
Abstract
Suicide has long been constructed as an individual, pathological problem of the mind, requiring a combination of clinical care and interpersonal support to prevent it. The endurance of this individualising and pathologising approach serves to reflect and maintain the marginalisation of sociology in suicide studies. This article contributes to redressing this balance, via analysis of creative, qualitative workshops, which formed part of a broader study exploring the politics of suicide. Informed by 33 participants’ contributions from six creative-response workshop groups, in dialogue with Lauren Berlant’s concept of ‘cruel optimism’, we propose a creative sociological (re)turn in suicide studies. Our analysis explores how the politics of UK suicide prevention constitutes a form of ‘cruel optimism’, obfuscating structural and sociological approaches to preventing suicide, and giving primacy to individual mental health-led interventions. We argue this provides a vital opportunity and urgent call for sociology to contribute more robustly to suicide research.
Introduction
Across research, policy and practice, suicide has primarily been constructed as a pathological problem of mental illness contained within the mind (Marsh, 2010), in part perhaps owing to the domination of psychology and psychiatry within suicide studies, and the relative absence of sociological perspectives (Wray et al., 2011). As such, suicide is often unquestioningly described as the tragic consequence of untreated or under-treated depression (Hjelmeland and Knizek, 2017), distorting a person’s perceptions and leading them to ‘unnatural’ desires for death (Tack, 2019). This framing, as has been argued elsewhere in work on depression, can have a depoliticising effect (Sandell and Bornäs, 2017), situating suicide as a health problem, and in turn reducing the possibilities for considering how socio-economic and political contexts might also play a role (Daley, 2020).
Psychologised framings of suicide that prioritise individualisation and pathologisation have consequences for suicide prevention, shaping the types of actions and approaches that are prioritised (White and Morris, 2019). Critical analyses of national suicide prevention policies, including our own, have argued that policies emphasise help-seeking, individual resilience and talking about suicide, rather than more structural or systemic forms of suicide prevention, such as addressing socio-economic inequalities (Fitzpatrick, 2021; Marzetti et al., 2022; Oaten et al., 2023; Pirkis et al., 2023). We term these dominant psychologising approaches the ‘mental health model’ of suicide prevention. However, despite emerging policy analysis in this area, to our knowledge no research has sought to understand how the public respond to political discourses about suicide and suicide prevention, which appears myopic given the pressing importance of the topic and the recognition across research areas of the need to include diverse voices, and particularly those with lived and living experience, in suicide research (Daya et al., 2020).
In this article, we explore public responses to the (a)political framings of suicide prevention as a matter of mental health in UK policy and political debates (2009–2019), as well as nine charity documents, through six series of ‘live’ (Back and Puwar, 2012) creative-response workshops held with groups identified in UK suicide prevention policies as at risk of or vulnerable to suicide, and practitioners working with them. These workshops build on our earlier work using critical, post-structuralist analysis to explore constructions of suicide and suicide prevention in the aforementioned documents (Marzetti et al., 2022, 2023; Oaten et al., 2023), using illustrative extracts from this analysis as prompts for the creative-response workshops. Using ‘live’ methods allowed us to explore meaning making dynamically in relation to participants’ engagement with UK suicide prevention policy and politics, reflecting that knowledge and theory are not static, nor neutral – but rather occur within and between relationships (between researchers, participants, their life worlds and the otherwise ‘dry’ material of political debate and policy). To help us theoretically navigate our own, and our participants’, engagement with the politics of suicide prevention, we draw on Lauren Berlant’s concept of ‘cruel optimism’. In the following sections, we introduce the intellectual context of our study – the topic of suicide, and the different ways that disciplinary practices and alliances have shaped understandings of suicide prevention; before turning to Berlant’s work, introducing the concept of ‘cruel optimism’ and indicating the ways in which it helped us to think with our data on the politics of suicide prevention.
Exploring Conversations between Psychology and Critical Sociology
While the mental health model of suicide prevention tends to centre individual pathology, an examination of socio-economic factors is not absent from suicide research. Indeed, socio-economic status is widely acknowledged in research as patterning rates of suicide, with lower socio-economic status associated with higher rates of suicidal thoughts, attempts and deaths (Cairns et al., 2017; Iemmi et al., 2016; Stack, 2021). This was reflected in our critical analysis of the eight suicide prevention policies in use in 2009–2019 undertaken in the first phase of this research, with lower socio-economic status identified as a risk factor for suicide (Marzetti et al., 2022; Oaten et al., 2023). However, we suggest that in the psychologising framework used within much policy and research, socio-economic factors are framed as external, ‘distal’ features that may affect an individual. These may be acknowledged or ‘controlled for’, ultimately leaving the roots of such risks uninterrogated, and certainly not considered as the consequences of social problems rooted in political decision making (Button, 2020). Rather, socio-economic problems were positioned as unfortunate pre-cursors to suicide that come from nowhere but lead to death.
To counter dominant framings, there have been important critical interventions, with recent sociological scholarship thinking with and between social structures, risk factors and the embodied, emotional affects they may produce (Abrutyn and Mueller, 2014; Chandler 2019). China Mills (2018) takes this approach in her psychopolitical autopsy of UK austerity suicides, arguing that although there is a relationship between having a low income and ending one’s life by suicide, additional affective elements are often unaccounted for: for example, that people in receipt of benefits are routinely positioned by the government, media and wider society as burdens, and that this stigmatisation is additionally difficult to live with (see also Tyler, 2022).
