
Abstract
While regularly applied to globalized migration, conceptualizations of hospitality have rarely been used to understand healthcare settings. Drawing on interviews with healthcare staff in Sweden, our article contributes to the current conceptualization of hospitality accounting for: the internal contradictions of hospitality that racialized staff experience in their everyday interactions with patients and other staff; the shifting boundaries between host and guest in everyday healthcare practices, especially when examined through the lens of racialization and finally; the subtle though troubled coexistence of hostility and un(conditional) hospitality that weakens resistance against racism. The analysis maps the complex contingencies of professional, ethnic and national relations between staff and patients, in light of their racialized and gendered nature, to suggest that the ambivalences theorized as part of the concept of hospitality show how the hurts of racism are so hard to pinpoint.
Introduction
The idea of hospitality has been important in discussing the politics and ethics of migration and the transnational movement of people across borders. In particular, the rights and obligations of migrants from the Global South with respect to hosts in the Global North have been examined with urgency as the dramatic increase in arrivals into Europe via the Mediterranean Sea crossing and the Balkan route from 2015 onwards. The International Organization for Migration estimates hundreds of thousands of people arrive in Europe every year and, the uncertainties of COVID-19 notwithstanding, 151,417 people arrived in 2021. 1
Statutory and inter-agency responsibilities were contested as gestures of welcome played out against a wave of post-colonial xenophobia enacted in the closing of borders and curtailing of support for forced migrants (Townsend, 2015). The United Nations called on industrialized countries to offer hospitality to forced migrants through a fixed quota system, with the international politics of hospitality playing out through the exercise of power and resistance (Bulley, 2017). Thus, mobility across borders is deeply embroiled with embodied and enacted practices of hospitality and hostility. ‘Refugees are welcome’ movements notwithstanding, forced migrants are portrayed as representing a fiscal burden in consuming more from the public purse than they contribute, thereby diluting the benefits enjoyed by long-standing citizens of host societies (Gal, 2018; Milanović, 2016). The unfounded presumption that new arrivals illegitimately and recklessly consume healthcare (Ahlberg et al., 2019; Bradby et al., 2020a) ignores the contribution of migrant labour to providing welfare (Bradby, 2016): from the best paid physicians, to the poorest paid cleaners, European healthcare depends on migrants. The ambiguities of the immigrant as un/wanted guest do not end when that migrant is awarded residence papers since, as a racialized minority, former migrants must navigate the hostile welcome long after initial arrival.
In this article, we analyse the complex and ambiguous experience of racialized healthcare staff in Sweden, a country exemplary in its practices of reception and welcoming forced migrants. By racialized staff we refer to people who have migrant forebears or who are themselves migrants and who are identified as not of Northern European descent as a result of appearance – bodily features and style of dress. We draw on the theoretical ideas of hospitality to make sense of the ambivalent experiences of conditional welcome and hostility described by racialized staff in Swedish healthcare. Our article draws on interviews with healthcare staff of various professional and ethnic groups to show that racialized healthcare staff, both highly skilled and low skilled, are made to feel unwelcome in their own work place, which might otherwise be a familiar space for them as staff.
Hospitality is a well-worked theoretical concept that we review as background to how racialized Swedish healthcare staff themselves use it to make sense of their encounters with other staff and patients. Contemporary healthcare settings have not been much explored as sites of hospitality, although the Latin root hospitales underpins ‘host’ and ‘hospital’. The 20th-century establishment of healthcare systems as part of European welfare state provision, funded by income tax or social insurance, has meant that accessible healthcare has been transformed into a citizen’s right to statutory resources or a human right (Bradby et al., 2020b), rather than a gift that constitutes a form of hospitality. Since the global financial crisis of 2008, austerity programmes have reduced healthcare access for certain groups, since human rights, like citizens’ rights, are always enacted in a more or less generous socio-economic and legal framework. Neoliberal reforms to reduce the costs of healthcare provision in the Global North, regularly adopt commercial profit-making service provision that has been one driver of migration of skilled and unskilled medical labour from the Global South (Bradby, 2014, 2016). The exploitation of migratory labour forces, whether they arrive as refugees or so-called ‘economic migrants’, is a key context for understanding the experience of racism.
Hospitality is not a metaphor through which contemporary statutory healthcare provision has been much analysed sociologically, although the commercial provision of catering, cleaning and bed-making in the healthcare sector is apparent (DeMicco and La Forgia, 2020). In this analysis, we focus on migrants to Sweden, employed in healthcare provision, where they experience, witness and enact everyday practices of hospitality with other staff and patients. Furthermore, as much as acts of hospitality establish and consolidate links between, subjects, kin and groups, our article also troubles the idea of hospitality by looking at its close links with hostility (Berg and Fiddian-Qasmiyeh, 2018). Hospitality and hostility ‘have in common the fact that both are expressions of the existence, rather than the negation, of a relationship’ (Selwyn, 2013: 20). How can the quotidian complexities of enacting, resisting and making sense of hospitality and hostility support an understanding of the ambivalences of racism?
After reviewing the meaning and practices of hospitality as an everyday and a theoretical, philosophical concept in the context of racism, which might be examined empirically, we describe the methods through which we interviewed Swedish health and dental care staff. We then offer an interpretation of interview material in which metaphors of hospitality and hostility were used to explain experiences of racism.
