
Abstract
In this article we propose a model of collaboration for school teams as a guide to the provision of effective, individualized and culturally responsive school-based mental health supports. When school teams embark on this process, they must be ready to provide a continuum of care within a comprehensive plan. Collaboration is essential when working within this continuum. Using a case-based approach, we provide a framework for working together leveraging the content and concepts of the three High Leverage Practices (HLP’s) for Collaboration within the MTSS model. We walk the reader step by step through a process that includes using the HLPs to strengthen practice, assist in planning and delivering collaboration. Imperative to the process is developing appropriate IEPs and establishing methods of input, including the family and outside providers. Using the HLPs as a framework can assist teams to develop and create a strong shared vision alongside and in support of the family and most importantly, the students we serve.

Elijah is an eighth grader receiving special education services to address his academic and behavioral/social/emotional needs resulting from attention deficit disorder and generalized anxiety disorder. During an individualized education program (IEP) meeting discussion about his transition to high school as a ninth grader, both he and his parents shared Elijah’s increasing concerns and anxiety regarding the upcoming school year. They reported he has been talking to his private counselor, Mr. Rice, about his fears and were encouraged to share this information with school staff. Elijah indicated that he is worried that he will fail his classes because he heard that high school was “really hard and the teachers are mean.” He is convinced that everyone is going to harass him because he is “Black and not interested in playing sports.” He has been told by his older siblings that other students will only be friends with Black students if they play football or basketball. Elijah’s case manager, Ms. Turner, attempts to assure him and his parents that he has nothing to worry about. Before the end of his eighth-grade year, Ms. Turner arranges for Elijah to visit the high school campus, meet his new special education teachers, and make sure he has a class schedule that matches his academic needs and skills. Looking forward, his first semester report card of his ninth-grade year indicates that he is failing all his classes. No other communication regarding support for his mental health needs were given to the family. His parents reported that they were unable to persuade him to attend school on a regular basis. Recently, Mr. Greene, the school dean, required Elijah and his parents to attend a meeting to discuss the school’s responses to Elijah’s frequent absences, which are aligned with the district’s truancy procedures. These procedures require the school, family, and student to develop a plan to increase his attendance and discuss the negative consequences of truancy, including failing grades, lack of credit, not graduating on time, and referral to the community truancy board. Elijah refused to attend this meeting in person and would not agree to participate by phone. During the meeting, his parents indicated their frustration with the truancy process and discussed their concern that this is not the best way to support Elijah. They reported that he is still seeing a private counselor; however, due to staff turnover at the community mental health agency, he has been treated by three different counselors in the last 9 months. Parents reported that Elijah’s current agency counselor, Mrs. Rodriquez, recently diagnosed him with school phobia and social anxiety. They want to know what the school can do to help their son.
Elijah is one example of the approximately 17% of school-age students in the United States who have been diagnosed with a serious mental health disorder and experience impacts of those disorders on their school attendance, performance, and completion (Bruns et al., 2016; Kern et al., 2022; U.S. Department of Education, 2021). Additionally, Elijah and other students like him illustrate the call for increased attention to the need for culturally responsive teaching approaches and culturally responsive mental health services for students who are from diverse cultural backgrounds (Dillard, 2019; Kern et al., 2022; J. Rodriguez & Hardin, 2017). School personnel are increasingly becoming aware of the mental health needs of their culturally and linguistically diverse (CLD) students and the impact of untreated mental health needs on positive school outcomes (Lazarus et al., 2021; Skaar et. al., 2020). Elijah’s vignette illustrates a layered set of challenges and opportunities. Special education in general presents a medical model highlighting what is “wrong” with a student—leading to a deficit-based perspective that can create further barriers to access. In addition to the deficit-based perspectives, there are cultural considerations that can make or break the success of the student, the family, and the overall team’s approach (J. Rodriguez & Hardin, 2017).
For students with disabilities, there is also an increased recognition regarding the responsibility for schools to address the mental health needs of this population through assessment as part of a comprehensive special education evaluation and, contingent on qualification, the provision of special education and related services in IEPs (Bruns et al., 2016; S. Hoover et al., 2019; Kern et al., 2022; Kutash et al., 2015; Mathur et al., 2017). Although the process does by design approach the evaluation and IEP from a deficit-based perspective, as illustrated in the initial vignette, taking a strength-based approach when working with students and families will result in plans and interventions that highlight the strengths and assets of the student, their family, and community (J. Rodriguez & Hardin, 2017).
Lastly, and we would argue most importantly, there is a need to increase collaboration with families of students and their outside mental health care providers to provide a seamless approach to high-quality and effective supports that generalize across settings. Unfortunately, this includes acknowledging that mental health supports often occur across multiple settings without an intentional focus on communication and cross-collaboration, leading to ineffective overall service delivery and poor outcomes (Garbacz & Mendez, 2021; S. Hoover et al., 2019). This also implies that we acknowledge that as educators we must educate ourselves about the unique backgrounds of students and families. Our “lens” may not be a cultural match to what students and families need. Mental health is perceived differently in and among various social and cultural groups. Understanding this is imperative toward building a healthy and respectful collaborative relationship. Otherwise, we risk attempting to collaborate in good faith without understanding the perspectives of our families that might not be a match (J. Jones & Miranda, 2021).
A Tiered Approach to School-Based Mental Health Services
A consistent recommendation for the delivery of mental health services in schools begins with conceptualizing mental health services as involving comprehensive systems that provide a full array of services, supports, and instruction “that promote positive school climate, social and emotional learning, and mental health and well-being, while reducing the prevalence and severity of mental illness” (S. Hoover et al., 2019, p. 10). This reframing of mental health services in the school setting expands the historical practice of such services being deployed only to treat illness or pathology to a more comprehensive approach involving individualized school supports to enhance and support the development of students’ well-being. This added component of school-based mental health services calls for a focus on increasing the quantity and quality of students’ positive emotion, engagement, relationships, and accomplishments (Doll et al., 2021). When done effectively, these comprehensive approaches to school mental health systems “contribute to improved student and school outcomes, including greater academic success, reduced exclusionary discipline practices, improved school climate and safety, and enhanced student social and emotional behavioral functioning” (S. Hoover et al., 2019, p. 10).
