
Abstract
This article focuses on young low-income mothers’ engagement with, and management of, potentially conflicting discourses within the context of maternal foodwork. Findings from qualitative, longitudinal interviews with 13 UK women illustrate the performance of identity and family work, in relation to infant feeding and wider maternal practices. Each participant was interviewed twice, once prior to, and then following, the birth of their first baby. We identify three rhetorical strategies. Adopting and resisting allow for the acceptance or rejection of prominent infant feeding discourses. Under reframing, young women transform the encouragement to breastfeed, subverting or reversing official discourses. Reframing thus provides an alternative means to appropriate and deploy versions of good motherhood, drawing on women’s lived realities and local maternal cultures, alongside wider experiences of building and managing family relationships.
Keywords
Introduction
Prior sociological studies identify the embeddedness of power relations within ‘maternal foodwork’ and how the classed nature of food practices contribute to notions of good mothering (Cappellini et al., 2016; Paddock, 2016). Young mothers on low incomes experience challenges meeting mothering ideals given the potentially negative discourses and associated stereotypes around their age as well as their access to material resources (Cooper, 2021). However, women can construct stories that function as identity work, seeking to counteract negative societal images (Carson et al., 2017) and present themselves as moral actors with respect to mothering ideals (May, 2008). We focus on how young mothers’ experiences and practices around infant feeding relate to prevalent discourses that recognise implicit links between breastfeeding and good mothering (Andrews, 2022).
We respond to calls for more research of a ‘socio-cultural kind that seeks to investigate women’s experience of feeding their babies in a context where breastfeeding is strongly promoted’ (Lee, 2007: 1076), acknowledging nuances to pro-breastfeeding discourses and its relation to the ‘policing of motherhood’ (Andrews, 2022: 56). Even in breastfeeding-friendly societies, Andrews (2022) highlights complexities; not only are there taboos around giving up breastfeeding too early but also continuation beyond a point that is deemed socially acceptable. Jamie et al. (2020) also demonstrate the operation of alternative moral norms for women in socio-economically deprived areas within the UK, illustrating the importance of both ‘resources and social location’ to the way in which mothers respond to ‘circulating discourses of maternal responsibility’ (Wright et al., 2015: 425). We therefore emphasise the importance of forging a more nuanced understanding of women’s local maternal cultures (LMC), referring to the way in which classed mothering norms are embedded within women’s familial and peer localities forming collective understandings of appropriate mothering behaviours (Paddock, 2016). Through this we shed further light on how responsibilities associated with maternal foodwork can be experienced by young low-income women, elaborating on the ‘diverse and situated everyday experience of mothering’ (Thomson et al., 2011: 8), given these social contexts are often overlooked (Braimoh and Davies, 2014).
We argue that LMC are key to understanding how young working-class women challenge and reverse the discourse (Foucault, 1978) that associates breastfeeding with good mothering and reconcile their infant feeding practices with a positive mothering identity (Murphy, 1999). In identifying three rhetorical strategies (adopting, resisting, reframing), we contribute to understandings of how agency is exercised in ‘assumed shared food narratives’ (Bissell et al., 2018) within the context of maternal foodwork. Rather than accepting potentially negative identity impacts, many young women seek to change the terms of the debate, developing more malleable understandings, with the reframing strategy providing the means to reverse the prevalent official discourse thus supporting a positive maternal identity. The participants expand the context within which infant feeding decisions are considered, to include wider infant care practices and family making, most notably by promoting paternal bonding.
We begin our literature review with a consideration of discourses around maternal foodwork in relation to infant feeding practices, and then outline the UK context before moving on to discuss the method and then findings.
Maternal Foodwork and Discourses of Infant Feeding
Recent sociological work has shed light on the importance of maternal foodwork (Harman and Cappellini, 2015), which includes ‘the practices that form the key food activities and exchanges’ (Wright et al., 2015: 422) and is largely seen as socially constructed (Paddock, 2016) and mothers’ responsibility (Cairns et al., 2018). Research has revealed complex class differences in the ways mothers engage in foodwork (Wills et al., 2011), with practices associated with upper and middle classes ‘prized, valued and aspired to’ (Beagan et al., 2016: 47), and helping (re)produce class inequalities (Brenton, 2017). Good mothering is associated with responsibility and self-sacrifice (Cairns et al., 2013) and informs intensive foodwork that is costly and time consuming (Brenton, 2017). Cairns et al. (2018) demonstrate how foodwork can be stereotyped at the boundaries, with both ‘Organic mom’ and ‘McDonald’s mom’ representing stigmatised classed positions, indicating complexity in women’s navigation of the classed norms and responsibilities involved.
