
Abstract
The IDEA requires schools to evaluate and provide services to students who have a mental health issue that is deemed an educational disability or a mental health issue that is comorbid with an educational disability. Etscheidt and colleagues (this issue) propose a six component approach to securing school-based mental health services for students with disabilities. This article illustrates the six component approach using two vignettes. The first vignette involves a preschool student referred due to aggression who has not been previously identified as eligible for special education. The second vignette involves a 5th grade student who was receiving special education services under the category of SLD who’s academic progress had plateaued.

The prevalence of mental health issues in children and youth has continued to increase for the last 5 decades (Herman et al., 2021), yet the percentage of students receiving special education services under the category of emotional disturbance (ED) has declined (Mitchell et al., 2019). The Individuals with Disabilities Education Act requires schools to evaluate and provide services to students who have a mental health issue deemed an educational disability or one that is comorbid with an educational disability. Yell et al. (2018) noted when determining if a student needs special education and related services because of an identified disability, one must consider more than the child’s academic performance. Educational performance may also be negatively impacted by other difficulties, including social, emotional, and behavioral problems (Yell et al., 2018).
A multitiered system of supports (MTSS) framework provides an opportunity to deliver preventive and supportive interventions to address student mental health needs (August et al., 2018). MTSS includes three tiers of instruction that increase in intensity with a student's individual needs. All students receive core instruction (Tier 1), and additional instruction is provided in Tier 2 and Tier 3 for those students in need. Other important components of MTSS include universal screening of students and practicing data-based decision-making to identify students’ progress and needs (Center on Multi-Tiered System of Supports, 2022). Within a MTSS framework, school-based mental health providers deliver evidenced-based interventions to students with a continuum of mental health needs (e.g., Arora et al., 2019; August et al., 2018) as well as challenging behaviors (e.g., Nichols et al., 2021; Njelesani et al., 2020). However, prevention and intervention through Tiers 1 and 2 may not be sufficient to meet the needs of all students. Students with disabilities may require more intensive mental health support, which must be developed and memorialized in the individualized education program (IEP).
“Within a MTSS framework, school-based mental health providers deliver evidenced-based interventions to students with a continuum of mental health needs as well as challenging behaviors.
Schools with well-established MTSS provide additional support for student mental health and the identification of students with significant mental health issues. Universal screening data are available for all students to assist in identifying those who need more support than what is provided through Tier 1 and Tier 2 and those who may require additional evaluation. These data provide information about a student’s response to available interventions across the MTSS, including special education, and should be considered as part of the comprehensive evaluation when a student is referred to special education due to mental health issues.
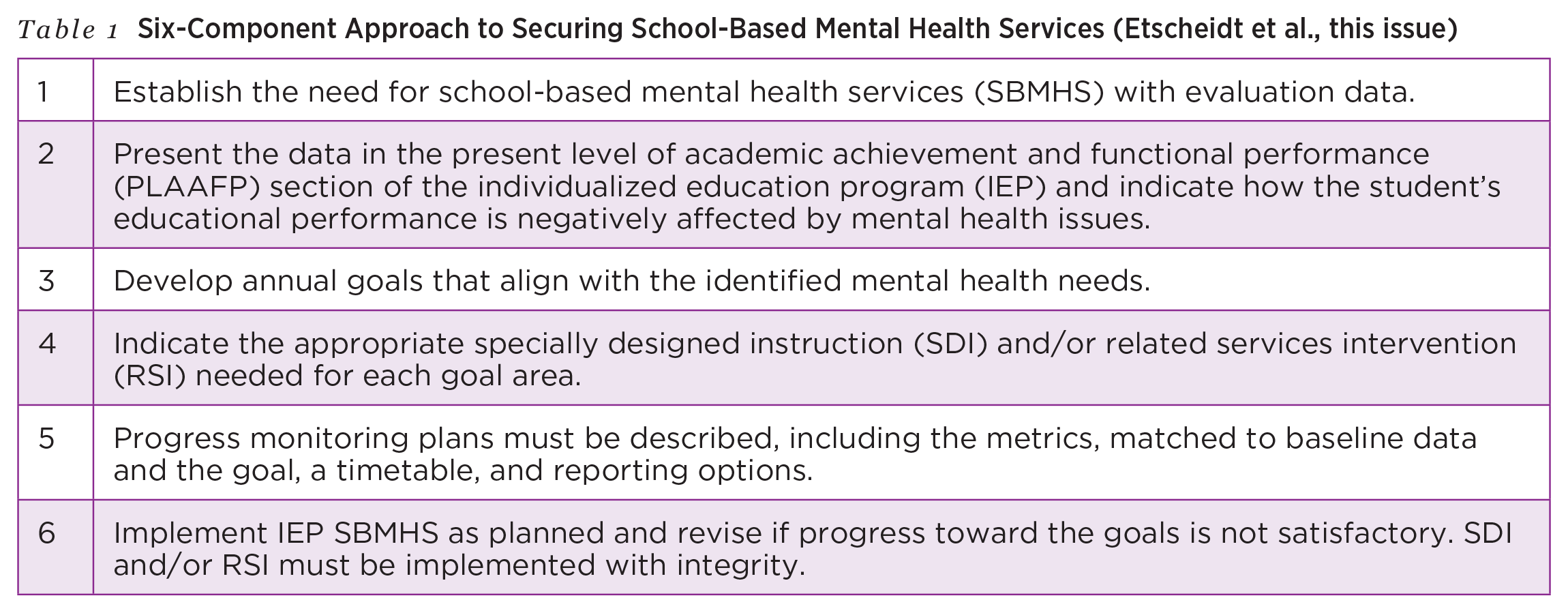