Mills’ argument is particularly salient because one of the core psychological frameworks underpinning understandings of suicide, Thomas Joiner’s (2006) Interpersonal Theory of Suicide (IPTS), positions perceived burdensomeness as one of the key stages in the development of suicidality. Proponents of IPTS often explain this is not because people are burdens, but is instead a problem of distorted perceptions due to mental health problems. Mills’ argument offers us a different way of understanding this, one that frames perceived burdensomeness, not as contained within the pathological minds of suicidal people, but rather as problematic socio-political positionings, which prompt affective responses among those that are subject to them. In this article, we are interested in the affective dimensions of the mental health model of suicide prevention, which, as we have argued previously, has dominated UK policy responses to suicide (Marzetti et al., 2022; Oaten et al., 2023). We now turn to Berlant to help us begin to theoretically navigate this affective domain.
Cruel Optimism
Lauren Berlant’s (2011: 1) ground-breaking work Cruel Optimism proposes that: ‘a relation of cruel optimism exists when something you desire is actually an obstacle to your flourishing’. Situated in cultural studies, Berlant was particularly interested in attachments to the notion of the good life under capitalism in post-Second World War USA: seeking to explain the moral-intimate-economic relationality to the good life. Berlant proposed that optimism becomes cruel when one becomes so attached to the possibility of the ‘good life’, that the pursuit of it becomes an insatiable desire that can feel impossible to step away from or critique. To do so would mean giving up on hope itself, which would be more painful than repeating the cycle of dissatisfaction. Berlant termed this a ‘double bind’, in which one experiences attachment to the object of hope – the ‘good life’ (the first bind) – which is compounded by a further affective attachment to the affective feeling of hopefulness itself (the second bind), fuelling a desire to maintain optimism for the ‘good life’, regardless of success or futility in attaining it.
To apply this logic to suicide, we stay with the example of socio-economic disadvantage, and, more specifically, austerity, 1 as a contributor to suicidal distress. We argue that conceptualising suicidal individuals as incorrectly perceiving themselves to be a burden because of the distorted perceptions rooted in individual mental health problems, usually depression, provides a logic that directs us towards the mental health model of suicide prevention as a primary pursuit. Through this construction, medication, talking therapies and the support of friends and family are illuminated as primary routes to wellness. We argue this dominant pursuit of the mental health model, without accompanying consideration of structural forms of suicide prevention, is a manifestation of Berlant’s double bind.
To illustrate, we borrow from Imogen Tyler’s (2022) Stigma: The Machinery of Inequality, in which Tyler shares the story of Stephanie who, after repeated spells of serious illness, loses her job and applies for benefits. Stephanie’s story is not simply one of financial difficulties, it is also one of social challenges. Stephanie is claiming benefits at the height of UK austerity, through a welfare system designed to be difficult to navigate, at a time where the media, supported by government, were filled with hostility towards benefit claimants, contributing to a culture of stigma and shame.
When Stephanie received a letter informing her that some of her benefits would be stopped, pending an investigation of a possibly erroneous benefits claim, her mental health deteriorated. Tyler provides us with an account of crisis, with Stephanie harming herself, then being forced, despite her injuries, to attend the Job Centre, as non-attendance could result in further benefits cuts. However, on arrival Stephanie was not allowed in, she was bleeding and clearly in crisis, and such a visible display of distress was not allowed inside the Centre. Tyler explains that the form was brought outside for Stephanie to sign; with no one checking how she was or offering help, an encounter that was wholly dehumanising.
Holding Stephanie in mind, let us return to the logic of cruel optimism: Berlant (2011: 2) argues that ‘optimism is cruel when the object/scene that ignites a sense of possibility actually makes it impossible to attain the expansive transformation for which a person or a people risks striving’. Building on this, in The Cruel Optimism of Racial Justice, Nasar Meer (2022) proposes that experiences of racial injustice can be understood as a felt, affective crisis that is terrible and traumatic, but also simultaneously a small part of a picture of crisis ordinariness, of systemic and structural choices that fail people who, if different choices were made, could be given justice. Applying this to our ‘scene’, it seems clear to us that while Stephanie might have benefited from mental health care: medication, talking therapies, support from her personal network or even, as we have previously critiqued, the Job Centre staff being trained in suicide prevention (Marzetti et al., 2022; Oaten et al., 2023), these would not sufficiently address the roots of her difficulties. Indeed, if that were all that Stephanie was offered, it is unlikely she would be able to maintain a sense of wellness, because Stephanie’s difficulties are significantly impacted by austerity, which could only be addressed through welfare reform.
Despite the seeming obviousness of the need to both provide mental health support and address the socio-economic and political barriers to living experienced by Stephanie detailed here, the suicide prevention policies, political debates and charity documents analysed in Phase One of this research, appeared to us to remain focused on the mental health model of suicide prevention – an approach that prioritised individual resilience, interpersonal support and clinical care. The question we were left with following this critical policy analysis was, did this appeal to those most implicated within the policy, namely groups of people identified in the policies as at risk of or vulnerable to suicide, and the practitioners working with them?
Methods
Phase One of this study examined dominant framings of suicide prevention in policies, political debates and charity campaigns; while Phase Two explored how these framings resonated with or were resisted by lay members of the public. We used ‘live’ methods to reflect the dynamic nature of meaning making and (political) contestation. Thus, the vitality and liveliness of research was attended to as a key part of the research process, acknowledging our role as researchers in the production of knowledge within, and beyond, the research encounter (Back and Puwar, 2012; Simopoulou and Chandler, 2023; Tarr et al., 2018).