In alignment with comprehensive systems necessary to support academic and behavioral success in schools, it is recommended that schools utilize a multitiered system of supports (MTSS) to address the mental health needs for all students (Bruns et al., 2016; Kern et al., 2022). MTSS has been promoted as an approach to efficiently and effectively organize and deliver a broad continuum of school-based mental health services (Walter et al., 2019). The MTSS continuum provides evidence-based interventions for a variety of prevalent mental health disorders, such as depression (Arora et al., 2019), anxiety (A. M. Jones et al., 2018), attention deficit hyperactivity disorder (Fabiano & Pyle, 2018), and aggression and noncompliance (Waschbusch et al., 2018). Trauma-responsive MTSS integrates services and supports to provide social-emotional learning to students affected by adverse child experiences (S. Hoover et al., 2019).
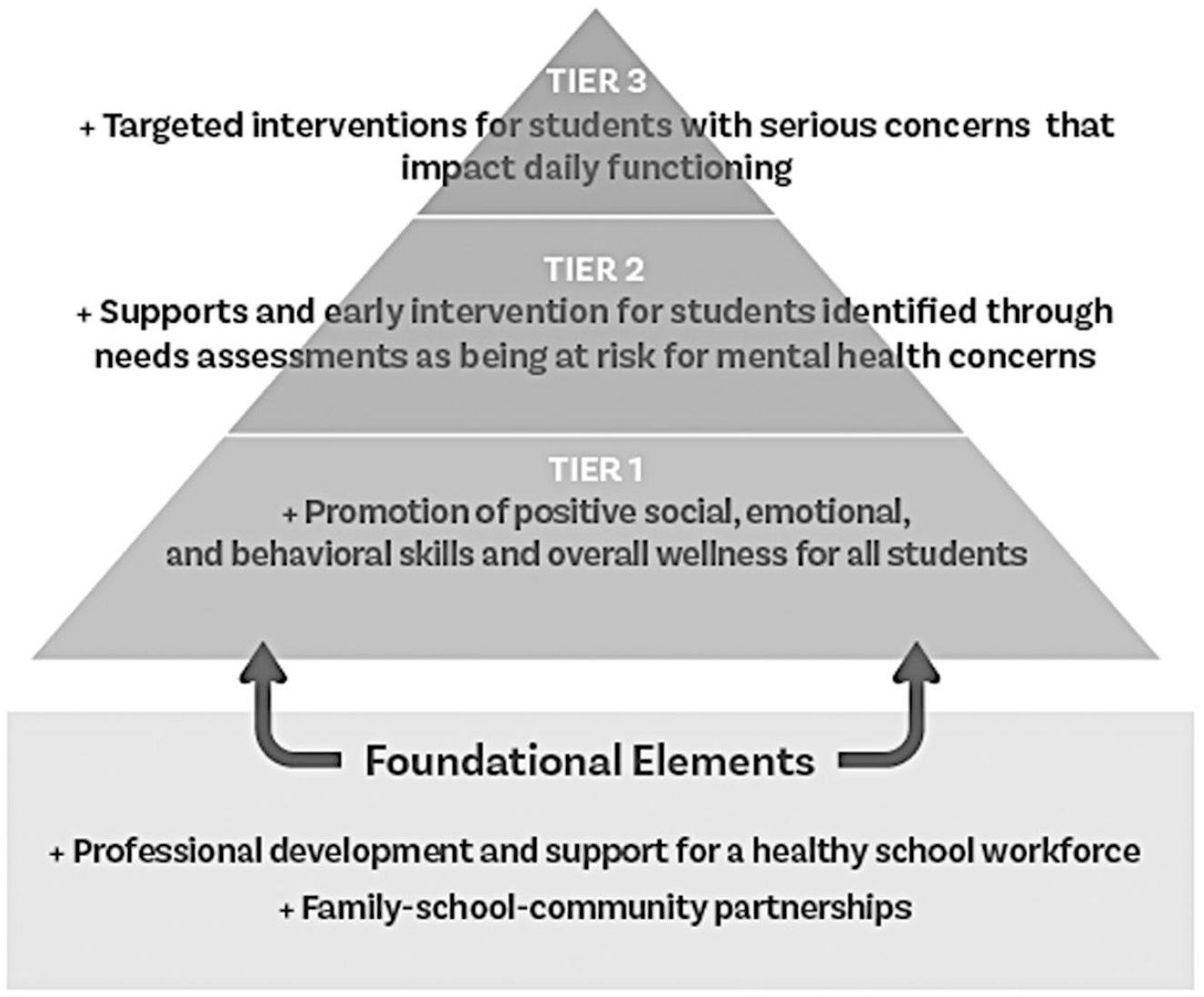
As described in Figure 1, MTSS allow for the delivery of a range of mental health services from preventive to intensive interventions (Bruns et al., 2016).