Wright et al. (2015) therefore draw attention to the importance of examining the way in which differently positioned mothers talk about their feeding practices and how this is informed by potentially contradictory social and cultural norms. Understandings of discourses are crucial for appreciating how knowledge is produced and reproduced in society and frame individuals’ positioning in the world, both informing and being a product of power relations (Foucault, 1972). Dominant discourses establish normative standards (Beagan et al., 2016) and exploring the ways in which individuals engage with prevalent health discourses can help to identify the extent to which they are ‘internalized, transformed or resisted’ (Armstrong and Murphy, 2011: 317). However, other maternal discourses circulate through a diverse range of channels including healthcare professionals, media, friendships and family (Beagan et al., 2016) and reflect the influence of social and economic circumstances on experiences and practices (Braimoh and Davies, 2014).
Official infant feeding advice draws on a range of medical debates as well as social and maternal discourses reflecting broader shifts towards individual responsibilisation for health (Brenton, 2017). The World Health Organization (WHO, 2018) recommends breast milk as the sole source of nutrition for babies up until the age of six months. While breastfeeding is linked to social constructions of good mothering (Andrews, 2022) some evidence promoting it has been challenged (Lee, 2011); in particular the role in infant bonding (Jansen et al., 2008: 503). However, women are increasingly pressured to account for their infant feeding practices, and the use of formula milk can leave women open to charges of maternal deviance (Murphy, 1999). This construction of mothers as ‘gatekeepers of their children’s health’ ignores the extent to which inequalities inform the way women experience and attend to such discourses (Brenton, 2017: 864). The ‘imperative’ to breastfeed does not reflect all mothering concerns, which might include mothers’ experiences of pain and discomfort and challenges/tensions associated with paid labour (see Lee, 2011 for a review). Suggestions that infant feeding is a matter of choice do not account for women’s personal circumstances (Andrews, 2022) and the ‘diverse set of values and influences across their social networks’ (Marshall et al., 2007: 2158). We now turn to the UK context as it relates to younger mothers.
The UK Context: LMC, Breastfeeding and Young Mothers
In England and Wales, conception rates for under-18s are more than twice as high in areas of high deprivation (ONS, 2018). While recent statistics are difficult to come by, in 2010, 58% of UK mothers under the age of 20 initially breastfed following birth, compared with 87% of mothers over 30. By one week, 42% of under 20s were breastfeeding their babies and by six months this was 11% (McAndrew et al., 2012). This national picture masks geographical differences. Breastfeeding rates are much lower in areas of material deprivation; this represents ‘a major health and inequalities challenge’ (Renfrew and Hall, 2008: 1066).
Existing negative discourses around young mothering constrain young women’s abilities to see themselves as ‘good mothers’ (Duncan, 2007), with low-income mothers also demonised (Cooper, 2021). This reflects broader narratives and stigma regarding childbearing at ‘too early’ an age (Carson et al., 2017: 817) and the contrast between the slow and fast lane to adulthood/parenthood (Duncan, 2007). Whereas ‘planned parenthood’ is presumed to enable wage-earning capacity, young mothers are seen as a drain on the welfare state (McRobbie, 2007). Breheny and Stephens (2007) identified how health professionals drew upon ‘developmental’ discourses to position adolescent mothers as problematic and Duncan (2007: 327) suggests that terminology itself, for example ‘teenage mother’, is problematic, given associations with ‘a priori, unitary, fixed, coherent, inherent and essentialized set of attributes and characteristics’.
Prior research findings often fail to acknowledge social inequalities, such as poverty and food insecurity (Rothstein et al., 2020), that are key to understanding the wider context of younger mothers, their social embeddedness (Bissell et al., 2018) and infant feeding practices (Newhook et al., 2013). Younger mothers look to their peers for emotional support (Hunter and Magill-Cuerden, 2014), and are informed by family infant feeding histories, in particular maternal grandmothers (Emmott et al., 2020). It is therefore essential to obtain greater insights into the local context of their everyday lives including the additional challenges experienced by low-income mothers (Cooper, 2021).
We seek to recognise the way in which classed mothering norms are embedded within familial and peer localities, and how this informs women’s infant feeding attitudes, beliefs and behaviours. Behaving in a way that is understood as ‘morally acceptable’ involves individuals feeling they belong to a particular peer group and following those shared norms (May, 2008: 472), practical logics and associated practices (Beagan et al., 2016). We use the term LMC to reflect this collective situatedness and contribute to understandings of maternal foodwork, picking up on the idea of women’s differences rather than deficiencies (Cooper, 2021). We build on the limited research stream that engages with the relevance of women’s social environments to what Entwistle et al. (2010: 230) term a ‘bottle feeding culture’ and ask: what are the local infant feeding discourses that young women are exposed to? How do young women balance LMC and associated discourses with official infant feeding discourses? How do their infant feeding practices contribute to notions of good mothering and other aspects of identity work?
Method
The research took place in an area of north England with high levels of multiple deprivation (Gov.UK, 2015) and under-18 conceptions, and lower than national average rates of breastfeeding (PHE, 2018). NHS ethical approval was obtained to recruit participants through an antenatal service for younger women. Specialist midwives discussed the study with women (aged 17–19), pregnant with their first child; further information was provided to those interested in participating, followed by informed consent and guarantees of anonymity/confidentiality.
