
Abstract
This manuscript offers an approach to secure needed SBMHS for students with disabilities through unique applications within the IEP development process, informed by an analysis of recent case law. We will discuss six components of this approach. First, the need for SBMHS must be established through evaluation data. Data sources to confirm the need for services include record review, interview, observation, and testing. Second, the evaluation data must be presented in the Present Level of Academic Achievement and Functional Performance (PLAAFP) section of the IEP. This section will also describe how a child’s educational performance is adversely affected by mental health issues. Third, annual goals must be developed for areas adversely affected by a child’s mental health status. The goals must be measurable and include performance targets established by criteria and matched to the baseline data and skills targets for intervention. Fourth, the specially-designed instruction (SDI) and related service intervention (RSI) must be planned for each goal area. The SDI must specify the methodology and strategies to be provided to address the child’s mental health needs. The RSI must explicitly describe the nature of the strategies or approaches planned. Fifth, progress monitoring plans must be described, including the metrics matched to baseline data and the goal, a timetable, and reporting options. Sixth, and importantly, the IEP SBMHS must be implemented as planned and revised if progress toward the goals is not satisfactory. One unique contribution of this IEP approach to securing needed SBMHS is the integration of recent case law to illustrate how courts relied on specification of the six components in confirming the need for SMBHS. A second contribution is providing specific examples of IEP statements for the six components when mental health needs must be addressed.

Despite an increasing need for school-based mental health services (SBMHS) for students with disabilities, the provision of those services is inadequate and insufficient (Becker et al., 2019). The failure to provide SBMHS is attributed to insufficient training, lack of administrative support, limited personnel to provide services (Castillo et al., 2017), and disparities across geographic locations and available resources (Sanchez et al., 2018). Disparities in age also exist, with beliefs that mental health needs in early childhood are transient and do not persist (Holland et al., 2017) despite data indicating the continuance of mental health issues in later grades. Skaar et al. (2021) proposed three additional factors influencing the lack of SBMHS to students with disabilities: (a) failure of individualized educational program (IEP) teams to recognize SBMHS as a related service available under the Individuals with Disabilities Education Act (IDEA; 1990), (b) failure of the IDEA to include the assessment of mental health needs in the evaluation provisions, and (c) the poorly conceptualized and fragmented approach to the assessment and provision of SBMHS. These factors present enormous challenges to IEP teams responsible for developing IEPs for students with mental health needs, with failure to provide needed SBMHS resulting in litigation.
The purpose of this article is to offer a six-step approach, informed by an analysis of related case law, to secure needed SBMHS for students with disabilities. Case law interprets legal requirements and standards for services, in this instance for SBMHS. Case law is a resource to local education agencies (LEAs) in designing programs and services and avoiding due process hearings and court cases in which LEAs are unlikely to prevail because of previous legal precedents. We discuss six components:
• establishing a need for SBMHS through evaluation data (e.g., gathering information from the instructional, curriculum, environment, and learner [ICEL] domains through record review, interview, observation, and testing [RIOT]);
• presenting evaluation data in the Present Level of Academic Achievement and Functional Performance [PLAAFP] section of the IEP, including a description of how a child’s educational performance is adversely affected by mental health issues;
• developing annual goals for areas adversely affected by a child’s mental health status;
• planning for specially designed instruction (SDI) and related service intervention (RSI) for each goal area specifying the methodology and strategies to be provided to address the child’s mental health needs;
• developing monitoring plans that include the metrics matched to baseline data, the goal, a timetable, and reporting options;
• implementing the IEP SBMHS as planned and revising if progress toward goals is not satisfactory.
Component 1: Establish the Need for SBMHS Through Comprehensive Evaluation Data
The IDEA (1990) requires evaluation data for an IEP be collected “to determine whether a child is a child with a disability and to determine the educational needs of such child” (20 U.S.C. § 1414[a][1][C]). The evaluation must use a variety of assessment tools and strategies, assess the child in all areas of suspected disability, and assist in determining the educational needs of the child (IDEA, 1990; 20 U.S.C. § 1414[b][2]). The evaluation informs the selection of services and interventions to be provided to the student. Student progress is ensured when IEPs are based on quality evaluation data (Yell, et al., 2020a). An evaluation can occur when a young child transitions from Part C (birth to 3 years/early intervention) to determine eligibility under Part B (3–21 years/preschool services) of the IDEA or any time during a child’s educational career.
Use the ICEL/RIOT matrix to assist in organizing data from multiple sources and investigating likely explanations for academic or behavioral health needs (Hosp, 2006). These tools guide the analysis of the influences on student performance and the child’s mental health status by gathering in the ICEL domains through the use of reviews or records (past and present); interviews with teachers, other school personnel, students, and their families; systematic direct observations; and tests (RIOT) to evaluate underlying causes of a problem and to validate a hypothesis (Christ, 2008).
Culturally responsive ICEL/RIOT assessments should consider the unique characteristics of culturally and linguistically diverse (CLD) students in determining the need for SBMHS. Such individualization will ensure the assessment meets the requirements of the IDEA (1990) specifying that evaluation materials are not discriminatory on a racial or cultural basis and are administered in the language and form most likely to yield accurate information (20 U.S.C. § 1412 [a][6][b]).
Review past and present data, including report cards, past evaluation reports (including independent educational evaluations [IEEs] secured by parent; IDEA, 1990, 34 C.F.R. § 300.502), universal screening data, student attendance and disciplinary records, state and district test results, student work samples and charts, and previous intervention data to identify both externalizing and internalizing behaviors because these data may alert school personnel to suspect a child has a disability requiring SBMHS. Externalizing behaviors are those that involve outward conflict and may be described as undercontrolled (Whitcomb, 2018). Externalizing behaviors may include verbal or physical aggression, oppositional behavior, hyperactivity, or delinquent behavior. Internalizing problems are problems within the individual or those behaviors that are overcontrolled (Whitcomb, 2018), such as anxiety, depression, or withdrawal.
Locate, select, appraise, and synthesize the data contained in various documents that are indicators of a child’s mental health status. A review of student records may reveal trends over time and provide insights into culturally relevant patterns over time (Hass & Leung, 2021).
Patterns to look for include:
• significant changes in academic performance, behavior, and/or social interactions, and previous intervention data;
• a decline in academic outcomes over time;
• changes in attendance.
