
Abstract
The mental health of students with disabilities has received increasing attention, yet it is difficult for early childhood teachers to identify young children with mental health issues and access support. Research has shown the lack of timely intervention might cause more serious emotional issues later. The interplay of disability, young age, and mental health issues complicate the teaching of early childhood teachers. The purpose of this article is to highlight the difficulties early childhood teachers are experiencing when a child with special needs requires additional support services for social-emotional and behavioral concerns. Barriers or challenges that exist to accessing mental health services for young children and their families are discussed. Through the use of vignettes, we present six strategies to assist early childhood special education professionals in addressing the mental health needs of young children, including 1) recognizing the warning signs of mental health needs for early identification and intervention, 2) utilizing screening tools to detect a child’s mental health needs, 3) selecting and providing school-based supports, 4) monitoring the child’s response to school-based mental health supports, 5) collaborating with mental health professionals and partnering with families, and 6) securing additional networks and resources to support children with special needs.

Nicole is a novice early childhood teacher and is now teaching in an inclusive preschool classroom. Although Nicole is passionate about teaching, she feels challenged by children with special needs and other children with social-emotional needs who do not respond to evidence-supported interventions. For example, John, a 4-year-old boy, was recently diagnosed with autism spectrum disorder (ASD). He has very limited verbal communication to express his emotions but would make sounds when he is excited, happy, or frustrated. John always plays alone, works with the paraeducator, and avoids social interactions with peers. He seldom stays in large group activities, and if he did, he would not stay more than 3 minutes. He would participate in the small group of three children with the paraeducator’s support. John acts aggressively toward other children around him, such as pushing, hitting, and biting when he is upset. Nicole would ask the paraeducator to take John for a walk when he feels agitated or overwhelmed in the classroom. He has thrown a chair at the teacher and his peers on several occasions when he could not regulate his anger. Nicole created a visual schedule to help John transition across the daily activities, but it did not work well for him. She has tried to engage John to play with his peers, but he did not like to be around other children. Nicole is concerned John’s behaviors and emotions might escalate later and influence his mental health if she does not provide timely and effective intervention. While Nicole tried some intervention strategies, she did not achieve the expected improvement, and she feels like she needs more support. After having John’s individualized education program (IEP) meeting, the team developed a goal to address John’s social and emotional needs. Nicole has worked with several professionals and learned the importance of ongoing data collection. However, she has not mastered monitoring John’s progress toward his IEP goal. By working with John, Nicole also wants to learn how to detect warning signs early and use data to inform her teaching to support other children with social-emotional needs in her classroom. She heard about the mental health service consultation in the K–12 grades but does not know how to get support in her preschool program. She reaches out to the school district and wonders what training or resources are available to utilize in her early childhood classroom. She tried to find effective ways to partner with John’s family and collaborate with the mental health service consultant and other professionals to support John’s social-emotional needs.
The vignette illustrates common concerns for novice teachers working at center-based early childhood programs when children with or without special needs exhibit ongoing aggressive challenging behaviors and mental health issues. The lack of timely intervention on the early onset of behavioral and emotional issues might cause adverse outcomes in learning and development later in the child’s life (Fanti & Henrich, 2010). The interplay of disability, young age, and mental health issues complicates the teaching for early childhood teachers. The purpose of this article is to highlight the difficulties early childhood teachers are experiencing when a child with special needs requires additional support services to address social-emotional and behavioral concerns. Barriers or challenges that exist to accessing mental health services for young children and their families are discussed. We present six strategies to assist early childhood special education professionals in addressing the mental health needs of young children, including (a) recognizing the warning signs of mental health needs for early identification and intervention, (b) utilizing screening tools to detect a child’s mental health needs, (c) selecting and providing school-based supports, (d) monitoring the child’s response to school-based mental health supports, (e) collaborating with mental health professionals and partnering with families, and (f) securing additional networks and resources to support children with special needs.
Importance of Early Childhood Mental Health
The mental health of young children has received attention because of an increasing trend of preschoolers being expelled or suspended for problem behaviors (U.S. Department of Health and Human Services & U.S. Department of Education [USDHHS & USDOE], 2016) and the estimate that one in six U.S. children age 2 to 8 years had a diagnosis of mental, behavioral, or developmental disorder (Cree et al., 2018). Early childhood mental health refers to the ability of young children from birth to 6 to experience, regulate, and express emotion; to establish intimate and secure relationships with others; and to actively discover the environment and learn. It synonymously reflects the essence of healthy social and emotional development (Zero to Three, 2016). Mental health and social-emotional competence are regarded as the same construct in early childhood (Sheridan et al., 2015). However, the detrimental effects of mental health problems on children’s learning and development are greatly associated with many unfavorable outcomes, such as the development of antisocial behaviors and juvenile delinquency (Qi & Kaiser, 2003). Children who demonstrate developmentally appropriate skills in social-emotional development lay a strong foundation for mental health.
Children shape their social, emotional, and cognitive development through their experiences and interaction with various people in different contexts (National Scientific Council on the Developing Child, 2008/2012). In many classrooms, preschool children who meet developmental milestones with competent social-emotional skills interact with others well and use different ways to express their emotions. These children play with each other rather than play alone and take turns during play. However, many children with disabilities are not experiencing these same positive interactions. Zeng et al. (2019) analyzed parent-reported data and indicated 174,309 preschoolers were suspended in 2015 (i.e., a weekly average of 4,842 preschoolers). Behavior problems of children with disabilities are 3 to 4 times higher than their typically developing peers (Baker et al., 2002, 2003). Research also shows that 30% to 35% of people with intellectual or developmental disabilities have a co-occurring mental disorder (Icovino & Esralew, 2019), and issues such as anxiety disorders, conduct disorders, and depression that affect mental health can occur at a very young age (National Institute of Mental Health, 2021). For example, mental health conditions such as disruptive behavior disorders and/or anxiety that impair the quality of life are frequently observed in ASD (Lai et al., 2019).
