1988). In our case, it applies to both motility and wellbeing.
We used the Maximum Likelihood Estimator (MLM) in the lavaan R software package (version 0.5-23) (Rosseel, 2012) with robust standard errors and Satorra and Bentler (1994) scaled test statistic to account for non-normality in our observed variables (Hoyle, 2014). The MLM estimator outperforms the Weighted Least Squares Means and Variance Adjusted (WLSMV) estimator in case of binary variables and small sample size (n < 1000) (Golob, 2003; Hoyle, 2014), which is the case here.
Data and case study
This study is part of the CURHA (Contrasting URban contexts in Healthy Aging) project (Kestens et al., 2016). Data collection was conducted between April 2015 and January 2016 in Luxembourg among 471 individuals older than 65 years. The sample was spatially stratified into five areas, in line with the degrees and types of urbanity. The total area (see the supplementary material S1, available online) covers 80% of the country’s population (the northern areas being scarcely urbanised). Luxembourg City is the capital and main attraction centre, and Esch-sur-Alzette the second urban centre. Esch-sur-Alzette and the southern areas are heavily industrialised and have specific demographic and urbanisation settings that needed to be considered in the sampling. In addition to spatial aspects, age and gender were also accounted for. For cost-effectiveness, the sample remains small and the sampling aimed to ensure sufficient coverage of each spatial and age/gender class, rather than maximising representativeness to the entire population (see Kestens et al., 2016, for details). However, overall, the sample is a relatively good representation of the population of older adults in Luxembourg.
After cleaning for missing data for some particular variables of interest, the research reported here relies on 448 records. About half of the participants are female (N = 221) and about half are aged between 65 and 75 years (N = 227). Relative to the census population (Statec, 2014), the sample thus slightly underrepresents females (53% in the census) and overrepresents the over 75s among the older population (47% in the census), yet the latter is underrepresented for females. Given these limitations in terms of representativeness, we do not infer in the discussion that our results can be extrapolated to the entire Luxembourg population.
The attributes used in our analyses are derived from various sources and Geographic Information System (GIS) processing. Individuals’ attributes were taken from a face-to-face survey (LuxCohort), which includes 204 questions about individual and household characteristics, health, activities, mobility and perceived residential neighbourhood attributes. Regular activity places were geolocated from an interactive mapping process, VERITAS (Visualization and Evaluation of Route Itineraries, Travel destinations and Activity Spaces) (e.g. Perchoux et al., 2016). Participants were monitored over seven consecutive days with a GPS. Lastly, accessibility indicators were geocomputed, based on OpenStreetMap and open data from the Ministry of Sustainable Development in Luxembourg. Environmental variables were computed around residential places using 10 or 20 minutes walking buffers along the street network. All questionnaire items used in the study are detailed in the supplementary material (S2, available online).
Definition of observed and latent variables
Observable variables are selected to represent latent variables (Figure 1). The first-order latent variables representing motility are competences, appropriation, access and attitudes; and the first-order latent variables representing wellbeing are HWB and EWB. Descriptive statistics for all the observable data used in the model are provided in Table 1.
Definition of the variables used and descriptive statistics (N = 448).