Multitiered system of mental health supports
When using an MTSS framework, Tier 1 interventions are delivered to all students and include a research-based core curriculum, culturally and linguistically responsive instructional practices, universal screening to assess current level of performance, social-emotional curricula delivered in the classroom, and clear behavioral expectations and supports (Bruns et al., 2016; Doll et al., 2021; Splett et al., 2018). For those students whose mental health needs are not fully addressed through Tier 1 interventions, the MTTS framework outlines a data-based decision-making and problem-solving process to prescribe and deliver more intensive and targeted Tier 2 interventions. These interventions are typically adult-led individual or small-group instruction and are delivered as part of general education services (Bruns et al., 2016). For students needing additional, individualized, and intensive support, Tier 3 interventions are warranted. Services and support at this tier are frequently needed by students with more complex profiles who require the involvement of specially trained professionals (e.g., behavior specialists, mental health providers, school psychologists, and social workers; Bruns et al., 2016; Doll et al., 2021; Eber et al., 2019).
The expansion of the MTSS approach to address students’ mental health needs involves a wide range of interventions provided by multiple professionals, including teachers, school support personnel, and related service providers. Schools must coordinate the roles of mental health professionals to assist teachers to help their students access school-based mental health services (Marsh & Mathur, 2020). Schools adopting an MTSS framework for the prevention and intervention of mental health concerns promote the identification of intervention needs through effective screening tools (Moore et al., 2019; Splett et al., 2018). Following screening, adaptive and sequential intervention strategies are selected in and across tiers based on the student’s responsiveness to the intervention (August et al., 2018). Students may be moved from more or less intensive tiers as indicated by ongoing data-based assessments.
“The expansion of the MTSS approach to address students’ mental health needs involves a wide range of interventions provided by multiple professionals.
Most importantly, utilizing an MTSS approach to addressing the mental health needs of all students provides a structure for schools, families, and communities to deliver a continuum of care (Vaillancourt et al., 2013). This continuum must include evidence-based practices that value and support culturally and linguistically diverse backgrounds in the learning environments:
Within MTSS for diverse learners, educators are encouraged to continue in their efforts to shape the cultural and linguistic responsiveness of teaching and learning by incorporating home, community, school, family and student factors into the instruction to best meet contemporary educational challenges. (J. J. Hoover & DeBettencourt, 2018, p. 184)
An effective MTSS is anchored in strong family-school-community partnerships and meaningful family engagement (Weist et al., 2017).
In Elijah’s situation, once the school staff became aware of his mental health concerns and needs and if both his middle and high schools had utilized an MTSS framework to address the mental health needs of their students, a comprehensive plan of prevention and treatment would have been developed and implemented. Because Elijah receives special education services, his IEP team would have considered and addressed his mental health needs through the provision of appropriate specially designed instruction or related services. As a first step to the process for providing school-based mental health services for Elijah, Mrs. Turner would begin by effectively utilizing a variety of collaboration skills. Lastly, the school would have reached out to collaborate with the family’s counselor so that mutual treatment planning could occur with the school supporting goals and strategies. Unfortunately, these interventions were not implemented, and the team found themselves in reactionary mode with no positive momentum or team-based interventions that included the family. Looking back at this case, what could teams learn and do differently?
“It is important to keep in mind that the main goal of these collaborative efforts is to effectively support the needs of the students and their families.
Collaboration
In answer to the question of “What could the team have done differently?,” we propose a model of collaboration to frame our recommendations for practice. Collaboration is key when identifying needs and planning for and implementing effective interventions—including the provision of school-based mental health services (S. Hoover et al., 2019). As a field, it is critical for educational professionals to acknowledge that our services do not begin or end at the school door. Conversely, they do not exist solely in the outside clinical world. Additionally, the burden of ensuring communication, collaboration, continuity, and alignment of services should not rest primarily on families. What can we use to guide our practice? Fortunately, school teams already have appropriate guidance right at their fingertips to use for building successful programs.
The high-leverage practices (HLP) for special education (McLeskey et al., 2017) include three practices related to collaboration, which are applicable to addressing the mental health needs of students through school-based mental health services. Although these high-leverage collaboration practices include efforts at various organizational levels and with a variety of individuals, it is important to keep in mind that the main goal of these collaborative efforts is to effectively support the needs of the students and their families. These critical collaboration HLPs include:
Enacting best practices from each of these HLPs can assist teams to strengthen their services, aid in better coordination, and increase understanding of mental health practices at all levels of the tiers. They can also assist the family to feel empowered as decision makers in the educational planning and implementation process.
If we return to the eighth-grade IEP meeting for Elijah, it is possible to identify multiple opportunities where the special education case manager could have utilized collaboration practices to successfully address the concerns raised by his parents and be intentional in their use of culturally responsive practices. Rather than waiting to address Elijah’s anxieties and concerns as part of his transition to the high school, Elijah and his family would have benefited from formal collaboration efforts between the school and his private counselor, including permission to exchange confidential information. Additionally, collaboration with the school staff responsible for providing tiered levels of school-based mental health services, with the information provided with parents, would likely have resulted in an intensification of tiered services at the school to address his anxiety regarding school performance and developing peer relationships. Lastly, collaboration efforts with the school psychologist would have supported the need for additional evaluation data so the IEP team could determine the role that special education may play in addressing his mental health needs.
