
Abstract
Loneliness, and its stigmatising nature, has long been of interest to sociology, with germinal contributions by writers such as Robert Weiss. Yet, the social stigma of loneliness remains under-theorised. Furthermore, recent scholarship on loneliness is dominated by psychological perspectives that often overlook the social role of stigma and its entanglement with factors like age-related norms and contexts. To address these gaps, we develop a conceptual understanding of the stigma of loneliness in later life. We focus on older people (65+) since loneliness is strongly linked with assumed age-related decline – illness, ‘uselessness’ and increasing isolation – which research suggests is more likely to be internalised in later life. In developing our conceptual lens, we creatively combine Erving Goffman and Imogen Tyler’s work on stigma. Such reconfiguration integrates relationality and power within micro and macro approaches, pushing forward sociological boundaries on stigma. It also foregrounds the connections between agentic and structural elements of stigma, which have been missing in loneliness studies. Through this lens, we derive key dimensions of the stigma of loneliness: enaction, reception and management. To apply our framework, we draw on interviews, diaries and ethnographic data capturing persistent loneliness among older people living alone and in care homes. Findings illuminate the complexity of loneliness stigma in later life contexts, offering new research and policy directions.
Keywords
‘Lonely? You are not alone!’
Loneliness gained wide attention during the COVID-19 pandemic due to lockdowns and related restrictions, prompting Japan to establish a Minister for Loneliness in 2021 (Osaki, 2021). Before the pandemic, in 2018, the UK had appointed the world’s first Minister of Loneliness to tackle a public issue of ‘epidemic’ proportions in industrialised countries (Jeste et al., 2020; Prime Minister’s Office, 2018). What seemed to be shifting with media depictions during COVID-19 was the acknowledgement that citizens of all ages may experience loneliness (O’Sullivan et al., 2021). Until then, loneliness research, policy and media portrayals focused predominantly on older people (aged 65+), an assumption being that afflictions of ageing bodies and diminished social connections make them especially vulnerable (Barreto et al., 2022; World Health Organization, 2021). However, loneliness is not a universal experience in later life, and later life is not a homogeneous stage (Neves et al., 2019, 2023a). Whilst some age-related changes can limit sociality among older people, the role of social devaluations of ageing in increasing vulnerability to loneliness in Western societies is often neglected in academic discourse. The very language used to describe loneliness, which is couched in deficits, implies that those who are lonely are somehow socially inadequate, reinforcing negative connotations (Jeste et al., 2020).
Loneliness is commonly defined as a subjective feeling of lacking companionship and missing social connection (Weiss, 1973). Yet it is surrounded with definitional ambiguity and even conflated with social isolation or living alone, despite a body of research showing those concepts differ (Shanas et al., 1968; Smith & Victor, 2019). Some scholarship describes loneliness as ‘perceived social isolation’, adding to that ambiguity (Campagne, 2019; Wenger et al., 1996). We approach loneliness sociologically, as both a personal and social phenomenon designating the absence of meaningful relationships. While felt at the individual level, experiences and expressions of loneliness are shaped by societal contexts. Feeling lonely is a complex emotion that interplays with social dimensions like stigma (McDaid et al., 2020).
Loneliness research, which is largely based on cross-sectional surveys undertaken in contemporary Western societies, provides only a snapshot of a historically and culturally variable phenomenon (Alberti, 2021). Longitudinal studies show that all age groups can be affected, but that persistent or prolonged loneliness (‘chronic’ in biomedical language) – rather than temporary or transient (episodic) – is usually reported among older people experiencing health issues and living alone or in care homes (Gardiner et al., 2020; Hawkley, 2022; Hawkley et al., 2019; Relationships Australia, 2018; World Health Organization, 2021). While these survey-based findings are valuable, they are generated by research that might exhibit epistemological blind spots like inattention to how classifications used to describe loneliness may shape experiences of and responses to it across different age and social groups. In failing to acknowledge these issues, researchers and policymakers can inadvertently reinforce stigmatisation and related harms. Discussions have arisen over whether, for example, survey questions that ask directly or indirectly about loneliness lead to underreporting due to stigma (Campaign to End Loneliness, 2023).
Whereas the association between loneliness and stigma is not new (Perlman & Joshi, 1987), references to it in many studies on the topic rarely extend beyond a sentence observing its relevance. As noted by McDaid and colleagues (2020), ‘There is ample evidence for the link between stigma and loneliness, but knowledge in this area goes little further than that’ (p. 13). Beyond the few psychological studies specifically examining the stigma of loneliness (Barreto et al., 2022; Kerr & Stanley, 2021; Lau & Gruen, 1992), conceptual and theoretical frameworks to grasp the links between stigma and loneliness are missing, especially in how they operate within personal and social contexts such as later life.
To help address this gap, we combine Erving Goffman’s (1963) thesis on stigma with Imogen Tyler’s work on the subject (2020) to develop a theoretical understanding of the stigma of loneliness. We conceptualise stigma as a complex social process of labelling, stereotyping and discriminating, which is situated within sociocultural contexts – including power relationships – that (re-)produce stigmatisation (Tyler, 2020; Tyler & Slater, 2018). This wider conceptualisation aligns with our sociological approach to loneliness. To explore the combined theoretical lens, we rely on studies of persistent loneliness among older people more likely to report feeling lonely – those living in care homes or alone and experiencing health issues (Neves et al., 2019, 2023a).
Context: Research on loneliness stigma
Loneliness has long been of interest to sociologists, as seen in the foundational work of Robert Weiss (1973) and Philip Elliot Slater (1971). However, sociological studies of loneliness have largely overlooked stigma. Whilst Robert Weiss (1973) referred to the shame of being lonely, the stigma of loneliness seems to have been first empirically studied in 1992 by psychologists Lau and Gruen. They conducted experiments with US college students, asking them to form impressions of people based on descriptions of hypothetical lonely and non-lonely persons. Findings showed the ‘lonely person’ was perceived as less sociable, competent, liked, attractive and sincere (Lau & Gruen, 1992). However, the experiments focused on a specific group of young people/context and drew on stereotypes about the deficiency of lonely people’s social skills: Don, the hypothetical lonely man, ‘doesn’t get along very well with his family and finds people in his community not interested in what he thinks or feels’, whereas Michele, the lonely woman, ‘envies and admires others in her dorm who seem to have no difficulty finding friends’ (Lau & Gruen, 1992, pp. 183–184). These psychological portrayals of lonely people as ‘loners’ or socially inept still pervade academic and public discourses (Franklin et al., 2019; Hauge & Kirkevold, 2010; Kerr & Stanley, 2021). Such deficit among lonely people is refuted by sociologists emphasising the role of social contexts in creating/maintaining loneliness (Franklin et al., 2019; Neves et al., 2023a) and by some contemporary psychologists who note that ‘lonely people are just as socially skilled as nonlonely people are’ (Kerr & Stanley, 2021, p. 171). Sociologists argue that Western societies’ praise of independence, self-reliance and hyper-sociability – alongside the pathologisation of loneliness via the popular ‘epidemic of loneliness’ discourse – contributes to those deficit perceptions and stigmatising practices (Barbosa Neves et al., 2023; Franklin et al., 2019; Hookway et al., 2019).