Hospitality
Marcel Mauss’s interest in systems of exchange in societies that did not use money, showed how symbolic gift exchange was a reciprocal and binding system. In ‘Essai sur le don’ (1923–1924), Mauss demonstrated that the gift is never free and independent of its giver, but rather carries obligations and responsibilities that constitute social networks. Elaborating this further in the context of ritual gift exchange, Bourdieu argues that giving is also a way of possessing – if a gift is not met by a counter gift of comparable quality ‘it creates a lasting bond and obliges the debtor’ to adopt a peaceful and obsequious attitude (Thompson, 1984: 56). So, relations of domination are not created by the mechanics of the state or the self-regulating market, but by the cultivation of personal bonds of obligation. Domination can be maintained if participants fail to recognize the act of domination and perceive these bonds ‘as disinterested and legitimate, even though they support relations that are quite literally suffused with power’ (Bourdieu, 1977; Topper, 2001: 36). Hospitality can be understood as constitutive of social relations and implying obligations and rights, shaped by specific contexts. For hospitality to be hospitable and demonstrate the capability to welcome the other, it needs to be offered unconditionally (otherwise it fades into commerce) and extended to anybody and everybody – an openness to receive whoever comes. As Derrida suggests, ‘hospitality itself, opens or is in advance open to someone who is neither expected nor invited, to whomever arrives as an absolutely foreign visitor, as a new arrival, non-identifiable and unforeseeable, in short wholly other’ (Borradori, 2003: 129, emphases in original).
Derrida refers to the ‘hospitality of visitation rather than invitation’ (Borradori, 2003: 129, emphases in original). Hospitality is never the simple and isolated offering of space, services and goods from one person, household or community to another, but rather is part of a wider system of exchange that constitutes social and cultural structures, with accompanying political and economic aspects. Practising hospitality implies being master of the space, services and goods that are offered (Derrida and Dufourmantelle, 2000) – the right and power of the host prevails over the guest, thereby implying a form of dominance, which foreshadows the possibility of hostility.
While the unconditional offer of hospitality implies the host’s dominance, a certain power also lies with the guest as stranger (hospitality tends to be envisioned between men, albeit supported by women’s labour [Still, 2010: 36], who has the potential to abuse the unconditionality of the invitation. Any moment of hospitality contains within it conflict such that an act of hospitality also holds the prospect of hostility. The tension between self-interest and altruism in hospitality is captured by Derrida’s hybrid term ‘hostipitality’, underlining the unstable mixture of enmity and generosity (Still, 2010: 18).
Derrida saw hospitality as foundational, being constitutive of culture (Derrida and Anidjar, 2002: 361), of ethics, of language, of humanity itself (Still, 2010: 5). Hospitality’s ambivalence requires engagement at an ‘unstable site of strategy and decision’ (Derrida, 2005: 6) with its inherent contradictions rendering it a self-contradictory concept that can only self-destruct (Derrida, 2000: 5). Derrida (2000: 15) drew a distinction between the other and the stranger, where hospitality is accorded to the stranger (who is ‘non-autochthonous, non-indigenous’), ‘the impossible must be done’ (Derrida, 2000: 14). These nice distinctions, along with their associated ambiguities, are part of a discussion of how to reconfigure host, guest, citizen and foreigner (Still, 2010: 79) to challenge the prevailing western dichotomous logic, which identifies friends from enemies and us from them (Kelly, 2012: 61).
Hospitality and the Immigrant
Hospitality as a generous welcome to the stranger, without expectation of recompense, to honour and humanize the guest through mutual recognition (Jelloun, 1999: 49), has been advocated as an ethos for contemporary European migration governance, by refugee-supporting social movements and the United Nations. Liberal discourses of inclusion suggest that immigrants are strangers and uninvited guests who should be shown generous and selfless hospitality. The metaphor of home-based hospitality is used to reject migrants, when ‘illegal immigration’ is compared with ‘breaking and entering a legitimate home-owner, who consequently has the right to eject the incomer’ (Calvo, 2013: 108). The rules of hospitality thus justify increased border control, displacing global responsibility for forced migrants (Kelly, 2006), creating binaries between the ‘deserving’ and the ‘undeserving’, to deter refuge-seeking (Gibson, 2007).
Whether an immigrant qualifies as a guest deserving of a hospitable welcome or as an illegitimate other whose incursions should be resisted depends on immigrants’ status as unknown strangers. Long-standing links between Europe and the countries from which most migrants currently originate – Iran, Iraq, Afghanistan, Somalia, Eritrea – mean that the immigrant is never a stranger. Post-colonial migration to Europe cannot involve strangers since with ‘Europe’s constitutive history of empire, colonial conquest and transatlantic slavery’ (Danewid, 2017: 1675), the assumption of immigrants as new arrivals is unwarranted, since the links were long ago made.
The network of relations that bind countries of emigration with countries of immigration are infused with the imbalances of colonial power. The sending countries are indebted to the European nations to which migrants head, both in terms of the International Monetary Fund’s calculations, and in the hierarchy of status around culture and authority. Long-standing socio-economic relationships between the receivers and senders of migrants, constituted in trade, colonialism and violent suppression underpin ongoing inequalities and the absent presence of race within those relations (M’charek et al., 2014). These historical structures mean that immigrants to the Global North may be treated as guests, but they are not strangers so much as acquaintances who have already been exploited in a previous encounter.