Etscheidt et al. (this issue) propose a six-component approach to securing school-based mental health services (SBMHS) for students with disabilities (see Table 1). This article illustrates this approach using two case examples. Each example includes a brief overview of the student’s background and reason for referral and a description of how each of the six components was addressed. We intentionally chose to share one example involving a student with an externalizing issue and one example of a student with internalizing issues as a reminder that symptoms of mental health issues (or emotional disturbance) present in many different ways. Together, these two examples demonstrate the recommended six-component process for securing mental health services for students with disabilities.
Six-Component Approach to Securing School-Based Mental Health Services (Etscheidt et al., this issue)
Applying Six Components to Externalizing Issue
Jasmine is a 4-year-old preschooler reported to be demonstrating physical aggression both at home and in her preschool classroom. Although she has shown aggression since the beginning of the year, her teacher, Mrs. Smith, reports an increase in the frequency, duration, and intensity of her aggression. Jasmine’s peers often complain or cry because Jasmine has hit or kicked them and/or they have been hurt.
The preschool team met on several occasions to discuss Jasmine’s case and possible interventions aimed at decreasing her aggressive behavior. Their ongoing discussion was framed within the context of the Pyramid model, developed to support young children’s needs and promote competence in social, emotional, and behavioral skills (Fox et al., 2003; Hemmeter et al., 2019). The current iteration of this model consists of four components that comprise three tiers, or levels of practice, including nurturing and responsive relationships and high-quality supportive environments (Tier 1), targeted social-emotional supports (Tier 2), and intensive interventions (Tier 3). Strategies and practices discussed and implemented for Jasmine include (a) structured transitions with a consistent, visually supported schedule of daily activities, daily reinforcement and modeling of classroom rules and expectations, and addressing important social-emotional skills classwide (Tier 1); (b) teaching, reinforcing, modeling, and role-playing social-emotional skills such as turn-taking, using words to ask for wants and needs and to respond to peers, and following directions; teaching and supporting identification and expression of emotions; and teaching and supporting self-regulation (Tier 2); and (c) development of a behavior plan that was implemented and monitored by the classroom teacher with support from the classroom paraprofessional and school psychologist over a 6-week period (Tier 3). Further evaluation was recommended due to her lack of response to these interventions.
Component 1: Establish the Need for School-Based Mental Health Services With Evaluation Data
The school team, including the school psychologist, early childhood special education teacher, the speech language pathologist, and the district’s behavioral interventionist, used the RIOT approach (i.e., Review, Interview, Observe, Test; Leung, as cited in Fisher et al., 2007) for this evaluation.
Review
This is Jasmine’s first year in preschool. There is little documentation to review. Available reports indicated no concerns with hearing, vision, or any significant health concerns.
Interview
Semistructured interviews were conducted with both Jasmine’s parents and her preschool teacher. The Kiddie Disruptive Behavior Disorders Schedule (K-DBDS; Keenan et al., 2002) was used when interviewing parents. The K-DBDS is a semistructured clinical interview that includes structured, developmentally sensitive prompts to assess for symptoms of disruptive behavior. This interview was originally developed to connect with criteria in the fourth edition of the Diagnostic and Statistical Manual for Mental Disorders for disruptive behavior disorders and has been found to provide reliable and valid results for assessment of symptoms associated with them (Keenan et al., 2007).