A major determinant of both physical and mental health outcomes is the presence of traumatic or toxic stress stemming from domestic violence, child abuse, neglect, or other disruptions to a family (Shonkoff et al., 2012). During the early childhood years, one in four children has experienced a traumatic event. The areas in the developing brain that govern emotions and learning are affected when children are exposed to trauma and high-level stress in their early years. Stress can be helpful as our body reacts to situations and learns how to cope with them. However, the frequent, strong, toxic stress that happens in childhood disrupts the architecture of the developing brain and might cause long-term effects on learning, behavior, and physical and mental health (National Scientific Council on the Developing Child, 2020). Teachers need to consider family functioning and whether adverse childhood experiences, including abuse, neglect, and household dysfunction (substance abuse, parent with mental illness, domestic violence), are contributing to the child’s behavior. The frequency, severity, and timing of trauma along with responsive relationships determine how a young child responds to stress (e.g., fight, flight, freeze; National Scientific Council of the Developing Child, 2020). A child with a disability like John in the vignette or other children who exhibit aggressive behaviors while facing several adverse experiences is facing a double dose of challenges to their social-emotional development, which puts them at greater risk for mental health needs.
The absence of a mental disorder or disability is not indicative of sound mental health, but the disability condition does influence the mental health of children with special needs. Young children with limited communication skills are more likely to engage in challenging behaviors to communicate their needs. Long-term engagement in challenging behaviors without proper intervention jeopardizes social-emotional development (Hauser-Cram & Woodman, 2016). Common characteristics of children with disabilities, such as deficits in communication skills (e.g., delayed language development), engagement in challenging behaviors (e.g., easily distracted), and lack of social-emotional coping skills (e.g., unusual emotional reactions), interfere with how they express feelings or act upon others, which affects their mental health in social, emotional, and behavioral functioning (Icovino & Esralew, 2019). Many adults who receive mental health support indicate the impact mental disorders had on their childhood and emphasize the importance of receiving intervention earlier (National Institute of Mental Health, 2021). The early childhood community has recognized the importance of providing timely evidence-based intervention to preschool children to promote social-emotional development (Dunlap et al., 2014). The chaining effects of challenging behaviors, emotional difficulties, and possible social rejections by peers place children in need of intervention to promote mental health.
John demonstrates a lack of using language to express his needs and feelings verbally. His challenging behaviors or lack of emotional regulation might further prevent other children from interacting with him and are detrimental to social interaction and play, which are important experiences for young exceptional children in inclusive classrooms.
Teachers’ Role in Children’s Social-Emotional Development
The time children spend in center-based programs and the quality of teachers’ interaction with them signify teachers’ critical role in supporting children’s social-emotional development, especially those with disabilities or already showing mental health needs. About 67.1% of the 815,00 children ages 3 through 5 served under the Individuals with Disabilities Education Act, Part B, spend some time in regular early childhood programs in 2018 (U.S. Department of Education, 2021). Children diagnosed with developmental disabilities typically require services to address behavioral and developmental challenges. In the overall preschool samples, about 10% of children are diagnosed with emotional or behavioral disorders (Forness, Freeman, et al., 2012). Such numbers reflect how early childhood teachers attest to teaching children with problem behaviors as most challenging (Anderson & Lindeman, 2017; Forness, Kim, et al., 2012). While school-age students might receive more attention to address their mental health needs, mandated mental health services are not commonly provided to preschool children (Forness et al., 2012). The teacher’s role in providing mental health services and in enhancing a child’s social-emotional development involves six strategies: (a) recognizing early warning signs, (b) screening for mental health concerns, (c) strategizing school-based supports, (d) monitoring the child’s progress, (e) collaborating with professionals and families, and (f) securing additional resources.
Recognizing Early Warning Signs of Mental Health Needs for Early Identification and Intervention
Observe children and document if they are exhibiting behaviors that deviate from typical development. Table 1 presents what children typically do at various age. Behaviors that deviate from what is typical may signal early childhood teachers to attend to children’s mental health needs. The prevalence of mental health issues in early childhood has directed our attention to take up the mental health concerns of children with disabilities because they often present persistent behavior and emotional issues. However, diagnosing mental health issues at a young age posts difficulty (McCrae & Brown, 2018) because young children may typically exhibit relatively insignificant oppositional behaviors at an early stage, such as minor peer adjustment problems or noncompliance to parental instructions. Without proper intervention, they may begin to exhibit behaviors in the preschool environment that progress more severely or disruptively over the preschool years (Feil et al., 2014).
Typical Social-Emotional Development: Ages 3 to 5
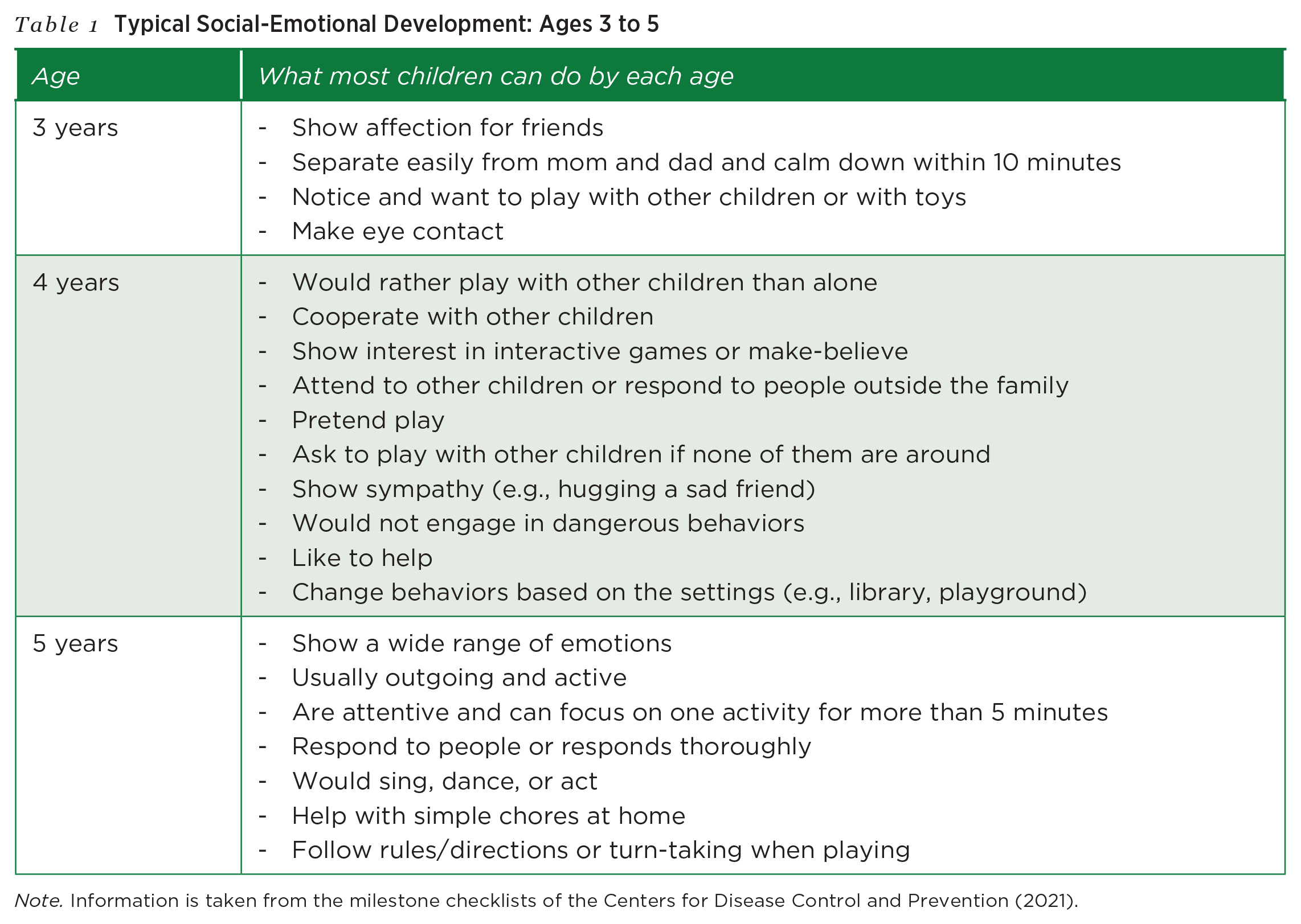
Note. Information is taken from the milestone checklists of the Centers for Disease Control and Prevention (2021).