Interview students, caregivers, teachers, or other service providers to examine behavioral patterns in different settings; include perspectives on the student’s strengths and current supports and barriers to their personal, interpersonal, and academic adjustment (Alshenqeeti, 2014; McConaughy & Ritter, 2014). The skillful questioning of children and other stakeholders is essential in gathering assessment-relevant information and informing intervention decisions (Kiyimba & O'Reilly, 2018). When evaluating younger children, interviewing the child’s caregiver, who is primarily responsible for tending to the child’s needs in all developmental areas, is necessary (Kruithof et al., 2020).
During the interview, determine a cultural definition of a student’s mental health problems and needs as well as a cultural perception of the cause, context, and support (Hass & Abdou, 2019). The interview should ensure shared understanding and agreement of the child’s needs and assess the child’s cultural identity and acculturation (Dennison et al., 2019). When interviewing CLD students and families, collaborate with interpreters and seek consultation with other professionals. The interpreter may assist in acquiring data regarding the student’s language status and developmental history (Cho & Kraemer, 2020).
Clinical interviews vary in structure, and those with more structure typically result in more accurate diagnostic information (Garcia-Barrera & Moore, 2013; Mueller & Segal, 2015). If structured interviews are not practical due to the lengthy administration time and a focus on diagnoses (Benson et al., 2019; Whitcomb, 2018), then use semistructured diagnostic interviews, developmental history interviews, unstructured interviews with students, and problem-solving interviews with teachers and caregivers (Benson et al., 2019).
Observe a child’s academic and behavioral performance (Cash & Pianta, 2014). As seen in the Table 1 case, systematic direct observation of the student’s classroom behavior is one of the most common assessment methods employed by school personnel (Lee et al., 2011; McConaughy et al., 2009). Systematic observation is frequently used to collect data and to screen and diagnose emotional and behavioral problems of children (Volpe et al., 2005). Published observation instruments such as the Behavior Observation of Students in Schools (Shapiro, 2003) or the Behavior Assessment Scale for Children, Third Edition (BASC-3 Student Observation System; Reynolds & Kamphaus, 2015) can be used, or other systematic direct observational tools such as event or interval recordings, duration recording, time sampling may be used (Miller et al., 2018). Multiple observations are needed to produce quality data about behavior. The appropriate selection of interval and observation length can also improve the quality of the observation data (see Ferguson et al., 2018). Targets for observation may include a student’s academic engagement time; performance during large group, small group, and independent work; interactions between the student and teacher or peers; or environmental factors such as rules, traffic, distractions, routines, or daily maps. Also, because mental health in early childhood is often discussed within the context of caregiving relationships (Zeanah & Zeanah, 2019), a target for observation when evaluating young children includes the interactions between the parent and child to gain information about the parent-child relationship (Larrieu et al., 2019).
ICEL/RIOT Matrix Example for Compton Unified School District (2015) Case
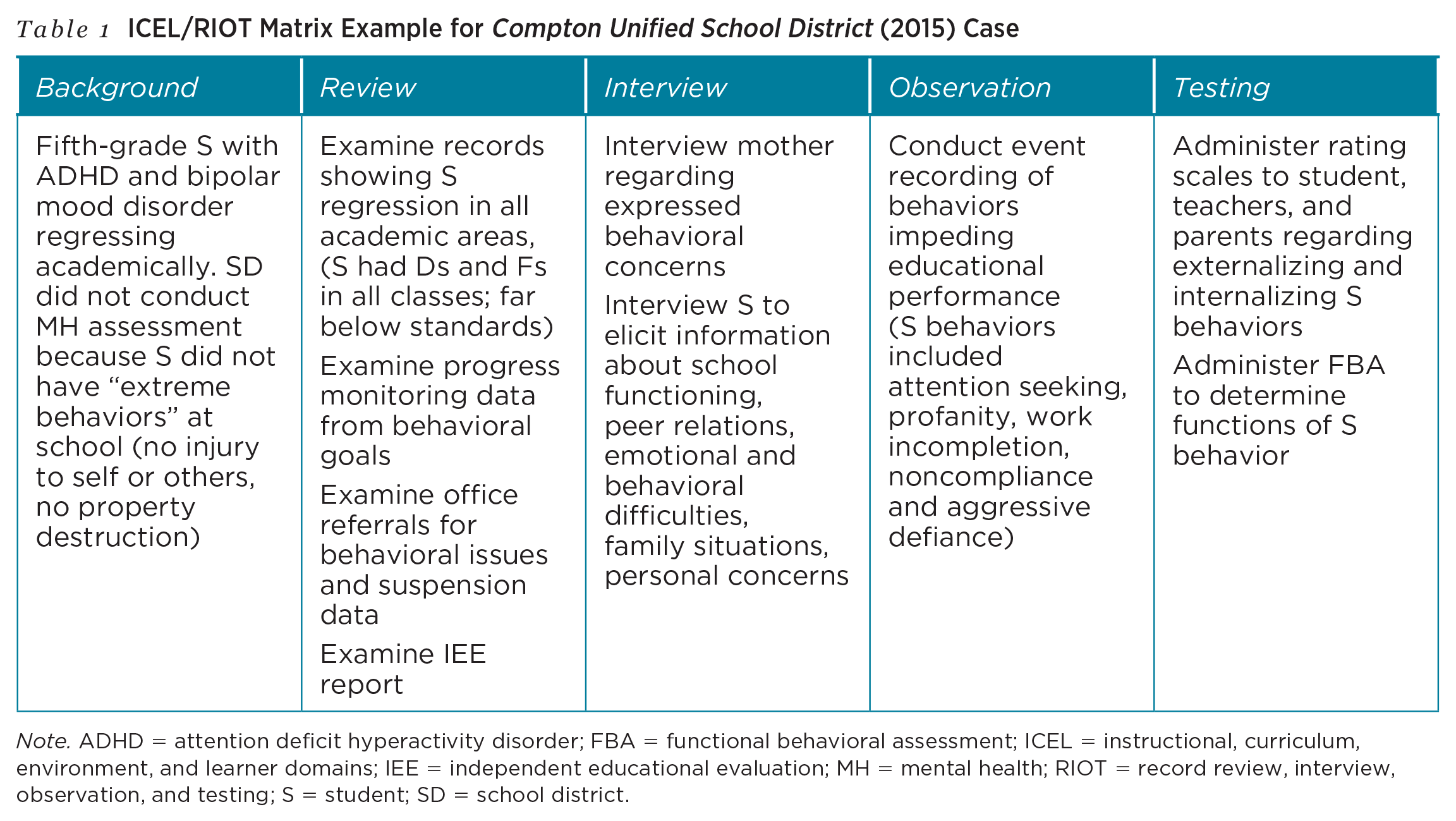
Note. ADHD = attention deficit hyperactivity disorder; FBA = functional behavioral assessment; ICEL = instructional, curriculum, environment, and learner domains; IEE = independent educational evaluation; MH = mental health; RIOT = record review, interview, observation, and testing; S = student; SD = school district.