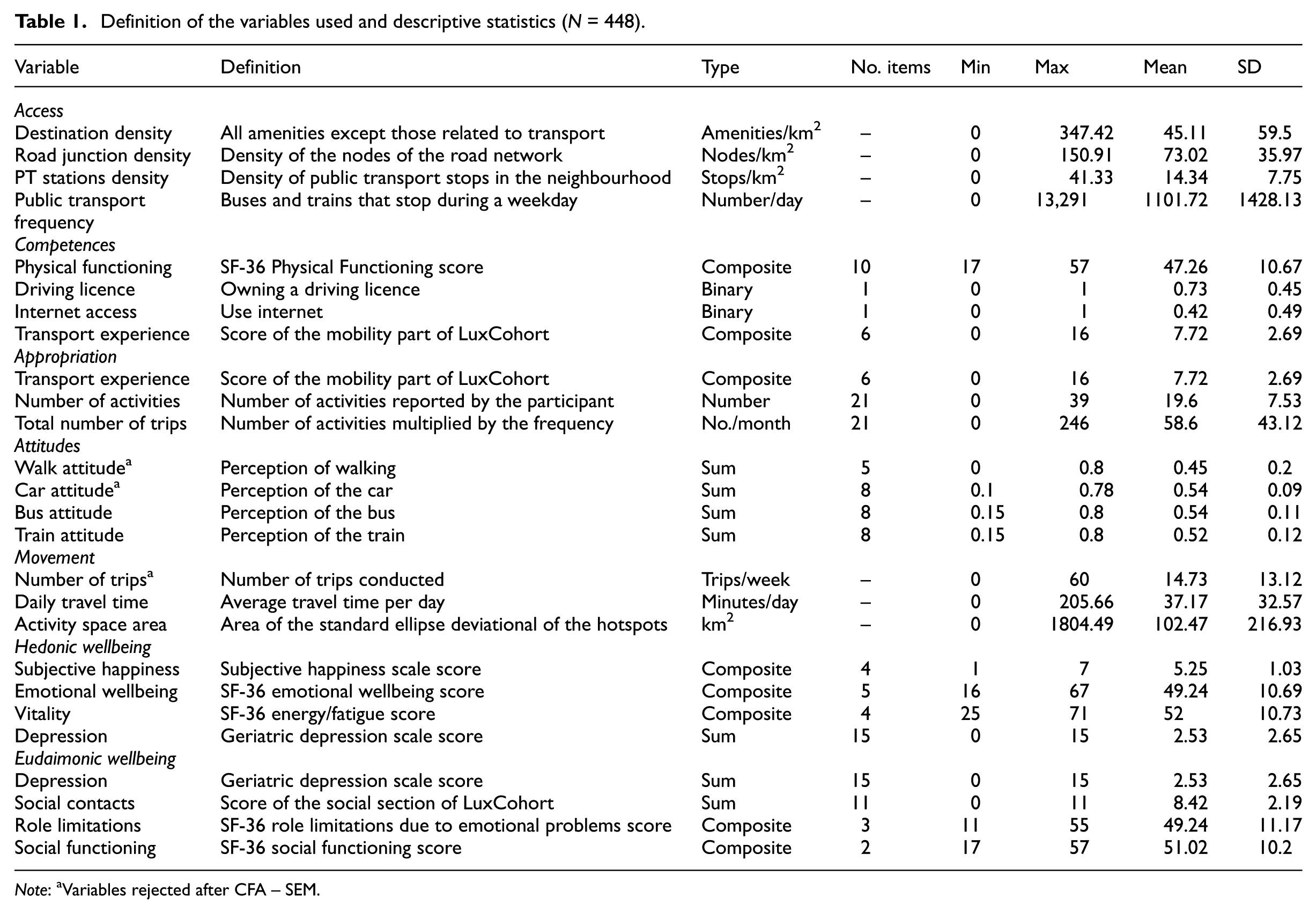
Note: aVariables rejected after CFA – SEM.
Access is defined according to the ‘five Ds’ of Ewing and Cervero (2010), encompassing density, diversity, design, destination accessibility and distance to transit, and the categories are as follows: (1–2) the number of amenities per km2 represents the destination density and diversity of the following items: open markets, supermarkets, fuel stations, restaurants and cafés, bakeries, butchers, tobacco shops, newspaper kiosks, banks, ATMs, post offices, hairdressers, libraries, theatres, cinemas, performance halls, swimming pools and gymnasiums, and parks and gardens; (3) the intersection density, computed as the number of nodes per km2, represents the design of the street network; (4) the number of public transport stations available per km2 is a negative proxy for distance to transit; while (5) shows the number of buses or trains that stop during a weekday, and represents the destination access.
Competences refer to organisational skills, acquired skills through experience, and physical ability (De Witte et al., 2008). Four variables are used: (1) physical functioning, based on the short-form (SF-36) health survey (Leplège et al., 1998); (2) having a driving licence; (3) usage of the internet; and (4) transport experience derived from the self-reported frequency of usage of different transport modes (LuxCohort).
Appropriation focuses on mobility habits of the participants by including again their transport experience (LuxCohort), the number of regular activity places and a proxy of the average number of trips per month self-reported in the VERITAS survey.