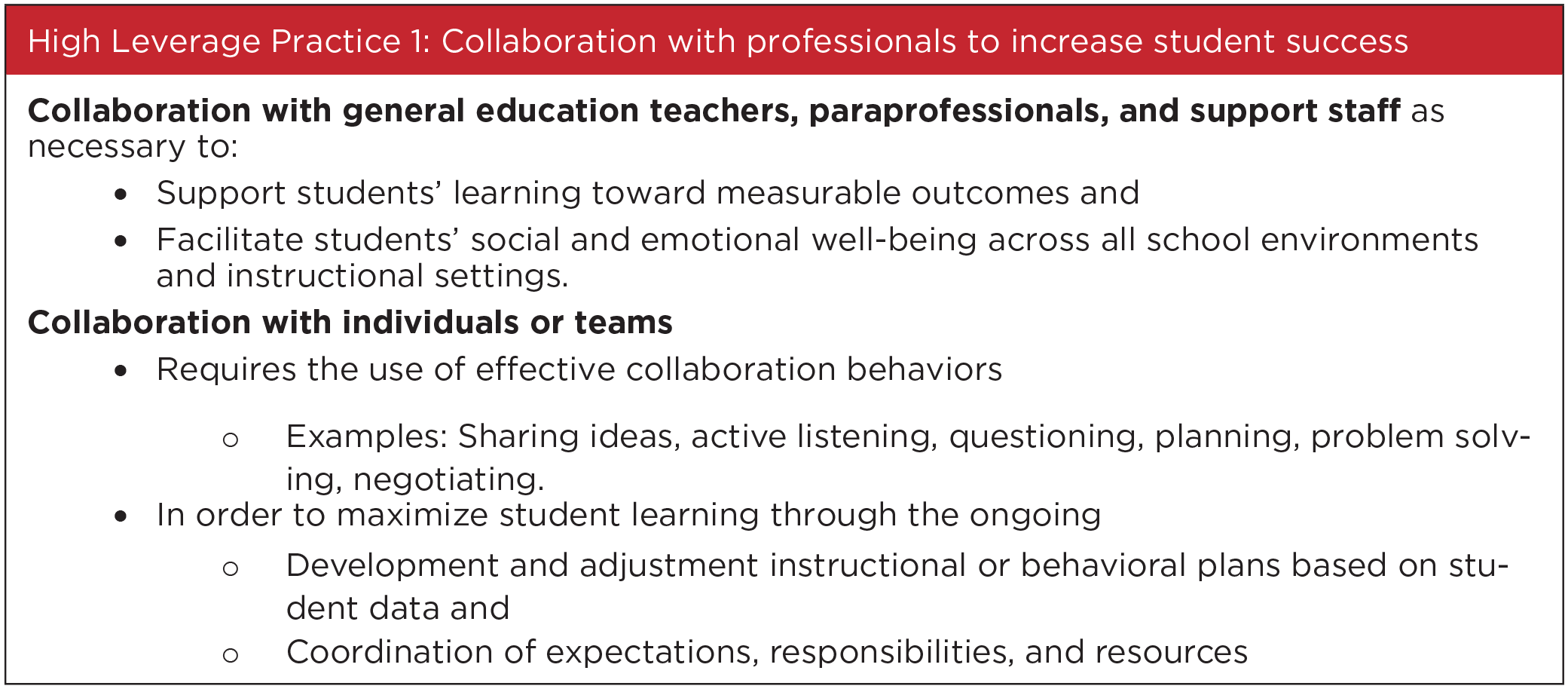
HLP 1 (see Figure 2) demonstrates the commitment of the special education professionals to work together rather than in isolation to produce quality outcomes for all students. When special educators center their collaboration efforts with other professionals around the mental health needs and services of students with disabilities, the conversations about services, and in particular mental health services, may begin to shift from an approach based on stigma, shame, and isolation to a strength-based approach that designs and provides comprehensive services that support the overall health and well-being of students. Additionally, because of this collaboration, professionals engage in conversations that increase their knowledge and skills related to providing preventive and proactive mental health services, developing students’ well-being, understanding various mental health conditions, and supporting the use of evidence-based practices across multiple settings to address specific mental health conditions. Collaboration with other professionals is particularly imperative in addressing the mental health needs of CLD students, who are overrepresented in special education (Bal et al., 2019) and who require culturally sensitive social-emotional supports to increase learning opportunities (Artiles, 2011; Wang et al., 2020). A “boundary-crossing collaboration” for CLD students with disabilities creates an integrated services delivery system across professional boundaries that “generated positive academic, social-emotional, behavioral, and mental health outcomes” for CLD students with disabilities (Ko et al., 2020, p. 11). Administrators, regular and special educators, related services personnel, families, and community members learn from each other’s work, share repertoires, and create new practices and paths to address students’ mental health needs.
High-Leverage Practice 1
The use of collaborative practices among professionals helps ensure that districts develop and implement IEPs that “provide meaningful opportunities for appropriate academic and functional advancement and to enable the child to make progress” (U.S. Department of Education, 2017, p. 6). In collaboration with other professionals, IEP teams can accomplish this by focusing on the individualized needs of a student by conducting thorough and meaningful assessments of all of a student’s needs and then focusing on (a) a student’s academic and functional needs, (b) the views of the student’s parents, (c) a student’s disability, and (d) a student’s potential for growth when developing their IEP.
Once again, reflecting on the efforts of the school to address Elijah’s mental health needs, collaboration between school staff and his private counselor may have resulted in the staff learning that cognitive-behavior therapy (CBT) is one of the most established evidence-based treatments to address anxiety disorders among adolescents (Higa-McMillan et al., 2016). They would also learn ways that CBT could be used in the classroom to support Elijah with utilizing positive self-talk to reframe his thinking and employ actions that would reduce his concerns about attending high school. The team would also learn that he was working with his counselor on developing awareness of the triggers for his anxieties and developing a toolkit of strategies for self-regulation through self-awareness and cognitive reframing. If school staff understood these strategies, they could have provided opportunities and supported Elijah’s development of his skills. Additionally, collaboration would have highlighted the intersectionality of Elijah’s identity as a student with a disability, a student with mental health needs, and a Black student. This increased understanding on the part of the school staff would result in more culturally responsive and individualized supports, services, and practices focused on increasing Elijah’s school attendance, engagement, and peer relationships. Without knowledge of the outside provider’s treatment plan, the team continued to implement Elijah’s IEP with limited interventions resulting in poor academic, social, and behavioral progress. Again, this was preventable.