Casting light on stigmatisation among those who are lonely is recent research examining the underexplored relationship between loneliness stigma and sociodemographic factors (Barreto et al., 2022). The study drew on the BBC Loneliness Survey that included multiple countries but mostly the UK, 1 expanding prior US-based psychological research. Barreto et al. (2022) measured impressions of lonely people derived from Lau and Gruen (1992), internal/external causal attributions for loneliness (internal being more stigmatising), perceived stigma in the community, shame and concealment (asking participants to imagine discussing loneliness with co-workers and whether they would disclose it). Results demonstrated limited evidence on perceived or endorsed stigma; however, older people tended to make internal attributions for loneliness (internalising responsibility/circumstances), whereas younger people viewed loneliness as controllable, perceiving more community stigma, shame and inclination to conceal it. Barreto and colleagues (2022) suggested that since loneliness is associated with older people – being more ‘normative’ in later life – younger people might feel more ashamed, vulnerable to community stigma, and more likely to conceal it. Whilst their study askedparticipants to mostly make attributions for another person’s loneliness rather than themselves, their data illuminate societal perceptions. Relatedly, Hauge and Kirkevold (2010) had found that lonely and not-lonely Norwegians held negative views towards lonely older people, seeing loneliness as their fault. Exploring such later life ‘normativity’ – and views of loneliness as deficits connected to old age – is critical. For that, we can gain from studying lived experiences of loneliness-related stigma among older people. A few studies have explored the topic, but usually as one theme among others (Neves et al., 2019, 2023a; Rokach, 2015).
In sum, we continue to lack conceptual and in-depth understandings of the links between loneliness and stigma, which are relevant to explore later life contexts associated with it: how is this stigma created and enacted in social contexts? How is it received and managed by those mostly affected by it? How do agentic and structural dimensions (i.e. personal and social) contribute to the creation and management of loneliness stigma? Sociology can provide novel theoretical insights to clarify these linkages, particularly through relationality and power. We turn to this next, reconfiguring existing sociological theories to support a conceptualisation of the stigma of loneliness and its dimensions.
Theorising the stigma of loneliness
Stigma relationality
Erving Goffman’s treatise on stigma (1963) remains widely used to explain the phenomenon (Scambler, 2009; Tyler & Slater, 2018). Thus, departing from Goffman offers initial ideas to frame the stigma of loneliness – in later life and more generally. We draw on his definition and engagement with different forms of identity to conceptualise stigmatisation processes.
Stigma is more than ‘an attribute that is deeply discrediting’ (Goffman, 1963, p. 12) like a disease or physique. Since stigma emerges and acts within social interactions, we require a ‘language of relationships, not attributes’ to understand it. The attribute is ‘neither creditable nor discreditable as a thing in itself’; it is socially constructed (Goffman, 1963, p. 12). To comprehend this relational process, we must consider social identity, including Goffman’s distinction between virtual and actual social identity. Social identity relates to socially classifying people based on attributes, leading to membership in social categories and the provision of comportment scripts/templates (Goffman, 1963). When we meet someone new, we rely on first appearances to categorise them, applying personal (e.g. sociable) and structural (e.g. occupation) attributes and developing a virtual social identity, which might not match their actual social identity (i.e. attributes that belong to the person and that they possess). When a person has an attribute setting them apart from the societal norm in an undesirable manner, they can become ‘tainted, discounted’: ‘Such an attribute is a stigma, especially when its discrediting effect is very extensive . . . . It constitutes a special discrepancy between virtual and actual social identity’ (Goffman, 1963, pp. 10–11).
Stigma is linked to how identities are perceived, created and managed in social interaction: if a person is linked to a stigmatising attribute, they are socially categorised and labelled as discredited or discreditable (Goffman, 1959, 1963). Being discredited means that the stigmatised individual discerns their difference is visible/known to others, and being discreditable that their difference is unknown/invisible (Goffman, 1963). Stigma entails structural dimensions beyond specific encounters. The stigmatised person often has the same beliefs about identity as the ‘normals’ – they might feel normal inside, yet in the presence of ‘normals’ they become the not-normal (Goffman, 1963, p. 14).
Identities also shape how stigmatised people manage their stigma (Goffman, 1963). The stigmatised person can attempt to correct their attribute, or they can reclaim/reframe their social identity. In encounters with others, they must decide what ‘to display or not to display; to tell or not to tell . . . and in each case, to whom, how, when, and where’ (Goffman, 1963, p. 50). This demands constant management of personal and social information. Discrepancies between virtual and actual identities cause tension management or information control. In such situations, we must attend to what Goffman (1963) terms visibility (different from knowing about it) and obtrusiveness (how it affects the flow of interaction) of a stigmatising attribute as well as its perceived focus (how it might disqualify a person). For instance, ‘ugliness’ might be visible and affect social situations through obtrusiveness, although it is usually perceived as having no impact on competency (Goffman, 1963, p. 58). These interplays, therefore, frame strategies of stigma disclosure and concealment.
Personal identity is another dimension affecting stigma management, particularly among close ties like family (Goffman, 1963). While social identity looks at larger group identification, personal identity differentiates the individual from others. This identity includes what makes a person unique, based on their name, legal documents and relationships. A common strategy of the discreditable person is to disclose their stigmatising attributes to close ties but not to wider networks, ‘passing’, ‘covering’ or ‘controlling information’ on their condition/status (Goffman, 1963, pp. 102–110). Because stigma can be extended to family/friends, social and personal identities interact in stigma management: social identities illuminate stigmatisation processes, whilst personal identities justify information control in stigma management (Goffman, 1963).
To understand what the stigmatised person feels, Goffman (1963) introduces ego identity, a subjective sense of oneself originating from social experiences (p. 114). This captures the reflexive part of the self, the connection between the individual and their self-image; what one thinks they are inside, rather than as ascribed by social and personal identities. Ego identity recognises one’s agency but brings ambivalence as the stigmatised individual must choose identity standards they struggle to conform with, leading to association or disassociation with other stigmatised people (Goffman, 1963). This explains why those stigmatised in one situation can stigmatise in another: ‘The normal and the stigmatized are not persons but rather perspectives’ (Goffman, 1963, p. 145).