Thirteen women were interviewed twice: once in the later stages of pregnancy, given most infant feeding intentions are decided before birth (Murphy, 1999), and again within their child’s first year. The youngest baby was eight weeks at the time of the second interview and the oldest was 10 months. Our initial sample size was 17, but four women were interviewed just once, owing to their transient living conditions, reflecting challenges often encountered when recruiting marginalised women in maternity research (Kerrigan and Houghton, 2010). We may have inadvertently prioritised some young women’s voices above others; those who chose not to participate, or who participated only in the first interview, may have had very different stories to share (Carson et al., 2017), possibly informed by less engagement with the midwifery service and less stable living conditions.
Table 1 summarises participants’ age, relationship status, employment and living arrangements. Eight women were in education when they became pregnant, four were employed (e.g. catering, childcare) and one was unemployed. Most women left work/college on discovering their pregnancy and were receiving state benefits at the time of the first interview; however, Table 1 gives their last occupation/course of study. Many were living in temporary accommodation, and three to five participants were officially homeless at the time of the first interview. Women’s backgrounds (e.g. poverty, educational attainment, low paid work) are fairly typical of new mothers in this age group (Graham and McDermott, 2006) and reflect the local area’s high levels of material disadvantage. While young mothering is often assumed to be synonymous with lone mothering (Graham and McDermott, 2006), 10 women were in a relationship with the baby’s father (one was described as ‘on/off’), one was in a relationship with a man who was not the baby’s biological father and two women were single. The majority of our participants had partners, and this had a bearing on their decisions and experiences around infant feeding, as will be illustrated in the findings.
Participant information and infant feeding trajectories.
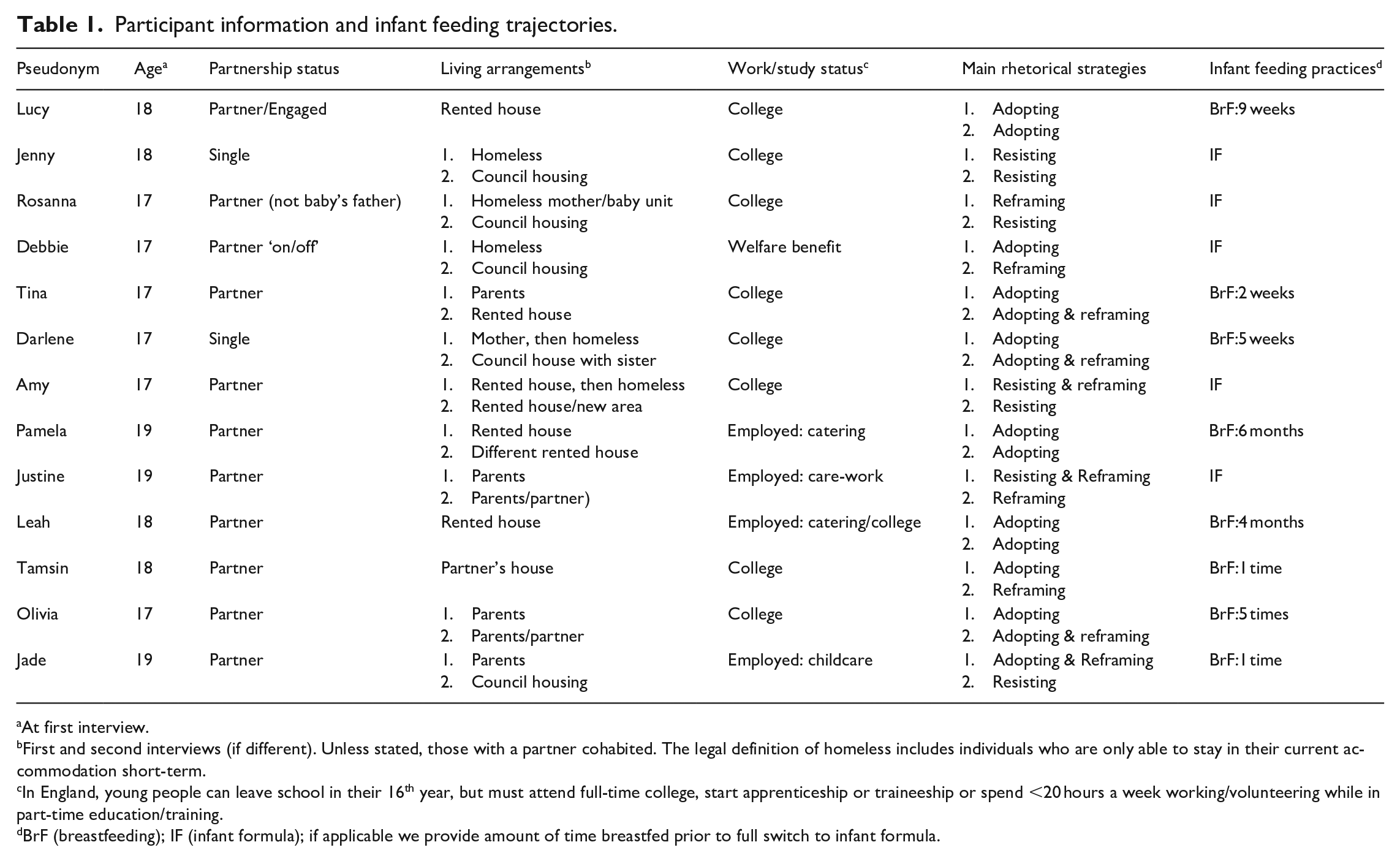
At first interview.