The ‘live’ methods we drew on in Phase Two were ‘creative-response workshops’ (Simopoulou and Chandler, 2023), enabling recognition of the potential difficulties of talking about suicide, which can be a highly emotional and stigmatised topic; offering an alternative to verbal communication (Leavy, 2015; Mannay, 2016). Participants were given extracts of data from the policies, political debates and charity documents that were analysed in Phase One (termed ‘data packs’), including data that illustrated our key findings and facilitated the opportunity to engage – both creatively and in conversation – with a variety of different, sometimes contradictory, perspectives on suicide and suicide prevention. 2
While we hoped that using live, creative methods would open up possibilities for expression of thoughts and feelings about the politics of suicide prevention that might be harder to communicate verbally, we were conscious that creative expression is a skill. As such engagement in creativity, if a participant is either unfamiliar with the method of expression, or lacks comfort or confidence with creativity, could be intimidating. This was proactively brought up by prospective participants when they expressed interest in the study, with the majority explaining that although they were interested in the politics of suicide prevention, they were ‘not arty’, signalling discomfort with the creative elements of the workshops.
Responding to participants’ concerns, we used a mixture of collaging, letter writing and black-out poetry, chosen for their accessibility to participants regardless of creative ability or experience. We also emphasised that the purpose of the creative activities was to enable participants to explore the data in ways that were productive for them, and provide opportunities for expression beyond words, but that we would not ‘judge’ their creative outputs and they did not need to share them with us if they did not want to.
Sample
We ran six workshop series (Table 1), recruited using social media (Twitter, Facebook and Instagram) and by contacting pre-existing groups working with people identified within the UK suicide prevention policies as at risk of or vulnerable to suicide. There were three groups of LGBTQ+ participants; one group that was open to anyone (but ultimately all participants had personal, lived experience of either suicidal distress, supporting someone else with suicidal distress or being bereaved through suicide); a group of practitioners and researchers working with people who had experience of imprisonment and the criminal justice system (current or past); and a group of volunteers from a listening service. Our participants included a range of people with diverse relationships to the topic of suicide, representing ‘publics’ who might be differently affected by suicide prevention policies and practices, through experience of suicidality, suicide bereavement and by taking an active role in supporting people living with suicidal distress.
Overview of creative workshops.
The 33 participants were aged between 16 and 69; lived across England (19), Scotland (11) and Wales (2), with one person preferring not to disclose their location. The majority of participants described their ethnicity as white (31), one as African and one as Bangladeshi. Twenty-two participants identified as female; three identified as male; six were non-binary (an umbrella term including genderqueer, agender and queer people); and two participants preferred not to disclose.
Recognising the complexities of monitoring social class, we asked both about participants’ housing status and occupations. Fifteen participants were homeowners; eight were living with parents or carers; five were privately renting, and a further one person was renting in social housing; two lived with partners, where the partner was a homeowner; one participant was staying with friends at the time; data was missing for one participant. Eleven participants lived in areas experiencing the highest amounts of deprivation (deciles one–five; with one participant in Wales, three in Scotland and seven in England); while 15 lived in areas experiencing lower levels of deprivation (deciles six–ten; 13 in England and two in Scotland). There was missing data for seven participants. Twenty-four participants were employed (two in addition to being students); five were unemployed; two were retired; three were students; and data was missing for one participant. Using the Office for National Statistics’ major groupings of occupations, we categorised participants who disclosed more detailed information about their occupation. Twelve participants were employed in professional occupations; five in associate professional occupations; three in care, leisure and other service occupations; one in administrative and secretarial occupations; one in an elementary occupation; and one in a managerial, directorial and senior official occupation. 3
Ethics
Given the sensitivities of the subject being discussed, the online workshops were facilitated by two members of staff (HLM and AO): one person led the activities, while the other could observe the chat-box and was free to talk if a participant became distressed during the workshop (although this was not ultimately needed). In Workshop Four, which was in-person and facilitated by HLM alone, the group’s regular facilitators were available throughout, ready to provide support if it had been needed. During online workshops, we planned a ‘soft ending’, with the researchers staying on the video call for 15 minutes after the end of planned activities. This was explained to participants as a virtual transition space, in which they were invited to ‘hang out’ and participate in ‘small talk’ if they wanted a gentler transition out of the workshop. Participants particularly made use of this space in Groups One and Three. We also offered participants the opportunity to chat between workshops if something had come up for them, although only one participant (from Group Two) made use of this.
The study was given ethical approval by the University of Edinburgh’s School of Health in Social Science’s Research Ethics Committee. With participants’ consent, five out of the six workshop series were audio recorded and professionally transcribed. Group Four was a pre-established group that used the workshop as just one activity on offer during their regular group activities, and selected not to be recorded, with participants instead writing a narrative to accompany their creative work if they chose to, rather than engaging in discussion. Participants were invited to donate their creative works to the project. All transcripts were anonymised, with participants given the opportunity to choose their own pseudonym.
Analysis
Analysis of the transcripts and creative works was led by HLM using Reflexive Thematic Analysis (RTA) (Braun and Clarke, 2022) to move abductively between the data, individual reflections on it and existing theory to help strengthen and deepen the analysis (Timmermans and Tavory, 2022). Our analysis was guided by our research questions – seeking to understand how participants, across different groups, responded to, understood and made sense of the ways that suicide prevention was framed in UK suicide prevention policy, political debate and charity documents. This approach is underpinned by an appeal to slow, immersive and in-depth approaches to analysis that embraces the spirit of adventure (Braun and Clarke, 2022) and surprise (Timmermans and Tavory, 2022). To do so, HLM worked in non-linear and iterative ways between RTA’s six phases, in discussion with AC, AO and AJ: (1) data familiarisation; (2) data coding; (3) initial theme generation; (4) theme development and review; (5) refining, defining and naming themes; (6) writing up. In the following sections we demonstrate how participants across the workshops discussed and responded to the data from Phase One. These findings are read through and connected to Berlant’s cruel optimism, facilitating further insights and implications, which we expand in the Discussion section.