Attitudes towards transport modes include four variables: attitudes about walking, car, bus and train. These variables are based on five items for walking and eight items for each of the car, bus and train alternatives. A five-tier semantic differentials scale is used, relating to the participants’ attitudes concerning the speed, comfort, safety, commodity, relaxation, ecology, cost and punctuality of each mode of transport (see supplementary material S2, available online).
In line with previous studies (e.g. Ding and Lu, 2016), movement is characterised by its objective dimensions of space and time. Based on the hotspots derived from the GPS tracks – that is the activity places detected by a kernel-based algorithm (Thierry et al., 2013) – the area of a standard deviational ellipse was computed for each participant, which gives an indication of the size of their activity space (Perchoux et al., 2014). Based on GPS valid trips, 1 daily travel times and actual numbers of trips were computed.
In order to account for the complexity of both HWB and EWB related to older adults and mobility, we need to consider health and medical status (Nordbakke and Schwanen, 2014). The 36-Item Short Form Health Survey (SF-36) offers a validated questionnaire assessing self-reported life satisfaction, health status and hedonic/eudaimonic wellbeing. It succinctly describes eight health concepts through 36 items (e.g. Leplège et al., 1998; Ware and Sherbourne, 1992). In addition to the physical aspects (with regard to assessing the latent variable competences), the SF-36 is also effective to estimate the latent variable hedonic wellbeing (HWB), by using the emotional and affective wellbeing score (five items) and energy–fatigue score (three items). The cognitive component of HWB is measured along the subjective happiness scale (four items) (Lyubomirsky and Lepper, 1999) and the geriatric depression scale (15 items) (Yesavage et al., 1983).
The latent variable eudaimonic wellbeing (EWB) also includes the geriatric depression scale; a social contact index (11 items, authors’ calculation) based on the social part of the LuxCohort survey. In addition, it incorporates the SF-36 social functioning score (two items), the SF-36 role limitations (three items), work or volunteering involvement (one item) and the need of assistance for daily activities (one item).
Results
The first subsection is dedicated to the measurement of motility and wellbeing using CFA. The second subsection reports the SEM analysis.
Motility and wellbeing latent variables
First, the second-order motility latent variable was estimated using three separated first-order latent variables for access, competences and appropriation. With regard to the potential role of attitudes towards transport modes as partly access, competences or appropriation, we performed successive tests, but no congruence was found. However, in line with Kaufmann’s hypothesis, attitudes towards public transport (bus and train) were retained in the model (Cronbach’s α > 0.7), and resulted in a separate first-order latent variable: public transport attitudes. In other words, public transport attitudes are part of the motility concept as suggested by Kaufmann, and complement the three motility components (appropriation, access and competences), instead of being part of appropriation as suggested by Kjaerulff (2011). The results of the CFA on motility (see supplementary material S3, available online) provide good estimates of Standardized Root Mean Square Residual 2 (SRMR = 0.042), Root Mean Squared Error of Approximation 3 (RMSEA = 0.055), Comparative Fit Index 4 (CFI = 0.958) and Tucker-Lewis Index 5 (TLI = 0.941), which indicates a good model fit. All factor loadings are significant at p < 0.001 and the error variances are acceptable (< 0.8), meaning that error terms do not concentrate a high proportion of variance. In line with our expectations (Figure 1), all the estimates of factor loadings are positive. Significant covariance is apparent between all the latent variables, apart from access and competences. The reason for this is mainly that access is based on neighbourhood-level characteristics, and competences focus exclusively on individual-level characteristics.
Second, the results of the CFA on wellbeing reveal a two-factor model (representing HWB and EWB) that correctly fits the data (SRMR (0.022), RMSEA (0.058), TLI (0.971) and CFI (0.983), see supplementary material S4, available online). Depressive symptoms show a negative sign for loadings on both the hedonic and eudaimonic latent variables. There is a positive covariance between the two latent variables.