Information from both interviews indicated Jasmine primarily yells and hits others but also sometimes will pinch, kick, or bite. Through the use of a problem identification interview (e.g., Bergan & Kratochwill, 1990) designed to identify and operationally define a target behavior and to gather contextual information, Jasmine’s teacher, Mrs. Smith, stated Jasmine engaged in physical aggression since the beginning of the school year. The frequency, duration, or intensity of her behaviors are increasing despite Tier 1 and Tier 2 supports. Mrs. Smith noted more unstructured activities with less supervision (e.g., centers) and transitions are especially difficult for Jasmine. She often needs adult assistance to complete tasks and successfully move to the next location and/or activity without laying her hands on other children. Because of these difficulties, Jasmine does not appear to have any friends within the classroom. Specifically, children resist playing with Jasmine or being at the same center or table because they don’t want to “get hurt.” Mrs. Smith also noted Jasmine has difficulty with preacademic skills (e.g., identifying and reciting the alphabet in the correct order, rote counting from 1 to 5, one-to-one correspondence). Mrs. Smith attempted positive and specific praise for following classroom expectations and/or teacher directions, having Jasmine in close proximity to adults during large and small group activities, assigning her to centers with certain and fewer peers, and using timeouts. She noted the effectiveness of any strategy was inconsistent.
Parents report Jasmine has “always” been “willful and independent”; for example, Jasmine cried often and for long periods of time as an infant and became upset easily with quickly intensifying tantrums as a toddler. Currently, parents noted Jasmine hits, kicks, and bites, sometimes breaking skin, when she wants something others have or she is told “no.” Parents indicated they have tried time-outs and taking desired objects away, but Jasmine rarely stays in time-out and will often scream and sometimes throw or even destroy her or others’ belongings until they “give in.” They indicated they often give in because it is “just easier.”
Observation
Direct observations were completed in Jasmine’s preschool classroom. Within the classroom setting, three 30-minute antecedent-behavior-consequence (ABC) observations targeting physical aggression in three different activities were completed (i.e., centers, large group, small group). Data indicated common antecedents to physical aggression to be what appeared as Jasmine wanting another’s toy (e.g., asking or trying to take the toy) or object or being told “no.” When Jasmine was aggressive, she momentarily obtained the toy 75% of the time. Common consequences included peers telling the teacher and/or the teacher providing a verbal redirection on 80% of occasions and the teacher having Jasmine tell the peer she was sorry on approximately 50% of occasions. Jasmine was required to serve a time-out following the verbal redirection on 50% of occasions. Time-outs consisted of her sitting in a classroom chair in the corner of the room for 4 minutes before returning to the activity. If Jasmine did not stay in her chair for the full 4 minutes, the time would start again. If disruptive while in time-out, Jasmine was removed from the room to the principal’s office. These behaviors occurred most often during centers (i.e., five occurrences in a 30-minute period) or transitions (four occurrences over four transitions), reinforcing interview data from Jasmine’s preschool teacher.
At home, parents collected frequency data on each aggressive incident as well as what happened before and after an occurrence. Over a 5-day period, Jasmine had 10 physically aggressive incidents, with nine out of 10 antecedents being not getting what she wants and the consequences being parents giving in to her demands on eight out of 10 occurrences. On the two occurrences where parents did not give into her demands, Jasmine remained in her room until she “calmed down” and could return to the family activity. Parents indicated each “calm down period” lasted approximately 30 minutes.
Test
For the test component, the Behavior Assessment System for Children, Third Edition (BASC-3; Reynolds & Kamphaus, 2015) was completed by each parent and the preschool teacher, and the Brigance Inventory of Early Development-III (IED-III; Brigance & French, 2013) was administered by the school psychologist. A language screening was also completed by the speech language pathologist to rule out language concerns or deficits as a contributor to Jasmine’s behavioral challenges.
The BASC-3 is a comprehensive rating scale designed to measure the behavioral, social, and emotional skills of children and adolescents. It measures both externalizing and internalizing behaviors and the child’s adaptive skills. Jasmine’s preschool teacher, Mrs. Smith, completed the Teacher Rating Scale (TRS), and her parents completed the Parent Rating Scale (PRS). Results from the TRS of the BASC-3 showed Mrs. Smith rated Jasmine’s behaviors in the clinically significant range on the Hyperactivity and Aggression scales, the Externalizing Problems Composite, and the Social Skills scale within the Adaptive Behavior Composite. Ratings were in the at-risk range on the Attention Problems scale.