Conversations about Suicide as Haunted by Blame
Across the workshops, it became apparent that discussions about suicide and suicide prevention were haunted by questions of blame and responsibility. As such, there was a sense of stickiness (Ahmed, 2014), such that a conversation about what suicide and suicide prevention are, was almost instantly transformed into a discussion about who is responsible for keeping a person alive and who is to blame if someone dies. This was particularly apparent in the first workshop with Group Two, in which we shared our three-page introductory data pack. Participants were invited to use collaging methods to explore and respond to them, before engaging in group discussion, part of which centred on whether participants saw the data as political. Participants in the workshops (particularly those held online, where recruitment had been conducted via social media) were likely to already be open to the idea that suicide prevention was a political issue, as they were recruited to take part in creative-response workshops about the politics of suicide prevention: a lot of my symptoms are exacerbated by external things that are political. So, when they try to take the politics out, it makes it a personal, you problem – you are not resilient, you can’t cope, you [. . .] actually, it’s like, no, well some people are really feeling depressed because they can’t afford things, they can’t afford food [. . .] So, when they take out the politics of mental health and suicide prevention, it makes it a personal issue, when actually, I think it’s . . . it’s not. (Elizabeth)
Responding to the introductory data pack, Elizabeth’s argument represented a sentiment shared within the group, that governments deliberately manoeuvred suicide outside of the political sphere and into the personal, shifting responsibility away from social conditions, and in doing so allowing governments to shield themselves and their actions from scrutiny; framing suicide as a personal problem and simultaneously de-politicising suicide and its prevention. Building on this, Emma offered a reflection on the consequences of such depoliticisation on mental health care, from their perspective as a practitioner: Even in, like, mental health services, we’re treating anxiety and depression, but we’re seeing it as that person needs to change something. You know, if they do something different in their life, then they’ll be better. When actually, you know, like, if you can’t afford to pay your bills, or you know, you can’t feed your kids, you know. [. . .] We’re just trying to mask their symptoms, and again, exacerbating the problem and saying it’s their fault. (Emma)
Speaking from slightly different experiential perspectives, nevertheless both Elizabeth and Emma’s accounts are underpinned by an understanding of the difficulties of living with socio-economic deprivation, and the inability of mental health care and treatment to ameliorate this, even though this was not a topic that was explicitly addressed in the data pack. Their accounts resonate with the neoliberal logic that Berlant (2011) argued applies to our understanding of health problems such as depression and obesity: that people are expected to engage with the very systems that contribute to the production of sickness in order to make them well. In this context, this neo-liberal logic responsibilises suicidal people for their own recovery, which by extension can engender the sense of failure described in Elizabeth’s account, and blame that we see in Emma’s, if an individual does not recover. This process encourages a sense of responsibility for one’s own recovery to be projected onto suicidal people, and simultaneously manoeuvres the possibility of suicide as a socio-economic problem that could invite political solutions away from view.
Anyone Can Be Suicidal
The majority of participants in Groups One–Five troubled the absence of suicide prevention methods designed to address systemic and structural contributors to suicide. However, this view was not shared by all. In Group Three, Marianne simultaneously resisted both the idea of suicide as a mental health problem and as a structural problem. Reflecting on her own experiences of losing her son to suicide and of connecting with and supporting others bereaved by suicide, she indicated that suicide was a response that anyone might have, if faced with significant challenges that they felt unable to overcome, regardless of socio-economic status, marginality or mental illness: I built that bonfire [in her collage] because it just seems to me that the language about the people that we’re talking about here, it’s as if . . . I mean, some are worse than others [. . .] but there’s a sense that there’s, [puts on a voice heavily laden with sympathy, mimicking policy makers and politicians] ‘oh you’re having these problems with how you’re feeling’, and, ‘oh you’ve got mental health problems, you need some help, you need some interventions, you need to do something about your state of mind and vulnerability’. And that’s very often not what’s going on at all. What’s going on is that someone is in a situation that they just cannot see a way out of. [. . .] they just haven’t got the strategy or [. . .] something feels impossible. You know, they’ve just been packed in by their girlfriend or they’ve failed their exam [. . .] and actually they haven’t got mental health problems. But they’ve collided in to a situation [. . .] and I feel like we just start saying, ‘oh shall I refer you to a counsellor?’. You know, I can . . . it’s . . . it ain’t gonna work. (Marianne, Series Three, Workshop One)
Marianne’s explanation seems to resist what she interpreted as the pathologisation of normal human responses to personal and interpersonal difficulties. In part this appeared to be connected to Marianne’s efforts to disrupt a singular construction of who could be understood as suicidal, which was particularly important as she described her own son as ‘pissed off’ and ‘angry’ prior to his death and therefore not fitting with the dominant construction of a sad or vulnerable suicidal person who might be imagined as the object of suicide prevention efforts. Marianne continuously emphasised that the kinds of suicide prevention she felt were needed were not professional ones, but instead kindness from all, including strangers, in response to all expressions of distress, including anger.
Marianne’s perspective, that anyone could be suicidal, was echoed in Group Six – a one-off workshop held for listening services volunteers, where participants also highlighted the universality of suicide: Lesley: Anybody can be vulnerable, can’t they? Somebody was talking to me recently and they said in their workplace, and there were high-achieving people there, they’ve had four suicide attempts in the last year, and I was really shocked [. . .] Blinker: It can come from a spur of the moment action or loss of a job or loss of anything, you know, a dear person in their life. Or it can come from the background they came from.