Managing stigma encompasses continuously managing identities. A stigmatised person is encouraged to accept their stigma and adopt normative behaviours, which can amplify the original stigma, resulting in phantom acceptance (Goffman, 1963, p. 130). In this context, self-presentation attempts (how one presents to others) arise to alleviate stigma and support a desired identity through ‘impression management’ – i.e. efforts to control others’ perceptions of us (Goffman, 1963). Analysing identity as multi-layered is, thus, essential to understanding stigma: social identity elucidates how stigma is socially created and sustained; personal identity how stigmatised people manage their stigma via how they socially present; ego identity how one feels stigma and internalises its outcomes. These identities are critical to grasp the stigma of loneliness and its management.
While Goffman’s approach informs our conceptual exploration of the stigma of loneliness, new criticisms of his work have shown the need for ampler structural lenses (Tyler, 2020). Goffman’s focus on everyday interactions (micro) was situated within unequal structures (macro) – and stigmatisation was seen as social control – but he relied on normative abstractions (‘normals’), neglecting structural dimensions such as power (Scambler, 2009; Tyler & Slater, 2018). Of value in this respect is Tyler’s (2020) exploration of stigma power, whose work we discuss next.
Stigma as productive power
Imogen Tyler (2020) contends that stigma is about power. As she argues, ‘psychological understandings of stigma often focus on individual experiences of being stigmatised in ways that occlude an understanding of stigma as a material force, a structural and structuring form of power’ (pp. 8–9). To advance such understanding, Tyler uses the concept of stigma power, as the ability to ‘keep people in’, ‘down’ and ‘away’ (Link & Phelan, 2014). Stigma is used, through obvious or subtle processes, to manage, control, exclude or exploit others: for instance, the ‘misrecognised’ interests of stigmatisers (and larger social system) affect how people with mental illnesses cope with stigma (Link & Phelan, 2014). Their coping through staying ‘in’, ‘down’ or ‘away’ responds to the negative social perceptions/actions about/towards those living with mental illnesses, which in turn align with the stigmatisers’ interests (Link & Phelan, 2014).
Centring power helps resituate stigma within diverse sociocultural contexts that produce social inequalities (Tyler, 2020). In this vein, Tyler (2020) sees stigmatisation as a practice that, although felt at the personal level, intertwines with broader social structures of control, exploitation and domination. Through the ‘political economy of stigma’, attention must be given to the role of stigma power ‘in the distribution of material resources and the transformation of cultural values, the crafting of stigma in the service of governmental and corporate policy goals, and the cultivation of stigma to extract political and economic capital’ (Tyler, 2020, p. 26). For example, welfare ‘stigmacraft’ 2 engineers the belief that poor people are to blame for their poverty due to lack of discipline and merit (Tyler, 2020). These beliefs and perceptions constitute ‘stigma-optics’, which are used to degrade people living in poverty, while justifying the machinery of neoliberal and extractive capitalism (Tyler, 2020, p. 197). Stigma is thus a form of ‘productive power’ – its creation and maintenance a way of leveraging capitals, of devaluing people and communities to reinforce existing social hierarchies and wealth (Tyler, 2020, p. 28). The deficit discourses imposed on those who experience loneliness and the normative assumption strongly associating it with later life reinforce the social values of youthfulness, hyper-sociability, independence and individualisation in late modernity (Franklin et al., 2019; Hookway et al., 2019).
Stigma is not ahistorical or apolitical. The word derives from penal tattooing and slavery in the ancient world – a way of marking an inferior social status into people’s bodies; a dehumanisation mechanism that is core to colonialism and imperialism (Tyler, 2020). Consistent with this history, stigma continues to be entwined with political punitive processes inscribed on bodies (Tyler, 2020). Conceived as such, stigma is useful to illuminate the sociopolitical functions of categorisation/classification, including its application to people of different ages. Recalibrating stigma as power in political economies offers an analytical tool to explore how social practices stigmatise and how stigmatisation influences how people see themselves and others, encapsulating ‘internal and external processes of de/valuation’ (Tyler, 2020, p. 239). Reconceptualising stigma as an inequality machine ‘trouble[s] individualistic understanding of stigma by developing a more structural understanding of stigma as a classificatory form of power’ (Tyler, 2020, p. 260). This requires considering sites of stigma production (politics, governments, corporations; stigmacraft by media, social media, cultural industries; everyday stigmatising interactions, etc.) to comprehend its functions and who gains from it (Tyler, 2020).
Whilst Goffman’s stigma is ‘relational’, i.e. situated within social relationships and contexts, he did not contemplate the ‘histories of power’ (Tyler, 2020, p. 99) creating those relationships, nor the wider sociocultural contexts of stigma, including the sites producing and benefiting from it. In our efforts to advance a conceptual understanding of loneliness stigma, we cannot neglect approaching stigma as productive power, and stigmatisation as a process of dehumanisation, exclusion and exploitation. Next, we show how we innovatively reconcile Goffman and Tyler’s perspectives, expanding the sociological canon on stigma but also our understanding of the processes and practices of loneliness stigmatisation.
Loneliness and stigma relationality and power
Analysing the relationality (Goffman) and power (Tyler) of loneliness stigma means studying its agentic and structural dimensions: i.e. the personal and individual meanings and actions attributed to it as well as the social and cultural contexts shaping them. This allows capturing processes of stigmatisation without overlooking its interrelations with social control and inequality (Link & Phelan, 2014; Tyler, 2020; Tyler & Slater, 2018). Such approach supports our definition of loneliness as both a personal/individual and social/structural phenomenon. The stigma of loneliness can be approached as a relational external and internal process and practice of labelling, stereotyping and discriminating (Goffman, 1963) based on sociohistorical contexts that devalue and exclude (Tyler, 2020) those perceived as not socially connected, sociable or with social aptitude. A language of relationships (Goffman, 1963) and power (Tyler, 2020) enables a comprehensive exploration of loneliness stigma through linking: (1) social interaction and identities (Goffman, 1963), and (2) devaluation/valuation practices and inequalities/equalities (Tyler, 2020). These combined insights allowed us to derive three conceptual dimensions to frame how loneliness stigmatisation in later life is created, felt and handled within personal and social contexts, namely through: enaction, reception and management (see Figure 1).

Conceptual framework.
Enaction of stigma relates to labelling, stereotyping and discriminating processes/practices, which can be internal or external. Linked to enaction are social identities and its contexts (Goffman, 1963), including structural forces and productive power (Tyler, 2020). Reception entails how those living with loneliness receive and understand stigma (enacted or potential) through (1) feelings, (2) identities (ego identity and tensions between social and personal identity) and (3) internalisation/externalisation optics. These ‘stigma-optics’ relate to internal and external de/valuation processes (Tyler, 2020). Management comprises mechanisms of control, self-presentation and impression management. Linked to it are personal identities (elucidating how stigma is coped with via self-presentation; Goffman, 1963) and forms of social control like stigma internalisation (Tyler, 2020). While enaction, reception and management of stigma can occur simultaneously, we see analytical value in distinguishing them. Nonetheless, they are related and interact, being situated within sociocultural, historical and productive power contexts enabling stigmatisation processes/practices and responses to it (Goffman, 1963; Tyler, 2020).