Results from the PRS of the BASC-3 showed both parents to have rated Jasmine’s behaviors in the clinically significant range on the Aggression scale and the Externalizing Problems Composite and in the at-risk range on the Hyperactivity scale. Taken together, results from the BASC-3 indicated both parents and the teacher have significant concerns with Jasmine’s aggressive behavior and some shared concern with hyperactivity. However, Jasmine’s parents did not indicate the same amount of concern as Mrs. Smith with Jasmine’s attention, and their ratings did not suggest Jasmine had issues with social skills.
On the Brigance IED-III, age-appropriate tests from both the Social and Emotional Development and the Academic and Cognitive Literacy sections were administered. The administered IED-III was the criterion-referenced version providing information on Jasmine’s overall skill level, highlighting specific areas of strength and need, through a compilation of developmental assessments. Information is gathered through observation, interview, or direct performance of the child, depending on the content of each individual assessment. Within the Social and Emotional Development section, results indicated Jasmine demonstrated “splinter” skills in her relationships with adults. She demonstrated some skills expected for her age but not others (e.g., following adult directions and classroom expectations, interacting respectfully). Jasmine’s skill level within the play and relationship with peers, motivation and self-confidence, and prosocial skills and behavior were below what is expected for her age level. Within the Academic and Cognitive Literacy section measuring Jasmine’s early reading and math skills, results indicated she is performing below what is expected for her age level across most areas (i.e., response to and experience with books; blending and segmenting word parts; visual discrimination between forms and letters; reciting, matching, and identifying letters; understanding number concepts; counting by rote to at least 5; and comparing different amounts). Jasmine was able to demonstrate expected skills with discriminating sounds (beginning and end), identifying rhymes and shapes, and sorting by color and shape.
Component 2: Present the Data in the Present Level of Academic Achievement and Functional Performance Section of the IEP and Indicate How the Student’s Educational Performance Is Negatively Affected by Mental Health Issues
Based on the information collected as part of this evaluation, Jasmine was eligible for special education services, and an IEP was developed. Within the present level of academic achievement and functional performance (PLAAFP) section, the team summarized the data collected through the RIOT approach, which together indicated Jasmine’s behavior to be significantly discrepant from her same-age peers and to significantly interfere with her development of preacademic and social skills. Specifically, Jasmine was reported to be demonstrating physical aggression (e.g., hitting, kicking, biting) both at home and at school, with the frequency, intensity, and duration increasing in both settings. It appears this behavior occurs most often when she wants another’s object or she is told no with no common consequence found to calm her once upset. Test results showed significant concern with aggression. The team determined a need for instruction and support in developing appropriate social skills, emotional-regulation skills and coping strategies, and preacademic skills. The team also highlighted a number of Jasmine’s strengths in the PLAAFP, including the positive aspects of her independence and her willingness to help others, especially the teacher, when asked.
“The team determined a need for instruction and support in developing appropriate social skills, emotional-regulation skills and coping strategies, and preacademic skills.
Component 3: Develop Annual Goals Aligned With Identified Mental Health Needs
In a discussion with the team, including both school staff and parents, social-emotional and preacademic skill goals were developed due to the apparent influence of Jasmine’s behavior concerns on her overall functioning. The goals were developed within the context of the state’s early learning standards and based on the evaluation results. Sample goals developed for Jasmine include:
• When given a direction by school staff, Jasmine will comply over a 5-day period 100% of the time with no more than two prompts and without becoming physically aggressive by December 1, 2023.
• When Jasmine is frustrated or upset, she will use learned words to express her emotions and what she needs over a 5-day period 100% of the time by December 1, 2023.
Component 4: Indicate Appropriate Specially Designed Instruction and/or Related Services Intervention for Each Goal Area
The special education teacher, Mrs. Brady, will provide specially designed instruction (SDI) for all goals. In collaboration with the school counselor, she will conduct social skills training with Jasmine using the Skillstreaming in Early Childhood program (McGinnis, 2012), an evidence-based program that promotes the systematic instruction of social skills to children demonstrating problematic behaviors. The program contains 40 skills divided into six groups, with the skills chosen for instruction based on the child’s individual needs. Each skill is taught using modeling of the skill and role-plays with feedback.