Nicole uses the warning signs (see Table 1) to help her check on John, who has behavioral and emotional issues. She identifies that John requires additional support to address his mental health needs. Although she has a solid knowledge base of children’s development from her undergraduate program, she does not know how to support John with ASD when he does not demonstrate appropriate social-emotional development. Nicole is aware children might display challenging behaviors when they are new to the environment. She also knows those behaviors might be typical for most children at their age and developmental stages. Because she has been in the preschool classroom for some time and John’s behaviors are persistent, Nicole has a concern. She recalled an assessment class that discussed using screening tools to validate her concerns as a first step before making the referral.
Utilizing Screening Tools to Detect a Child’s Mental Health Needs
Choose reliable social-emotional screening tools coupled with classroom observations to identify children who are at risk or may need referral for mental health concerns early. Screening is considered part of a comprehensive and effective school-based mental health program (Dvorsky et al., 2014). Most mental health referrals for school-age students with mental health needs rely on teachers’ nominations, and those students who show severe signs are easier to identify (Dvorsky et al., 2014). Young children with mental health needs might not be evident due to their age. Programs should exchange information with families about their child’s learning, social-emotional, and behavioral development gathered through regular and ongoing screenings (USDHHS & USDOE, 2016). Screening is a systematic process of confirming concerns, especially when children raise a red flag such as difficulty in regulating their emotions, and/or detecting children who need mental health services but have shown smaller signs. If the child is confirmed with a delay, teachers can refer the children for further evaluation. If the child’s screening results show the development is within normal range, the child may not be eligible for referral. The teacher should continue to monitor the child’s development and consider the need for further assessment tools. The developmental or universal screening provides teachers with an understanding of the child’s current development in various domains when compared with his/her same-age peers who are typically developing. The intent of focusing on social-emotional development is to find children who are at risk or in need of mental health services early on and provide timely intervention (Dvorsky et al., 2014; McCrae & Brown, 2018). Depending on the different educational/cultural contexts, screening might require administration by trained personnel. For schools in which screening tools are unavailable, teachers can utilize observations or interview to gather children’s data and consult with other professionals, such as special education teachers.
Teachers can use screening to gain valuable information in checking children’s social-emotional development against their typically developing peers. The goal of screening influences the arrangement of timing and frequency (Dvorsky et al., 2014). For example, screening can be administered at critical transitions, such as entry to the preschool program, to help teachers identify children who might be delayed. However, screening at entry should be done and interpreted with caution because the results could be problematic for children entering a group setting for the first time due to common separation issues. If teachers are interested in children’s change over time, screening can be conducted periodically, such as in the fall and the spring of a given year or yearly across years. Comprehensive assessment and universal screening of social-emotional development and challenging behaviors are essential to the process of identifying children’s mental health needs (Division for Early Childhood [DEC], 2014, 2017).
A variety of effective screening measures are available for early childhood teachers to gather information of social-emotional development in children. McCrae and Brown (2018) used a set of criteria to evaluate social-emotional screening instruments for very young children (infants, toddlers, and preschoolers) and suggested two tools: (a) Ages & Stages Questionnaire – Social Emotional (ASQ-SE; Squires et al., 2002) and (b) Preschool and Kindergarten Behavior Scales–Second Edition (PKBS-2; Merrell, 2003).
ASQ-SE
The first tool, ASQ-SE, includes items in seven key social-emotional areas: self-regulation, compliance, adaptive functioning, autonomy, affect, social communication, and interaction with people, and had a revised second edition, ASQ-SE:2 (Squires et al., 2015). ASQ-SE:2 is used to screen children in the first 6 years of life. It consists of nine age-sequential questionnaires and three questionnaires (36-, 48-, and 60-month intervals) covering the preschool age range. A starter kit consists of nine questionnaires, scoring sheets, a CD-ROM with a printable PDF questionnaire, a user’s guide, and a quick start guide, available for $295 from the publisher’s website (Paul H. Brookes Publishing, 2018). Each questionnaire requires the parent’s input and takes about 10 to 15 minutes to complete. It takes the child’s teacher about 2 to 3 minutes to score. ASQ-SE:2 has four languages available: English, Spanish, French, and Arabic. The publisher also provides in-person and virtual training for a fee, depending on the program’s needs.
PKBS-2
The second tool, PKBS-2, consists of two scales: social skills (social cooperation, social interaction, and social independence) and problem behaviors (externalizing problems and internalizing problems; Merrell, 2003). It measures children 3 to 6 years of age. There are 76 items, which take 8 to 12 minutes to complete. Parents, teachers, and other caregivers who know the child well can complete PKBS-2. Raters rate each item on a 4-point Likert scale and refer to different score conversion tables for home- or school-based use. PKBS-2 is available in English and Spanish. A complete PKBS-2 kit includes a test manual and 50 test forms, available for $151 from the publisher (PROED, 2022).