In the sociology of health, Scambler (2009) has also drawn on Goffman to derive conceptual dimensions of stigma. Focusing on people with epilepsy, Scambler (2009) and Scambler and Paoli (2008) identified enacted (discrimination), felt (shame and fear) and project stigma (strategies to contest or evade enacted stigma and avoid felt stigma). This work illustrates similar understandings of Goffman’s oeuvre to inform theorisations of stigma. Nevertheless, our dimensions are analytically broader: reception of loneliness stigma can comprise Scambler’s felt stigma but also includes Goffmanian identities and Tyler’s stigma-optics. Enaction comprises labelling and stereotyping, not just discrimination. Management encompasses all coping strategies, which do not have to necessarily challenge stigma.
While our lens and related three dimensions can be used to conceptualise the stigma of loneliness more generally, we apply it to frame how stigmatisation is linked (implicitly and explicitly) to lived experiences of persistent loneliness among older people. This facilitates an exploration of the deficit discourses associated with feeling lonely in later life and its ‘normativity’, as suggested in the literature (Barreto et al., 2022).
Applying a stigma of loneliness lens
Employing a multiple case study method, we merged two research projects on loneliness in later life (Yin, 2009). Projects focused on older people (aged 65+) who are more vulnerable to loneliness: (1) those living in care (nursing) homes and (2) those living alone (community-dwelling) while experiencing health issues that affect social interactions. Both studies aimed to understand meanings and lived experiences of loneliness. Through cross-synthesis, we integrated findings via similarities and differences (Yin, 2009). Projects were approved by our ethics committees. Participants signed informed consent forms, but we ensured ongoing verbal consent throughout the research.
The first project collected qualitative data in two Australian care homes (2018) through participant observation and semi-structured interviews with 22 residents. Participant observation mapped the everyday social and institutionalised contexts of residents, interactions with staff, visitors and other residents, in-house programmes/activities and daily routines. Interviews asked about meanings, feelings and experiences of loneliness. Bluebell home (pseudonym) had mainly single rooms and a ‘luxurious’ environment with public areas, gardens and a cafe. Rosewood (pseudonym) was a smaller facility with shared rooms, accommodating low/middle-income residents. Recruitment was done in collaboration with staff, identifying residents without cognitive impairments affecting consent capacity. We then approached those residents independently, sharing our aims/approach and recruiting 16 women and six men (aged 65–95) who volunteered to participate (see Table 1). Nineteen interviewees reported loneliness, three reported social isolation. We asked participants to define both loneliness and social isolation; however, most conflated the two concepts, only defining loneliness.
Participants’ sociodemographic characteristics.
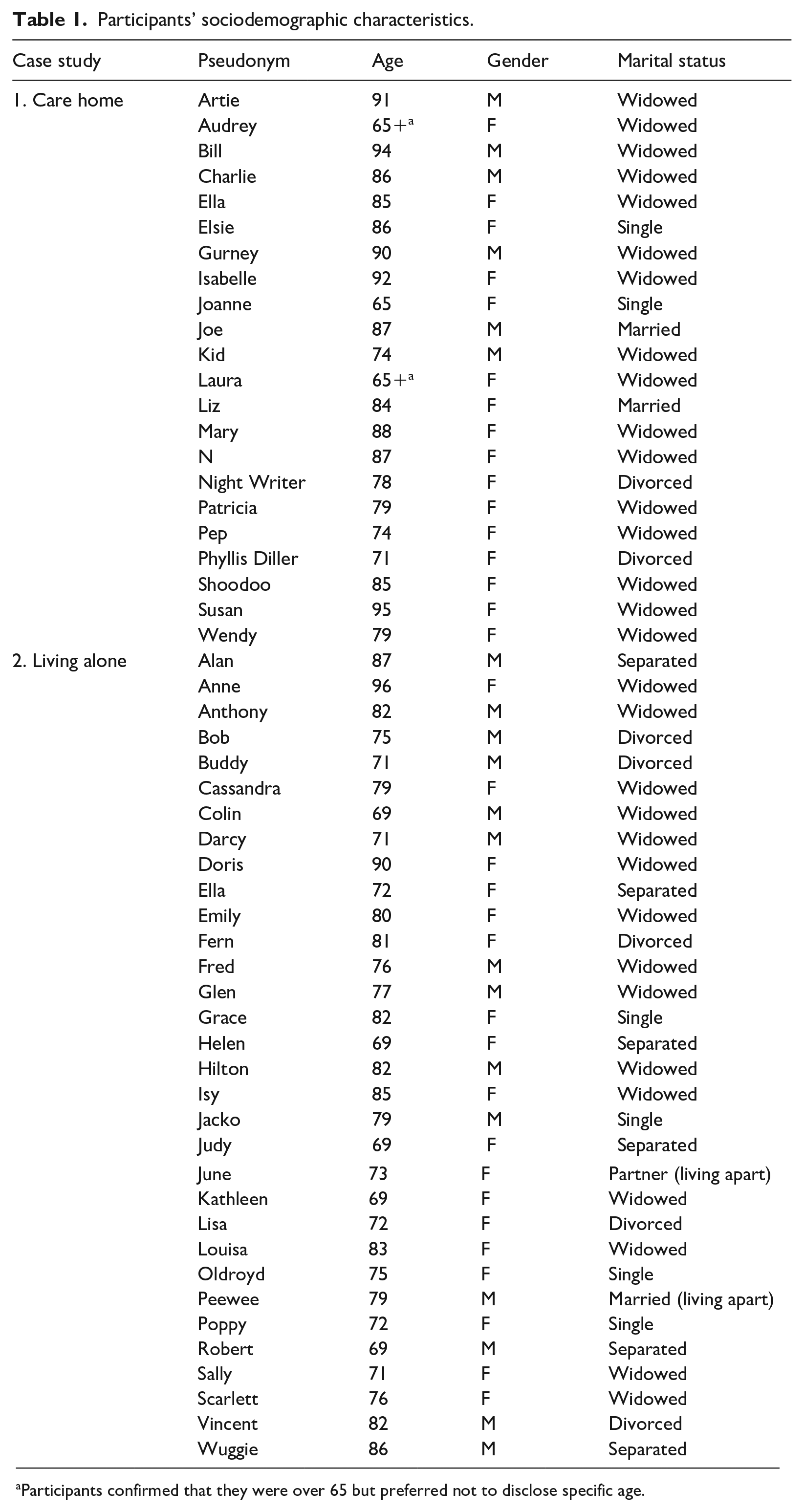
Participants confirmed that they were over 65 but preferred not to disclose specific age.