Collaboration, IEP Development, and the Provision of Free Appropriate Public Education
In working to address a student’s mental health needs, the IEP must determine and highlight all areas of concern:
To ensure that a student’s IEP is crafted to enable the student to make academic and functional progress, the student’s parents and school-based personnel who compose the IEP team should develop a special education program that is ambitious and challenging. (Yell et al., 2020, p. 345)
As a beginning step, Yell et al. (2020) recommended that IEP teams conduct assessments to identify the student needs and describe those needs in the student’s present levels of academic achievement and functional performance. For students with mental health needs, the social, emotional, or behavioral needs should be addressed in students’ IEPs in the statement of functional performance. “Functional performance . . . refers to any nonacademic area that allows a student to function independently on a day-to-day basis, such as cognition, communication, motor skills, behavior, or social emotional” (Center for Parent Information and Resources, 2017). Yell et al. recommended IEP teams address the student’s identified needs with “(a) annual goals; (b) special education services, supplementary services (including accommodations and modifications if needed), or related services; or (c) both annual goals and services” (p. 345). Lastly, Yell, et al. emphasized the need for IEP teams to “develop or adopt a system to collect data to monitor a student’s progress and use data to guide future decisions” (p. 345).
As part of a well-established MTSS model of school-based mental health services, Elijah’s IEP team could have, when notified about the student’s mental health needs, enacted the steps suggested from Yell et al. (2020). Let’s see how this would play out in his caseand how it theoretically may have changed his outcome(s).
When the IEP team first meets with Elijah and his family and learns about his outside treatment, current diagnoses, and his and his family’s expressed concerns, they recommend that the evaluation be opened to consider his current needs. They obtain consent and begin the reevaluation process, carefully considering outside treatment reports from providers that the family provided for them. The information obtained from outside sources and the psychologist’s mental health reassessment indicates that his current needs continue to present an adverse educational impact to accessing general education and benefiting from special education services. After completing the reevaluation, the team meets to craft a new IEP that includes this information. They intentionally ensure that Elijah and his family have a strong voice to determine what they want to see in terms of support for his school year through the use of person-centered planning. They have also invited his counselor, who provides specific recommendations to the team. The IEP includes an updated functional behavior assessment and positive behavior intervention plan that reflects feedback and input from all members of the team. It is positive in its focus and leverages the outside mental health provider’s treatment plan to provide collaborative services in the school setting. New goals are written along with numerous targeted accommodations that the team agrees will assist Elijah to practice and strengthen his self-advocacy skills, such as requesting to take a test in another environment rather than with/in front of peers. The team agrees to meet quarterly to look at the data available from his grades, attendance, teacher feedback, family input, and ongoing classroom-based assessments. Elijah will get to have a large role in planning and conducting meetings with his team and, in fact, has a goal for self-awareness in his IEP that addresses this important skill set. Finally, the team implements the IEP, including specific training for staff on his specific mental health needs, intervention, and ways to promote skill development—in his case, self-awareness of how his anxiety manifests and ways to reframe his thoughts and reactions. At the first quarterly meeting, Elijah is ready with an agenda, feedback from teachers, data on his grades, and input from his family. The team makes numerous changes to the IEP and obtains further training on cognitive strategies for reframing/restricting and supporting self-awareness skills related to anxiety disorders. By the end of the school year, Elijah has missed only 3 days of school, and his teachers report an increased level of engagement with peers during various learning activities. Elijah is now leading his IEP meetings, and both he and his family have a very positive outlook for the following school year. Had these steps been taken, the true outlook for Elijah may have been much more successful.
In this vignette, the team took the route of reevaluation to ensure that all data were considered related to his disability. They took the appropriate steps to craft an IEP that was designed based on the information gathered during the evaluation and his unique needs arising from the intersectionality of his disability and race. In particular, they identified many areas of strengths and assets that reflect genuine input from the student, his parents, his outside counselor, and school staff. This led to the development of an IEP with present levels reflecting his current needs, which informed the IEP team about the services required as well as goals and accommodations. This is a critical step in the process of supporting a student and emphasizes the role of the IEP meeting in its form and function. We would argue that the IEP meeting is often underutilized as an incredibly important contribution to the overall quality of programming.
The second collaborative HLP involves strategies to include and support all participants in the IEP meeting.