Both tools are considered reliable to help identify children at risk of social-emotional difficulties and in need of support and have multiple advantages for use for early childhood teachers. They take a short time for administration, are suitable for children in the 3 to 5 age range, require less training in scoring and interpretation, and have family input. Specifically, such standardized mental health screening involves families in the service delivery process and has the potential to improve the equity of service access (McCrae & Brown, 2018). Once a child’s screening scores result in a referral, the teacher refers the child for further evaluation. A team of professionals, teacher(s), and parent(s) collaboratively develop an IEP under the coordination of special educators if the child is determined eligible for receiving special education services (Yell et al., 2020). Of importance, the section on present levels of academic achievement and functional performance (PLAAFP) provides information such as the student’s strengths and needs in support of developing annual goals and serves as the baseline to monitor the student’s progress toward the goal (Harmon et al., 2020). PLAAFP statements also help the planning, delivery, and evaluation of the instructional intervention (Harmon et al., 2020), such as implementing the instruction systematically with fidelity and addressing generalization by embedded instruction within or across the student’s routines, activities, and environments (DEC, 2014).
Observational tools
Screening tools may be enhanced through classroom observation. The preschool teacher or other support personnel may follow up on the results of the ASQ-SE if one or more of the seven key social-emotional areas suggest possible mental health needs. Observation of compliance, social communication, and social interactions of the preschool child may confirm the need for intervention. Similarly, if the PKBS-2 indicates difficulties in either the social skill or problem behavior scales, classroom observation may help identify target behaviors to increase or decrease through intervention. Table 2 describes two common observation tools with examples of target behaviors.
Observational Tools with Behavior Examples
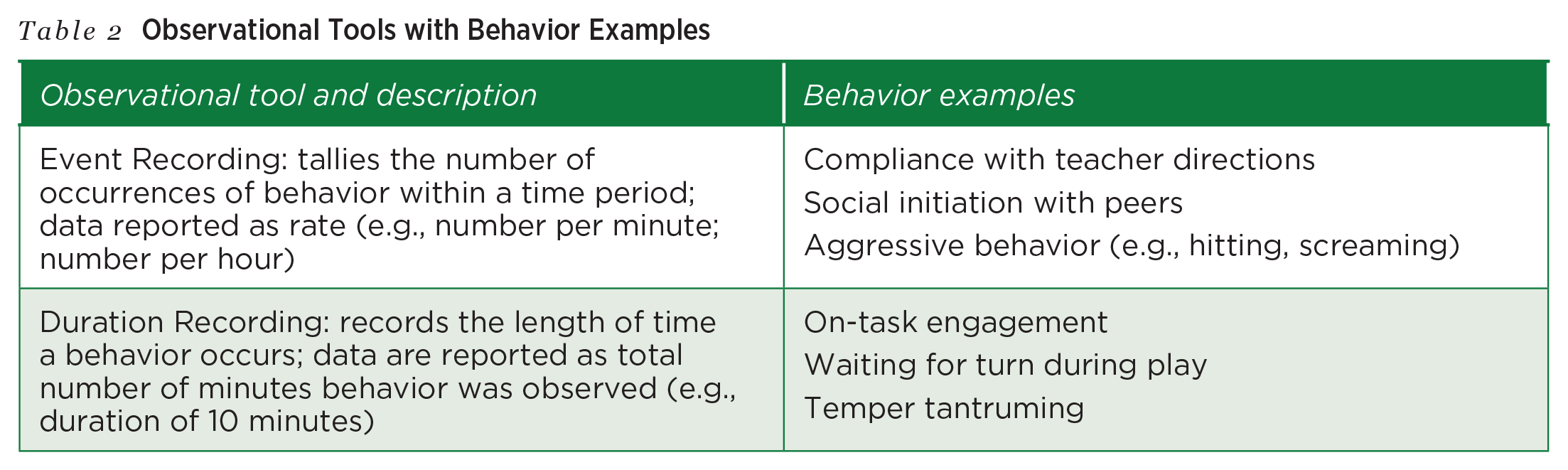
The results of classroom observations coupled with the screening results will help the preschool teacher select and provide appropriate school-based mental health supports.
Nicole now has the two reliable screening tools that could help her identify children she might have a concern for with social-emotional needs. These tools are readily available, and she can collaborate with the local Area Education Agency to access the tools if her program does not have them. Nicole can also attend professional development to learn how to use these two tools with support from the school district. Her program carries ASQ-SE:2. She sent the 48-month interval questionnaires (suitable for children 42–54 months old) to the parents of children (including John as described in the vignette) who might be at risk of mental health needs. The parents returned the completed questionnaires to Nicole. She scored these questionnaires, shared results (no or low risk, monitor, refer) with parents, and discussed helpful resources with parents so that they can promote their children’s social-emotional development at home. Taking John as an example, the ASQ-SE:2 reconfirmed his delay in social-emotional development. Nicole can now share the screening results with the IEP team to select and provide school-based mental health supports. The IEP team will then develop a goal for John to express his emotions using verbal and picture cards. The intervention teaches him to verbally express or use pointing and picture cards that represent different emotions. Along with the observation tools, Nicole and the IEP team decided to use event recording to gather the frequency John uses pointing or picture cards to express different emotions.
Selecting and Providing School-Based Supports
Create a supportive environment to nurture social-emotional development and use evidence-based practices by considering each child’s individual needs. Strategies to improve early childhood mental health can follow along the continuum of promotion, prevention, and intervention (Zero to Three, 2016). DEC (2017), in the position statement on challenging behaviors and young children, endorsed by Zero to Three, also emphasizes the importance of preventing and addressing challenging behaviors caused by social-emotional incompetence and delays in communication. The DEC’s recommended practices have guided the services and intervention in promoting children’s positive outcomes (DEC, 2014). Early childhood teachers can support children’s mental health through supportive environmental arrangements and evidence-based practices.
Arranging a supportive environment
A supportive environment that promotes mental health (World Health Organization, 2018) is fundamental for teachers to foster children’s social-emotional development as preschool children spend much of their time in early childhood settings. The environment should be stable and sensitive to children’s needs, protect them from threats, provide early learning opportunities, and allow interaction responsive to social-emotional development. Children must feel welcomed and cared for by their teachers and peers. Especially for children with disabilities who typically do not initiate interaction or play, teachers can create opportunities to engage them in learning. Teachers should consider physical, social, and temporal features in the environmental arrangement (DEC, 2014). Features such as soft lighting, comfortable spaces, quiet corner, and headphones with recorded stories of calm music reduce overstimulation. For example, calming music has been proven effective in reducing aggressive behaviors (Goldbeck & Ellerkamp, 2012). Children who have better social-communication skills can pair and play with children with disabilities. Teachers and adults in the classroom should attend to every child’s needs and respond to appropriate behaviors and prevention by identifying signs of agitation or need for quiet time.