Mental health symptoms can be expressed differently for CLD students, making traditional tools questionable for determining SBMHS (DeBoer et al., 2022). In observation, students might conform to behaviors and values consistent with the majority culture rather than demonstrating sensitivity to students’ unique cultures (Fong et al., 2016). Cultural responsiveness in observation “stresses the importance of focusing on the individual and the distinct intersecting cultural variables impacting the individual’s behavior . . . and highlights the importance of identifying aspects of the environment (i.e., cultural variables) that impact behavior” (Jimenez-Gomez & Beaulieu, 2022, p. 2). Peer comparative data regarding behavior must be carefully analyzed through a lens of cultural distinctions and similarities.
Test for SBMHS. Skaar et al. (2021) proposed a three-dimensional model to guide the assessment and intervention development of SBMHS for students with disabilities. When data suggest the need for further mental health assessment, the selection of appropriate assessment tools should be informed by student need and adequate level of reliability and validity (Moskowitz et al., 2017).
Include multiple informants who are familiar with the student’s behavior. Moreover, the correlation between the presence of internalizing and externalizing problems suggests beginning with a broadband tool that assesses both is prudent (Achenbach et al., 2016). Examples of assessment systems that can be used to obtain ratings from a student, teachers, and parents and also assess for internalizing and externalizing problems include the Achenbach System for Empirically Based Assessment (e.g., Achenbach & Rescorla, 2001) and the BASC-3 (Reynolds & Kamphaus, 2015). Discrepancies in ratings are common due to context and rater variability and should be explored instead of disregarded. Decades of research indicates greater consistency in ratings of externalizing behavior than internalizing behaviors. Greater consistency also occurs when informants observe the child in the same setting and when the assessments are dimensional (e.g., ratings of severity or frequency of behavior) instead of categorical (yes, the behavior occurs or no, it does not; De Los Reyes et al., 2015). Consider the research on multiinformant assessment in the data interpretation process to make sense of differing results.
Linguistic bias and content bias associated with tests or assessments may contribute to misinterpretations (Newkirk-Turner & Johnson, 2018) and fail to assist in determining a student’s SBMHS needs. Recognize unique culturally relevant linguistic variables when assessing CLD students’ social and emotional functioning (Garcia-Joslin et al., 2016).
“The need for SBMHS is established through a multimethod evaluation.
The need for SBMHS is established through a multimethod evaluation. Several recent cases highlight the importance of establishing the need for SBMHS through evaluation data.
In Burbank Unified School District (2014), the school district’s data collection and analysis supported the need for parent and student counseling. In A.G. v. District of Columbia (2011), the failure to conduct a timely observation of a student with emotional and behavioral disorders resulted in an IEP that did not include needed counseling services, social work services, psychological services, and parent counseling services. Deteriorating academic performance in Compton Unified School District (2015) and High Tech High (2013) should have triggered a mental health assessment. Without evaluation data, appropriate goals could not be developed or appropriate SBMHS provided.These cases illustrate that the first step we recommend in securing needed SBMHS is the collection and analysis of data that show how a student’s mental health status is adversely affecting educational performance. The evaluation should include school-based RIOT data, including data from IEEs obtained by the parent. An example of the ICEL/RIOT evaluation matrix for the student in the Compton Unified School District (2015) case is presented in Table 1. Once collected and analyzed, the data must be presented in the PLAAFP.
Component 2: Presenting Data in Level of Academic Achievement and Functional Performance
Summarize evaluation data from the ICEL/RIOT matrix and include in the PLAAFP section of the IEP. The IDEA (1990) requires each child’s IEP includes a statement of the child's PLAAFP, including how the child's disability affects the child's involvement and progress in the general education curriculum (20 U.S.C. § 1414[d][1][A][i][I]). The PLAAFP provides a “needs-based” rationale for SBMHS (Patti, 2016; Spiel et al., 2014) and a baseline by which IEP teams can write annual goals and monitor student progress (Yell et al., 2016). Failure to address all of a student’s needs in their PLAAFP statements is a common substantive violation of IEP development (Yell, et al., 2020a). The PLAAFP must be comprehensive and provide data from current and previous multimethod, multisource evaluations, including data documenting the student’s progress toward previous IEP and related service goals (Capizzi, 2008; Harmon et al., 2020). The PLAAFP must contain detailed student assessment and performance data so IEP teams can develop goals (Couvillon et al., 2018), which include specific criteria for progress monitoring.