However, in contrast to Marianne, there appeared to be an acceptance that suicide was primarily a mental health problem within the group, with some participants offering examples of individuals they considered particularly vulnerable: I was a dinner lady last year and I looked after a class of five year olds, and it’s really interesting to see that even at that age, after spending quite a short amount of time with them, you can see the children that unless something happens, they’re going to have depression, and that sounds really awful, but you can see just the way they were wired already at four and five years old, the way they talk, the way they responded to things, you can see that unless something changes for that child . . . I know some of the families they came from, they’re nice families but those kids, they whinge incessantly, everything that happens is negative, negative, negative. (Chrissie-Clare)
Setting aside the problematic notion of a small child being ‘wired’ in such a way that they could be on an inevitable path to depression (the spectre of suicide hanging somewhat unsaid in the air over this conversation); there are perhaps parallels that can be productively drawn between the child from the nice family who whinges incessantly and has a negative outlook, and the adult who suffers from distorted perceptions of burdensomeness offered to us by the Interpersonal Theory of Suicide. Within Chrissie-Clare’s explanation of the children she looked after, we see the early origins of responsibility (and indeed blame) beginning to take root in the problematisation of the children’s ways of thinking, talking and responding. To some extent, suicidality here is framed as an almost patho-ontological problem with their way of being, absent within this is a consideration of the relationality raised by Marianne (that the child might be responding to interpersonal difficulty) or the structural challenges raised in Group Two.
Indeed, the reassurance that Chrissie-Clare provides that these children are from ‘nice families’ but are nonetheless ‘negative’ almost seems to respond to an anticipated question about what might be happening in children’s lives outside of how they are ‘wired’. To extend the metaphor, doing so allows us to focus on the child’s internal wiring (or psychology) as suicide prevention, without having to consider the more complicated and unwieldly landscape of their life. It allows a focus on what is more immediately and directly possible. We argue that it is this sense of possibility, that one can act now and effect change, that comprises the affective bind to the mental health model of suicide prevention: in contrast to suicide prevention as socio-economic, political and structural transformation, which requires more power than perhaps is commonly felt.
The Mental Health Model of Suicide Prevention Promotes a Sense of Possibility
A call for ‘upstream’ suicide prevention efforts united participants across all workshop series, although their suggested methods of implementation were diverse. In contrast with Groups One–Five, participants in Group Six acknowledged socio-economic and political contributors to suicide, such as benefit sanctions or toxic workplace cultures, but tended to focus on individual and interpersonal methods of prevention; potentially because – as volunteers at a listening service – this was seen as within their area of expertise and something over which they could effect change. They advocated for the creation of a healthier culture focused on building resilience, encouraging positive thinking and developing inner strength. In doing so, it appeared that the participants embraced a neo-liberal logic that placed within each individual the power, and thus responsibility, for their own resilience and recovery.
Group Six proposed that it should not be the government’s responsibility to provide care across multiple areas including suicide prevention and instead this should be the role of the community: Robert Zimmerman: There’s the notion that the government should pick up everything, but potentially that’s terrible because [. . .] that’s saying you want a one-to-one relationship between everybody and a professional. What’s actually, and you were alluding to this earlier, highly desirable is that people live in community where you don’t wait to have a worker to come round and see you with their clipboard, you just want to see your mates and talk about real heartrending issues with your mates. [. . .] Blinker: You don’t need to be a professional or do anything extraordinary; an open conversation about suicide and listening and talk about how we can help save lives. And sadly we can’t save everybody, but if we can save some that’s all that matters really.
These participants challenged the professionalisation of suicide prevention, in a manner that seemed consonant with the vision that was often provided in the documents analysed in Phase One: that talking about suicidal feelings was the primary way to prevent suicide and that anyone could have such conversations. This discussion of saving lives underlines the affective dimension of suicide prevention that we argue binds those who view themselves as preventers to the mental health model. Simultaneously this orientation empowers and responsibilises; however, given the limitations of individual power discussed elsewhere, this then constitutes a double bind – encouraging further action, which may ultimately ‘not work’.
The Mental Health Model as Suicide Postponement
The positioning of suicide prevention as a type of care that should be provided by one’s community was simultaneously embraced and resisted by the majority of participants in Groups One–Three. Participants portrayed talking about one’s suicidal feelings and being listened to as important, and saw the provision of community care as necessary for this. However, they were also clear that this should not be a replacement for statutory services. Rather, they indicated that community care was needed due to gaps in government care for marginalised communities, specifically the LGBTQ+, minority ethnic and socio-economically deprived communities that the majority of these participants belong to.