First and second interviews (if different). Unless stated, those with a partner cohabited. The legal definition of homeless includes individuals who are only able to stay in their current accommodation short-term.
In England, young people can leave school in their 16th year, but must attend full-time college, start apprenticeship or traineeship or spend <20 hours a week working/volunteering while in part-time education/training.
BrF (breastfeeding); IF (infant formula); if applicable we provide amount of time breastfed prior to full switch to infant formula.
The longitudinal design allowed women’s biographical details to emerge during the in-depth interviews (Bissell et al., 2018). First interviews focused on women’s experiences of pregnancy and intentions/expectations regarding motherhood. Follow-up interviews focused on experiences of motherhood thus far (including infant feeding) seeking to maintain a natural conversational and non-judgemental approach (Murphy, 2003).
The initial approach to data analysis shared similarities with grounded theory (Glaser and Strauss, 1967). Themes were coded and compared, with detailed notes and memos exchanged between researchers. We focused on individual participants, then worked across the sample to identify emergent themes, moving back and forth between the data and literature to refine understanding and further develop analytic categories. The responses reflected general notions of accommodation and resistance, but as our analysis progressed, we developed more nuanced understandings, resulting in the three strategies that provided narrative accounts of maternal foodwork. We then re-reviewed these analytic categories, revisited the data and wrote an agreed overall interpretation of the data.
Findings: Maternal Foodwork and Young Women’s Social Embeddedness
Our findings illustrate how local contexts and activities structure daily lives and maternal foodwork (Hausman, 2008). While some women had challenging family relationships and only five were living with their parent(s) at the time of the first interview, discussions illustrated how babies’ maternal grandmothers, wider family members and friendships informed LMC norms and expectations, and ultimately infant feeding practices. Women drew on characteristics of their LMC to respond to the dominant discourse that associates breastfeeding with good mothering.
This social connectedness is highlighted here by Pamela, both in terms of her understanding of the influence of maternal grandmothers on infant feeding practices as well as wider expectations of young women’s social needs:
Not a lot of people that I know, their mums have[n’t] breastfed. So they copy what their mum’s done. I think it’s a lot of influence from it . . . I think they say ‘Oh just stick them on the bottle, it’s easier, someone else can get up with them and you can go out and you can have your time.’ (Interview2)
The advice Pamela refers to ‘have your time’ illustrates potentially contradictory challenges faced by young mothers as they negotiate their new responsibilities while also ‘doing youth’ (Sniekers and Rommes, 2020). In order to explore further how women navigate infant feeding practices, within the wider context of infant care, social networks and family making, we next discuss women’s use of rhetorical strategies within the maternal context.
Infant Feeding and Rhetorical Strategies
Rhetorical strategies shed light on young women’s lived realities and inform how ‘mothers defend themselves against the charges of maternal irresponsibility that arise when their practices do not conform to expert medical recommendations’ (Murphy, 2003: 433). We see links to women’s LMC, and examples of how they sought to exercise agency, particularly by challenging and reversing the discourses around ‘breast is best’. We conceptualise three rhetorical strategies that capture how explanations interact with official infant feeding discourses. 1 These rhetorical strategies link with what Bissell et al. (2018) term ‘assumed shared food narratives’, the socially informed narratives that women draw on to protect their identity in the light of public health messages around food consumption.
First, adopting describes an engagement with, and acceptance of, official (in this case pro-breastfeeding) discourses (resulting in breastfeeding practices). Second, resisting reflects a lack of interest in, or resistance to, these discourses (resulting in the rejection of breastfeeding practices). The third strategy was reframing. Reframing indicates an awareness of, and partial attendance to, those official food discourses that encourage women to breastfeed. However, reframing allows women to maintain adherence to LMC-relevant mothering ideals through incorporating competing considerations, and results in the rejection of a longer-term commitment to breastfeeding practices.