In post-colonial migration, arrivals from former colonies may have been explicitly invited as a work force, as was the case for Caribbean nurses and Indian subcontinent doctors arriving in the UK in the mid-20th century, but this does not make them stranger-guests. Hospitality as a gift given to a stranger implies a temporary sharing of goods and space and this temporality is critical: a permanent guest is a contradiction in terms (Still, 2010: 14). When immigrants seek to become permanent residents or citizens, their status as ‘guests’ may be inhospitably emphasized (Still, 2010: 37). Furthermore, the ‘precarious status of guest (where that is how an immigrant is perceived) can last, if only in vestigial form, even after citizenship is granted, and indeed can be a perverse inheritance passed on through the generations’ (Still, 2010: 188).
While the laws of hospitality imply both rights and duties, immigrants, whatever their formal status, may be treated as guests without rights, but with duties to work hard, to be polite (Jelloun, 1999), to be unobtrusive to the point of invisibility (Tyler, 2003). Kelly (2006: 460) points out that on their part, guests must be ‘assimilable’ and respectful of ‘the rules of the house’; they should use the ‘front door’ and be invited to enter. Thus, hospitality demands the setting of some limits beyond which the other cannot trespass as the risk of transgression by the guest can turn a hospitable host into an inhospitable one – the twin processes of selection (welcoming some migrants over others) and discipline (conformity to the rules of the house) working together. Using hospitality to think with offers some purchase on the slippery nature (M’charek et al., 2014) of racialized discrimination and its articulation with other dimensions of contested identities (Essed and Trienekens, 2008).
Healthcare and Hospitality
Placing these debates within healthcare opens up a range of issues in relation to how biomedical practices are perceived and shape medical dispositions. Clinical spaces tend to be organized around professional priorities, and can be alienating and unwelcoming for the un-initiated (Underwood, 2016). The lack of hospitality, in terms of welcoming strangers into clinical space, may be justified in terms of clinical priorities such as infection control and the protection of vulnerable patients. The association of medicine with the natural sciences means that clinical practice contributes to the reproduction of race as an absent presence (M’charek et al., 2014) and understanding hospitals as formerly exclusively White institutions contributes to making sense of the emotional labour (Ahlberg et al., 2022) that disproportionately burdens people of colour (Evans and Moore, 2015); emotional labour that is both gendered and racialized (Cottingham et al., 2018; Essed and Trienekens, 2008; Van Riemsdijk, 2010).
In terms of the dyads of hospitality, staff should be at home in healthcare settings in the sense of being regular inhabitants, familiar with the organizational logic, such that any expectation of performing hospitality would fall to professionals rather than patients. Research into the adoption of a novel piece of information technology explicitly conceptualized surgeons as host and the information system as guest, to analyse the process as involving an ambivalent mixture of hospitality and hostility: ‘the mutual and co-constitutive relationship between the users and the technology and the continued co-existence of both positive and negative attitudes among the users’ (Jensen and Aanestad, 2007: 672). Surgeons are highly placed in the medical hierarchy such that their acceptance or otherwise of innovative practice and technology influences other cadres of staff. While hierarchies make a difference to how much time staff spend with patients, healthcare staff could be seen as hosting patients in the settings that the staff occupy on a daily basis, not least because the physical location and comfort of the patient is under explicit medical supervision.
Interviews with healthcare staff are examined to explore whether hospitality can explain the ambivalence around contested gendered and racialized national and professional identities in health and dental care work places. The interviews were part of a wider project with racialized minority and majority staff to examine their experience of racism in health and dental care.
Methods
As part of a larger project looking at racism in Swedish healthcare, we interviewed 58 healthcare staff between 2018 and 2020 from various professional and ethnic backgrounds with the aim of interrogating their views as a way to address institutional and individual racism in healthcare. We interviewed physicians, nurses, auxiliary nurses, midwives, dentistry staff as well as other healthcare staff involved in the organization of healthcare such as public healthcare professionals. Ethical approval for the study was granted by the Uppsala Regional Ethics Board (Dnr 2018/201). Both verbal and written informed consent to participate in the study were taken.
We employed individual, paired semi-structured interviews and focus group discussions in our study resulting in 35 interviews with 58 healthcare staff. All interviews were audio recorded except for where notes were taken as per the request of the informants. The interviews lasted between 23 minutes and 110 minutes, averaging around 80 minutes. All recorded interviews were transcribed, stored and coded in AtlasTi 8. Most interviews were conducted in Swedish, but Arabic and English were also used, sometimes in a single interview. All interviews were anonymized and pseudonyms are used in this article to refer to the informants.
Analysis involved a first step of deductive coding where the authors, after reading the interviews carefully, came up with a set of codes to index the interviews. These codes were initially tested in a couple of interviews and revised until a final set of codes were developed. The interviews were then analysed for the purpose of this article to examine how the theoretical ideas of hospitality can make sense of the ambiguities of being a racialized professional dealing with racism in healthcare from both patients and other healthcare staff.