The CFA results confirm the different subcomponents of wellbeing and motility. Additionally, two second-order latent variables were tested (Figure 1): one wellbeing variable encompassing both the HWB and EWB first-order latent variables, and one motility variable encompassing the access, competences, appropriation and attitudes first-order latent variables. Both second-order latent variables prove to be non-significant in our case (supplementary material S5.a and S5.b, available online). For older adults in Luxembourg, the concepts of motility and wellbeing are not identified as such, thus challenging our theoretical framework built on Kaufmann and colleagues (2004), De Vos and colleagues (2013) and Diener and colleagues (2009). The subsequent analyses accordingly only consider the first-order latent variables.
Main model results
When included in the SEM, all indicators present a significant loading on the latent variables with no variation of sign compared with the CFA. Robust estimates of SRMR (0.053), RMSEA (0.059), TLI (0.893) and CFI (0.911) indicate an acceptable model fit (Figure 2).
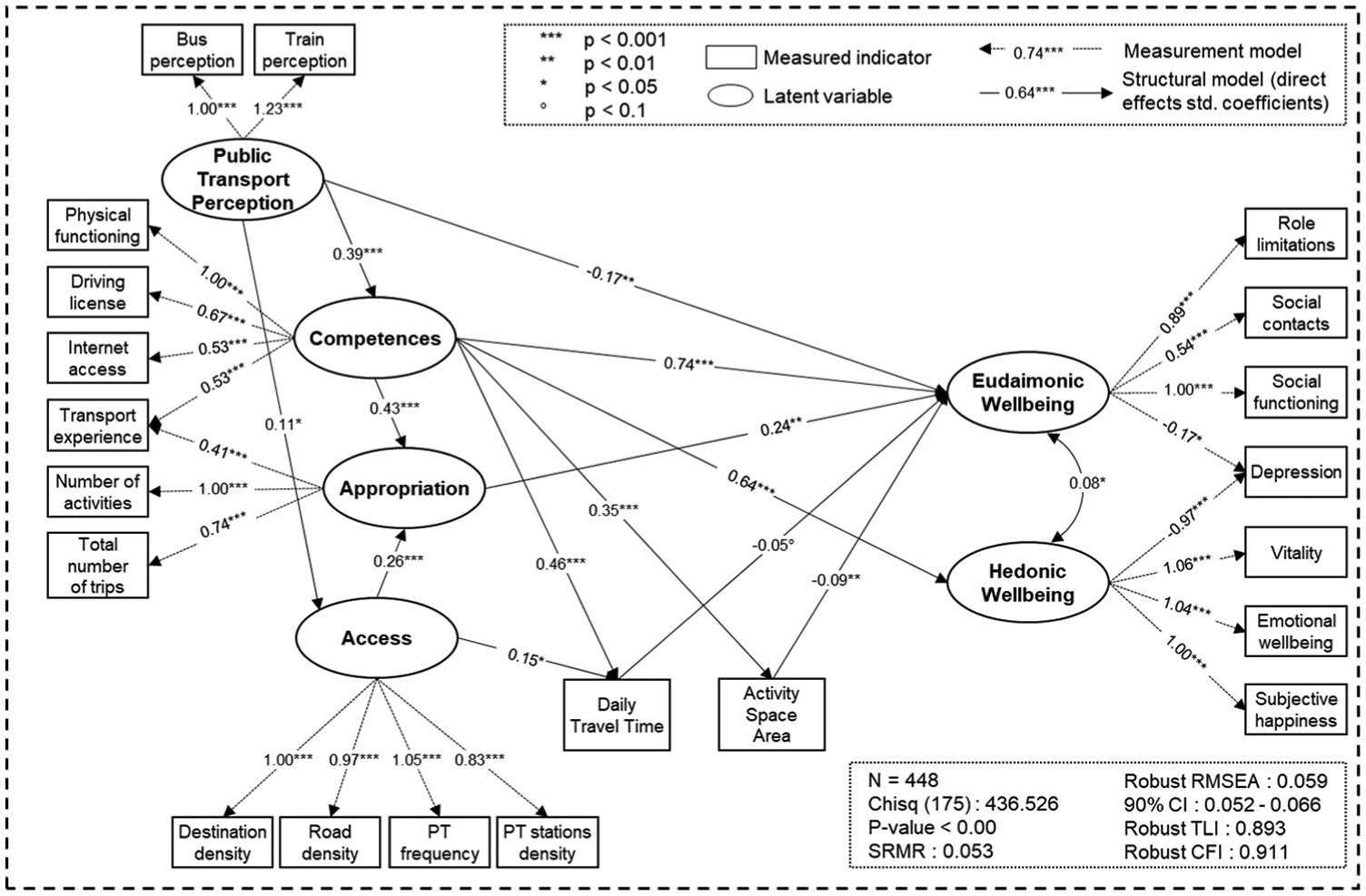
SEM path diagram of the complete model.
