
Abstract
In this article, I describe the experience of a chronic pain diagnosis. Combining memoir, medical history, and literary precedents, I begin with a reflection on my own history with walking. Walking leads to foot pain which eventually leads to diagnosis of a full-body chronic condition: fibromyalgia. Through an exploration of the history of hysteria, one of fibromyalgia’s ancestors, I consider some of the resonances between these conditions.
Keywords
But things can be over in horizontal time and just beginning in your body, I’m learning.
First steps
The good ice only formed in certain places. Never on the road or the sidewalk, but just between – that narrow gray strip dividing sidewalk from road where the rising concrete gave the ice a shape to become and cling to. We would try to run past one another in order to reach the parts that hadn’t been cracked yet. It was on gray days, when the light was flat all day long, but at its flattest just after school, and on our walks home we wouldn’t speak, just walk one winter boot in front of the next in order to hear the satisfying sound of the ice giving in. The sun was always dropping below the rooflines and all around was a silence that seemed to be waiting for our arrival, like it was waiting for us to break it up.
This was our trajectory, up this narrow strip; sometimes I led, sometimes he did. When he led, I tried to let him crack the new ice selflessly, but always I felt worried that his feet would get the last of it, or the best of it. The pleasure I felt when the pressure of my foot released that crisp snap was always followed by the possibility that there was nothing else up ahead to break.
At 16 I realized we hadn’t broken the ice in ages. We had been growing up and not noticing the weather, talking instead about important things on our walks home from school (e.g. Could Tiffany be considered a musician even though she was manufactured pop? What was the nature of authenticity in artistic practice? Which Peter Sellers movie should we watch next? . . .) and forgetting those childish games. Then one year he went off to a different school and for the first time in my life, I would trudge home without him. On one of these solo walks, made before iPods and even Walkmans were de rigueur, I noticed the ice. I heard in my memory that joyous snap. I wanted to feel that craaaaaack again, so I raised one boot on to the glassy surface, anticipating that perfect aural connection between foot and ice. But the ice was muted; its response to my pressure was dull and flat. At the time, I thought I had just misjudged the ideal spot for my foot to make contact, but of course the difference was his absence. Without him, there was no communion of silence and desire to generate such reverberations. It was an early lesson in mourning.
At 14, I owned cherry red Gloria Vanderbilt heels with alchemical properties. When I put them on, I became impenetrable, like Sigourney Weaver in Working Girl. The name – Gloria Vanderbilt – sounded so fancy. I thought she must be like Barbie, living in a mansion somewhere wearing the exact same shoes while she did grown-up things like wear glamorous dresses and make phone calls. At age 5, I was the Wicked Witch of the West for Halloween. The crowning jewel of my costume was a pair of matte black pumps. I clomped around the school fully in possession of my temporary evil. Early on, I learned that other kids mistook me for the teacher, because of the sound my shoes made in the hallway. Sneakers or little black plastic soles – it didn’t seem to matter – something about the way I walked in all those shoes sounded to them like the roundness and solidity of authority. Each footfall was deliberate, one after the other generating a rhythm on repeat. If the teacher was already in the classroom and they heard that sound, they knew it could only be me. I had liked the sound my heels made until I heard how it marked me as me. I knew immediately that it would be better not to stand out like that, so when I found myself alone in a hallway, I walked on tippy-toes.
I don’t remember the year I got my first pair of cowboy boots. I was riding horses every summer by then and at some point, these leather boots replaced the rubber ones I began with as an 8-year old. They were black with white stitching, and I rode tall in the saddle with them. I wore those boots when Snort, the 17-hand high wall-eyed horse, tried to buck me off in the middle of a pond. I was so short that I couldn’t bridle him myself, but I was strong enough to stay on and stay upright. The stacked heel kept me in the stirrup while my thighs squeezed tight. I knew Bryn – the cowboy guiding us through the mountain – was watching from the other side of the pond, so I wouldn’t let myself hold on to the horn for fear he’d lose respect. I heard him laughing so hard during the bucking, but when Snort and I made it across the water and my hands were calmly holding the reins, Bryn just looked at me and nodded. I fell in love with Snort that day, and for many years after I daydreamed about the two of us together. I imagined a life in which Snort and I just lived and rode in the mountains; it was a modified Thoreau-style existence in the woods, just as peaceful and pure as the one written about by that New England walker. I never felt as though I ‘mastered’ Snort. Rather, I tried to show Snort that I could learn his rhythms, that I understood his strength. In that slough, we established trust.