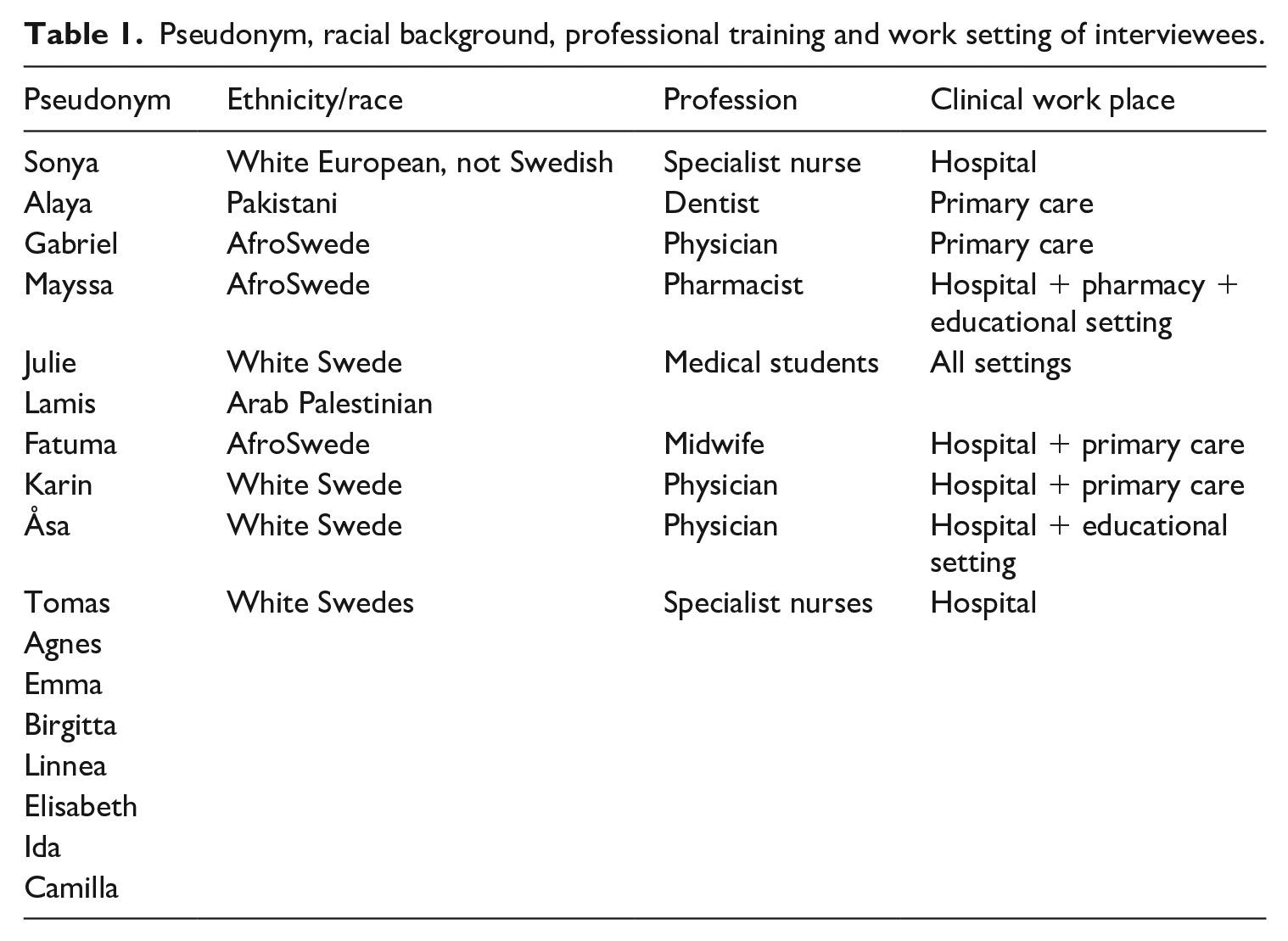
This analysis draws on a subset of 17 people’s interviews. As shown in Table 1, these 17 were made up of 11 White Swedes, one non-Swedish White European and five professionals or trainee professionals who had a non-European background that was racialized. This group of racialized staff had African, Pakistani or Arabic origins. These 17 people, involved in nine interviews (see Table 1) were sampled (from the wider group of 35 interviews with 58 people) on the grounds that they used hospitality and/or hostility as a means of explaining their experience in healthcare settings. The use of metaphors around hospitality and hostility in these interviews was particularly interesting because the topic was not prompted for, in that the interviewer posed no specific questions and the topic was raised spontaneously by interviewees.
Pseudonym, racial background, professional training and work setting of interviewees.
Results
Project Interview Material in General
Our project interviews were with healthcare staff (highly skilled, as well as lower skilled) and trainees who were born outside Scandinavia as well as ethnic majority, that is White Swedes. The language of dedicated professionalism was widespread: the desire to apply expertise and skills obtained through education and practice in order to make a difference to people’s lives. Unspoken or less emphasized in the material is the idea that staff should receive appropriate recognition for the skills and expertise that they offer. Racialized professionals’ and trainees’ experience of being deprioritized, over-looked and subject to overt racist abuse was commonplace and often interpreted as a lack of basic rights to be treated equally and to have qualifications, whether gained in Sweden or elsewhere, recognized. Some staff noted the emotional labour incurred by racism (Ahlberg et al., 2022), confirming earlier analyses (Evans and Moore, 2015), while others denied that discrimination was harmful to them, insisting that they could rise above it. The contested nature of gendered and racialized professional, ethnic and national identities is analysed here. In what follows, we analyse instances where hospitality was described as part of how subtle hostilities play out, to explore how hospitality can facilitate an understanding of the ambivalence of staff experiences of racism in healthcare settings.