The second project was conducted with 35 older Australians (65+) living alone and reporting loneliness, recruited through municipal councils in Victoria. Data collection took place during COVID-19 (July–December 2020), but asked participants to reflect on loneliness before the pandemic. It included semi-structured interviews, loneliness scales and qualitative diaries. For this article, we use diary data produced during a lockdown (October 2020). Diaries were flexible participatory tools for participants to collect/narrate their feelings, actions and contexts (Milligan & Bartlett, 2019). This method was useful to avoid ‘reproduce[ing] or naturalis[ing] existing stigmatising social hierarchies’ (Tyler, 2020, p. 213) by empowering participants to control what/how to share their experiences as research partners rather than subjects (Neves et al., 2023a).
Diaries were developed by 32 participants (aged 69–96), including 18 women and 14 men (see Table 1). Diarists were asked to record daily feelings, thoughts and activities at least twice a day (morning and evening) for seven days. Duration and format were agreed beforehand: 19 participants opted for paper diaries and were sent a package with pens and journals; the remaining chose digital diaries (emails, text, audio).
Data of both projects were thematically analysed through identification of codes and themes within (individual) and across (collective) cases (Saldaña, 2021). Coding was deductive (including codes corresponding to research aims) and inductive (new information identified in the data) (Saldaña, 2021). After in-depth reading of transcripts/diaries, we generated codes and combined them into themes. Data were coded independently and then collectively by the first author and a research assistant, reaching consensus on final themes. We did not enquire directly about stigma, although it was identified as a main theme. We then fine-tuned our analysis by re-engaging with data through thematic narrative analysis to tease out ‘what’ was being ‘told’ (Riessman, 2008, pp. 53–54) about stigmatisation and its dimensions (stigma enaction, reception, management) in participants’ stories. To apply our theoretical approach to stigma, we attended to descriptions of social interactions, identities and broader sociocultural contexts. This narrative approach addressed Tyler’s call for stigma researchers to ‘care in how we draw on the voices and experiences of others’ (2020, p. 213). Goffman’s depictions of those stigmatised are criticised as thin, abstract, and even dehumanising, demonstrating the need for thick accounts of stigma (Tyler, 2020, p. 269). We have made similar arguments regarding loneliness accounts (Neves et al., 2023b, 2024).
Next, we report the thematic narrative results, concentrating on the links between loneliness and stigma enaction, reception and management. We prioritise thickness, engaging deeply with a few participants to capture overall and nuanced experiences in the two settings, beyond just enumerating themes or separating excerpts from each participant to fit across dimensions.
Findings
Enaction of stigma
While most participants did not mention the enaction of the stigma of loneliness, their narratives illuminate its processes, particularly in how the label ‘lonely’ might reinforce stereotypes and discrimination. Labelling and stereotyping development were visible through perceptions of loneliness in later life. Enaction of stigma was mostly internal, as the majority concealed their loneliness from loved ones to avoid a sense of personal failure or demise. Loneliness stigma did not seem to operate in isolation; it was interrelated with the stigma of being old and frail, demonstrating the role of broader sociocultural contexts that value sociability, productivity and young healthy bodies. Participants seemed unable to hide their ageing or frailty; yet were able to hide their loneliness. For a few, stigma was enacted through external interactions and then internalised.
Gurney, at age 90, describes himself as ‘old and lonely’, while joking about wanting to join a youth club. He moved to the care home due to illness, after retiring as a hospital warden. His loneliness started when his wife of 65 years passed away. Gurney’s only surviving son lives in Scotland but calls every Saturday. He feels lonely because ‘there’s nobody I can talk to here’ and many residents have dementia, restricting conversations. Life and activities at the care home are ‘booooring!’ He is passionate about aviation and when a former woman pilot moved in, he was excited by a friendship based on shared interests. But ‘management found out we were being friendly’ and relocated her. Gurney emphasised ‘there was nothing romantic!’ and they were both devastated by management’s actions. He feels stigmatised by staff: Always talking to them about different things and I’m being shot down at every turn . . . this asylum is not being run by the inmates, you know, I’m not allowed – and of course my age, that’s a bit of a stigma. People are saying, ‘90 years old, come down a notch’, you know? You’re not given credit for any logical thought so . . . not allowed to think.
Throughout participant observation of the care homes, we witnessed this constant diverting behaviour by staff (and family). When residents mentioned sadness or loneliness, conversations were rapidly redirected to more positive topics like the garden. This active evasion seemed to reinforce loneliness as a negative subject to avoid – ‘you give up trying to talk about it’, explained Gurney.
Evident in Gurney’s accounts of loneliness and its stigma are the constraining contexts of care homes at micro- and macro-levels. The latter seems to reflect Western ageing policies and aged-care industries that stigmatise and control frail ageing bodies; the former, types of interactions tolerated or available. A care model that homogenises later life, through activities and routines, and devalues older people’s agency by dismissing or ignoring it, can contribute to stigma enaction by controlling residents’ emotional expressions (Brossard, 2016; Neves et al., 2019). The fixation on emotional ‘positivity’ in our neoliberal age, whereby resilience and happiness are especially prized (Gill & Orgad, 2018), can lead to concealment of loneliness. Gurney’s ‘compromised’ social identities as old, frail and lonely (Goffman, 1963) appeared to shape the enaction of the stigma of loneliness (external and internal), which cannot be dissociated from wider social contexts of devaluation and productive power (Tyler, 2020).
Lisa, 72, has been living alone with her 15-year-old cat, Lion, since she got divorced. She works part-time in health administration to supplement her meagre pension. Previously, she was a flight attendant. She has struggled to make ends meet, and her house needs urgent repairs. Her diary captured loneliness already felt before COVID-19, yet ‘The pandemic does make you more aware of loneliness because you are restricted from finding sources to overcome it outside of using technology’ (see Figure 2 for full entry).