Adopting the Discourse
Discourses regarding the pronounced health benefits of breastmilk in the early weeks were picked up by participants, with many women initially expressing an interest in breastfeeding for the first few weeks (Table 1 shows women’s strategies at interviews 1 and 2, and the length of time women breastfed, if applicable). Beyond this, women like Leah identified wider benefits, including its bonding role:
I know it is better for your baby and there’s that bonding thing as well, isn’t there? Between you and your baby, being able to do that. And it’s a lot more convenient you know, not having to sterilise and make sure everything’s really clean and things. (Interview1)
Leah emphasises convenience, and other mothers referred to breast milk as ‘free milk’. It was clear this small group of breastfeeding young mothers defied others’ expectations that they would not breastfeed (e.g. their family, wider social networks). Pamela, whose mother also breastfed, notes how she believes her young age informs the reaction of others: ‘at the doctor’s I can go and breastfeed and the older woman, she’s smiling and happy to see a young person breastfeeding’ (Interview2). While her association with breastfeeding norms could potentially distance her from her peer group (Brenton, 2017), it could also inform other young mothers’ infant feeding attitudes: ‘When they see me breastfeeding in the clinic, they go “Oh I wish I’d have breastfed” because they’re seeing someone young doing it’ (Interview2). Pamela’s narrative (e.g. ‘I love it, I love the bond that we have and I love him looking up at me and stuff like that’) suggests self-mastery (Entwistle et al., 2010), which contributes to her confidence in surmounting commonly experienced social barriers, for example public feeding to which we now turn.
Breastfeeding in public has been identified as particularly socially challenging for young mothers (Dyson et al., 2010; Hunter and Magill-Cuerden, 2014). Participants who breastfed noted their avoidance of the public gaze: ‘I tended to go upstairs or put a blanket over her’ (Darlene: Interview2); ‘I wouldn’t ever do it in public’ (Leah: Interview1). LMC attitudes to public breastfeeding operate in direct contrast to Andrews (2022) where it is the presence of a bottle, rather than the breast, early on which evokes Mary Douglas’ ‘matter out of place’. For Lucy the thought of public feeding informed her decision to switch to formula milk: ‘I didn’t plan on finishing breastfeeding . . . I had a wedding to go to and I didn’t want to breastfeed in front of everybody’ (Interview2). These excerpts illustrate an alternative moral framework to that which operates in other maternal contexts (e.g. Andrews, 2022; Murphy, 1999), with different norms and considerations evident (Jamie et al., 2020). However, expectations of young mothers were confronted head on by Pamela: ‘I breastfeed in KFC, McDonald’s, the middle of town, on a train, just doesn’t bother me’ (Interview2). Her reference to breastfeeding in the public spaces she frequents indicates a refusal to let her feelings or others’ reactions dictate her infant feeding practices and interrupt her everyday life as a young woman.
The experiences of young women like Pamela and Leah who adopt the official discourse and publicly display their infant feeding practices highlight issues with treating young mothers as a homogeneous group, whereby identical outcomes are often assumed on the basis of age alone (Wilson and Huntington, 2005). Infant feeding practices allow women a political site from which to (re)negotiate their positions as teenage mothers. Rather than accept the negative connotations often associated with teenage mothering (Tyler, 2008), young women can present themselves as capable and knowledgeable using foodwork to help distinguish themselves from particular class locations (Beagan et al., 2015).
Resisting the Discourse
There were very few women who did not engage with breastfeeding discourses at all (Table 1) with participants generally knowledgeable regarding the purported health benefits, particularly in the early weeks. However, it was clear that many young women’s LMC do not encourage breastfeeding, and this informed their reluctance to behave in line with wider motherhood ideals (Murphy, 1999). The infant feeding norms for many of these women were focused on the use of formula milk, with the breast, rather than the bottle, positioned as a break from the norm, or even taboo (Andrews, 2022).
Amy was fairly typical, describing her family’s infant feeding experiences as follows:
My mum never breastfed, my grandma never breastfed, no-one in my family ever has. And then one of my sisters did try it at the hospital and she said it was a bad experience and she would never do it again in her life . . . that’s what put me off. (Interview1)
Amy illustrates her embeddedness in her family social network (Bissell et al., 2018), characterised by the strong influence of her mother’s and grandmother’s feeding practices, suggesting these negatively impact her self-confidence and openness to breastfeeding. In her first interview, Rosanna articulates an intention to breastfeed for the first few days; initial engagement that switches to disengagement or avoidance post-birth:
I just went straight on to bottles because I couldn’t be bothered breastfeeding, I just felt so exhausted . . . Whereas with breastfeeding, I’d have to hold her up and I didn’t have the energy to even hold her really. She used to lie on the bed with her head slightly propped up and I used to hold the bottle to her. (Interview2)
Both narratives contain passive elements both in terms of the language adopted (e.g. Rosanna: ‘couldn’t be bothered’) and the way in which Amy presents her decision as almost inevitable. Amy’s familiarity with the infant feeding practices of her wider family and suggestion she will adopt practices in line with their experiences was common across the study. Rosanna’s narrative included considerations for maternal well-being in contrast to Murphy’s (1999) observation that it was rare for women among her (more heterogeneous in age/class) sample to acknowledge prioritising their own needs and preferences when using formula milk, considerations that run counter to intensive feeding ideology (Brenton, 2017). And there were also indications that low levels of self-confidence could inform the resistance to breastfeeding discourses. Jenny was clear that she did not intend to breastfeed: ‘I just always said from the beginning that I wasn’t going to breastfeed’ (Interview1). In her second interview she remarked: ‘I reckon it’d have knocked my confidence if he didn’t take it’ (Interview2) suggesting low self-efficacy (Entwistle et al., 2010) informed her rhetorical stance. Further elaborations demonstrate the important role assumed shared food narratives (Bissell et al., 2018) played in her confidence levels. Her stance is pre-emptive and draws on a local (family) evidence base:
I think it was just like because my mum, when she had me and my sisters, she tried breastfeeding and none of us took to it. My nephew didn’t take to breastfeeding either and neither did my niece . . . I didn’t want to try it and him not take to it. So I thought best just going straight to bottle instead of having to try breastfeeding and if he doesn’t take to it, then you know. (Jenny: Interview2)
In prioritising babies’ health, official discourses may fail to account for (young) women’s feelings, experiences and LMC. There is a combination of both active and more passive elements at work. Jenny demonstrates conviction in her infant feeding intentions and practices, yet her acknowledgement of the potential confidence knock means her resistance also comes across as having passive elements, pointing to the potential for breastfeeding to be experienced as a psychological hurdle (Entwistle et al., 2010).