I was wearing those boots when I learned to ride bareback. I fell off and landed – hard – straight on my head. It was the 1980s and we were in the mountains, so I stood up and got back on the horse. Nobody thought about checking for concussion or calling it a day, least of all me. There was an unspoken pact among our small group of girls that we would out-ride anybody and never complain about cold or pain or fear. When we came to a part of the terrain so steep that the horses had to sit and slide down because they were afraid of the angle, we white-knuckled our way through it and laughed at the bottom.
We took to waking earlier than the rest of camp, to go and get the horses out from pasture for feeding and bring them back to their stalls ready for the day. One morning, we had a little time to kill before breakfast, and we lingered around the fencing. It was electrified. We decided to form a chain holding hands, and the one closest to the fence would touch it. We wanted to feel the current run through us. We hypothesized that it would gain in strength with each body it passed through. We took turns at the front of the chain and at the rear. We laughed to stave off the fear. Hands holding hands would jerk upwards with increasing speed and force until the current reached, or was presumed to reach, the girl at the end of the line. Her body would shudder, and she would flail her free arm about, dispensing the charge. I remember enacting those same gestures when it was my turn at the tail, but I’ll be damned if I can recall whether the charge was real or imagined. Had the electricity really affected us? Or had the first girl at the end exaggerated the sensation, and had we all privately agreed to mimic the performance of the first, not to be left out of such an experience of extremity? It has taken years for me to understand that the real and the imagined coexist and co-create all the time. When I picture that scene today, I see a group of girls convulsing and shaking like a cowgirl version of mass hysteria.
Now, I read those cowboy boots as a sign of growing up. The rubber boots were fine for trail rides, or trotting around in the ring, but these leather stitched beauties were a visible affirmation of leaving childhood behind, of being able to stay upright in the face of all sorts of rearing up and falling down. This desire to stay upright and super-charged would return, disconnected from the memory of Snort and all the other singular, beautiful beasts I loved during those summers. Those camps I’d been going to had been Christian camps. That fact had always been incidental to me, and yet somewhere along the way, I came to associate the warmth and love I felt there with a Christian God. For most of my adolescence, I was a born-again Christian. It took years before I figured out it was Blaze and Ryder and Winnie – and finally Snort – with whom I had actually established a connection. In retrospect, it’s as though someone pulled the plug out of my horse-receptor and inserted it into a new, God-shaped receptor. The story I tell at parties is that I mistook my love of horses for love of God. People laugh, and I laugh, and we move on. But it’s true. I got my wires crossed and the boots were disconnected from those beasts and from that glorious group of girls.
I was wearing those boots in high school Biology class when Dave laughed at how I walked. He never could explain what specifically was peculiar and different, but he maintained that my feet carried my body in a way that was strange and worthy of attention. I thought it might be the boots, but he said I walked weird in any old shoe. It was good-natured ribbing, but I think back on those days and wonder if he had lit on something secret going on inside my body, something that the kids in elementary school had gleaned as well. Did they all recognize something that I – and later all the doctors and physiotherapists and massage therapists and chiropractors and acupuncturists and New-Agey prophets and nutritionists and healers and naturopaths – just could not see?
In the first two years of my undergraduate degree, I walked. Sometimes hours per day. I walked either with K, or alone. More than 20 years later, I remember those walks with K as a time I unloaded despair after despair on to her, how she bore it and endeavored with so much love to relieve it. I’ve forgotten the precise nature of each anxiety, but the shape of it all was theological doubt that had been activated, that threatened to destabilize the structure of belief I had erected after the horses, and that shook me to my core. I walked in hopes of resolving my skepticism, of putting to rest once and for all that most toxic thought: doubt. The two of us, like a teenage Virgil and Dante, trudged through Ontario falls and winters seeking release, seeking answers. Somewhere in the midst of these wanderings, K’s feet began to hurt. She changed boots, more than once, but nothing helped. Her feet became enemies. They screamed at her each morning and harangued her through classes and dinnertime and even into her dreams. Her pain was unforgiving and brutal. For so long – longer than she should have – she kept walking with me.