Space and Place
Protracted proximity of patient and staff is central to most models of clinical care (telemedicine being the obvious exception). Fatuma was a midwife of African origin, who worked in both primary care and hospital settings and who spoke about the ambiguities of sharing clinical space where women were giving birth. She had worked in nursing for 20 years when we spoke to her, starting out as an auxiliary nurse, before qualifying as a nurse and later as a midwife. In reflecting on her experience, she described an episode from when she was an auxiliary.
A labouring mother-to-be and her partner had been offered space in a birthing room. As healthcare staff, Fatuma was hosting this couple, but her racialized status disrupts the host–guest relations. Fatuma described the process of being made unwelcome in the birthing room, despite being staff. She said that with particular patient groups – whom she described as ‘special people . . . who have it good and rich people who come from particular neighborhoods’ – as soon as she came in the door ‘they show with that body language, a mistrust’. On arriving to care for the labouring woman, Fatuma reported that she:
said hello and presented myself – that I was the auxiliary that was taking over – I got no real greeting in return. They just looked at me questioningly: ‘Who are you?’ . . . without saying a word, it’s the body language and they were very stiff and they show . . . what do you call it, distance, that they do not want to know me.
Fatuma said that ‘deep down, within the first two minutes, I felt that I am not welcome here’. She found this difficult, not least because of the inequality in how patients and staff can react to one another; even when she was made to feel unwelcome, Fatuma had to continue with her work with those patients, whereas patients could (and did) request to have her swapped out for someone else, somebody ‘more suitable’. When Fatuma felt the negative, distrustful body language, it was difficult to even cross the threshold into the birthing room. For the most part, Fatuma reported she could win her patients round, but the process of doing so was difficult and draining.
Despite Fatuma being a staff member and the symbolic host, working in familiar space, with familiar colleagues, she did not necessarily have a host’s power to specify who was welcome in the clinical space; indeed, quite the opposite, since she herself could be made to feel unwelcome by the guest-recipients of health services. If sharing time and space is core to the idea of hospitality (Dikeç et al., 2009: 12), this was something that Fatuma was willing to do but found her ‘guest’ (birthing mother and partner) unresponsive. The discomfort of the unresponsive ‘guest’ is part of the emotional labour that previously exclusively White clinical spaces imply for people of colour (Evans and Moore, 2015). The co-constitutive boundaries between host and guest shift in everyday healthcare practices and when social values associated with hospitality intersect with race and ethnicity, a different configuration of ‘hostipitality’ unfolds. The racialized dimension of the host–guest relations can be seen as a means of confining racialized staff to the category of ‘illegitimate stranger’, rather than host or guest (Lynch et al., 2011: 6).
Feeling unwelcome in one’s own work place was also described by Gabriel, an experienced physician of African origin who received his training outside of Sweden. After considerable difficulties getting licensed to practise in Sweden, Gabriel was unwelcomed by other staff and especially nurses while working in a hospital setting. He noted that although most of the patients were foreign-born, Gabriel still felt out of place and uncertain of his position as a physician. He described how his medical abilities were constantly questioned by ‘Swedish’ nurses whom he felt were watching and judging him. He reported that his medical authority was undermined as illustrated by an incident in the emergency unit where, despite his role as physician in charge, a nurse tried to take over: ‘This happened twice and it seemed like they did not want to have me there. It felt like they did not want me here.’
This pattern was also described by dental staff who were welcoming patients into the consulting room, but were themselves made to feel unwelcome. Alaya, a dentist of Pakistani origin, working in primary care with a White Swedish hygienist, described how patients made her feel unwelcome in her own consulting room:
Like when they come in, they don’t look me in the face, I can promise you, it is as if I am merely a spectator in the room, but they speak with the dental hygienist and yet I still have to treat them, when there’s this poor communication. It felt really awful, actually.
Alaya explained how she worked to welcome patients at the start of every consultation, even when patients would not respond to her, speaking only to the hygienist:
As soon as someone comes into the room, I am very welcoming. It’s like ‘Hello there! Come in! Are you in pain?’ And I speak directly with the patient and figure out the problem that has brought them to the consultation but I get no response except that they just turn their backs and speak with someone else. So that feels like ‘OK, but why can’t we have that conversation instead?’
We asked Alaya why she thought patients sometimes refused to speak with her and she suggested that patients think she’s not a good dentist because of her outward appearance, as a woman of colour and as a Muslim. The derogatory implications of some patients’ refusal to speak with her, were sometimes more explicit: one patient entered the consulting room saying ‘Ah! It smells of curry in here!’, which Alaya described as a personal attack. She asserted that there was no smell, but still the patient insisted on pointing out ‘I can smell it!’ Alaya described the difficulty of ignoring this patient’s insistence on the smell and continuing with treatment.