Discussing his response to the Black, Asian and Minority Ethnic suicide and suicide prevention data pack and the austerity and suicide prevention data pack (depicted in Figure 1), Will explored the limitations of both professionalised mental health support and charity provided listening services as the sole methods of suicide prevention offered: I feel quite strongly about palming responsibility off onto charitable organisations and putting the responsibility on the individual or the community to deal with the problem. When to me, the underpinning issue is very systemic and full responsibility of the government to fix it, rather than saying we need to train more psychiatrists. We do, like . . . that’s another thing. We need to signpost people to mental health charities, you know. Yeah, text this number and somebody will talk to you. Which are all good things to an extent but I feel that a lot of the solutions that are proposed are just plasters being slapped on instead of actually addressing the root causes. (Will)
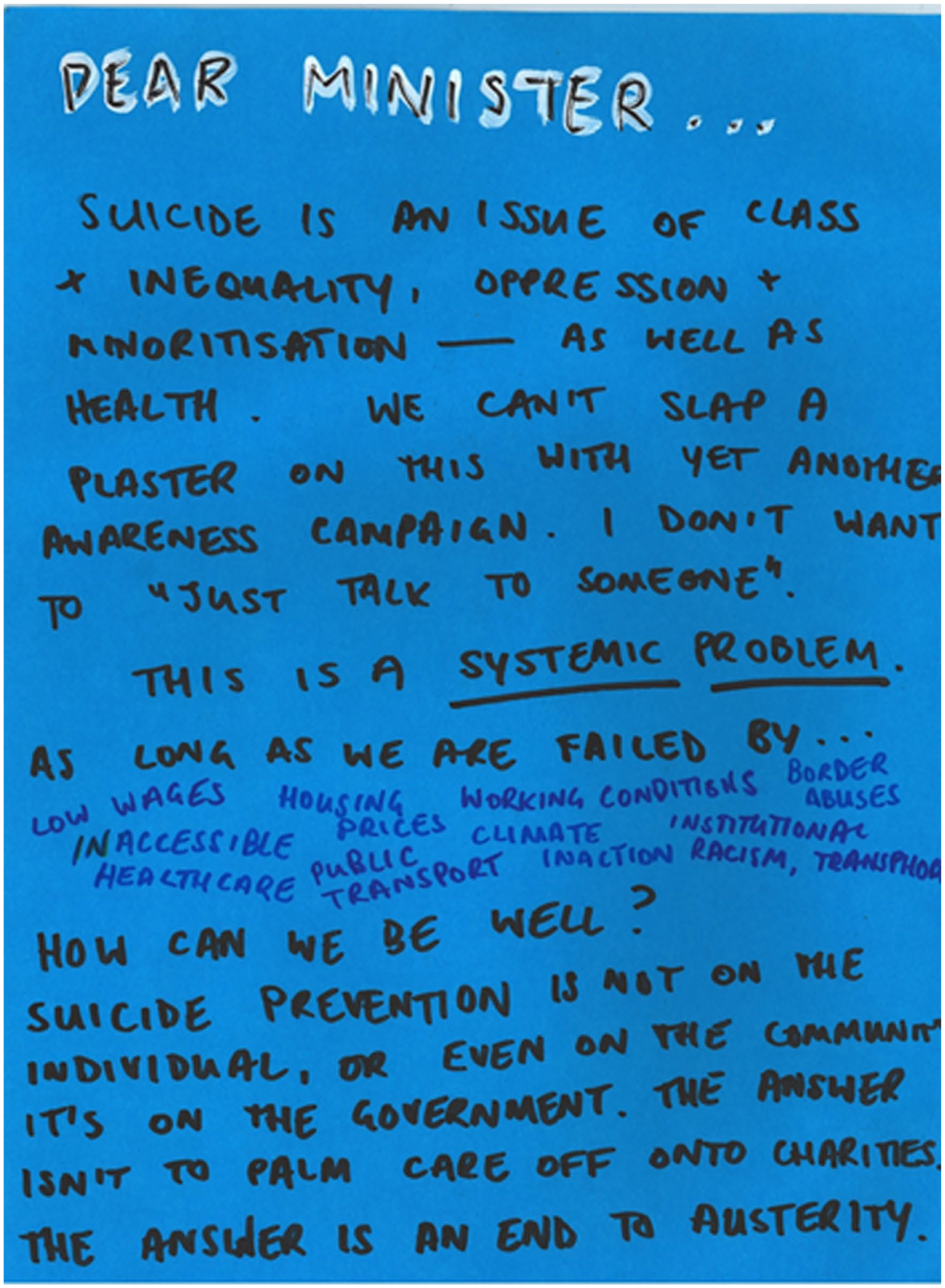
Will – Dear Minister. . . so what are you gonna do about it this austerity thing? (Suicide in/as Politics Exhibition, 2023).
The need to address the roots of distress beyond the ‘sticking plaster’ of the mental health model, can also be seen depicted by Alex in Figure 2. Both figures explicitly name oppressive, structural forces, gesturing towards the systemic burden of suicide faced across a number of marginalised communities named within policies and debates as being at risk of suicide. But rather than conceptualising identities themselves as risks as often appeared to be the case in the policies (see Marzetti et al., 2023), participants’ creative works positioned this riskiness as situated within society’s structures. As perhaps most explicitly put forward in Figure 2, where Alex has written ‘a cup of tea and a bath can’t fix a terrible world to live in. Make the world easier to survive in.’ This sentiment was neatly summed up by Hollie (Group Three) who described the focus on mental health methods of suicide prevention, without a corresponding attention to the systemic contributors to suicide, as ‘suicide postponement’ rather than suicide prevention.