We learned eventually that K had developed bilateral plantar fasciitis. She woke each morning with that telltale stabbing through the heels and since she had it in both feet, there was no escaping the build-up of scar tissue with each and every step. Centuries of memoirs and walking essays establish a romantic link between walking and thinking. In writings by Rousseau, Wordsworth, and Thoreau, the body disappears on a rural walk: the poet’s imagination, or glorious Reason, or transcendent Nature feature prominently while the body seemingly dematerializes. 1 In more city-based writing about walking and observation – flânerie as it came to be known – a solitary man (usually a man) drifts aimlessly through the city, noting his observations down for posterity. Marcel Proust describes his two childhood walking routes – the Méséglise and Guermantes Ways – as providing him with ‘poetic pleasure’ for contemplation of all manner of people and objects. These routes took him through both town and countryside, such that his observations extended from encounters with the gunsmith, to contemplation of a ‘neurasthenic’ water lily. 2 Page upon page of detailed ruminations about hawthorns, or the angle of the sun as it strikes the steeple at Combray, take us deep into the maze of the narrator’s memories, but we float through these memories without any sense of a body attached to them. 3 Similarly, in Virginia Woolf’s glorious Street Haunting, the writer’s observing gaze is central to the narrative; her body is not. 4 Even Rebecca Solnit, who lovingly traces an idiosyncratic history of walking, rarely describes pain during her thousands of hours on the trail. Walking is like riding a bike – once you learn how, it’s automatic and mostly unconscious. It allows you to get from A to B, or to think through a question, or to watch the passing of everyday life. It’s by turns Romantic, poetic, artistic, a form of protest against urbanism, or, simply, a means of transport. But the feet, and by extension the bodies, of these writer and artist walkers are elusive.
K became a detective of pain. She scrutinized each part of her foot in precise detail, wanting only to crack the code of which movement made it worse, which better. Could she walk on the edges of her feet, or on the balls? If she iced them morning and night, if she took anti-inflammatories, if she rested (how can you rest as a student getting to class then work then class again) – would any of this bring relief? She began cycling everywhere, even through Ontario freezing rain, to save her feet from the pressures of carrying her. I remember the first time she uttered the word ‘chronic’. I was 18 and lucky – I had no reason to understand that word. Quietly one day, she asked: what if it’s chronic? She sat on her bed; the sun poured through the window behind her and made lines on the quilt. She traced the lines and whispered the word. I could tell she’d been holding on to it for a while, that it had been weighing heavy on her. It hung in the air between us, charging the atmosphere like a black hole or an opening into a new world, unmapped and unwalked, but with a specific gravitational pull. It did not seem benign. Later, I would be more able to trace its contours, to map its terrain of uncertainty and thwarted futures. But in this moment, with the sun filling the room and the lines on K’s quilt and her fingers tracing those lines, I felt only a vague danger.
My father had also suffered from bilateral plantar fasciitis when he was training for a marathon. In high school, I had watched him return from training runs and put his feet on ice after dinner, watching the hockey game and suffering in silence. He eventually found a skilled massage therapist who ground the scar tissue out of his feet, but pain never stopped him from running. It seemed normal, to run through pain. Eventually, we convinced K to move to Calgary and live with us in the summers so that she could see this same massage therapist. And, eventually, this therapist helped K recover. Over time, we discovered that the issue wasn’t restricted to her feet; some kind of referral from a hip was to blame. 5 K’s experience was my first lesson in how the source of pain may not be identical to its site of emergence. It was a lesson I would need to learn many times before understanding how a pain signal can get garbled because a network is overloaded. But for K at that moment, the news was good: her feet weren’t chronic. She returned not only to walking, but also to hiking, to Capoeira, to all sorts of movements that demanded harmony with her feet.