The roles of guest and host implied by hospitality are not fixed but contingent on people’s frames of action, responses and approach. They alternate and shift between different actors and open up for different forms of social interaction and relation, changing the subjectivities in that instance, at least temporarily. Furthermore, in these medical interactions, the taken for granted, obligations commitments and responsibilities of medical staff (as hosts) are redefined and to some extent, unsettled and dismantled by their guests (patients), and by other staff, highlighting the ambivalent and unstable nature of the relations. In challenging the professional and personal identities of the medical staff, patients can revoke rather than accept the hospitality of medical staff, by resisting, for instance, Fatuma and Alaya’s welcoming words. Staff can also disrupt the ability of a racialized doctor to authoritatively create the conditions for patient treatment, as explained by Gabriel.
Illegitimate Presence
Fatuma, Gabriel and Alaya were made to feel unwelcome and unauthoritative in their own work place. Fatuma went on to say that most clinical staff of African appearance were continuously made to feel illegitimate as they went about their daily business, which undermined self-confidence:
Someone is at them the whole time, seeing what they’re doing, what they’re up to, why are they doing that. . .? They say ‘Sometimes we feel as though we are thieves, even when we go into the sluice room to get stuff or whatever. It feels as though someone is looking and keeping tabs: “What has she taken? Why has she taken it?”’
Fatuma felt that staff of African origin were under constant suspicion, being surveilled for theft and illegitimate behaviour, when simply conducting their daily duties. This sense that staff of African appearance were subject to surveillance was confirmed by our experience of recruiting people to interview: a number of healthcare employees felt that they could not risk speaking with us, for fear of being accused of causing trouble in their work place (Ahlberg et al., 2022). This fear was not always assuaged by arranging interviews away from work places, nor by assurances of confidentiality.
The hostile attention that Fatuma described was covert and hard to pinpoint, in contrast to overt, aggressive hostility described by Mayssa, a pharmacist of African origin working in a hospital. Mayssa, who was raised and educated in Sweden, described various moments of hostility from patients and other staff, but one stood out as particularly damaging. A White Swedish physician talked about Africans in derogatory racist terms during a break in the staff common room. While discussing an event in Kenya, the physician went on to describe Africans as ‘un-civilized baboons:’
‘These Africans they are like baboons . . . I would never go to Africa! These Africans,’ he says ‘they are uncivilized!’ I panicked a bit . . . I just became completely stiff so extreme . . . really pissed, so I boiled, my whole body shook as well, and then I calmed down and looked at him and said: ‘Now you have to excuse this baboon who is sitting here in front of you and I would like to tell you that you are never welcome in Africa if you ever intend to go there.’ And then I left.
Sonja, an immigrant to Sweden from another European country, also described how auxiliary nurses who were of non-European background were made to feel unwelcome by White Swedish patients: an Ethiopian auxiliary nurse was asked to leave a hospital room when attending a Swedish patient. Sonja described an Iranian auxiliary nurse who was not recognized as a nurse and viewed by patients as part of the cleaning staff.
We also had a parent couple who were very unpleasant both towards her and told her . . . ‘No!’ She should leave the room and ‘Learn proper Swedish!’ So that they could understand what she was saying. And then we have another one who is from Iran and she has also been told that she was mostly cleaning staff and she should not be involved in their care.
Having worked for many years in different healthcare departments, Fatuma had observed that her colleagues did not like to work under the leadership of a manager who was seen as ‘not properly Swedish’: ‘They do not want to take orders from a (pause, silence) and they always shit-talk a nurse or midwife if you have a background other than Swedish. They always find something to complain about.’
Patients who were seen as foreign were treated as illegitimately taking up space in clinical settings. Two medical students told us how particular types of patients – described as being of Middle-Eastern, Roma or Somali background – were routinely treated as problematic, causing medical staff to ‘moan and groan’ about the difficulties such patients brought. One student, Julie, was White, while the other, Lamis, was of Arabic origin and both were nearing the end of their training, through which they had regularly heard negative comments about these difficult patients, such as ‘They are so noisy!’ and ‘Oh no! Are they bringing the whole extended family with them?’ Julie and Lamis said that they very seldom heard such derogatory comments with respect to White patients. In fact, if an old White man was visited by his wife, daughter and grandchildren, staff would interpret this as a caring family: ‘But with non-White people, there’s a completely different harshness in the tone of voice and it’s like “No! Only one relative is allowed here. All the others must leave!”’
There was no doubt for Lamis and Julie that during their training they witnessed outright aggression against non-White patients from healthcare staff, citing a supervisor who used the n-word in front of a group of students. Alongside harsh and outright hostility, they described indirect ways that non-White patients were side-lined and made to feel uncomfortable and unwelcome, with nonetheless negative effects: ‘So, such rather subtle stuff, but which still makes such a huge difference in . . . how I think people feel treated and how you . . . how welcome you feel when you come and seek care.’ Two White doctors – Karin and Åsa – confirmed that particular groups such as Roma were widely unwelcomed as patients. Migrant patients were undeserving of care as they were seen as illegitimately consuming welfare, while Åsa told us that ‘foreign’ patients exaggerate their pain: ‘They scream a lot and they scream their pain and they do not understand and things like that.’