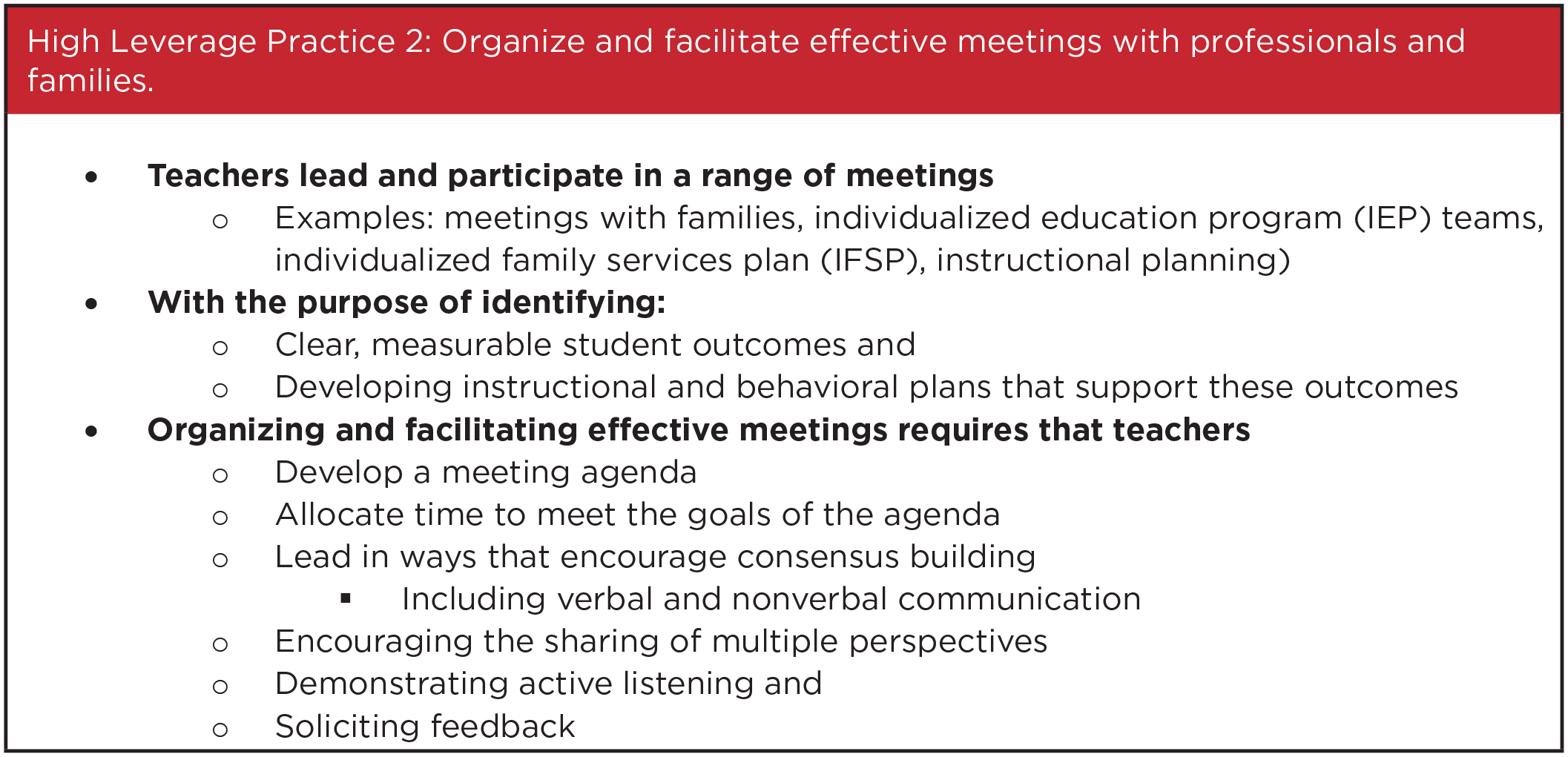
When focusing on the set of collaboration practices that contribute to effective organization and facilitation of meetings, it is critical to do so with the acknowledgment that “each education partner brings a unique set of skills that collectively enhance each student’s academic and behavioral achievement” (Harry & Ocasio-Stoutenburg, 2020; Lesh, 2020, p. 279; Sheehey et al., 2009). A frequent error made by school staff when organizing and facilitating meetings is to focus on efficiency by spending the majority of the conversation explaining what actions the district is going to take and the reason for said actions. In contrast, when meetings are organized and facilitated utilizing effective collaboration practices, the focus shifts to leading the meeting in ways that “encourage consensus building through positive verbal and nonverbal communication, encouraging the sharing of multiple perspectives, demonstrating active listening and soliciting feedback” (McLeskey, et al., 2017, p. 18).
Elijah’s team had an opportunity, in fact multiple opportunities, to collaborate with him and his family as partners in the context of the IEP meeting. This is often easier said than done, and many teams struggle to include families or outside providers in a meaningful way. IEP teams can use specific guidance from the HLP 2 (see Figure 3) to effectively include and support all members and their contributions. In Elijah’s case, this means establishing open communication with his outside mental health providers and family and including his own input to best support him in the school setting. Additionally, collaboration strategies will need to address the cultural needs of Elijah and his family and acknowledge the institutional racism that students of color frequently encounter in our educational and mental health systems. (Harry & Ocasio-Stoutenburg, 2020; Sheehey et al., 2009). Meeting facilitation practices that are centered on cultural humility and avoid the assumption that norms of the White dominant culture are the goal are culturally responsive practices and promote family engagement (Achola & Greene, 2016; Dillard, 2019; Harry & Ocasio-Stoutenburg, 2020). Facilitating involvement of CLD families requires an understanding of the factors associated with reduced involvement, such as culturally based beliefs and language barriers, so that strategies to empower and enhance participation are implemented (R. J. Rodriguez et al., 2014). Strategies to support CLD families and their children with disabilities include promoting a family-centered approach to educational planning (Achola & Greene, 2016; Cote et al., 2012).
High-Leverage Practice 2
Effective IEP meetings start with some basic “nuts and bolts” that lead to effective work environments. These include (a) all required members notified and present, (b) all team members prepared in advance for what parts they are sharing/contributing, (c) a clear agenda with all topics planned and communicated, and (d) time for all members to contribute, ask questions, and make comments. Demystifying the IEP process for all parents of children with disabilities can be accomplished by providing information and guidance before, during, and following the IEP meeting (Lo, 2012). Professionals should also examine the quality and quantity of interactions with CLD families between meetings to assure a positive and reciprocal relationship exists (Rossetti et al., 2017). Families of students with mental health needs require the reassurance of a clear plan for prevention and intervention that should be communicated intentionally, especially if/when they disclose their child’s mental health status. Once aware of parents’ concerns for their child’s mental health, school professionals must help families secure information, services, and advocacy to address mental health needs.