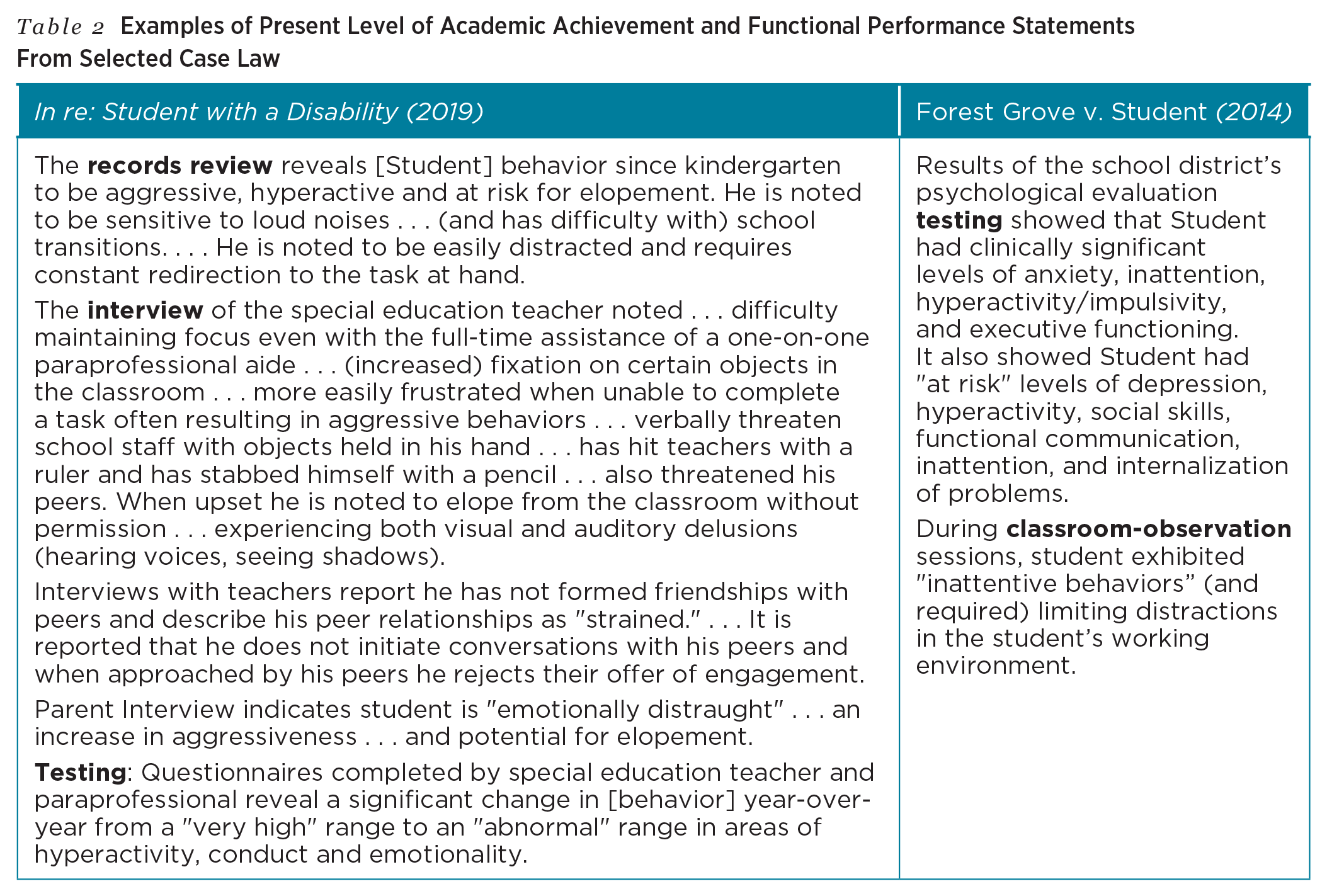
A PLAAFP for students with mental health needs must present and prioritize data to demonstrate the need for SBMHS. Case law illustrates how courts relied on PLAAFP data to determine the need for SBMHS.The school district in In re: Student with a Disability (2019) collected data from a review of records, interviews, and observations to justify placement at a special day school with intensive counseling for a 9-year-old student with autism. In Forest Grove v. Student (2014), the evaluation data reported in the PLAAFP showed the need for SBMHS for a student with autism with significant levels of anxiety. Excerpts from the PLAAFP for students in both cases are presented in Table 2.
Examples of Present Level of Academic Achievement and Functional Performance Statements From Selected Case Law
These cases reveal presenting data indicative of need in the PLAAFP an important step in securing SBMHS for students with disabilities. See Table 3 for examples of statements for the PLAAFP. IEP teams should identify both the strengths and concerns for both academic and functional performance of the student because mental health needs may adversely affect both curricular progress and social/emotional/behavioral status. The PLAAFP must provide prioritized statements of a student’s needs so goals and SBMHS may be developed and provided.
“The PLAAFP must provide prioritized statements of a student’s needs so goals and SBMHS may be developed and provided.
PLAAFP Examples
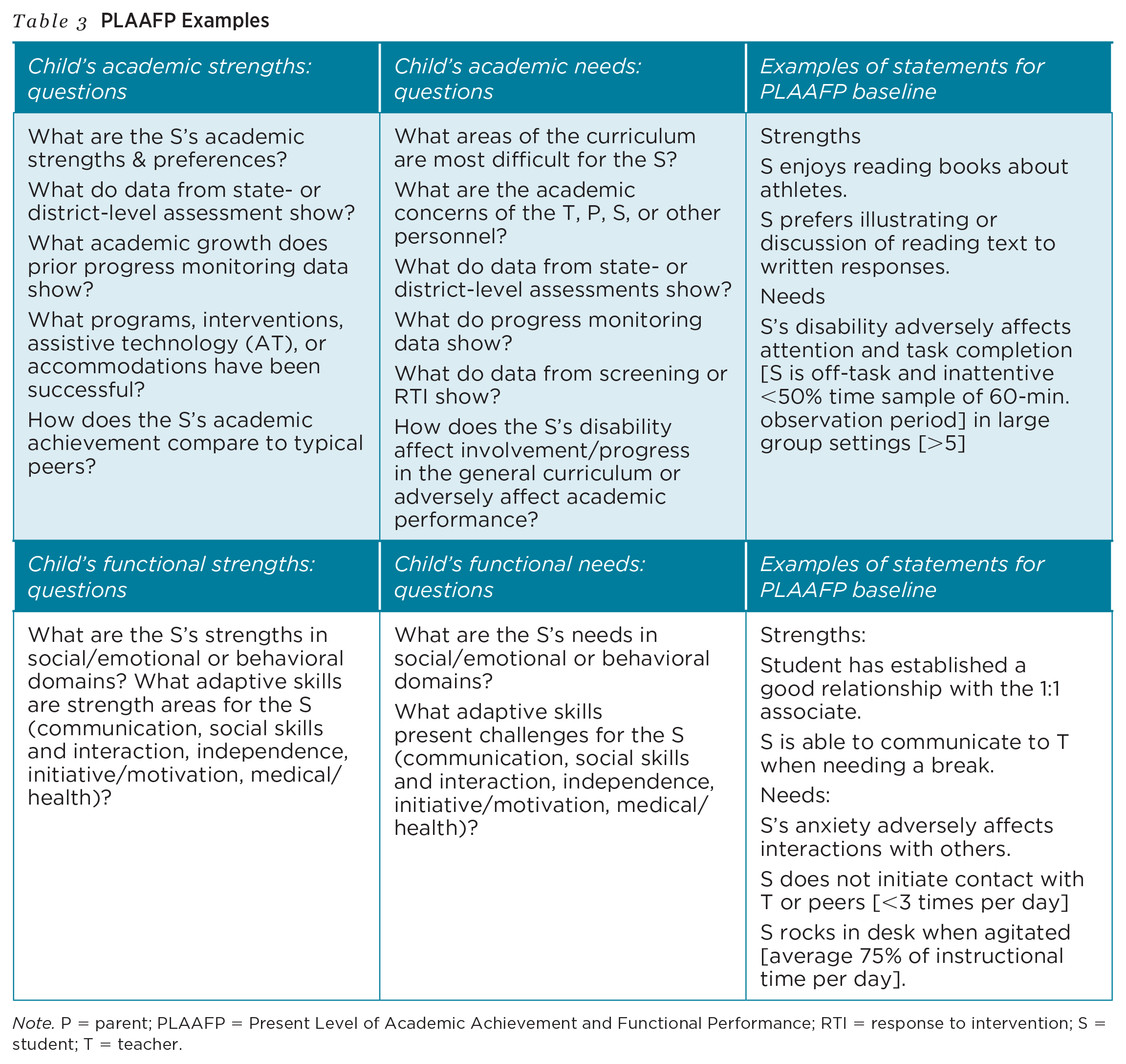
Note. P = parent; PLAAFP = Present Level of Academic Achievement and Functional Performance; RTI = response to intervention; S = student; T = teacher.