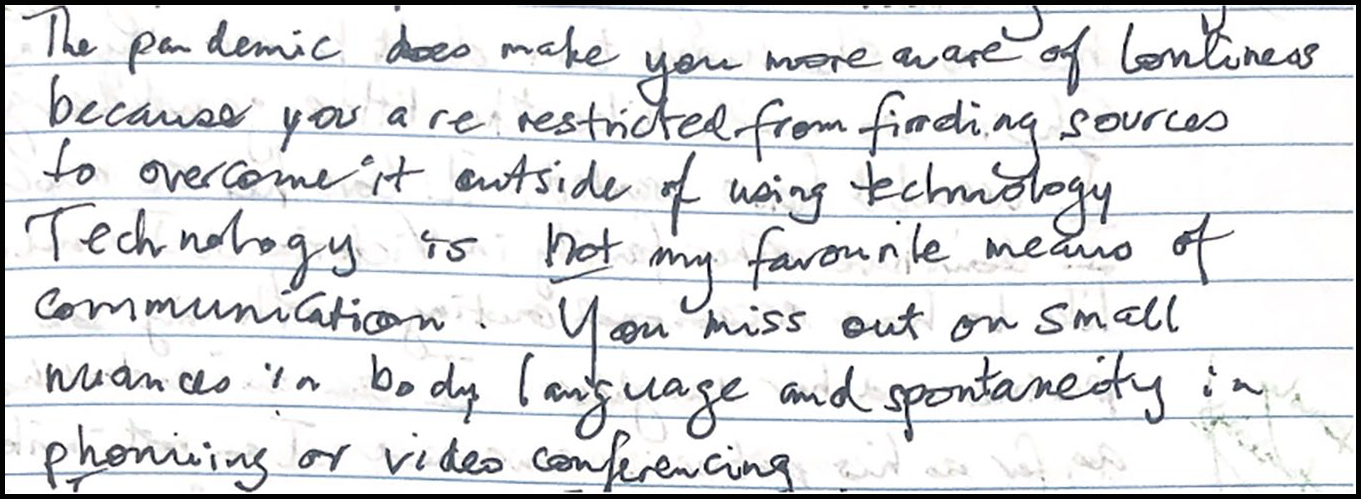
Lisa’s diary entry.
Lisa feels lonely because she has no one to share her life with. Her only son seldom calls, and that frequency diminished with the pandemic: ‘his call takes about 3 minutes, this is about as much time that my son can spare me’. She has a few friends, but visits and outings ceased during the COVID-19 lockdowns.
Lisa also feels lonely in her workplace: ‘The set-up at work shows me that you can be lonely even when you are not alone.’ She is labelled ‘old fuddy-duddy’, which affects how co-workers engage with her: It infuriates me that you get a label, and it sticks. It has been decided that I am ‘past the due date’ and if fault can be found, it will add an arrow to the quiver . . . . I can’t get a job because of my age. There are laws against age discrimination but on legal advice I have been told you have nothing to gain by lodging a complaint – you are better off using your sick leave.
For Lisa, being an old woman who is lonely and financially precarious provides a collection of labels, contributing to the stigma of loneliness and workplace discrimination. For instance, despite her requests, she is not given more work. Lisa’s accounts of loneliness illuminate the intersections of age, gender and social status in stigma enaction. Stigmatisation of loneliness can interact with stereotypes about older workers and with the growing financial hardship faced by single and widowed older women concerning income and housing insecurity (Burn et al., 2020). These circumstances can compound one’s loneliness and its negative connotations.
These cases exemplify how loneliness in later life is situated within complex social and personal contexts; and how loneliness intertwines with categories such as ageing and related social identities. Enaction of loneliness stigma can be a straightforward process of labelling, stereotyping or discriminating, but also a covert one. Most participants described an internal process – which was the result of potential or encountered external interactions and processes. Or, as in Gurney and Lisa’s cases, they may be both encountered and potential. Implicit in participants’ understanding of loneliness was the relationality of stigma (Goffman, 1963) and other forms of control and inequality (Tyler, 2020), from ageism and precarity to care homes, which foment labels and constrain sociabilities (Brossard, 2016).
Stigma reception: Feelings, identities and optics
Participants conveyed the pain of loneliness that left them feeling forgotten and rejected. All narrated embarrassment about feeling lonely and blame for ‘not making more friends’, ‘being a loner’ and ‘not being interesting anymore’. Most concealed loneliness due to fear of indignity and of compromising personhood and identity: for those living in care homes, disclosing their loneliness would add more ‘load’ to their status of dependent older people; for those living alone, it would threaten their independence and autonomy. Former identities seemed spoiled (Goffman, 1963) by their current loneliness too, as many mentioned not being ‘like this’ before. Participants internalised the stigma of loneliness through feelings of shame and guilt (often based on social optics about later life as decline), and experienced tensions between who they are and who they want to be.
Patricia, 79, moved to a care home because she had no one to look after her. She was a factory worker and loved ballroom dancing. Patricia’s four children visit or call occasionally, but ‘they’ve got their life to live’. She lost her husband years ago. Central to Patricia’s narratives are broader meanings and contexts about ageing shaped by individualistic notions of family and care in late modernity (Torbjörn & Peter, 2017). For instance, Patricia, along with most participants, cited families’ ‘very busy lives’ to excuse their infrequent contact. She feels very lonely, because: You’re just here on your own . . . . That’s the main factor with all us people. They [family/community] don’t bother with us once we get too old . . . they forget what it was like for us once . . .
Patricia does not disclose loneliness to those around her since she does not want to make anyone ‘miserable’ or bother her children. She wants ‘to get on with life’ and not ‘get lonely’. To distract from loneliness, she sits by her bedroom’s window: ‘I look out there when I feel lonely . . . the trees are not lonely, see?’
Bob, 75, divorced and living alone, worked as a security guard before retiring. Every morning he receives a brief phone call from the Red Cross ‘just to check that I am still alive’. He distinguishes between being alone and loneliness, although sometimes they intertwine, as ‘if it wasn’t for these phone calls, I’d spend many days on end without uttering one word!’ He wrote about the ‘bitter sadness’ of being lonely and its ‘“dark feelings” . . . not really clinical depression, but close to it’. He does not ‘believe that psychology or psychiatry drugs would alter the mood and make the root of a situation disappear’.
Producing the diary helped him express his loneliness but also confront ‘the reality [his] generation is suffering’. Bob believed he was part of a caring community; however, as he grew older, he ‘was horrified to discover otherwise’. Loneliness ‘is a real fact of older age’ and his body must cope now with illness and loathing. The ageing body can act here as stigmata, showing the materiality of stigma via bodily classifications/inscriptions (Tyler, 2020). Loneliness brings despair and adds to a conceded sense of social value and identity: Bob is a lonely ‘old-age pensioner regarded as unproductive (anymore), invalid, good-for-nothing-old-man, parasite on the community’. Internalisation of loneliness stigma seems heightened by other internalised stigmas attached to being old and frail, resting on wider social structures of productive power (Tyler, 2020) that devalue and marginalise ageing bodies.
As illustrated by Bob and Patricia, the stigma of loneliness can be an internalised process of social devaluation and ‘stigma-optics’ (Tyler, 2020) affecting ego identity (who they feel they are) and creating tensions between social and personal identities (who others think they are and who they want to be) (Goffman, 1963). This was a reality affecting most participants. For them, it was preferable to be ‘discreditable’ and suffer in silence (Goffman, 1959, 1963) rather than disclose their loneliness, which unintentionally ends up supporting exclusion and marginalisation (Link & Phelan, 2014; Tyler, 2020).