Jasmine will be part of a small group with two other preschool children identified as needing assistance with social skill development and two role models selected by the general education preschool teacher. Instruction will focus on school-related skills, dealing with feelings, and alternatives to aggression. The group will meet daily for approximately 15 to 20 minutes, with additional opportunities for practice and feedback provided throughout the rest of the school day. These additional opportunities will be planned on a weekly basis with the general and special education teachers and the school counselor.
“Instruction will focus on school-related skills, dealing with feelings, and alternatives to aggression.
The school counselor and school psychologist will include Jasmine’s parents in a parent training, an effective treatment for young children who demonstrate challenging behavior (e.g., Holland et al., 2017). Based on recommended formatting, the training course will include (a) an overview, definitions, and explanation of included behavioral terminology (e.g., ABC, positive and negative reinforcement, punishment, escape, extinction burst); (b) strategic attention, comprised of “time-in” (establishing positive parent-child interactions), using the 5:1 rule (five positives to one negative), catching the child being good, when and how to provide positive attention, and using planned ignoring; (c) using the Child’s Game (paying positive attention); (d) how to give effective commands; (e) discipline techniques for inappropriate behaviors (e.g., effective use of time-out and of privileges); (f) managing behavior in public places; and (g) promoting generalization (e.g., in public places) and maintenance (e.g., “booster” sessions) of skills (Holland et al., 2017).
Component 5: Describe Progress Monitoring Plans
Jasmine’s progress across all goals will be monitored on an ongoing basis. Quantitative data collected for each goal will be graphed weekly by the special education teacher and discussed with the team bimonthly to determine progress and the need for changes or modifications. Following directions will be monitored two times per week using a checklist by both the general and special education teachers. The checklist includes a place to mark the time of day, activity, if a direction was or was not followed along with how many prompts were needed, and whether Jasmine used physical aggression. The general education teacher and the special education teacher will each complete this one day per week. Because transitions and centers are most problematic, these activities will be the focus. However, bimonthly, the classroom paraprofessional will track these data throughout the entire day. Totals will be calculated, providing a frequency count and a comparison of following directions to not following directions with two or less prompts and without physical aggression.
The special education teacher will be responsible for monitoring whether Jasmine uses given words rather than physical aggression. This will be tracked through observing Jasmine’s response, both during Skillstreaming sessions and role-plays and generalization opportunities in the classroom, primarily during centers and pair/small group activities. The special education teacher will describe the event and Jasmine’s response. The classroom paraeducator will also track these data throughout the day in the general education classroom to ensure reliable data collection.
Component 6: Implement and Monitor IEP School-Based Mental Health Services
Implementation integrity checklists, to be completed by both the group leader and an independent observer, are included as part of the Skillstreaming program. The checklists include the sequence of steps for each lesson, with each step including several actions to be carried out per the instruction manual. The group leader and observer are to mark either “yes” or “no” for each action to indicate whether or not it was carried out and then total the number of “yes” and “no” responses across the form. The school counselor will act as the independent observer. She will observe and complete the implementation checklist two times per week until lessons are implemented with at least 80% integrity, and then she will observe once per month. The frequency of observations will be increased if integrity is below 80%.
To monitor the integrity of the parent training program, lesson plans for each session will be developed, and the two group leaders will mark when each lesson component is completed and if the steps were followed correctly. If any modifications to the lesson were needed based on participant questions, feedback, or identified needs, these will be noted in the comments section.
Applying Six Components to Internalizing Issue
George is an 11-year-old fifth-grade student receiving special education services for a specific learning disability. George’s special education teacher, Ms. Rose, convened an IEP meeting to discuss concerns about changes in George’s behavior and academic progress. George was invited to the meeting but refused to attend. Ms. Rose indicated George’s progress in both reading and writing has plateaued. She believes the lack of progress is due to issues with motivation because he is less engaged in both small and large group instruction and more distracted than in the past. She indicated the quality and quantity of his work has decreased; he is currently turning in 50% to 60% of assignments, compared to past work completion rates of 90% to 100%.
Ms. Rose reported on two different interventions used to support George. First, she implemented a home-school note system focused on work completion. The home-school note system is a common Tier 2 intervention in this school. George earned a reward at home on the second day of the intervention and then refused to show his parents the notes for the next 5 days. Mrs. Rose met with George to develop a second Tier 2 intervention when he resisted the home-school note system. He indicated he wanted to work for computer time, and they agreed that George would earn 10-minutes of computer time for each completed assignment. George’s progress was monitored using the number and percentage of assignments completed daily. When progress monitoring data showed no change in George’s assignment completion, the rate of reinforcement was increased, but there was no change in George’s assignment completion. Mrs. Rose convened the IEP team to discuss progress.