Component 3: Developing Annual Goals
IEP teams must examine data presented in the PLAAFP to guide the development of annual goals to enhance and improve the child’s academic, social, or emotional status. The IDEA (1990) requires IEPs include a statement of measurable annual goals, including academic and functional goals, designed to (a) meet the child's needs that result from the child's disability and (2) enable the child to be involved in and make progress in the general education curriculum (20 U.S.C. § 1414[d][1][A][i][I]). Write one goal for each area of identified educational need described in the PLAAFP, beginning with the baseline data from the PLAAFP (Goran et al., 2020). Annual goals show the direct relationship between the PLAAFP data and the student’s learning needs (Kowalski et al., 2009) and guide daily implementation of the IEP (More & Barnett, 2014). Essential components to annual goals are: (a) a time frame, (b) conditions under which the skill/behavior is expected, (c) a specific description of the skill/behavior, (d) how the skill/behavior will be measured, and (e) the criterion against which progress will be measured (Capizzi, 2008; Marx & Miller, 2020). Rather than only focusing on decreasing negative behavior (e.g., disruptive behavior, aggression), IEP goals should focus on increasing the alternative or replacement behavior/skill (Marx & Miller, 2020), which in turn will reduce the problem behavior. For example, if a student is demonstrating aggressive behavior toward peers, the IEP could include a goal that increases the use of a learned de-escalation strategy, therefore decreasing aggressive incidents.
Annual IEP goals often fail to address needs identified in the PLAAFP. Spiel et al (2014) indicated “even though these areas of need are recognized, close to half of IEPs contained no goals for improving these behaviors” (p. 461). Develop ambitious, individualized, and measurable annual goals to address the student’s mental health needs (Yell et al., 2020a).
IEP annual goals for students with mental health needs must set targets for academic, social, or emotional improvement. Several cases illustrate the relationship between a student’s need for SBMHS and the annual goals of the IEP (i.e., Component 3).
In Sacramento City Unified Sch. Dist. v. R.H. (2016), the district court concluded that because a student’s IEP included social/emotional goals, more intensive SBMHS were required than what the district proposed. Both in Castro Valley Unified School District (2015) and in North Hills School District (2010), school districts failed to develop goals and provide services to address the students’ social-emotional needs and challenging behavior.
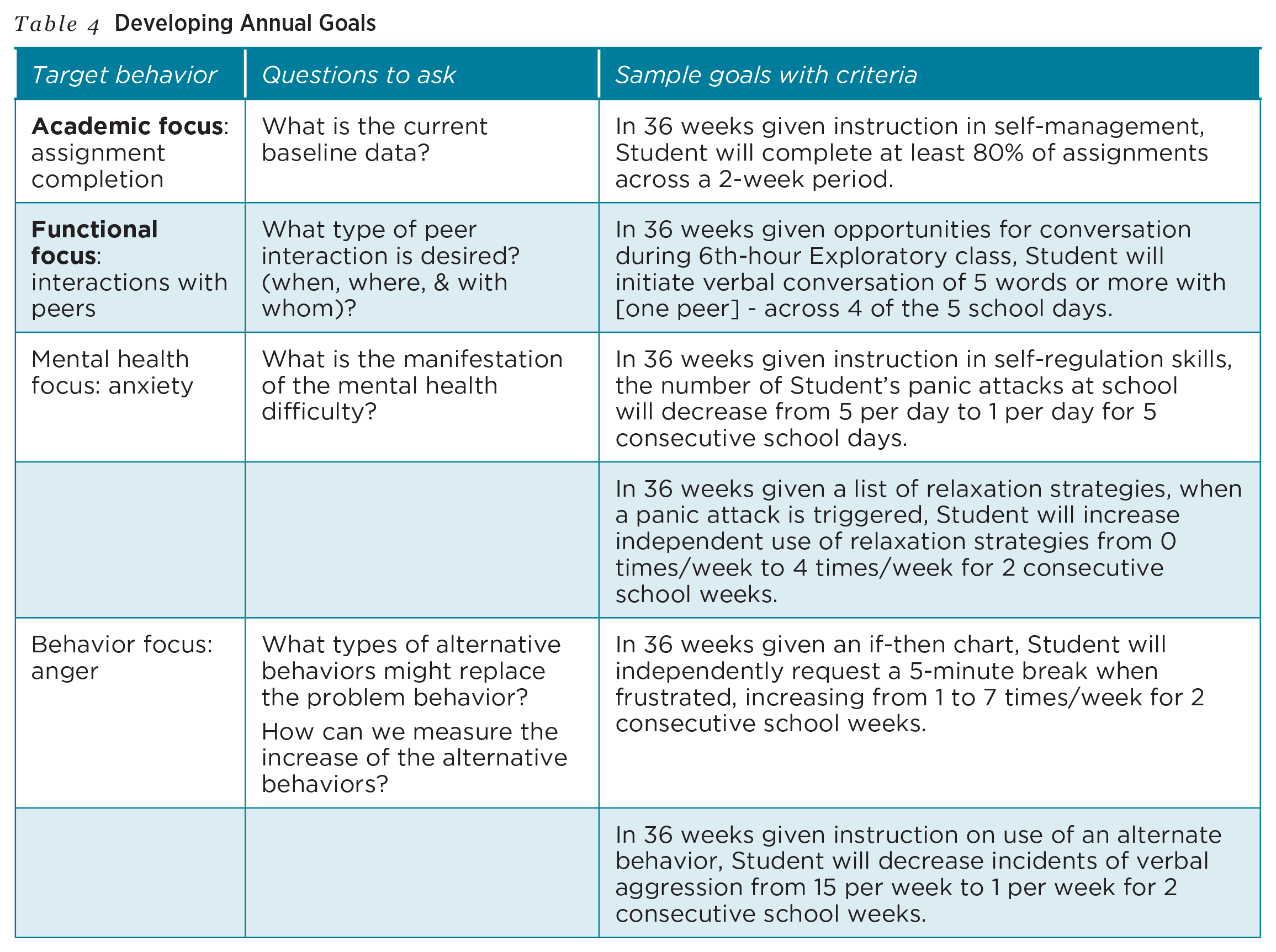
These cases illustrate when evaluation data reveal the need for SBMHS, the IEP team must develop goals to address the student’s academic, social, and emotional needs. See Table 4 for examples of statements for social-emotional annual IEP goals for students. Follow the SMART framework for writing IEP goals: specific, measurable, achievable, relevant, and time-bound (Hedin & DeSpain, 2018). Goals may target decreasing inappropriate behavior but should also target increasing or improving adaptive or alternative-appropriate behaviors.