As K healed, my body began talking to me. About a year earlier, I had done a number on my hip while swimming breaststroke. It had always been my strongest stroke, and I went at it that day with unbridled enthusiasm. I kicked out hard and felt something shift in my left hip. Pain was not intense or immediate – the joint just felt off. I finished my swim, walked home, and noticed over the next few months that it became harder to put weight on that leg. The day I couldn’t put my jeans on without sitting down, I arranged a physiotherapy appointment. The physio declared nothing was wrong, so I limped home. For the rest of the school year, I gritted my teeth until I could return to my hometown to find better healthcare. The first specialist diagnosed a hypermobile and extremely irritated left sacral-iliac joint. Her prescription was a long rehab process that would take months, and I should start out by walking for brief periods back and forth across the shallow end of a pool. Water, she explained, would take pressure off of my joints. I found this utterly absurd. I was not remotely interested in committing to a several months-long rehab plan; I was certain I could heal more quickly. Part of my impatience was due no doubt to being 18, but more significantly, I am a product of industrial and late modern capitalism: faster is always better. I visited my father’s massage therapist, who suggested I try a chiropractor. After one treatment with him, I felt just about normal. After one week of seeing him daily, I had no pain in my hip. This didn’t last.
Next, I started receiving messages from my feet. A stabbing through my heels each morning convinced me I had caught K’s pain through some occult form of contagious magic (Freud, 1990, p. 103). I went back for massage, I got orthotics. I learned that I pronated – a lot. Once again, bilateral plantar fasciitis was the diagnosis. Time passed. I changed all my shoes. I wore anything that could hold my orthotics: hiking boots, Doc Martens, men’s dress shoes, runners. All the shoes were ugly. Other people recover from plantar fasciitis. Almost everyone in my immediate family and many friends have had it and healed from it. But no matter what I did, I couldn’t exorcise the demons in my feet. My hip kicked up regularly too, sending twinges and punches, reminding me that it was still present and irritable. I was told that my hypermobile left hip was complemented by a hypomobile right hip, and the two of them together created a compensatory dance that was sending asymmetric pressures down to my feet. Back at school, I stopped walking and relied instead on my bicycle, that most rational of inventions. As Angela Carter, that glorious fantasist who pulled me through my undergraduate degree, writes, ‘To ride a bicycle is in itself some protection against superstitious fears, since the bicycle is the product of pure reason applied to motion’ (1993, p. 97). Reason took me places in those days, but it always left me just outside where I needed to be. I’d lock it up and then face the few remaining steps to class. Those steps had a soundtrack: I’d walk with Annie Lennox’s Walking on Broken Glass running through my head. I imagined tiny shards of glass embedded just underneath the skin of both soles. Each step dug the glass in deeper. I told people I had ‘bad feet.’ I dreaded grocery shopping.
Returning to Calgary for another summer, I narrowed my perimeter. I drove to work, to the pool, to massage and chiro, and then home. I’d sit at my desk and spend hours anticipating the agony of standing up to leave. I ruminated on feet. I watched the feet of others. I saw people pay no attention to how their feet could play tennis, rollerblade, jog or chase a soccer ball. I saw how feet kept them standing at parties and going on weekend hikes. I saw people kick their shoes off at the end of the day and walk around barefoot and oblivious. I could no longer walk without orthotics; I began to resent all the shoes I could not wear, and the feet that could: anyone in Birkenstocks; platforms; jellies; flip-flops; heels; anything without a strap or a lace; anything for sale at the mall. I envied those feet; I hated mine. I fantasized about cutting them off.
One night in 1996, I lay sleepless in bed, unable to get comfortable. It was summer in Calgary and I was home from school. I tossed from side to side. I blasted Sarah McLachlan’s Solace, trying to drown out my throbbing feet. I kicked the duvet off; I watched the clock. I sensed something distant coming closer. Something was becoming palpable, if not tangible. The CD player shut off. I looked to my feet, a knee-jerk response to anything that seemed strange or unwelcome those days. Jamming my knuckle into the fascia, I tried to discharge some pain by grinding it out. Scar tissue popped and crunched under my thumb. Following the contours with my knuckle, I tried to find the edges of it, a ritualized demarcation of good territory from bad: the place it didn’t hurt. I couldn’t find the boundary line: the map had changed. Katie Stewart describes this kind of moment as an ‘atmospheric attunement’; Lauren Berlant calls it a ‘situation.’ In Stewart’s words, it’s a ‘pause, a temporal suspension animated by the sense that something is coming into existence’ (2010, p. 446). For Berlant, a situation ‘is a state of animated and animating suspension that forces itself on consciousness, that produces a sense of the emergence of something in the present that may become an event’ (2011, p. 5). In that suspended animation of a summer evening, I came to sense that something had taken over my body and replaced it with this aching, despairing flesh. I had only been seeing my body in pieces; I had missed the moment that I became a chronic condition.