The team reviewed the progress monitoring data for both behavior interventions and George’s academic goals and decided more information was needed to understand George’s decrease in work completion. The team decided a functional behavior assessment (FBA) was needed to learn more about the variables related to George’s work completion. Ms. Rose indicated when George is not working he has his head on his desk or is out of the classroom to get something from his locker or use the restroom. She noted when George is allowed to leave the classroom, someone needs to look for him because he is gone longer than expected. The team decided to focus on two interfering behaviors: George putting his head on his desk and George requesting to leave the classroom. George’s parents consented to the FBA.
Component 1: Establish the Need for School-Based Mental Health Services With Evaluation Data
The school psychologist conducted an FBA, including completing the Behavior-Analytic Problem-Solving Interview (Steege et al., 2019) individually with Ms. Rose, Ms. Daisy (George’s general education teacher), and George’s parents. She observed George numerous times across different classroom activities and subjects. Ms. Rose collected data about the time, context, antecedents, and consequences of the two interfering behaviors. The school psychologist analyzed the data and could not find a clear function for either behavior. She called another meeting with the IEP team to discuss the results of the FBA and to determine next steps.
The IEP team discussed the results of the FBA and George’s continued decrease in the work completion. The school psychologist asked the team about possible mental health issues. The team reported no concerns about George’s mental health. The school psychologist followed up with more specific questions about possible symptoms, and Ms. Rose indicated noticing a change in George’s mood. She indicated he rarely laughs or smiles, and he now prefers to work alone. She reported he is easily irritated and rarely engages in conversation with her, even when she brings up his favorite topics. Ms. Rose worked with George for several years, and despite their positive relationship, he will not talk to her about the change in his behavior or any concerns about home, school, or social issues. George’s parents indicated they have also seen a change in George’s mood and his willingness to spend time with the family. They reported he is more irritable, but they assumed the change was just part of him being a preteen.
Due to the lack of a clear functional hypothesis and the indicated concerns about George’s change in mood, the team decided an evaluation of his mental health was necessary. His parents consented to the evaluation. The school psychologist followed the RIOT process.
Review
The school psychologist reviewed George’s educational record, attendance data, current grades, and current work products. There was no history of attendance issues until this year. George missed more days in the first semester than he typically misses in an entire academic year. There was also no history of social or behavioral issues, and teacher comments indicated he gets along well with others and has a couple of good friends. Reports indicated George is polite, outgoing, and eager to assist others. Progress monitoring data indicated George was making expected progress on his goals for the first 4 weeks of this academic year, and then his progress plateaued. There were three notations indicating George stopped midway through the progress monitoring task, put his head down, and refused to continue. A review of George’s current and past data confirmed George is currently turning in 50% to 60% of assignments, compared to past completion rates of 90% to 100%.
Interview
George, his parents, Ms. Rose, and his general education teacher, Ms. Daisy, were interviewed separately using the Semistructured Student Interview (McConaughy 2013b), the Semistructured Parent Interview (McConaughy, 2013a), and the Semistructured Teacher Interview (McConaughy, 2013c). The information from the behavior-analytic problem-solving interviews was also considered. George’s parents reported his strengths are his kindness and empathy toward others. They indicated he gets along with peers and adults. He has a small group of boys he has been friends with since early elementary school. Prior to this year, he spent a lot of time with these boys. George enjoys sports and video games.
“George’s parents indicated they are most worried about his change in attitude toward school and his irritability.
George’s parents indicated they are most worried about his change in attitude toward school and his irritability. They indicated his attitude toward school changed at the end of last school year. They could not identify an incident or any social or environmental issues that may have caused the change. In the past, both parents helped George with his homework, but he is now resistant to their help. He is most willing to accept help with science and math homework. They indicated at the beginning of the year, George would either ignore their offers of help or “snap” at them, so they stopped offering. George’s parents indicated the irritability is new and is getting worse. They said he spends more time in his room and will join family activities about 50% of the time. Previously, he was happy to join family activities and did so almost 100% of the time. When asked specifically about anxiety or depression, George’s parents said they don’t see George as sad or nervous. They reported no history of medical concerns or behavioral problems. George follows the rules at home, and they use grounding as a consequence when needed. George’s parents indicated he spends less time with his three friends, but he continues to see them at least once a week. They indicated George initiates contact with them less than in the past and that he gets agitated if they suggest he call them. George and his friends ride their bikes and play basketball at the park when the weather allows. When they are unable to be outside, they play ping pong and video games.