Using visual support
A predictable sequence of routines and activities supports children with disabilities to engage in learning experiences in the natural environment. Many children with ASD are visual learners (Quill, 1997). Visual support, an evidence-based practice, can help them cope with the different needs of the environment and communicate with others with appropriate social behaviors by providing concrete prompts related to an activity, routine, expectation, and skill practice (Kidder & McDonnell, 2017; Wong et al., 2014). These visual supports include activity schedules, consequence maps, cue cards, social narratives, and symbol exchange (Kidder & McDonnell, 2017).
Keeping the child’s individual needs in mind, Nicole decides to make an individualized visual schedule with pictures for John. She took photos when John participated in different activities in the classroom’s daily routine. She creates an activity schedule with John’s photos that follows the classroom routine (arrival, circle time, center time, cleaning up, snack time, outside play, circle time, departure). The visual support of the activity schedule eliminates John’s insecurity by providing a predictable routine. Nicole has found John reduces the number of tantrums during transitions. However, John continues to have difficulty expressing his emotions and interacting with his peers positively. His IEP goal is to express his emotions using verbal and picture cards.
Monitoring the Child’s Response to School-Based Mental Health Supports
Determine the appropriate data collection methods based on the criteria of the IEP goal and collect data to monitor the child’s progress regularly with documentation. Monitor a child’s progress using the same observation tools discussed earlier. Ongoing monitoring tracks children’s development so teachers can act early (Centers for Disease Control and Prevention [CDC], 2021). Using the gathered data can provide timely intervention, assess the effectiveness of the intervention, and provide necessary feedback to adjust the intervention accordingly. This continuum of data collection serves the function of promotion, prevention, and intervention. While the PLAAFP provides baseline data to help monitor the progress of the student with disabilities toward the IEP goals (Harmon et al., 2020), ongoing monitoring is needed to check if a child’s social-emotional development is on track (CDC, 2021).
A range of data collection methods can help with continuous monitoring. Gathered data and progress toward the IEP goals are used to inform the adjustment of instruction (Yell & Bateman, 2020). McAfee et al. (2016) identify three major types: (a) those that describe, (e.g., running records, anecdotal records), (b) those that count or tally (e.g., checklist, frequency), and (c) those that rate or rank (e.g., rating scales). The tools utilized for observational screening provided in Table 2 should also be considered as the metric selected for progress monitoring. These methods provide early childhood teachers with an array of ways to collect and monitor children’s social-emotional development and skills through observations.
Nicole decides to start the documentation from John in collaboration with the special education teacher and extends her observations to a few other children who exhibit challenging behaviors. Nicole also develops some data recording sheets that help her document the data for progress monitoring. She made an emotion check-in and check-out system to allow all children to identify and express their emotions. Every child puts a smiley face, an upset face, or a question mark next to his/her name. Nicole has a quick check and uses the opportunity to teach children emotional literacy or talk about feelings during circle time. Considering that John would act aggressively toward his peers when playing, Nicole increases two check-ins at the center time and outside play when John has an opportunity to play with his peers. Nicole presents John with his individualized visual schedule and follows with the emotion check-ins. If John seems overwhelmed, he has an opportunity to use a symbol exchange card “I need a break” to stay in the quiet corner. Nicole checks John’s emotions four times daily and uses frequency counts to monitor John’s progress toward his goal of expressing emotion. See Table 3 for the data sheet that can collect and monitor John’s progress toward his IEP goal. Nicole uses the four check-ins and asks how John feels. She then marks whether John expresses his emotions verbally or using a picture card (including pointing). Nicole marks on the data sheet and tally. The sheet has 5 days of data collection, and Nicole can easily adapt it to collect data on other children.
An example of data collection/monitoring sheet using event recording
Child: John
Goal: Express emotions verbally or using picture cards
Date: 8/22–8/26/2022
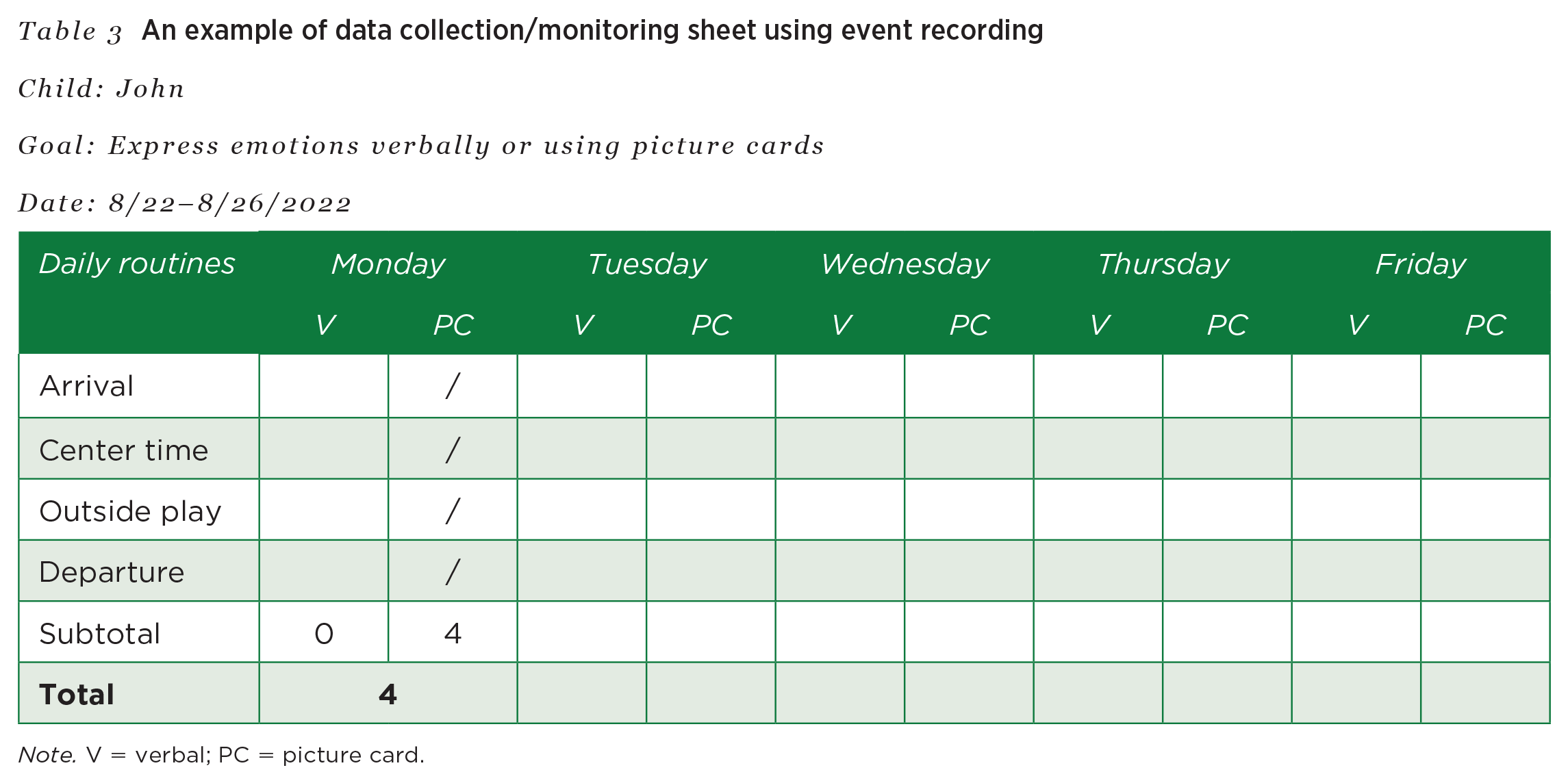
Note. V = verbal; PC = picture card.