In addition, teams should be prepared to include the input of outside agencies who are involved with families to provide maximum coordination and support. Although many students with disabilities depend on supports from outside agencies, effective interagency collaboration has been challenging because of educators’ lack of preparation to create linkages with those outside agencies (Noonan et al., 2008), particularly mental health agencies (Cornell & Sayman, 2020). Many teams do not know, and therefore underutilize, this critical step of establishing interagency collaboration. If the student is accessing mental health or other services outside of the school, the school team should actively seek parental, and when appropriate, student permission and releases of information to talk with their outside counterparts. The sharing of information can lead to generalization and strengthening of skills across settings—a much more powerful outcome than operating in isolation. The IEP meeting is the perfect opportunity to weave the “out with the in.” In other words, the IEP team has a golden opportunity to learn from families, leverage their outside resources, connect them with resources, and, in the case of a student with mental health needs, develop and support a robust home/school relationship. The IEP meeting is also the place for multiple service providers to cross-collaborate for effective sharing of ideas that are otherwise kept largely in one’s own classroom or therapy room.
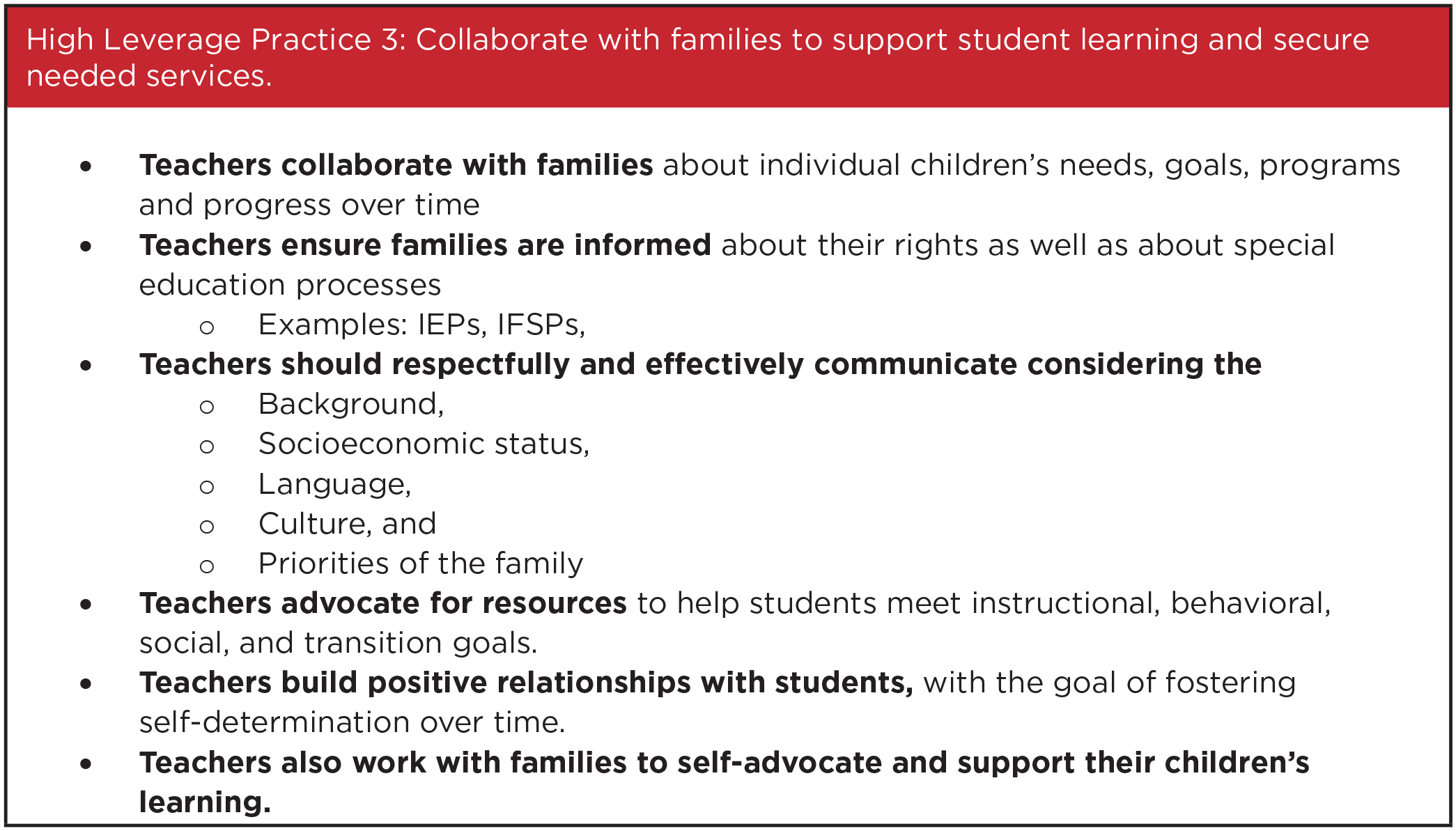
Families may feel overly cautious about disclosing information regarding their child’s needs for fear of breaching confidentiality or receiving judgment. Presenting the school’s overall approach for social and emotional health as planned and beneficial for all students can help normalize the school-based mental health services and assist families to understand that information shared will be used to support their child’s needs. Openly and proactively communicating that the school’s philosophy is guided by a tiered level of interventions focused on meeting the needs of the whole child, rather than a deficit view of “fixing problems,” may be extremely comforting to a family that is otherwise reluctant to trust or participate. This leads us to the third HLP (see Figure 4), which assists teams to truly include families as partners.
High-Leverage Practice 3
The third high leverage practice involves building a positive relationship with family through the identification of their strengths, goals, and visions: “Be sure to create an authentic, collaborative partnership with parents by respecting and including their input for a shared vision of their child’s future” (Lesh, 2020, p. 279). Due to cultural challenges and a lack of understanding of the American special education system and parental rights, many CLD families have difficulties sharing goals and advocating for their children (Achola & Greene, 2016; Lo, 2019).
The previous vignette of the steps the team took to support Elijah assumed that he had routine and consistent access to mental health services outside of the school setting. What does a team do if this access doesn’t exist? For many families, access to services is a wish, not an absolute. Schools can help to connect families with important resources that provide the coordination of services that are often necessary to meet the level of need. Let’s look at Elijah’s care from this perspective.