Developing Annual Goals
Component 4: Planning Specially Designed Instruction or Related Service Intervention
SBMHS in the IEP may be conceptualized as specially designed instruction (SDI) or as a related services intervention (RSI), or a combination of both SDI and RSI. SDI involves adapting the content, methodology, or delivery of instruction to address the unique needs of the child (IDEA, 1990; 34 C.F.R. § 300.39[a][3]). SDI may include social, emotional, or behavioral content intended to develop appropriate, alternative skills for students with mental health needs. Examples include social skills, relaxation strategies, or coping skills instruction.
Related service interventions include psychological services, social work services, and counseling services (IDEA, 1990, 20 U.S.C. § 1402[26]). As a related service available under the IDEA (1990), (Etscheidt, 2002) counseling services are defined as services provided by qualified social workers, psychologists, guidance counselors, or other qualified personnel (34 C.F.R. § 300.34[c][2]). Federal law and regulations do not further define counseling or therapeutic services, but they can be defined as a “set of interventions designed to promote the social, emotional, and behavioral well-being of children and adolescents” with identified “goals and objectives” (Plotts & Lasser, 2020, p. 5).
“SBMHS in the IEP may be conceptualized as specially designed instruction (SDI) or as a related services intervention (RSI), or a combination of both.
SBMHS included in an IEP are individualized interventions, distinguished from schoolwide, class-wide, or general education interventions. The IEP should identify SDI or RSIs to address the goal areas identified. The specific method, strategy, or intervention must be described in detail to inform instructional decisions and monitor intervention fidelity. Importantly, the SBMHS must be based on peer-reviewed research to the extent practicable (IDEA, 1990, 20 U.S.C. § 1414[d][1][A][i][IV]).
Select SBMHS from a variety of sources, based on the evaluation, student need, and the intervention target goal (e.g., reduce anxiety, depression, attention deficit hyperactivity disorder, disruptive behavior; improve task engagement, interactions, self-control). Existing databases offer mental health providers information on current evidence-based interventions. The PracticeWise Evidence-Based Services Literature Database (PracticeWise, 2014) was developed to summarize and support selection of evidence-based mental health services.
SDI led by a special education teacher might include academic supports as well as social-emotional and behavioral supports. For example, a student with depression may be struggling to keep focus on schoolwork and may be falling behind with assignments. SDI for this student may include teaching the student self-monitoring strategies for maintaining attention to tasks. A student who is struggling behaviorally due to past trauma might also be struggling socially, and the SDI might include social skills instruction from special educators and collaboration with general education teachers to support for social interaction in the general education classroom.
RSI provided by a school psychologist or school social worker may be added to the IEP when the need for mental health services requires additional, specialized intervention. RSI is often combined with the SDI provided by the special education teacher. A school psychologist might provide counseling services (RSI) to teach strategies to improve positive self-talk and eliminate negative thoughts while the special education teacher works with the student daily to use those strategies during the school day (SDI). A school social worker might provide relaxation techniques and later model the intervention for the special education teacher (RSI), who continues that intervention as SDI. In another example, the school psychologist might start an intervention with a student to teach problem solving and anger management skills (RSI), with the special education teacher partnering to facilitate the intervention in the classroom (SDI). The selection of the SBMHS instruction/intervention must be a collaborative decision by all members of the IEP team, including the parents (Yell et al., 2020b).
Case law illustrates examples of SDI and RSI provided to students requiring those interventions. In Barrington Borough Bd of Ed (2002), the court concluded a 10-year-old student with autism required individual play and talk therapies as RSI to address internal and external conflicts. In Augusta Public School (2009), a high school student with other health impaired required counseling services as RSI, as did the 11-year-old with ADHD and anxiety in Ross Valley School District (2014). These cases illustrate once IEP goals are developed, the IEP team must specify the SDI and/or RSI necessary to enable the student to make progress toward those goals—Component 4. Table 5 includes examples of special education services included in the IEP (i.e., SDI, RSI).
School-Based Mental Health Services as SDI and RSI in the IEP.