Collaborating With Mental Health Professionals and Partnering With Families
Engage in frequent and regular communication with families and collaborate with mental health consultants to guide the selection of interventions. What children experience at home might reflect on their behaviors, emotional expression, and interaction with others in the early childhood settings (e.g., child care, classrooms) and vice versa. DEC (2014) recommends practices such as sharing information with families, respecting family choices, and collaborating with families in the development of intervention. Effective communication between parents and teachers is key to ensuring children’s mental health is monitored and supported through school-family collaboration.
Research shows engaging families in the intervention positively improves children’s social-emotional skills. In a randomized controlled trial study (Feil et al., 2014), 149 preschool teachers (Head Start, state-funded, tuition-based, private preschool classrooms) in Indiana, Kentucky, and Oregon received training to learn behavior intervention strategies through a daylong workshop and a behavioral coach’s ongoing mentoring of the First Step to Success program (for details, see Frey et al., 2013). The random assignment was based on the classrooms, thus children and parents were matched with their teachers in the same group. Parents in the intervention group also received coaching to learn and implement the strategies in the First Step to Success. The results indicate preschool children in the experimental group demonstrated significantly higher social skills and lower problem behaviors compared to those in the control group (Feil et al., 2014).
Effective communication between teachers and parents can occur during daily routines or structured contact. For example, teachers can easily check in with parents during daily drop-off or pick-up. This allows relationship building. Structured contact such as a monthly newsletter can provide parents with social and emotional supporting strategies, resources in the community, and what the school has been doing. Daily observations through a written note can document what excites children or unusual emotional changes in children at school.
As a new teacher, Nicole talks to other experienced teachers and learns there are many ways she can communicate with families and involve families in promoting children’s social-emotional development. She decides to try the daily check-in, such as asking John’s mom about how he plays with his brother and a brief update about John’s day when his mom picks him up. She also starts a monthly newsletter to share information with families, such as storybooks on expressing different emotions, calming strategies taught in the classroom, and resources for parents.
Early childhood mental health consultation
An effective approach to addressing emotional and behavioral issues in preschool practices and helping develop early childhood teachers’ competencies to support the social-emotional development of children with challenging behaviors is through early childhood mental health consultation (ECMHC; Brennan et al., 2008). This mental health consultation is aligned with classroom-based behavioral consultation, recognized as an important resource in early childhood (Albritton et al., 2019). Nearly 2 decades ago, Gilliam (2005) indicated early childhood teachers’ access to classroom-based behavioral consultation had the potential to reduce the likelihood of preschool expulsion and suspension. The policy statement (USDHHS & USDOE, 2016) also suggested early childhood programs include access to consultants and specialists (e.g., ECMH consultants). A recent systematic review reconfirms ECMHC as promising in addressing preschoolers’ behavioral concerns across different settings (Albritton et al., 2019).
ECMHC is a collaborative, problem-solving intervention to build capacity to address social-emotional needs of young children (Cohen & Kaufmann, 2000). DEC (2014) recommended practices highlight the importance of practitioners’ promotion of children’s social-emotional development and engagement in positive interactions with others. The focus on consultative services may occur at the child, family, or program levels (Cohen & Kaufmann, 2000). In ECMHC, a consultant with mental health expertise collaborates with early childhood teachers/staff, programs, and families to improve their ability in prevention, identification, and intervention and to lessen the impact of mental health problems in young children (Gilliam et al., 2016).
In the classroom-based ECMHC, the direct interaction between the early childhood teachers and mental health consultants leads to positive changes, and such change in teachers’ skills and knowledge results in favorable outcomes in promoting children’s social-emotional development (Williford & Shelton, 2008). The collaboration of expertise from both early childhood teachers and mental health consultants is vital to better children’s outcomes (Icovino & Esralew, 2019), such as improvement of social skills, reduction of challenging behaviors, prevention of suspensions and expulsions (USDHHS & USDOE, 2016), and lower ratings of hyperactivity, restlessness, externalizing behaviors, problem behaviors, and total problems (Gilliam et al., 2016). In addition, ECMHC is effective in reducing teachers’ stress, burnout, and turnover (USDHHS & USDOE, 2016) and increasing self-efficacy, competence in addressing challenging preschool behaviors, and sensitivity toward students (Brennan et al., 2008).
Early Head Start and Head Start programs are the primary consumers to receive ECMHC service across the nation (Duran et al., n.d.) because the performance standards require sufficient and timely identification and intervention to address the concerns of a child’s mental health raised by family and staff (Head Start Program Performance Standards, 2016). Other early childhood programs might rely on some public funding sources to access more child-focused ECMHC (Duran et al., n.d.) for children with disabilities, such as Section 619, Part B in the Individuals with Disabilities Education Act (2004), Early and Periodic Screening, Diagnostic, and Treatment (EPSDT). The EPSDT benefit requires states to provide children under age 21 enrolled in Medicaid with comprehensive health services, including mental health (Centers for Medicare & Medicaid Services, n.d.).