With 448 observations for 77 free parameters, the ratio (5.8) is below the ideal sample size to parameters ratio of 20, but still in line with the minimal five to ten observations per estimated parameter (Bollen, 1989). The error term is not shown in Figure 2 for each component to simplify the graphic. Total, direct and indirect effects are presented in Table 2.
Direct, indirect and total association of motility and movement with wellbeing (N = 448).
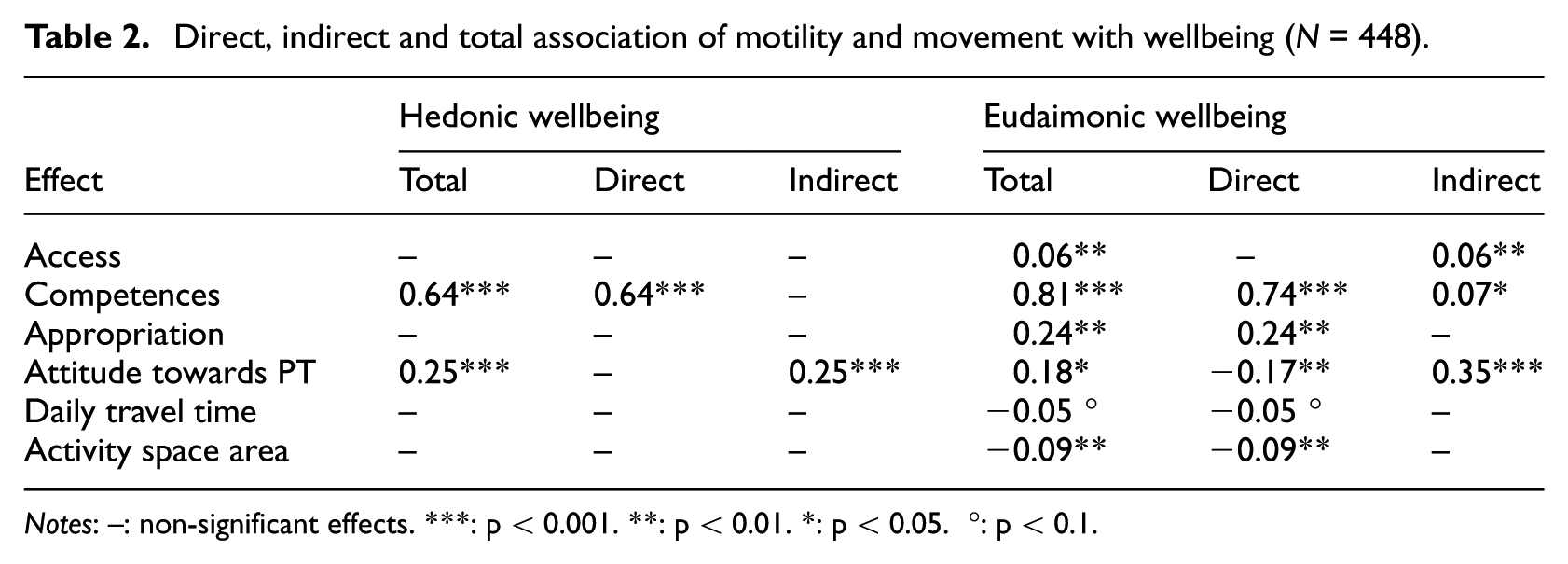
Notes: –: non-significant effects. ***: p < 0.001. **: p < 0.01. *: p < 0.05. °: p < 0.1.
Regarding the links between motility components and movement, it first appears that access and competences are both positively associated with longer daily travel time, and second that competences are positively associated with the size of the activity space, meaning that people with more competences are more likely to travel further away from their residence.