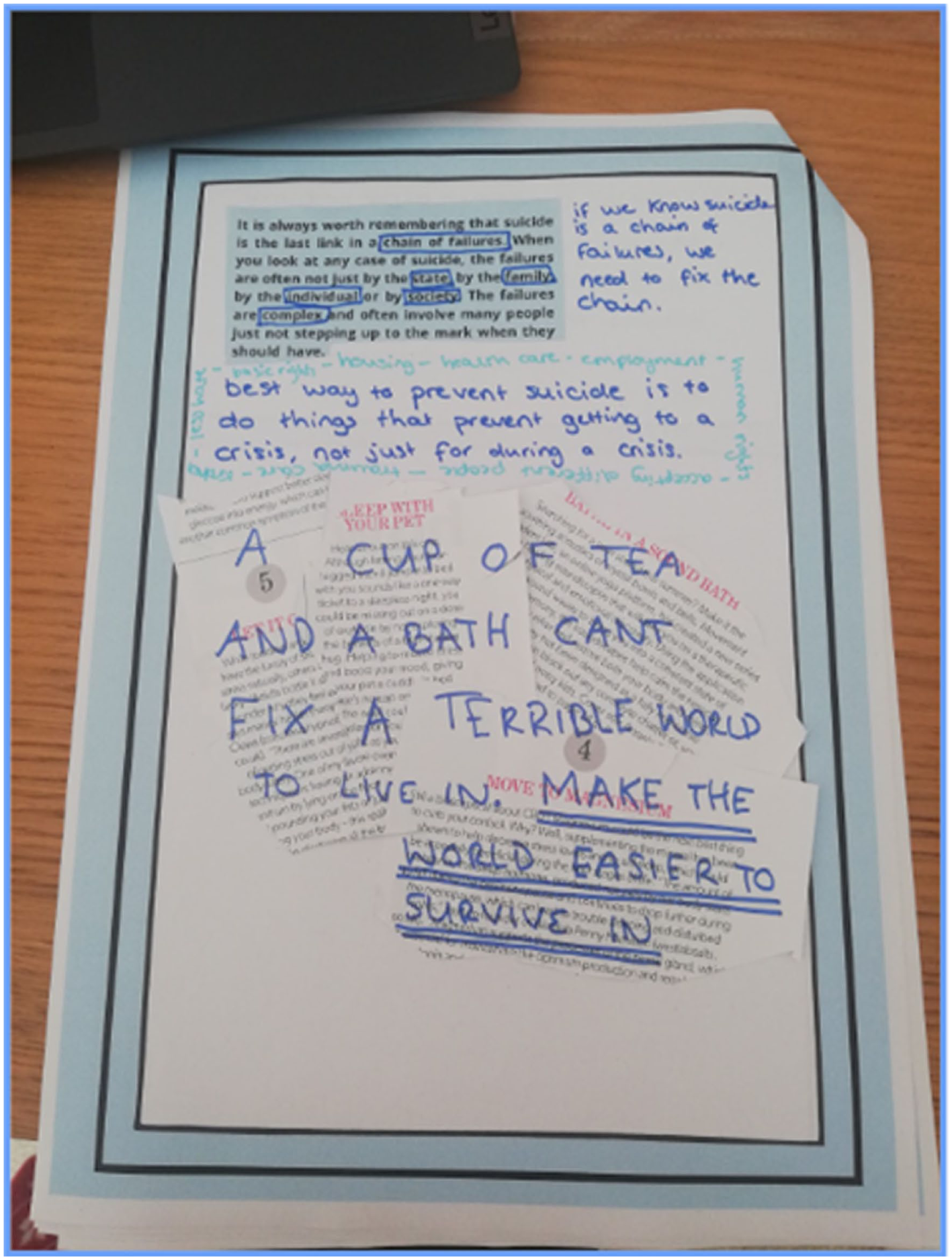
Alex – frustrated queer who finds surviving in a world set up to make existing difficult reflects on how life can be made easier to continue. (Suicide in/as Politics Exhibition, 2023).
The motif of the sticking plaster of suicide prevention was repeated by Helen in Group Three, drawing on her own positionality of living in ‘an area of disadvantage’: I’ve got this kind of like image in my head of like almost being like a mummy. You know, like embalmed . . . and sort of really tight like this, and that the wounds are seeping. You know, because of all the plasters. You know, like how many more plasters can you put on. It stinks. It’s putrid. You know, so how many more plasters, you know, can you actually slap on, you know, to communities. (Helen)
We suggest that this very visceral description of the mental health model of suicide prevention, as a poorly adherent sticking plaster over the putrid wound of socio-economic deprivation, also helps us to understand the affective bind to do something in the face of immediate crisis, to avoid being a passive bystander or silent witness to this traumatic scene. However, as Helen so vividly depicts here, and as Nasar Meer (2022), describes in his account of the cruel optimism of racial justice, while this wound may seem fresh to the outside eye, the wounded individual knows that this is just one manifestation of a ‘crisis ordinariness’, the history of which weaves its way through the present, the past, the future. This crisis is not contained in a single moment, and to see it that way is to miss the point entirely, for the root causes are not at hand nearby, but instead lay invisibilised in the very systems that we hope will help, but that as this argument suggests, also harm.
Discussion: The Cruel Optimism of Suicide Prevention
It has been argued in both critical suicide studies (Button, 2016; Fitzpatrick, 2021; Mills, 2018) and in mainstream suicide research (Pirkis et al., 2023; Reeves and Stuckler, 2016) that more attention should be paid to the socio-economic and political structures in which suicide occurs, and the ways in which these get under the skin (Chandler, 2019). However, the mental health model of suicide prevention has maintained primacy within suicide prevention policies, politics and practices (Fitzpatrick, 2018). This reflects the dominance of the psy-disciplines, and the relative marginalisation of sociological perspectives in suicide research. In this final section, we return to Berlant’s theory of cruel optimism to explore how the felt affect of the mental health model can bind us (researchers, policymakers and diverse ‘lay’ publics) to individualistic ideas about recovery and resilience, encouraging a divestment of our attention from the structural politics of people’s lives – an area that would otherwise offer fertile ground for sociological intervention. A key part of this return focuses on using Berlant’s theory to navigate the space between the two almost opposing positionalities expressed by our participants: with some invested in the mental health model as a primary method of prevention (with the structural acknowledged, then swept aside), while for others structural forms of suicide prevention were given primacy (with the mental health model seen as playing a secondary role).
As a brief reminder, Berlant (2011: 2) proposes that: Optimism is cruel when the object/scene that ignites a sense of possibility actually makes it impossible to attain the expansive transformation for which a person or a people risks striving; and, doubly, it is cruel insofar as the very pleasures of being inside a relation have become sustaining regardless of the content of the relation.