ECMHC occurs in the context of collaboration, and the examination of best practices helps promote the effectiveness of ECMHC. Early childhood teachers share their expertise in child development and learn from consultants about mental health. However, the hurdle is that many systems work independently from other groups, meaning the systems that cope with developmental disabilities may not attend to mental health and vice versa (Icovino & Esralew, 2019). Specifically, a mental health consultant needs to have a deep understanding of best practices of mental health as well as typical and atypical child development in the context of early childhood settings, with foundational knowledge of social and emotional milestones and intervention strategies (Center for Early Childhood Mental Health Consultation, n.d.). Cross-disciplinary training is important yet insufficient. DEC (2014) recommended practices indicate that “the quality of relationships and interactions” among the adults serving children who have or are at risk of developmental delays and disabilities impacts the effectiveness of the services and education (p. 15). Nonetheless, the collaboration between early childhood teachers and consultants develops the capacity to serve both children with and without disabilities with child-focused intervention in producing better social-emotional outcomes. The following items in Table 4, adapted from Green et al. (2012), allow an early childhood teacher to examine best practices of early childhood mental health in her classroom.
Examination of best practices of early childhood mental health consultation
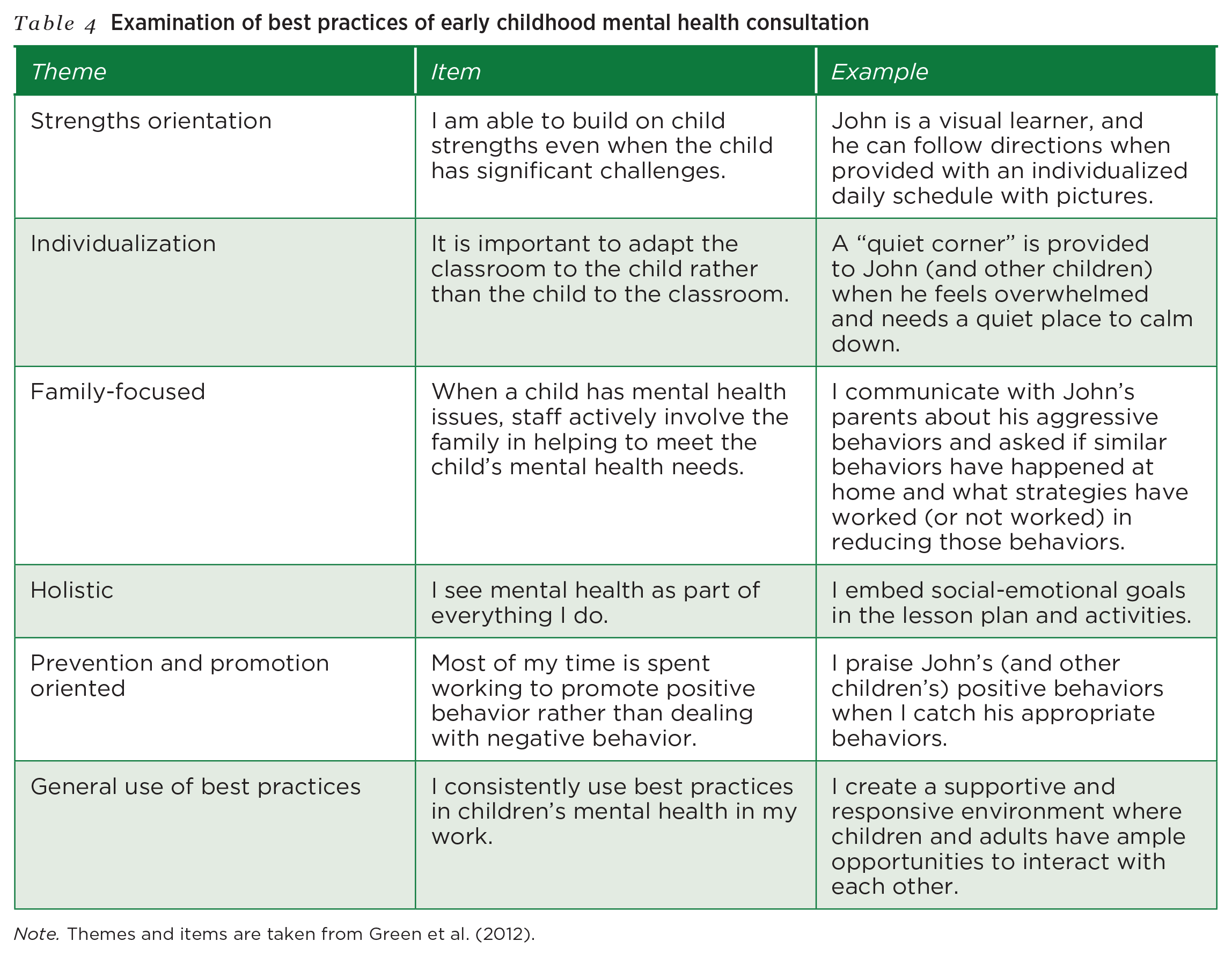
Note. Themes and items are taken from Green et al. (2012).
Together, Nicole works with the school psychologist in the building to develop interventions to address John’s social and emotional needs. They explore the themes and items regarding the best practices of ECMH in Table 4. They discuss possible examples and activities. Nicole uses items in Table 4 to observe and document examples of what she has been doing with John to reflect on her practices either by herself or with another teacher. For example, this ECMHC is child-focused, and it will help Nicole develop strategies based on John’s strengths and tailored to his needs with consultation from the school psychologist. Input from John’s family can provide Nicole with information to determine what can be done in both school and home to allow parent involvement. Because a positive environment can foster every child’s social-emotional development, Nicole can embed the social-emotional goal in John’s IEP into the lesson plan for the entire class to ensure that evidence-based practices are consistently promoted in the classroom.