George’s parents reported George used to talk about attending the local community college to learn a trade that will allow him to work outside. He also talked about attending a 4-year university, but mostly to be involved in sports. They said he isn’t sure he wants to “voluntarily” go to school for 4 more years. The school psychologist made note of George’s parents’ comments about his strengths and career interests to include in his updated IEP.
Both general education and special education teachers reported a decrease in George’s work completion and a noticeable decrease in his peer interactions. They said George continues to sit with his peer group at lunch, but he is less boisterous. Ms. Rose indicated George “just isn’t himself.” When asked about specific changes in his behavior, she indicated he is less talkative and shows little emotion. She said he rarely smiles, and when he does smile, it is brief. She indicated George is less willing to accept help and is less focused on instruction. She set up a system of discrete prompts with him to remind him to focus, but she doesn’t feel it has been effective. She recently suggested a self-monitoring intervention, but George was resistant, saying, “Just leave me alone!” When asked to prioritize her concerns, she indicated she is most concerned about his mood and withdrawal.
Ms. Daisy indicated George doesn’t have behavior problems beyond his lack of work completion. She noticed him responding harshly to peers several times a day a few weeks ago, but the behavior decreased. She also reported George seems to be interacting with his peers less than at the beginning of the academic year. Ms. Daisy’s comments about George’s work completion and willingness to accept help were consistent with Ms. Rose’s comments. She indicated she spoke to George about his work completion twice in the last 2 months, and both times, he just shrugged his shoulders.
The school psychologist has a relationship with George, but during the interview, he was less talkative and forthcoming than in the past. She needed to meet with him several times to complete the interview because he provided brief responses to her questions. George indicated he has three good friends he has known since kindergarten and that he enjoys being outside, riding his bike, and playing basketball. He indicated he likes his teachers but not school. His favorite parts of school are seeing his friends and PE, and his least favorite parts are “all the reading and writing stuff.” George answered, “I don’t know” to questions about anxiety and depression and denied thoughts about suicide.
Observation
The school psychologist reviewed data collected as a part of the FBA and decided to complete additional observations. She observed George’s on-task behavior three times in reading and two times in math using a 10-second, whole interval recording procedure with peer comparison. Each observation was 20 minutes. Observations were completed during reading because of the decrease in George’s work completion in this area. The school psychologist observed George during math because he previously indicated it was a preferred subject and he typically earns As and Bs in this area. The school psychologist asked Ms. Rose and Ms. Daisy to keep track of the number of times they offered George help and the number of times he accepted for 5 days. She also observed George during lunch twice.
George was on task 42%, 57%, and 48% of the time during the observations in reading (peers = 86% and 91%, 93% and 96%, 92% and 93%). George was on task 63% and 58% of the time in math (peers = 97% and 90%, 91% and 88%). George accepted help from Ms. Rose 26% to 34% of the times offered each day, and he accepted help from Ms. Daisy 32% to 40% of the times she offered. Ms. Daisy offered George help approximately half of the number of times per day as Ms. Rose.
George sat with the same three friends during both observed lunch periods. He ate a part of a sandwich during the first observation and an orange during the second. George spoke less than his three friends during both observations but appeared attentive to the conversation most of the time. He stared out the window for longer than a minute two different times during the first observation. George’s peers smiled and laughed most of the lunch period during both observations, whereas George was observed laughing once during the second observation. George smiled briefly three times during the first observation and four times during the second.
Test
The school psychologist used the BASC-3 to broadly assess George’s emotional well-being and adaptive skills. Both of George’s parents completed the BASC-3 PRS, and his general education and special education teachers each completed the BASC-3 TRS. George completed the BASC-3 Self Report of Personality. Based on research, the school psychologist expected to see some differences in results in the home and school environments. The school psychologist had George complete the Subjective Units of Distress Scale (SUDS; Wolpe, as cited in Joyce-Beaulieu & Sulkowski, 2015) each time she met with him during the assessment process. She explained the scale during their first meeting.
George’s parents’ responses placed George in the average range for adaptive skills, whereas teachers indicated adaptive skills to be low. Teachers’ responses indicated George is exhibiting behaviors consistent with attention problems, but neither parent report suggested they perceive attention as an issue. Both teachers indicated elevated levels of internalizing problems (anxiety and depression), whereas parents only identified depression as an issue. George’s responses indicated he is experiencing significant emotional distress, including depression, anxiety, and social stress. His responses indicated he does not perceive himself as having the skills or social support to cope with his difficulties. George indicated he does not feel good about school. His responses also suggested he is experiencing problems with attention.