The subtle way that the lack of welcome was communicated was described by Fatuma:
It is not upfront, they don’t do it straight but I’ve sometimes noticed, whenever there are patients from another background, my colleagues usually say like this: ‘Ah-ha! How many visitors have they got then?’ That tone – they anticipate that immigrants will have more visitors and it’s thought to be awkward when there are many people visiting. They say ‘Yes, that’s their culture . . .’ It is all about them and us, making a distinction between patient groups.
This division of patients into ‘them’ and ‘us’ that Fatuma describes, affected her too, by implication. Fatuma was born in Somalia, and described how her African origin came into play when patients who were seen as immigrants arrived on the ward:
And then sometimes patients arrive from, for example, the Horn of Africa, from Eritrea or Ethiopia, so the doctors come – and this has happened many times: ‘Excuse me, do you speak African?’ What kind of language is that? African? I usually say ‘I didn’t know that there was a language called African. I don’t know but you can teach me!’ ‘Yes, but that patient over there, in that room!’ I say ‘Yes, but she is perhaps from Eritrea and speaks Tigrinya. I cannot speak that language!’ Africa is not a country. Africa is a continent. It’s a shame that we have to put up with that.
Fatuma’s account of being co-opted by physicians assuming that she can communicate with any patient who seems to be African demonstrates how she straddles uncomfortably between a positionality of a host welcoming White guest-patients and a host acting as a bridge between the White colleagues and racialized minority patients. The repeated presumption that Fatuma, as an African, could communicate with other racialized patients makes the African patient’s lack of Swedish or English Fatuma’s responsibility. Fatuma herself is positioned as a stranger, and she is also made responsible for the short-comings of other illegitimate strangers. The discomfort that Fatuma describes in being identified primarily as ‘African’ can be understood in terms of hospitality as a ‘structure that regulates relations between inside and outside, and, in that sense, between private and public. Someone or ones, categorised as “outside”, as not necessarily, by right or legal contract, part of the “inside”, is temporarily brought within’ (Still, 2010: 11, emphases in original).
The social relation of hospitality is wholly dependent ‘on the relation between the one offering and other accepting or refusing’ (Still, 2010: 11). Patients can refuse a welcome; staff can refuse the authority of another staff member. And, despite racialized power imbalances, Fatuma resisted being positioned as an outsider, a stranger and described, in some detail, how she did this:
They often say ‘Oh, you speak such good Swedish!’ Why shouldn’t I speak Swedish? I’ve lived here for 30 years. They want to compliment me, but it’s wrong. Sometimes they want to push it a bit ‘Are you adopted? You speak such good Swedish!’ Am I adopted? No! ‘Are you married to a Swede?’ No, I am actually married to a man from Somalia and I was born and raised in Somalia but I grew up in Sweden. I came here as a child and I learned the language. I say to them ‘Swedish is only a language. Anyone can learn a language!’
When asked where she comes from, Fatuma answers ‘Somalia!’ Hostile questioners then query the possibility of her being both a Somali and educated as follows:
‘Are there educated Somalis?’ I’ve heard that so many times. ‘I thought that there weren’t so many Somalis who worked. I thought it was mostly Eritreans who worked. Somalis just sit home and give birth!’ I say ‘OK, that is not a picture that I knew about!’
In recognizing the range of intentions of her interlocutors, Fatuma noted that the questions could be hostile or posed with more neutral curiosity. Fatuma noted one particularly hostile patient group that she described as ‘rich people who are offhand and who are ill with cancer and I am there to help them and they have a lot of aggression’: ‘some people cannot cope with getting a cancer diagnosis, get aggressive and look for others to hurt in turn’. But regardless of their individual intentions, people are nonetheless pointing out that Fatuma is a stranger in Sweden – neither a legitimate, nor a welcome stranger:
Sometimes I feel, through the body language and how they put the question, sometimes it is pure curiosity and sometimes it is to show ‘Oi! You are still a guest in this country!’ There’s a lot of this from patients and also from work colleagues.
Fatuma points out that she has worked in Sweden for her whole career and never, in all of that time, has she had a single work session when her status as a stranger not been pointed out to her: ‘All the years that I’ve worked as an auxiliary or as a student (. . .) There has never been a single session without someone asking “Where are you from? You speak good Swedish.” Never.’ Fatuma has never been permitted to work in Swedish healthcare, without being reminded that she comes from elsewhere. This insistence on her status as someone whose presence needs to be explained is not lessened by her speaking fluent, idiomatic Swedish and working in an essential service, but rather intensified. Fatuma has a clear grasp of this irony as she told us that, rather than requiring her to justify herself, Sweden should be proud of her since she offers good knowledge of both Sweden and Somalia: ‘I can speak both languages, I know both cultures, I am a link to the Somali market. But Sweden doesn’t understand that. And . . . they will understand it too late.’
The concepts of hospitality and hostility usefully draw attention to the indeterminate aspect of staff–patient relationships while simultaneously highlighting the ambivalence and complexity of healthcare interactions. Racialized healthcare staff felt unwelcomed both by patients and other staff through explicit as well as more subtle refusal. Racialized healthcare staff whose medical abilities and expertise were not recognized had their contribution to healthcare organization ignored and discredited. Certain patient groups that were read as non-European and migrant, were regularly seen as undeserving of care and as exploiting the healthcare system. As such, both racialized healthcare staff and patients were positioned as illegitimate strangers, even if they have been born and raised in Sweden.