Securing Additional Networks and Resources to Support Children With Special Needs
Locate creditable and free online resources to increase the knowledge and skills to promote mental health of children with disabilities through self-paced learning. Recognizing the critical role early childhood teachers play in promoting young children’s social and emotional development, different stakeholders have put together funds, research, and training to enhance teachers’ knowledge and skills in using evidence-based practices. The pyramid model is a well-known framework developed by two national, federally funded research and training centers: the Center for the Social and Emotional Foundations for Early Learning (CSEFEL) and Technical Assistance Center on Social Emotional Intervention for Youth Children. The National Center for Pyramid Model Innovations (NCPMI) has promoted the multitiered system of the pyramid model to improve the social, emotional, and behavioral outcomes of young children with and at risk for developmental disabilities or delays through ongoing and collective efforts of faculty members and research scholars. Early childhood teachers benefit from the resources and training opportunities. Table 5 lists resources and self-paced training tools for early childhood teachers.
Selected Useful websites for early childhood teachers
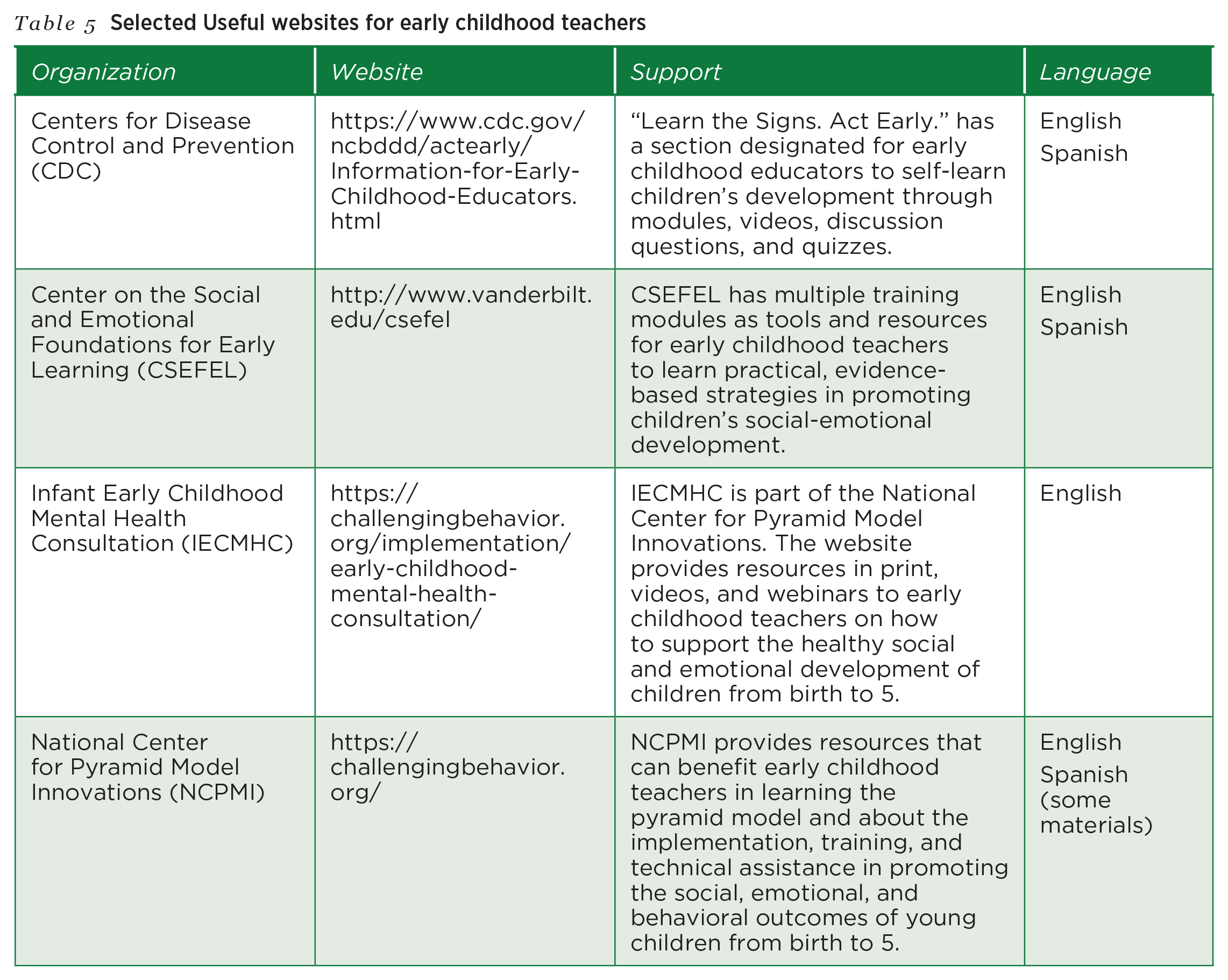
With the resources in place, Nicole can easily navigate these websites and access the training modules and materials to increase her knowledge and skills in promoting the social-emotional development of John and other children in her classroom. She first went through the training modules of CDC’s “Learn the Signs. Act Early.” to review children’s developmental milestones. Next, Nicole studied the materials in multiple formats (print, videos, case studies, activities) in CSEFEL and NCPMI to meet her learning needs. She further gained knowledge of the research underlying the training modules and practiced hands-on, evidence-based strategies. She also had an opportunity to attend the professional development training of the pyramid model at the program or state level.
All the resources are available for teachers like Nicole, who is a novice and eager to support children’s mental health. With the ongoing data collection to monitor children’s progress and continued consultation with mental health consultants, other professionals, and families, early childhood teachers support children’s social and emotional development through collaborative efforts.
Concluding Thoughts
Young children’s aggressive challenging behaviors and emotional distress that result in mental health concerns have called for the need for promoting the social-emotional development of these young children and accessing support for families. Children are vulnerable, and factors such as family crises and trauma may impact their mental health. In this article, we focus on children who show signs of mental health needs that are typically related to social-emotional development and behaviors that are frequently observed in early childhood settings, such as aggressive behaviors and noncompliance. Children with disabilities are particularly vulnerable due to the impact of disability on regulating emotions and managing behaviors and the difficulty of diagnosing mental health issues at a young age. Learning the deviation of children’s behaviors from the typical social-emotional development helps a novice early childhood teacher like Nicole to identify a child who may need mental health support early. Regular developmental and behavioral screenings, especially with a focus on social-emotional development, help teachers to make a referral for children who need further evaluation or continue to document children’s development. The provision of school-based mental health supports and the ongoing monitoring of children’s responses to those supports inform instructional decisions and what additional support children with disabilities need. Partnering with families, teaming with mental health consultants and other professionals, and securing additional resources can support teachers in early childhood programs to address the mental health needs of young children. Teachers like Nicole are not alone, but adopting the six strategies presented may pave the road to supporting the sound mental health development of children with special needs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.