Stigma management: Control, self-presentation and impression management
Participants managed their loneliness as a coping mechanism and a way of avoiding potential stigmatisation. Reporting of stigma management was indirect, as stigma seemed embedded in both general understandings and responses to loneliness in later life. Besides engaging in impression management to maintain a self-presentation that avoids the ‘lonely’ label and conceals loneliness, participants adopted control strategies involving individual activities to keep themselves distracted (e.g. reading) or social activities (e.g. volunteering) as opportunities for connecting with others.
Audrey has been living in a care home for a few months after a fall. She did not want to leave her ‘real home’ but felt pressured by her doctor and family. Audrey is widowed and like many of our interviewees, had no one to support her at home. These circumstances also reflect a broader shift from family- and community-based care to institutionalised later-life care in contemporary Western societies (Phillips, 2007). Moving to a facility impacted her independence and exacerbated her loneliness. As she does not want to disclose her situation to friends, they are unaware she lives in an institution, furthering her loneliness: ‘They’ll be shocked to find me here!’, she justified. She still calls friends, but ‘they think I’m at home talking to them . . .’. She does not want to mention her new status and loneliness, offering only ‘I can’t. Too much!’ as explanation. At the care home, she has no one to converse with since most residents ‘have Alzheimer’s’. She feels lonely, because: There’s nobody you can talk to. Most of the time, when the tea lady comes with the tea, I talk to her. Because they’re the kitchen staff. They’re normal people. But – anybody here – who can you talk to?
Stigmatised people’s own stigmatisation of residents living with dementia (found across interviewees) adds to Goffman’s claim (1963) that stigma is about perspectives, while revealing the role of ego identity in stigma management – in this case, through disassociation from other stigmatised people. This also reflects Tyler’s arguments (2020) on how stigmatisation emboldens social divisions.
Audrey was ‘a very independent person’ – she told us, while crying. She tried to regain her independence by keeping busy at the facility with housework and small jobs, like organising religious services. To alleviate loneliness, Audrey must: Keep myself occupied. In the bathroom, I’m washing my underwear, my clothes, my nightdress. And then my room – I make my bed. I don’t allow anybody [staff] to do anything. I do it myself. I dust and clean.
She described herself as ‘old’ and ‘lonely’; yet she did not want to divulge her age to us, just confirming she was over 65.
June, 73, has been living alone with her canary, Smoky, for many years, after getting divorced. Contact with family is infrequent, except with a son located in Melbourne, with whom, before lockdowns, she had dinner once a month. June was a nurse, but is now the president of a seniors’ club, which brought purpose to her life, helping tackle loneliness. However, the pandemic-related lockdowns stopped the club’s activities, aggravating her loneliness: ‘I often wonder what my life has to offer’, she wrote in her diary. June appreciates her independence but confided that despite telling everybody she loves being on her own, she hates it.
Her entries fluctuated between hopeful words about returning to her club and expressions of deep loneliness, often associated with being ‘old’. She noted: I get so lonely – nothing to do – nowhere to go – I just lay there trying to sleep, but everything goes through your mind . . . When you get old, no one wants you, I often feel I’m in the way (see Figure 3 for full entry).
The recurrent notion that old age means ‘no one wants you’ demonstrates how loneliness and later life can interact at the micro-level through internalisation and at the macro-level through social values, relationships and ageism.
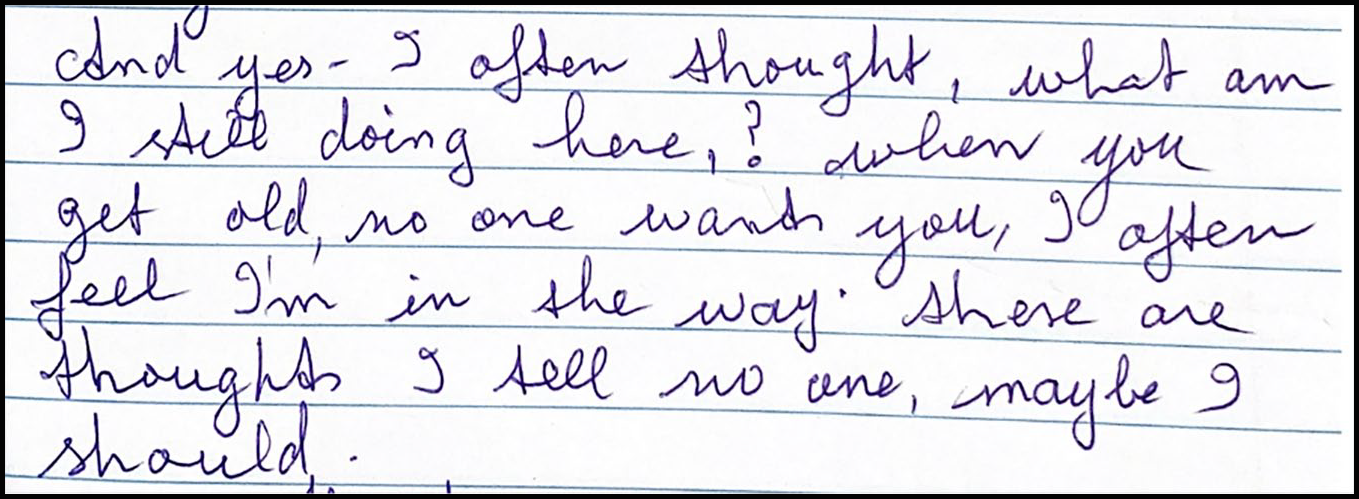
June’s diary entry.
As disclosing loneliness can imperil a desirable self-presentation, it is easier for June to allude to how her generation – and not her specifically – is ‘really done by without company’.
These examples show how management of stigma and loneliness can interweave through control (from distraction to concealment), self-presentation and impression management (Goffman, 1963). Practices of stigmatisation are perceived at the individual/micro-level, justifying the mechanisms used to manage potential stigma like suppression, but interrelate with broader structures of devaluation and power from loss of autonomy to indignity (Tyler, 2020).
Discussion
We combined the work of Goffman and Tyler through relationality and productive power to explore a theoretical approach to the stigma of loneliness in later life. This approach identified three conceptual dimensions to capture stigmatisation processes and practices: enaction, reception and management. These dimensions draw on agentic/personal and structural/social contexts of stigma, highlighting linkages between identities (Goffman, 1963), interactions and internal/external devaluation(s) (Tyler, 2020). Our findings demonstrate that such dimensions offer rich sociological frames, at both micro- and macro-level, to understand loneliness stigmatisation in later life circumstances.