For the links between motility components and wellbeing, only competences are directly linked to both EWB and HWB, appropriation is directly linked to EWB, while access has no direct link to wellbeing. There is an impact of access on EWB, but mediated through appropriation and time movement. Of the three components of motility, only access embeds the geographical context. Geographical context, as measured here, influences wellbeing through movement.
Regarding the links between movement and wellbeing, the size of the activity space – and to a lesser extent, daily travel time – are negatively correlated with EWB. This contrasts with our expectations, and suggests that increased travel time and the size of the activity space are perceived as costs rather than gains.
Discussion and conclusion
To the best of our knowledge, this is a first in-depth analysis of the relationships between dimensions of motility, movement and wellbeing. Access, competences and appropriation are three distinct factors, and could be unified into a unique motility factor. Attitudes towards transportation modes play a role within the concept of motility, but remain a separate component of motility, in parallel with access, competences and appropriation. Motility is positively associated with EWB, and to a lesser extent with HWB. Movement is negatively associated with EWB and partly mediates the association between motility and wellbeing.
Our results are partly consistent with the hypothesised links between mobility and wellbeing. First, compared with previous attempts to quantify motility (e.g. Viry, 2011) and the three components indicated by Kaufmann, we identified a fourth component based on transport attitudes. This component is mostly related to competences, implying that attitudes towards public transport are linked to individuals’ physical condition, and not related to appropriation as suggested implicitly by Kaufmann and colleagues (2004) or explicitly by Kjaerulff (2011). Yet, since our second-order latent variable motility is non-significant (with or without the attitudes; results not shown), the role of each component in motility remains uncertain and should be further investigated.
Second, the negative relationships between both daily travel time and size of the activity space with EWB are interesting in many ways. Regarding the association between the size of the activity space and wellbeing, a potential explanation relies on the escape theory (Heinze, 2000): (leisure) mobility may compensate for a declining quality of life by offering new opportunities and environments away from home. In this sense, mobility and accessibility are intrinsically related to health resources, thus wellbeing. People living in areas with few resources may have to compensate by travelling beyond their residential neighbourhood to increase their accessibility (Vallée et al., 2015). The negative correlation between travel time and wellbeing is consistent with Stutzer and Frey (2008), who find that longer trips are associated with increased monetary cost and increased exposure to environmental stressors (noise, crowding, pollution and adverse temperatures) that contribute to physical and mental burdens. The time–geography perspective further supports this, since the time spent travelling cannot be re-allocated to other personal or social activities that benefit wellbeing. Moreover, this negative aspect is reinforced among older adults, as they need more time to perform daily activities (Kim, 2003). However, others go beyond the notion of travel time as a burden, suggesting that the experienced travel time is context dependent and could affect travel satisfaction and wellbeing in multiple ways (Jain and Lyons, 2008). As argued by these authors, travel time has an intrinsic value for an individual by allowing social relationships to be maintained across space. Further studies linking space and time movement to wellbeing would benefit from exploring the interplay between context, social networks and attitudes.
Third, more generally, our empirical results show stronger relationships between motility and EWB than motility and HWB. This echoes other authors (e.g. De Vos and Witlox, 2017) who stress the link between mobility and EWB, while transport research has mostly focused on utilitarian aspects of satisfaction, particularly through utility maximisation models (e.g. Schwanen and Lucas, 2011).
Finally, we show that the geographical context (i.e. access) impacts wellbeing only through movement. This is in line with previous studies suggesting that greater access increases the number of activities within a short distance, thus leading to several wellbeing benefits (e.g. Föbker and Grotz, 2006). However, we go a step further, by showing that potential mobility is not sufficient per se, because a part of its effect on wellbeing is mediated by movement, which in turn strongly depends on competences (including the frequency of usage of different transport modes) and geographical context (i.e. access).
Limitations
The notion of motility is defined by appropriation, which in turn encompasses mobility habits and related strategies of transport. Empirically, we partly characterise appropriation by the ‘number of regular activity locations’ and the ‘number of trips’ to these locations. These variables are self-reported and defined from the VERITAS map-based survey. In this case, there is a thin line between mobility habits characterised by self-reported regular mobility information, and observed movement characterised by GPS tracks. While we believe this distinction makes sense with regard to the data used, we recognise that appropriation and movement are linked.