While Jade initially discussed an intention to ‘try’ breastfeeding (adoption), like many participants this intention was a short-term rather than longer-term commitment: ‘I wouldn’t be doing it for long anyway’ (Interview1). On the day of her child’s birth, she initially took her infant to her breast (adoption), but her approach switched, based on what would appear to be feelings of visceral disgust associated with breastfeeding:
I don’t know, I just . . . I can’t explain it, it’s just like it didn’t . . . it wasn’t something for me to do. Whereas people . . . like my sister-in-law, she’s just stopped breastfeeding . . . I just couldn’t get my boob out for her to suck on it, if you know what I mean. It just wasn’t a thing for me to do. I can’t really explain it, it just wasn’t me, it just made me feel a bit sick in a way. (Jade: Interview2)
Familial elements (sister-in-law) supported Jade’s intention to breastfeed, yet her wider LMC may inform her practices in ways she finds difficult to articulate. Jade foregrounds personal thoughts, feelings and preferences appearing to grapple with tensions between what is positioned as right via official discourses (e.g. healthy) and her LMC-informed perceptions of what is normal (Murphy, 1999), further highlighting the extent to which local communities and families inform women’s beliefs.
Jade aligns herself with the norms and practices of her peers (Beagan et al., 2015) that inform a sense of ‘matter out of place’ (Andrews, 2022: 67). These beliefs shaped participants’ frequent positioning of breasts as ‘something you keep covered up’ and formula milk as ‘normal milk’, baby’s ‘own milk’ or even simply ‘milk’; understandings and terminology that counter wider notions of naturalness, and further reveal assumed shared food narratives (Bissell et al., 2018), which in Jade’s case seemingly inform feelings of disgust. Women thus employed similar strategies to the ‘rhetoric of naturalness’ referred to by Murphy (1999/: 195) whereby natural and normal are informed by perceptions within LMC rather than connections with ‘mother nature’ and elements of the maternal breastfeeding discourse.
Reframing the Discourse
The majority of our informants (Table 1) engaged in an agentic strategy that we term reframing. Those who reframe official discourses may end up adopting the same infant feeding practices as women who resist (e.g. bottle feeding), yet they operate with acknowledgement of official recommendations, and the strategy allows scope for individual judgement, taking into consideration other practices and competing demands of being a young mother/person. These women therefore engage with a form of moral repair work (Andrews, 2022) incorporating LMC-informed understandings. As in Murphy (2003), they did not reject expert knowledge (as was sometimes the case with resistance), instead they demonstrated agency by reversing the discourse, picking up on elements that were then used to develop alternative counter discourses. This allowed space to develop/display ‘a different kind of expertise’ (Armstrong and Murphy, 2011: 321). Reframing generally resulted in the decision to breastfeed for shorter periods of time or to use formula milk. It implies a more active process of everyday resistance whereby existing power relations are challenged (Croghan and Miell, 1998) in such a way that accommodates a range of perspectives and considerations.