For our respondents, the enaction of stigma mainly occurred at the internal level as most reported not disclosing loneliness to others. They preferred to be discreditable rather than discredited (Goffman, 1963). These internal enaction(s) are, nonetheless, justified via external social interactions, norms and values. As Goffman (1963) explains, stigmatised individuals frequently share the same social ideals as their stigmatisers – and so keeping one’s actual social identity and virtual social identity aligned is paramount to avoid identity discrepancies and social tension. We also saw how labelling, stereotypes and discrimination unfold in social interactions, through how lonely older people, such as Gurney and Lisa, are dismissed and ignored in care or work institutions. Their experiences illustrate that stigmatisation involves devaluation practices linked to wider forms of control and inequality affecting those with intersecting categorisations (Tyler, 2020) like old age and frailty. For some participants, the gender label of being an old ‘lonely woman’ (Lisa) or ‘lonely man’ (Bob) added to those devaluations. The assemblage of stigmas encountered shows that loneliness does not function in isolation, helping clarify its assumed normativity in later life and why older people seem more likely to ascribe internal attributions for loneliness (Barreto et al., 2022).
Older people – particularly those who are frail or require long-term care – are perceived as a counterpoint to idealised ‘normal’ people in Western societies (Nussbaum, 2019). The literature on disgust elucidates how ageing is often reviled because of physical decrepitude, unattractiveness, dependency and unproductiveness (Miller, 1998). Ideas that are evident in the enaction of ageism in present times (Cook et al., 2021). It is unsurprising then that our participants internalise interweaving stigmas (old, frail, lonely), concealing and masking their loneliness. As later life is seen in these devalued contexts as non-productive, the productive power of the stigma of being old, frail and lonely acquires added complexity (Tyler, 2020).
In stigma reception, we observed intricate feelings (emotional pain, shame, embarrassment, guilt) and different identities at play. Ego identity illuminated the subjective feelings of loneliness and their internalisation, whereas tensions between social and personal identities illustrated how stigma can be received. These identities interact deeply in our participants’ accounts. For instance, Audrey tries to regain her ‘independent’ identity by hiding her institutionalisation and loneliness from friends. Internalised stigma-optics (Tyler, 2020) about what it means to be lonely in later life were also evident across our studies. Bob stressed how being lonely in ‘old age’ is degraded via derogatory terms, sometimes adopted as self-descriptors: ‘parasite’, ‘invalid’, ‘unproductive’, ‘good-for-nothing’. As Goffman expounds (1963), the individual who becomes stigmatised ‘late in life . . . has thoroughly learned about the normal and the stigmatized long before he [sic] must see himself as deficient. Presumably he will have a special problem in re-identifying himself, and a special likelihood of developing disapproval of self’ (p. 42). Bob’s terms result from social optics configuring later life loneliness and its stigma through the inequalities embedded in societal ideals that over-emphasise independence, self-sufficiency, sociability, youthfulness and generational conflicts (Franklin et al., 2019; Hookway et al., 2019; Neves et al., 2024; Torbjörn & Peter, 2017). Such optics and ideals amplify social divisions by ‘pit[tting] people against each other in struggles over resources and value’ (Tyler, 2020, p. 267).
In both our studies, stigma management manifested in practices of distraction from and concealment of loneliness. Contrary to Goffman’s expectations (1963), concealment occurred in relation to family/friends, not just larger networks. Our findings further revealed that stigma management relied on self-presentation and impression management. Participants’ performance of a desired-self emerged as precarious resistance – often not to resist the ‘lonely’ label or their actual social identity as ‘lonely’, but rather to resist its public presentation and how it would reflect on their virtual identity. Stigma management was also controlled by understandings of one’s personal identity (Goffman, 1963): e.g. Audrey hid her situation from friends and suggested there were few ‘normal’ people at her facility, since most have dementia; June mentions to others she loves being on her own but told us she hates it. Those who attempted to disclose loneliness, like Gurney, saw their efforts ignored or dismissed, reinforcing the stigmatising condition of feeling lonely. External and internal dismissal of loneliness and the preferred silent suffering due to shame, blame or fear of more stigma(s) represent forms of control rooted in stigmatisation processes (Tyler, 2020). Management of loneliness stigma can, therefore, enhance enaction and reception of stigma as the experience of loneliness is hidden and suppressed, supporting the societal values and practices that stigmatise it in the first place (Link & Phelan, 2014; Tyler, 2020).
Conclusion
This article contributes a sociological lens to the stigma of loneliness in later life, offering a creative reconfiguration of existing sociological theories and addressing a gap in loneliness studies. This lens illuminates the interplay between personal and social contexts, often overlooked by dominant individualistic approaches to loneliness. It also demonstrates the relevance of combining seemingly divergent sociological perspectives (and micro- and macro-level insights) to understand loneliness and its stigma as a social system, process, practice and consequence – not merely as an individual construct or feeling. Such perspective challenges prevailing psychological models of loneliness and helps map how loneliness gets politicised in neoliberal discourses through praise of one’s resilience, positivity and proactiveness. This praise serves forms of control and inequity, augmenting stigma power (Tyler, 2020).
The dimensions of loneliness stigma analysed here provide a conceptual framework for interventions and policy too: grasping external/internal enaction, reception and management of stigma can inform more inclusive responses. Furthermore, destigmatising loneliness demands reflection on how stigma can be entrenched in programmes designed to alleviate it (Barbosa Neves et al., 2023; Scambler, 2009; Tyler & Slater, 2018). An industry creating services to tackle the so-called epidemic of loneliness that separates stigma from its sociopolitical contexts can restigmatise rather than destigmatise loneliness. Ensuring programmes do not lead to phantom acceptance of stigma (Goffman, 1963) is essential. It is similarly crucial to question who benefits from loneliness stigma in our so-called ‘networked’ society (Hookway et al., 2019; Neves et al., 2024; Tyler & Slater, 2018).
Our application of the stigma of loneliness framework focused on a particular generation, context, country and qualitative approach. We believe this theoretical lens can be applied to other age and sociocultural groups, but its applicability must be investigated. Due to its relationality, separating enaction, reception and management is not clear-cut. Likewise, the assemblage of stigmas encountered (old age, frailty, institutionalisation) can complicate the study of loneliness stigma. But, as stigma does not operate in isolation, requiring a language of relationships and power (Goffman, 1963; Tyler, 2020), this confluence of stigmas may advance our grasp of stigmatisation processes and how to contest them. We concur with Tyler (2020, p. 29) that ‘understanding the wounds of stigma as social and political injuries can assist in the forging of networks of care and solidarity’, which are vital to tackle loneliness.
Footnotes
Acknowledgements
We would like to thank all our research participants, care home staff, and local councils involved. A special word of gratitude to Monash City Council, namely to Sallenna Skye and Mary Martin. We are also grateful to Sandra Sanders for her support with this project. Additionally, we are indebted to Dr Baptiste Brossard for comments on an earlier draft. Finally, we thank the anonymous reviewers and the editor for their constructive feedback.
Funding
The research reported in this article was funded by Monash University grants awarded to the first author. The University of Melbourne also provided support to the first author through an ‘early career researcher’ award. Both authors are funded by an Australian Research Council Discovery Project entitled ‘Understanding the role of digital technologies in addressing loneliness’ (DP230101234).