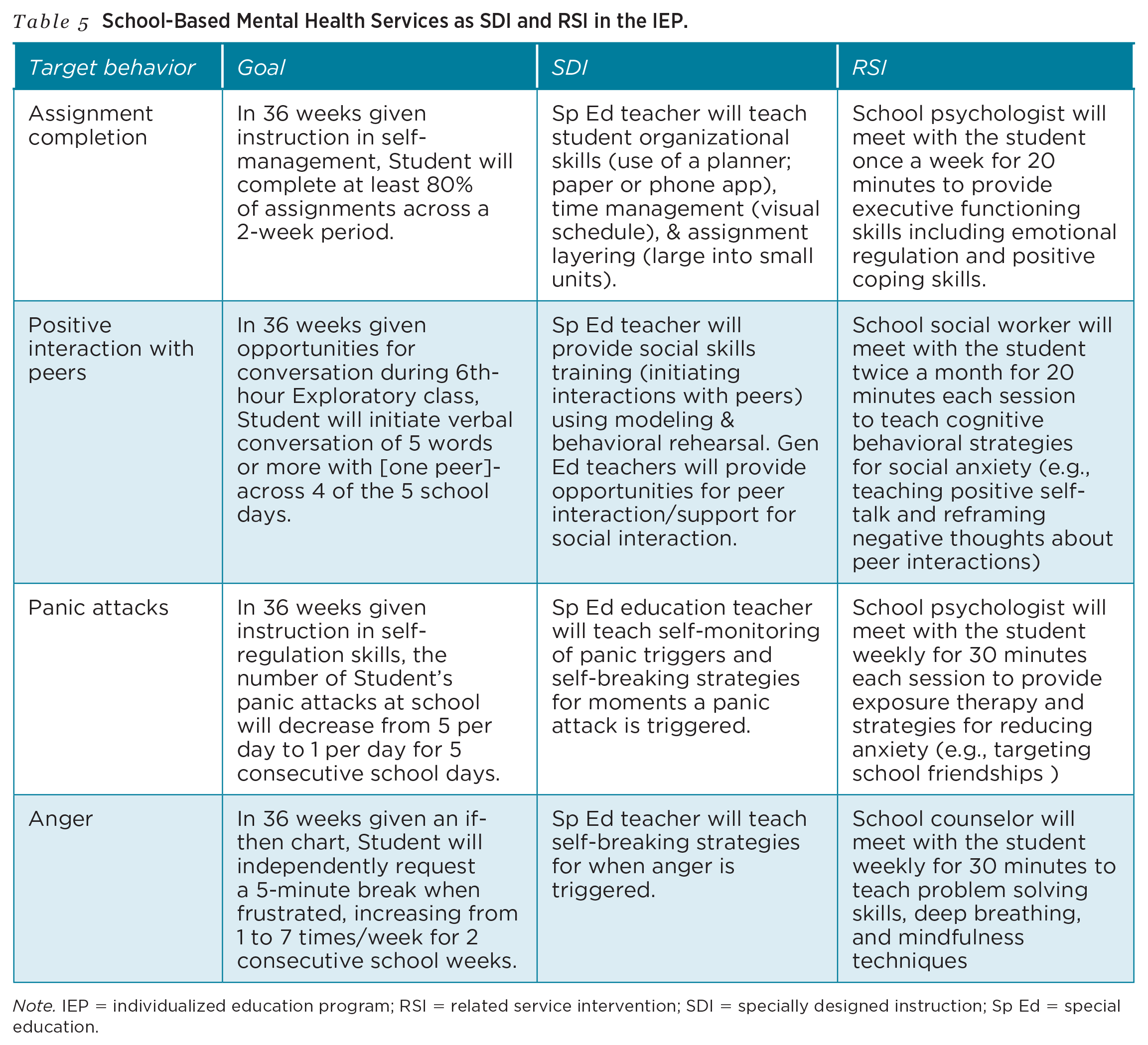
Note. IEP = individualized education program; RSI = related service intervention; SDI = specially designed instruction; Sp Ed = special education.
Component 5: Describing Progress Monitoring Plans
The IDEA (1990) requires a child’s IEP include a description of how the student’s progress toward meeting annual goals will be measured and when periodic reports on the progress the student is making toward meeting the annual goals will be provided (20 U.S.C. § 1414[d][1][A][i][III]). Yell et al. (2020a) found a common substantive violation of IEP development was the failure to measure a student’s progress toward their annual goals.
Progress monitoring measures should be connected to the IEP goals and the target behaviors, which means often the behavior of concern and the alternative behavior/skill will both be measured (Marx & Miller, 2020). The observation tools used to collect evaluation data in Component 1 may be appropriate tools for progress monitoring. For example, if time sampling was used to gather data regarding a student’s on-task engagement in the evaluation, time sampling might continue as a progress monitoring tool to determine if selected SDI and RSI interventions are, indeed, improving on-task engagement. Progress monitoring data informs decisions about whether interventions should be maintained or changed (Chafouleas et al., 2010). In addition to student outcome data, progress monitoring should include data about the intervention, such as when and how the intervention was delivered (Bickman et al. (2016). The IEP team may determine that extending the time of the SDI or RSI is needed.
In addition to systematic direct observation, questionnaires and rating scales may also be appropriate for frequent use in school settings (Dart et al., 2019; Joyce-Beaulieu & Sulkowski, 2015). Table 6 includes three of the most commonly utilized methods. Progress monitoring cognitive and behavioral skills that are taught as part of SDI or RSI may be a good indication of student growth. For example, a student may have no methods of reducing anger when the intervention begins, but after 8 weeks of intervention provided by the school psychologist, the student can demonstrate two strategies independently as evidenced in progress monitoring data. For students who experience distress due to depression, anxiety, or trauma, the school psychologist may use subjective units of distress (SUDs) for progress monitoring the RSI. SUDs are a student self-report of their current level of distress on a defined scale (e.g., 1–100 or 1–10). Progress monitoring tools for recording a decrease in internalizing or externalizing behaviors or for recording an increase in alternative appropriate behaviors are provided in the Table 6 (including information about format, rater, frequency, and possible target behaviors aligned with IEP goals).