During the first meeting with the school psychologist, George rated himself a 75 on the SUDS, indicating he was feeling quite distressed and experiencing physiological signs of distress. It also indicated he felt his feelings were interfering with his functioning. George rated himself between 75 and 86 the next four times they met. Overall, assessment results indicated George is experiencing anxiety, depression, and social stress. He is withdrawn and irritable, and he is having difficulty concentrating. Issues with withdrawal, concentration, and irritability are consistent with emotional distress, including anxiety and depression.
Component 2: Present the Data in the PLAAFP Section of the IEP and Indicate How the Student’s Educational Performance Is Negatively Affected by Mental Health Issues
After reviewing the assessment data, the team decided George’s internalizing problems were adversely affecting his ability to pay attention in class and request and accept help when needed. His internalizing problems also impact his interactions with peers and teachers. The assessment data and George’s strengths and needs were summarized in the PLAAFP.
Component 3: Develop Annual Goals Aligned With the Identified Mental Health Needs
The team decided George needed additional support to strengthen his self-regulation skills related to attention and persistence. The following are examples of George’s new annual goals:
• When George does not understand academic content or an assigned task, he will accept help offered by teachers across a 3-day period at least 70% of the time by December 1, 2023.
• When asked to self-report his emotional distress, George will rate his distress in the mild range or lower (score of 40 or lower) as measured by the Subjective Units of Distress scale across a 2-week period, for at least 90% of the ratings by December 1, 2023.
Component 4: Indicate Appropriate SDI and/or Related Services for Each Goal Area
SDI will include 30 minutes each day of instruction from the special education teacher in the general education classroom. Ms. Rose will spend 15 minutes with George during independent work in reading or math class teaching him a work-break strategy to help increase his on-task behavior. George will learn to work for 5 minutes and then take a 3-minute break. Ms. Rose will teach him to use a timer to measure the time he is working and the time he is breaking. During this time, she will provide either a positive comment (e.g., “I know accepting help can be hard, way to go!”) or positive physical gesture (e.g., thumbs up, high five) when George accepts help from her or his general education teacher. Ms. Rose will also work with George for 15 minutes during large group instruction. She will teach George note-taking skills to support his active listening throughout instruction. Ms. Rose will teach him how to ask questions as part of his note-taking. She will then encourage him to raise his hand after instruction is complete to ask the general education teacher to answer his question. Ms. Rose will also provide positive reinforcement when she observes George using any of the coping skills he is learning with the school psychologist.
George will receive school psychological-related services. The school psychologist will meet with George for 30 minutes weekly to provide cognitive behavioral therapy focused on his depressive symptoms. The school psychologist will use cognitive restructuring to teach George how to transform his negative thoughts into more positive ways of thinking, and she will work with him to identify and practice positive coping strategies, such as listening to music, talking to a friend, going for a walk, or any other positive coping strategy he might be willing to try.
Component 5: Describe Progress Monitoring Plans
The special education teacher will measure the percentage of times George accepts help from Ms. Rose or his general education teacher three times a week. Measurement should alternate between the general education setting and when George receives instruction for his academic goals in the special education setting. The special education teacher will put five copies of the SUDS in a folder for George every Monday and prompt George to complete a SUDS sheet at the end of reading a minimum of 80% of the school days. George and the special education teacher will update his progress monitoring graph each Friday.
Component 6: Implement and Monitor IEP School-Based Mental Health Services
The school psychologist will create an implementation integrity checklist on a Google Document that includes the elements of the SDI and the related services intervention. This checklist will include attendance information to ensure George is attending his weekly related service sessions and daily SDI. The special education teacher will complete the checklist daily for the first week of implementation. The school psychologist will complete the checklist on the first day of meeting with George. She will also observe instruction twice during the first week of implementation. The school psychologist and special education teacher will meet at the end of the first week of implementation to discuss the implementation data and any obstacles or needed changes. Once the instruction and interventions are implemented with at least 80% integrity, the implementation integrity data collection will be faded to once a week and then once a month. Feedback will be shared with the special education teacher after each observation.
Conclusions
The six-component approach (Etscheidt et al., this issue) illustrated with the two cases examples provides a collaborative, data-based approach to meeting the mental health needs of students. The same approach presented here can be used to substantiate a student’s need for mental health services regardless of their eligibility for special education.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.