When the team hears about the family’s struggles with accessing consistent mental health providers, they prioritize this as a support area. In addition to initiating a reevaluation to determine his current needs, they assign the school counselor to assist the family to locate a single provider in practice who takes their insurance and who is a better match to Elijah’s unique needs and strengths. This provider begins treatment with the family about 2 weeks after the referral has been accepted. The school, as part of their support plan in the IEP, sets up a monthly meeting to collaborate with the new provider, the family, and the team. This meeting frequency is designed to decrease once the family indicates that they are seeing progress and continuity of care. The input from these meetings is considered in the quarterly meetings that Elijah is being trained to “run” as the lead. Elijah is also working with his school team to evaluate how his outside services complement and inform his school services. The team helps him to identify ways to increase access to the skills he’s working on in treatment. As a result, his anxiety decreases significantly while his set of coping strategies increases in all major life areas. Eventually, the team fades back the monthly meetings and instead relies on quarterly input to assess the data.
In this slightly different scenario, the team is identifying a need expressed by the family and is leveraging their knowledge of outside resources to assist in filling this gap. As a result, the family’s ability to access and utilize this important resource increases, with more consistency and success. The team also took the extra step of ensuring, through frequent communication, that the services were accessible and working for the family. This type of advocacy on the part of school staff can make a tremendous difference and positive impact on the family’s overall functioning and experience. The outside service world often contains both attitudinal and structural barriers, which are difficult for many families to overcome. Collaboration with families around accessing community services will identify what supports and services families, including those from CLD backgrounds, need to overcome those barriers and access appropriate and comprehensive services (Fallon & Mueller, 2017).
Elijah requires one more type of support in the school’s journey to provide services that are a match to his and his family’s needs, and that support must center on his identity as a Black male. As Dillard (2019) noted, “When Black students exhibit negative behaviors or become withdrawn, educators often label them as problems and subject them to reactionary, zero-tolerance policies and other practices that disproportionately affect Black students but don’t address the root causes of such behavior” (p. 47). Elijah started his high school year with a lack of trust in the school, his peers, and the environment. This was based on several factors, including sibling input, past experiences as a Black male, and anxiety based on his disability. His school team must support him from a culturally responsive stance and focus on what he needs to come to school each and every day feeling safe, engaged, and supported (Hammond, 2015). Too often, Black students experience harm from school systems, including the use of curriculum that is not culturally responsive, lowered academic expectations, and segregating Black students in special education (Dillard, 2019; Hammond, 2015). Furthermore, evidence confirming the racial disparities in child and adolescent mental health services for African American students (Alegría et al., 2015) necessitates an increased vigilance by school personnel to assure mental health supports are provided as needed. In classrooms, each of his teachers will need to intentionally develop authentic and respectful relationships with Elijah and his family, getting to know his interests, likes, dislikes, and dreams (Hammond, 2015). Additionally, they will need to design and deliver instruction and support needed to meet the academic rigor and needed for him to attain his postsecondary goals. His school team will also need to work with Elijah to identify groups and activities for him to participate in that will provide him with opportunities to develop positive peer relationships and leadership opportunities. All of this is further supported by his developing leadership skills with the IEP team and his transition planning, fostered by the encouragement and modeling of staff.
“The outside service world often contains both attitudinal and structural barriers, which are difficult for many families to overcome.
Conclusion
It’s the end of Elijah’s 10th-grade year at his high school. He is now a B student with a role in the student council. He’s an active member if not the leader of his IEP team and recently wrote his first transition plan with staff assistance. Elijah’s positive relationships with peers and staff have allowed him to find a “safe place to land” when he has particular difficulties, and he is able to use this support to get back on track. He continues outside therapy at the local clinic where his family was referred by the school counselor, which has been vital in helping him to understand that anxiety is manageable. He is able to openly discuss the strategies he’s learned in quarterly meetings and even gave a presentation to his teachers last spring to educate them about anxiety disorders and self-regulation/reframing strategies. His parents are an active part of every meeting and are always informed and aware of what is happening to and for their son. In retrospect, everyone at the high school has benefited from the collaborative relationship in positive ways. His future is brighter because of the active collaboration his school team developed to meet his unique needs. When asked what he wants to be when he’s older, Elijah confidently states that he wants to be . . . a teacher!
Students with mental health needs benefit from intentionally planned systems that focus on prevention, recognition, and action. An MTSS addressing children’s mental health needs integrates schools, families, and communities in a continuum of care (Vallancourt et al., 2013). In Elijah’s case, the outcome in absence of a planned system was an exacerbation of his anxiety disorder and school refusal. It does not have to be that way. As our field embraces school-based mental health services as one more tool in our arsenal, we are investing in the valuable futures of students in our care and their families. Collaboration is one of the key components of the investment.
“Students with mental health needs benefit from intentionally planned systems that focus on prevention, recognition, and action.
As described in the multiple vignettes above, collaboration took many forms to ensure procedural and substantive fidelity with the design and implementation of the IEP. Professionals took the disclosure and concerns of the student and family seriously and began a reevaluation to determine his current needs and present levels. The team actively and intentionally included the family and all service members to create a robust plan, with Elijah directly at the forefront. They empowered Elijah to grow in his self-awareness skills so that eventually the IEP became “his” road map. The school team also leveraged their knowledge of outside resources to assist the family, on their terms, to access consistent mental health care. Perhaps most importantly, the school took an active role in developing a collaborative relationship with his outside counselor to enact the most supportive interventions in both settings. When necessary, the team accessed training to deepen their skill set. The collaborative efforts illustrated here have the potential to change the trajectory of lives, strengthen the supports offered in an MTSS, and be a source of growth and professional development for teachers. Go forth and collaborate!
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.