A key element to reframing is the development of alternative discourses where different elements of child-centred baby rearing are emphasised and acted upon. Attachment and bonding between mother and baby, an important element of the breastfeeding discourse (Jansen et al., 2008), was often broadened to apply to fathers, as Amy and then Olivia highlight:
If we do bottle-feed, he gets to take part as well, he gets to feed it as well. Whereas if I breastfeed, he doesn’t get to take part in that. (Amy: Interview1) He says he wants the best thing for the baby but obviously he won’t be able to have a connection with feeding the baby if I’m breastfeeding. So I’ve said I’ll express for him, so he can do it too. (Olivia: Interview1)
Amy and Olivia engage in reframing to different extents. Amy reframes the discourse to prioritise the bonding element and the opportunity for her partner to participate in feeding, resulting in an intention to feed formula milk. Olivia depicts a more selective reframing; she engages sufficiently with the discourse to prioritise breastmilk but is very keen for her partner to benefit from the bonding elements. In her second interview she reports that although she tried expressing milk it was too painful, so after five days of breastfeeding and attempting to express, she switched to formula milk. The above extracts suggest a reluctance by couples to accept a more secondary fathering role as provider of support for breastfeeding mothers. Fathers’ involvement was positioned positively, akin to the ‘pleasure’ of formula use highlighted by some of the women in Lee’s (2007) study. This illustrates the responsibility these women took, not just for infant feeding decisions but also for the production and facilitation of wider family life and relationships.
A second recurrent theme related to the importance attached to early breastfeeding, and specifically the associated infant health benefits (Burns et al., 2012). Jade partially accepts a role as nutritional provider yet reframes her understanding to stress only the importance of early breastfeeding, at the expense of current advice to breastfeed exclusively for six months:
I wouldn’t be doing it for long anyway, I’d only probably be doing it for about two weeks, maybe not even that, maybe just a week, just to get maybe the nutrients that are in me over to my baby, that’s if she latches on properly. And then probably she’ll go onto a bottle, but I’ll be mixing in between anyway . . . they say you need to like breastfeed up until six months. Well, you don’t need to do it; yeah, it’s the best way that they’ve found out, but I think a week or two weeks is long enough for my nutrients to go into their body. (Interview1)
Jade reframes the discourse to emphasise one element (initial versus longer-term breastfeeding) and demonstrates agency through actively resisting official discourses with her comment ‘you don’t need to do it’. She positions herself as knowledgeable, in contrast to stereotypes surrounding young mothers, thereby rejecting imposed categories. She draws on language (nutrients) used by professionals to clarify her views on the required length of time to realise the health benefits, and challenges fundamental assumptions regarding breast milk’s superiority. Jade also incorporates a caveat, her eventual decision depends on her baby’s ‘performance’ and ability to latch on, suggesting some elements are out of women’s control.
Third, as already discussed, many participants highlighted the issue of feeding in public, established as a key concern among younger mothers (Dyson et al., 2010). Leah’s experience demonstrates fluidity in the strategies. She breastfed for four months, and describes it as ‘a natural thing and you have to feed your baby’ (Leah: Interview1), she also reframes this imperative to prioritise the feelings of others (audience) when feeding in public:
I wouldn’t feel comfortable doing it. Because I know it’s not nice to say but I do myself feel uncomfortable when people breastfeed their babies in front of me. I don’t know where to look. And I wouldn’t like to put other people in that position. (Leah: Interview1)
What is considered natural is socially defined (Wall, 2001), and here is pitted against what is appropriate, reflecting the moral norms identified in Dyson et al. (2010) and the anxieties associated with a sense of matter out of place (Andrews, 2022) where in this context breastfeeding is understood as a ‘problematic transgression of bodily behaviours’ (Jamie et al., 2020: 1696). This is further emphasised when Leah describes another woman breastfeeding in public as ‘kind of exposing herself and it’s not normal for people to do that’ (Interview1). This provides an example of selective reframing; while Leah herself practised breastfeeding, her discussion around privacy demonstrates the reversal of an element of the discourse (e.g. that public breastfeeding is normal) to better suit her own LMC situatedness.
Participants using the reframing strategy demonstrated knowledge and engagement down to the vocabulary and categories of the dominant discourse (Foucault, 1978). Reframing is not simply a middle ground between accommodation and resistance, it shares elements with the ‘recalibration’ in Cairns et al. (2018) where women are constantly negotiating their food identities and practices. These young mothers exercise agency through exploiting inconsistencies and tensions both within and between discourses, in order to transform their meaning. This allows women to promote alternative identity positions (e.g. knowledgeable, considerate); by taking into consideration their LMC, they resist the imposed stigmatised category of ‘teenage mum’ (Tyler, 2008).
Discussion
This article adds to a growing body of sociological work that seeks to understand how the ‘diverse and situated everyday experience of mothering’ (Thomson et al., 2011: 8) works alongside responsibilisation, within the context of maternal foodwork. The young women in this study refuse the wider moral positioning that associates (only) breastfeeding with motherhood ideals (Jamie et al., 2020), instead embracing an approach recognising alternative pathways to good motherhood (Carroll and Yeadon-Lee, 2022). Young women’s classed positions shape foodwork in line with the ‘finer, complex ways’ acknowledged by Karademir-Hazır (2021: 1210), incorporating LMC-informed scrutiny and concerns (Bissell et al., 2018). In one sense those women who fed their infants formula milk challenge middle-class ideals regarding the best way to feed babies. Yet most participants were careful not to position themselves against other mothers whose infant feeding practices differed from their own. Like the women of colour in Brenton (2017), they instead demonstrate how their practices go beyond health narratives to encompass (local) knowledge and experience, related to their classed identity positions. Our findings therefore answer calls ‘to locate mothers’ ideas about food and their experiences feeding children within a web of broader social problems’ (Brenton, 2017: 876).