The ignition of optimism by the mental health model of suicide prevention was particularly pronounced within Group Six, which is perhaps unsurprising as Group Six was organised within an out-of-hours, voluntary listening service, providing the type of support suggested by this model. Group Six’s participants expressed that suicidal feelings were oriented within a particularly negative outlook that anyone can possess, echoing in more lay terms perhaps the ideas offered that suicidal feelings are rooted in psychopathology (Joiner, 2006). As such, in Group Six suicide prevention was constructed as an act of friendship: encouraging a suicidal person to disclose their feelings and then working with them to develop better resilience. This neoliberal logic that suicide prevention is in the power of an individual preventer creates the first loop in the affective bind, not only by offering hope, but also through the more subtle process of responsibilisation, wherein if the model is not working, the problem is in the implementation and not the model itself. This then creates the conditions for repetition, because if a failure of the model is attributed to suicidal people and suicide preventers, there is always the possibility that different, better, implementation may offer the hope of a better outcome.
While this construction of suicide prevention may invite us to feel a greater sense of agency, that anyone can save a life, critical scholars have encouraged us to question whether this sense of increased agency empowering as it can be, might be an act of governmental misdirection that encourages us to focus on our individual power, while quietly removing welfare resources that would facilitate alternatives to individualistic prevention methods (Button, 2016; Fitzpatrick, 2018). This individualisation of suicide and suicide prevention enables governments to obfuscate structural forces, such as socio-economic deprivation that are known to contribute to suicide (Cairns et al., 2017; Chandler, 2019; Reeves and Stuckler, 2016), which they could, but may choose not to, change (Mills, 2018). In constructing suicide prevention as an act everyone has power to do, responsibility is refracted across social actors, and the power to prevent becomes oriented around individual acts of reaching out, concentrated in both suicidal people, their loved ones, the practitioners they come into contact with; an act of deep depoliticisation.
A key question here is why has this depoliticisation not only been accepted, but embraced and celebrated through the mental health model of suicide prevention? We argue that this can be answered by the second loop in Berlant’s double bind, which can be found in the affective response to seeing suicidal distress as the seeping, putrid wound described by Helen. The pain of recognising this wound as gouged not by an individual injury, but as a consequence of crisis so long-term that it, as Meer (2022) suggests, could be considered ‘ordinary’. This recognition requires us to take up Mills’ (2018) invitation to reject the notion that this is a problem of perception, and instead see it as a problem of material reality, and socio-economic and political positioning. Through this recognition, a structural – perhaps sociological – approach to suicide prevention is repositioned, not as an accompaniment to the mental health model, but as a necessary condition for moving past suicide postponement and facilitating the potential for prevention. In acknowledging this symbiotic relationship between the mental health model of, and the structural approach to, suicide prevention, we propose that a repositioning of the latter also necessitates a repositioning of the former. As such, seeing the structural approach to suicide prevention as necessary for the success of the mental health model, requires also recognising that the mental health model cannot be successful without structural transformation. The cruel optimism of the mental health model of suicide prevention therefore, is that it dupes us into thinking that one is possible without the other.
Conclusion
Early on in our research we wondered how our critical policy analysis might ‘land’ with different audiences. The creative, ‘live’ methodological approach we developed enabled us to explore this question dynamically with diverse publics, each of whom brought different experiences with suicide, and broader positionalities (across gender, sexual orientation, social class, race/ethnicity and age). Our analysis of the data generated by these groups worked between the theoretical device of cruel optimism, and its affective binds, and the affective, dynamic discussions and ‘makings’ that happened in our creative-response workshops. This abductive, creative and interpretive process has driven further theoretical insights that help to further interrogate tensions, contradictions and absences in suicide prevention policies and parliamentary debates about suicide. Undoubtedly, had we engaged with other groups, we may have opened up further theoretical avenues, and future work in this area should certainly consider adapting these methods to work with different communities and individuals.
This article adds to a small, but growing, body of research exploring suicide and suicide prevention beyond the ‘psy’ disciplines, arguing for a creative sociological (re)turn in suicide studies. Our analysis underlines the urgent need for further sociological attention to suicide – an inherently structural issue that has been (like many issues associated with mental health) framed as wholly individual – a matter best dealt with by psychologists and psychiatrists (Fitzpatrick, 2018). Our analysis of participants’ accounts and creative contributions – put into dialogue with Berlant’s cruel optimism – exposes how the mental health model of suicide prevention can have affective appeal. We showed how this might empower ‘everyone’ to see themselves as potential preventers, but that this can also responsibilise suicidal people for their own distress and recovery, as well as responsibilising those around them. Participants’ engagement in the workshops demonstrated how these affective moves might be embraced, resisted and troubled. Further, our analysis underlines how focusing on individualistic methods of suicide prevention might enable structural forms of suicide prevention to slip from collective view. We suggest that the relative lack of sociological voices in suicide research and discourse can contribute to this unseeing. Ultimately, we propose that the obfuscation of structural methods of suicide prevention, and the simultaneous primacy of the mental health model, is a type of cruel optimism. It is essential that these two approaches must be seen in symbiosis, each necessary for the other’s success. However, to realise this goal, sociologists must more robustly engage with and contribute to suicide studies.
Footnotes
Acknowledgements
We would like to thank all the participants who took part in the workshops for their generosity of time and for sharing so openly with us. We would also like to thank Dr Veronica Heney for her feedback on earlier versions of this manuscript, and the reviewers for their helpful and encouraging comments.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this project was funded by a Leverhulme Trust Project Grant (RPG-2020-187).