The Hippocratic ideal that healthcare is offered unconditionally and compassionately on the basis of clinical need has links with the model of unconditional hospitality to the stranger. Our interviews show that racialized healthcare staff and patients were regularly made to feel unwelcome, treated with hostility, and for staff, their host status was destabilized. The conceptualization of hostility as inherent to hospitality, allows racism to be understood as part and parcel of the experience of working in a European healthcare setting as a racialized person.
Doing Welcome
Fatuma offers an articulate guide to the complexities of managing a work identity while subject to racism, where her status as Swedish and as a healthcare professional, were repeatedly challenged, underlining the contingent nature of her claims to legitimacy, because her appearance was read as an interloper. Her detailed account was unusual in our material; much more usual were accounts of types of patients who were marked as illegitimate, as witnessed by Julie and Lamis, the medical students quoted above, and described by physicians Karin and Åsa. The harsh and subtle undoing of welcome, the hostility that undermines a person’s comfort as a patient or as a professional, stands in strong contrast to the (pre-pandemic) performance of welcome, which is standard in Swedish dental and healthcare practice. As a pre-pandemic norm, a patient, once they are identified by name and social security number is offered a hand to shake and told ‘Welcome!’ (in Swedish a one-word imperative greeting: ‘Välkomna!’). In some settings, it is the junior clinical partner, such as the dental hygienist or auxiliary nurse who takes on the welcoming duties, with the greeting sometimes repeated later by the more senior colleague – the dentist, midwife or obstetrician.
During a focus group interview with eight specialist surgical nurses from a teaching hospital, discussion arose about the failures of certain minority groups to participate properly in the welcome greeting. These nurses – mostly women, and all White Swedish – agreed that it was important to communicate with and understand the people in one’s care. As a specialist surgical ward, patients were drawn from across Sweden, with some cases travelling in from abroad for particular interventions. One nurse identified the challenge of meeting people ‘from extremely different cultural, religious backgrounds’ who, she contended, did not see ‘a woman as equally valued’, which for her was a ‘very basic’ value. The nurse said that it was difficult to:
understand such a person and still find a way of getting the job done and they feel themselves to be welcome and we feel OK with it. Because that goes against all that one thinks and believes. I have great difficulty with this thing, that people don’t shake hands. When one puts out one’s hand and says hello and they just (meaningful pause). I mean, what do they do?
The discussion continued, with the group agreeing that as healthcare professionals, they greet patients by shaking their hands in order ‘to show respect. Then you want to do the right thing.’ One nurse expanded on this idea as follows:
You greet each other and introduce yourself so we all feel welcome. That is normal behaviour here in my life, and for them it is: ‘We do not take unclean women by the hand.’ Or whatever their idea is there, I do not know.
This group of nurses were clear that patients should, ideally, feel welcomed into the clinical space, as part of good care. However, they also felt that it was impossible to welcome a person who indicated, through a reluctance to shake hands, that they did not value women appropriately. For these nurses, a patient’s refusal to shake hands was presumed to be based on sexism, which they found unacceptable. Their welcome was far from the ideal unconditional hospitable welcome of the stranger, and is much more suggestive of a conditional acceptance of long-standing acquaintances whose well-known difficulties are defensively anticipated. Discussing some patients’ refusal to shake hands allowed a naming of the sexism presumed to characterize certain foreign cultures. In the pandemic era, the meanings of hand-shakes may have shifted, but not the conditionality of the welcome into clinical space.
Conclusion
In this article, we revisit and operationalize the theoretical understandings of co-existent hospitality and hostility, through empirical insights from staff–patient interactions in healthcare. While hospitality is broadly defined by ‘reciprocity and exchange’ (Calvo, 2013: 110), it coexists, as our analysis demonstrates, with hostility where the guest is construed as challenging or threatening to take over the host’s social position as a medical provider (McNulty, 2007: xi). We identify two empirically driven nodes, which underpin the main contributions of this article. First, race and ethnicity highlight the internal contradictions of hospitality, identified in racialized staff’s everyday interactions with patients and other staff. Racialized minority staff are vulnerable to the hostility that is implicit in hospitality: as healthcare providers, they are required to maintain a good ethic of service towards patients, regardless of the hostility they receive, while also being ‘othered’ as potentially illegitimate strangers who must actively demonstrate their clinical worth. Second, and in line with Bulley (2017), we demonstrate how the subject-positions of host and guest shift alongside the spaces of belonging and non-belonging, as indicated by feelings of comfort and discomfort, security and insecurity, ease, and awkwardness (Bulley, 2017). The discomforts, sometimes masquerading as compliments about a person’s excellent language skills, persist long after a migrant has become a citizen, and are a manifestation of the hostility that is enfolded into hospitality. Arguably, this aspect of the unstable shifting subject position adds to the contested nature of racialized identities (Essed and Trienekens, 2008) in Sweden and the silencing of negative experiences in work place settings, including healthcare (Ahlberg et al., 2019; Bradby et al., 2019).
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Swedish Research Council, Vetenskapsrådet, Diarienummer: 2016–04078 Projekttitel: Rasism inom hälso-och sjukvården: utveckling och implementering av antirasistiska strategier genom gemensam kunskapsproduktion och utvärdering.