Progress Monitoring Tools for School-Based Mental Health Services in IEPs
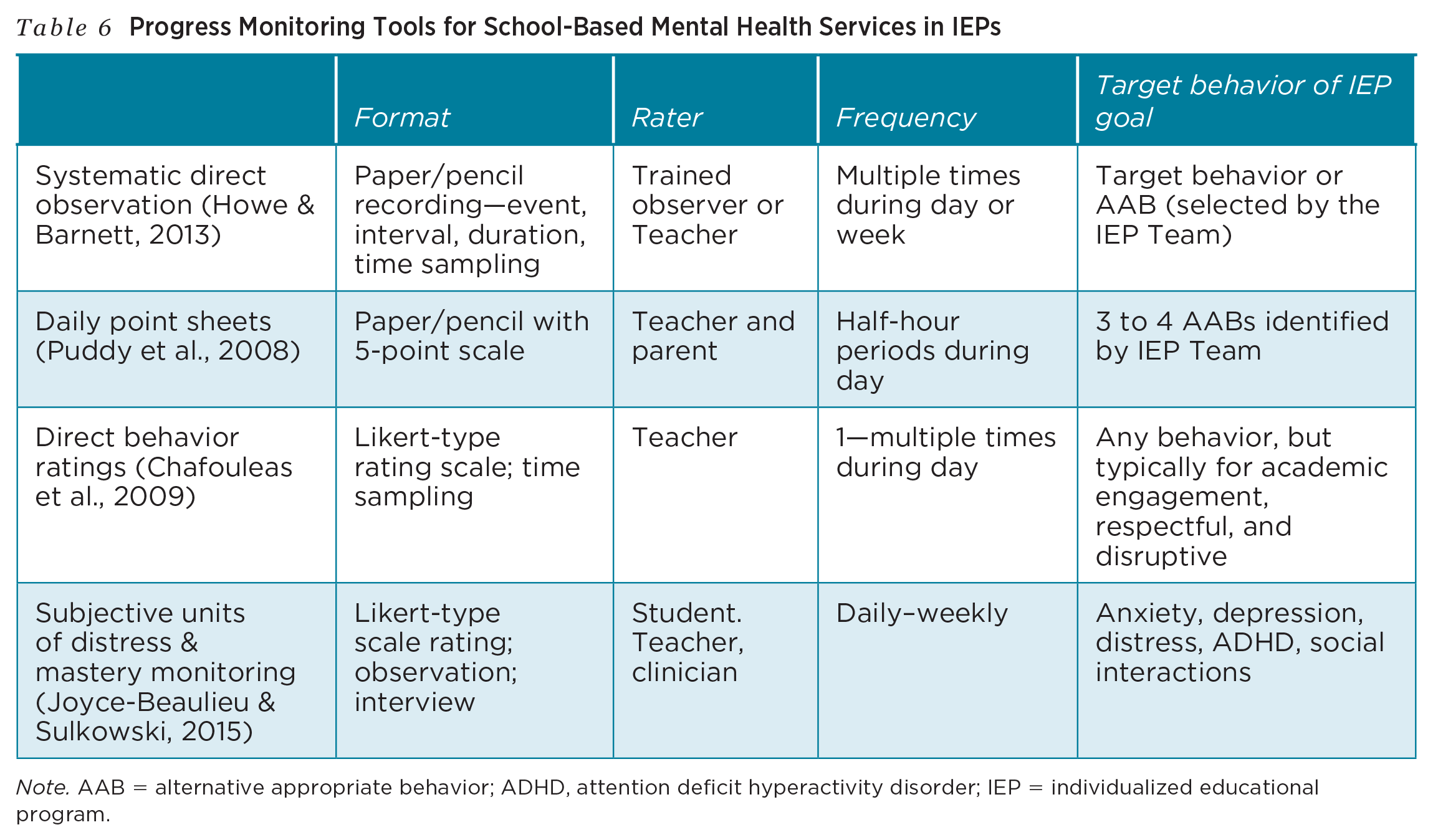
Note. AAB = alternative appropriate behavior; ADHD, attention deficit hyperactivity disorder; IEP = individualized educational program.
G. S. v. New York City Department of Education (2016) illustrates the importance of collecting progress monitoring data. Whereas parents of a 9-year-old student with autism requested the school district provide music therapy as a SBMHS, the school district proposed more general counseling. The court concluded the progress monitoring data confirmed the school’s provision of SBMHS was appropriate based on psychoeducational evaluations and progress monitoring data from observations that revealed the student was benefitting from the district’s counseling, as evidenced in her verbal communication and purposeful participation in social/emotional interactions with others.
Component 6: Implementing the IEP SBMHS With Fidelity and Revising if Progress Is Not Satisfactory
Following the development of the IEP, the SBMHS must be implemented as planned and monitored to ensure student progress and the fidelity of the instruction/intervention. The IDEA (1990) requires the IEP team reconvene to review the IEP “periodically, but not less frequently than annually, to determine whether the annual goals are being achieved and to revise the IEP to address any lack of expected progress toward the annual goals” (20 U.S. C. § 1414[d][4][A]). IEP teams should utilize progress monitoring data in determining student progress toward goals and also monitor the fidelity of the instruction or intervention provided.
Intervention fidelity is the delivery of an intervention or program as designed (Swanson et al., 2013). The IDEA “galvanized interest” in fidelity by requiring educators to implement evidence-based practices (Capin et al., 2018, p. 886). Fidelity assessment can enhance the content, process, and outcomes of interventions (deVos et al., 2013) and is strengthened by clear and specific descriptions of the intervention, adequate training and feedback, and frequent monitoring of intervention delivery (Corley et al., 2016; Suhrheinrich, 2016). Instructional coaching by professionals to teach the implementation of SBMHS may assure and maintain intervention fidelity (Gilmour et al., 2017).
Importantly, student engagement with the intervention, student use of intervention skills in daily life, and improved student outcomes depend on both intervention fidelity and intervention effectiveness (Fixsen et al., 2013; Gearing et al., 2011). SBMHS providers must determine and specify plans not only for progress monitoring but also for determining instructional and intervention fidelity.
The importance of intervention monitoring proposed as Component 6 is illustrated in several cases.Failure to provide the SBMHS identified in the IEP resulted in violations of the IDEA in Omidian v. Bd of Ed New Hartford Central SD (2009), McMinnville School District (2019), and Roxanne J. v. Nevada County Human Services Agency (2006). As a result, the students’ social and emotional problems intensified and significantly impacted learning. The failure to revise SBMHS as needed was illustrated in Dayton Public Schools (2019), where the failure to reconvene the IEP team or revise the IEP to address the student’s increasing behavioral problems violated the IDEA.
By monitoring both student progress and instructional or intervention fidelity, IEP teams can determine if changes to the SBMHS are warranted. Based on monitoring data, modifications to the content of the instruction/intervention, intensity of exposure to the instruction/intervention, or delivery of the instruction/intervention may be proposed.
“By monitoring both student progress and instructional or intervention fidelity, IEP teams can determine if changes to the SBMHS are warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.