We analyse our participants’ approach to infant feeding with regards to three rhetorical strategies. Adopting and resisting refer to young mothers’ acceptance or rejection of prominent infant feeding discourses. While participants’ use of these two strategies can reveal much about the intersection of youth, poverty and motherhood (Cooper, 2021; Sniekers and Rommes, 2020), it is reframing that best illustrates young women’s active negotiation of infant feeding alongside other LMC-informed concerns. Under reframing, women transform the encouragement to breastfeed, dismantling or reversing official discourses. Reframing therefore facilitates the ‘ongoing negotiation of food identities and practices’ (Cairns et al., 2018: 177). Some women subvert the very nature of maternal foodwork, in order that wider issues such as paternal involvement take centre-stage, emphasising the differences rather than deficiencies in their approach (Cooper, 2021). The focus on women’s rhetorical strategies allows us to engage with what can be complex and heterogeneous experiences, considering women’s socio-cultural locations and the accompanying logic to their social practices (Beagan et al., 2016) rather than only their resulting infant feeding practices. In so doing, an altogether more nuanced picture emerges and women reject the good/bad motherhood binary, instead demonstrating a concern for informed, responsible motherhood (Carroll and Yeadon-Lee, 2022). Such an approach allows more flexibility to claim an identity as a good mother (Cairns et al., 2013; Wright et al., 2015) and illustrates how women’s moral selves relate to their socio-cultural contexts and norms around motherhood (Beagan et al., 2016; May, 2008).
Conclusion
We now turn to the key contributions of our study. First, we contribute to understandings of how LMC inform women’s response to official recommendations and discourses, equipping them with the knowledge and skills to integrate or counter discourses. Second, we contribute to understandings of how women exercise agency in order to challenge and reverse discourses that associate maternal practices, in this case breastfeeding, with good mothering. We demonstrate how young women change the terms of the debate around infant feeding, infant and self-care practices, and family relationships, widening the context within which maternal foodwork is considered.
Our findings suggest that while all mothers operate within an overall system of power dynamics, these are complex. The outcomes of the three adopted strategies may be understood by others (e.g. health professionals, other parents) simply as the ‘choice’ of breast or formula milk, yet these outcomes relate to a complexity of official and local knowledge, combined with embodied infant feeding experiences and other infant care practices. We therefore concur with studies (e.g. Andrews, 2022; Braimoh and Davies, 2014) that critique understandings of women’s infant feeding decisions as straightforward choices. Such an approach does not fully recognise LMC-informed constraints; in this sense choice reflects elements of class privilege (Hausman, 2008). While women were familiar with public health recommendations to breastfeed, these were seen to restrict other elements of family making (e.g. mothers’ health, paternal bonding). Discourses were therefore re-shaped and re-incorporated into wider concerns and family life responsibilities (Head, 2017). While women’s infant feeding practices were carefully considered, they were not highly accountable within the same moral context as has been experienced elsewhere (e.g. Andrews, 2022; Murphy, 1999); instead, their LMC highlighted moral issues around public feeding and opportunities for paternal bonding. Women’s approaches ran counter to prevalent understandings of class-based approaches to foodwork, which suggest a middle-class emphasis on health and a working-class emphasis on practicality (Karademir-Hazir, 2021). While there were elements of these young women’s foodwork that prioritised a more pragmatic approach, this was intertwined with wider considerations. Women also invariably selected the more financially and time-costly option, again lending further complexity to intensive foodwork (Beagan et al., 2015).
Our findings shed light on the performance of identity work within existing power relations. Some of the young women demonstrate agency through adopting practices that might indicate ‘stepping outside’ the boundaries of their LMC (Wills et al., 2011), but in general this agency involved developing more malleable understandings of official recommendations, reframing discourses to support the development of positive (maternal) identities. The use of rhetorical strategies, and accompanying practices, allows individuals to develop their own culturally acceptable paths to positive mothering identities, using ‘talk to establish their moral credentials’ (Murphy, 1999: 191). On the one hand, in accepting the value of official discourses, the women seemingly do little to disrupt power relations. However, reframing official recommendations allows space for contestation and malleability. We therefore support Foucault’s (1977: 100) observation that understandings of discourses should appreciate the ‘multiplicity of discursive elements that can come into play in various strategies’. We also build on work in the tradition of Duncan (2007) who understands young women’s approach to motherhood as much more considered than popular opinion and many prior studies suggest. Exploring what individuals do with discourses allows deeper exploration of the challenges faced by situated populations and the potential complexities and identity intersections that exist.
Footnotes
Acknowledgements
We would like to thank the women who participated in the study and the teenage midwifery service who helped with recruitment.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.