We must also acknowledge potential reverse causality and self-selection issues. Our study relies on the assumption that mobility has an effect on wellbeing; but critically, there is a lack of evidence of causality with regard to the direction of the association. While it is highly likely that wellbeing does affect mobility, we believe that our focus on potential mobility reduces the strength of the issue of causality, as motility – defined by access, competences and appropriation – might be less influenced by wellbeing than actual movement might be. The positive relationship between attitudes towards public transport and access is potentially influenced by self-selection: people with more positive attitudes to public transport might choose to live somewhere with greater access to public transport amenities. Additionally, the issue of reverse causality also questions this relationship: competences and access might contribute to shape the attitudes towards public transport. Ziegler and Schwanen (2011) and De Vos and colleagues (2013) discuss the direction of causality, with potential reverse effects from wellbeing, on residential location choice, general orientations, motility and activity patterns; in that people may change their residential location, adjust their orientations, motility and activity patterns precisely in order to increase their wellbeing.
Our results should be treated with caution given the relatively low sample size and complexity of the model. A larger sample size would have allowed us to run a multiple group analysis and account for socio-demographic characteristics. We performed additional analyses where we adjusted for age and gender, but the SEM did not converge, and prevented further control for potential socio-demographic confounding factors. While the lack of statistical adjustment for socio-demographic factors is a concern, we have good confidence in the results given the many specifications we tested. Obviously though, there is a need to repeat similar analyses with more data-rich cases.
Lastly, the data used in this case study are not based on a questionnaire aimed at defining motility. Building such a questionnaire would support future refinements in the empirical definition and measurement of motility components, and provide guidance for replication studies.
Conclusion
Building on the mobility turn and Kaufmann’s sociological approach to mobility, this study is the first to quantitatively separate mobility into motility (i.e. mobility potential) and actual movement, and link them to the wellbeing of older adults. Overall, motility is positively related to eudaimonic wellbeing, and to a lesser extent to hedonic wellbeing. Movement appears to mediate the association between geographical context (access) and wellbeing, and partly mediate the association between motility and wellbeing. Research into the links between mobility and wellbeing would benefit from a further focus on the role both of the potential to be mobile and of realised movement. It is too early to draw strong general conclusions that would be palatable to urban and transport planners, and could guide their actions in favour of more pleasant, less unequal and more sustainable cities. However, our results already point to the fact that changing the local physical features of cities and neighbourhoods – typically by increasing access – is important for enhancing movement and eudaimonic wellbeing, even if they do not necessarily trigger increased aggregate utility values. In turn, supporting appropriation and competences for an ageing population via tailored infrastructures and information is certainly key to empowering people and progressing sustainable and equitable motility. Through planning actions that improve access, policy makers may better help elderly people to blossom and project themselves in their environment. More generally, shifting the focus from travel satisfaction (and largely hedonic wellbeing) to the eudaimonic parts of wellbeing seems key to future planning actions.
Supplemental Material
USJ852033_supplemental_material – Supplemental material for Mobility among older adults: Deconstructing the effects of motility and movement on wellbeing
Supplemental material, USJ852033_supplemental_material for Mobility among older adults: Deconstructing the effects of motility and movement on wellbeing by Timothée Cuignet, Camille Perchoux, Geoffrey Caruso, Olivier Klein, Sylvain Klein, Basile Chaix, Yan Kestens and Philippe Gerber in Urban Studies
Footnotes
Acknowledgements
The CURHA project (Contrasting Urban Environments and Healthy Ageing: The International Longitudinal CURHA Study) is an international study conducted in Luxembourg (LISER – Luxembourg Institute of Socio-Economic Research), Canada (CRCHUM – Centre de Recherche du Centre Hospitalier de l’Université de Montréal) and France (INSERM – Institut National de la Santé et de la Recherche Médicale). It is cofounded by FNR (Fonds National de la Recherche, INTER/JCRA/12/6542889), IRSC (Institut de Recherche en Santé Canada TEA-124969), and FRSQ (Fonds de Recherche du Québec, #28837). We are grateful to the people in LISER from Survey Team.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.