There’s a never-painted Kahlo rolling around in my head: a woman stumbles down a broken city street. The air is lousy with the smell of fermenting yeast. Flat, grey sky presses down on her; store windows are covered in grime and despair. Trash has settled into concrete depressions in the road and the woman’s brilliantly white skirts blow about, giving form to erratic and invisible gusts. Trailing from her stomach and extending in a wave behind her, a ragged, bloody umbilical cord connects with the pavement, shooting city signals back through her belly each time it strikes ground. There’s a red current of pain traveling from ground to abdomen, from woman to ground. It takes her measure; it measures the number of steps she’ll need to take before rest and how far she’s come. It calculates the hardness of the concrete with the accumulation of shocks to her system. It makes a calculus of her pain. The cord is a disinterested accountant, tracking the compounding cost of each step. If she reels the umbilical cord in towards her, she finds only the frayed ends of desire.
Tender points
In 1996, at the age of 22, I’m told I have a syndrome that can’t be cured, whose reasons for emergence are shrouded from view, and that the symptoms themselves are largely invisible and unverifiable. I’m told that this syndrome usually affects middle-aged, or older, women, and that I’m a relatively uncommon case. I’m told there’s no reason for tears (which were leaking out of my eyes by then), and that at least I have a diagnosis.
I recall two distinct actions I took following the diagnosis. First, I drove to my gym, jumped in the pool, and swam as hard and as fast as I could. As the tears erupted again and then again underwater, I dug in and swam harder. I swam to deplete myself. I swam to forget. When I was spent and felt only the exhausted endorphins shooting around my brain, I got dressed and drove home to the computer. I began to research this new word: Fibromyalgia. It didn’t take long – not much was digitized at the time – but I did find confirmation that my set of symptoms was now being recognized as a syndrome with no cure. Today, the Mayo Clinic describes fibromyalgia thus:
Fibromyalgia is a disorder characterized by widespread musculoskeletal pain accompanied by fatigue, sleep, memory and mood issues. Researchers believe that fibromyalgia amplifies painful sensations by affecting the way your brain processes pain signals. Symptoms sometimes begin after a physical trauma, surgery, infection or significant psychological stress. In other cases, symptoms gradually accumulate over time with no single triggering event. Women are more likely to develop fibromyalgia than are men. (Mayo Clinic, 2021)
That summer night in bed, I became aware that my entire body ached. I had been laser-focused on feet for so long that the rest of my body had dematerialized, like an inversion of all those writers whose feet disappeared from consciousness as they walked.
In 1996, the procedure for diagnosis was two-fold. Doctors would rule out other autoimmune conditions through blood tests, and then conduct a Tender Point test. My blood came back clean: nothing to see here, it said. Clean blood leaves me feeling simultaneously grateful and crazy because I have no proof, no alibi. It’s the second diagnostic component that renders ‘positive’ results. Tender points, first described by Scottish surgeon William Balfour in 1804 and elaborated on in more detail by F. L. Valleix in 1841, are ‘painful points in various parts of the body’ (Inanici & Yunus, 2004, p. 369). Theories of these tender points evolved over the next two centuries in relation to myriad rheumatic conditions. The first contemporary description of fibromyalgia in 1972, by Smythe, includes a description of tender points. In 1990, the initial criteria are established both for research and for clinical diagnosis: if the patient reports widespread pain, as well as tenderness from pressure applied to at least 11 of the 18 tender points, and those points are distributed both above and below the waist, and on both sides of the body, then a diagnosis of fibromyalgia could be made (Wolfe et al., 1990).
In order to illustrate the location of these special points, the authors of the 1990 criteria include an image, which stops me in my tracks. Based on Jean-Baptiste Regnault’s 1793 painting The Three Graces, the authors have altered the image to suit its new context (Figure 1).
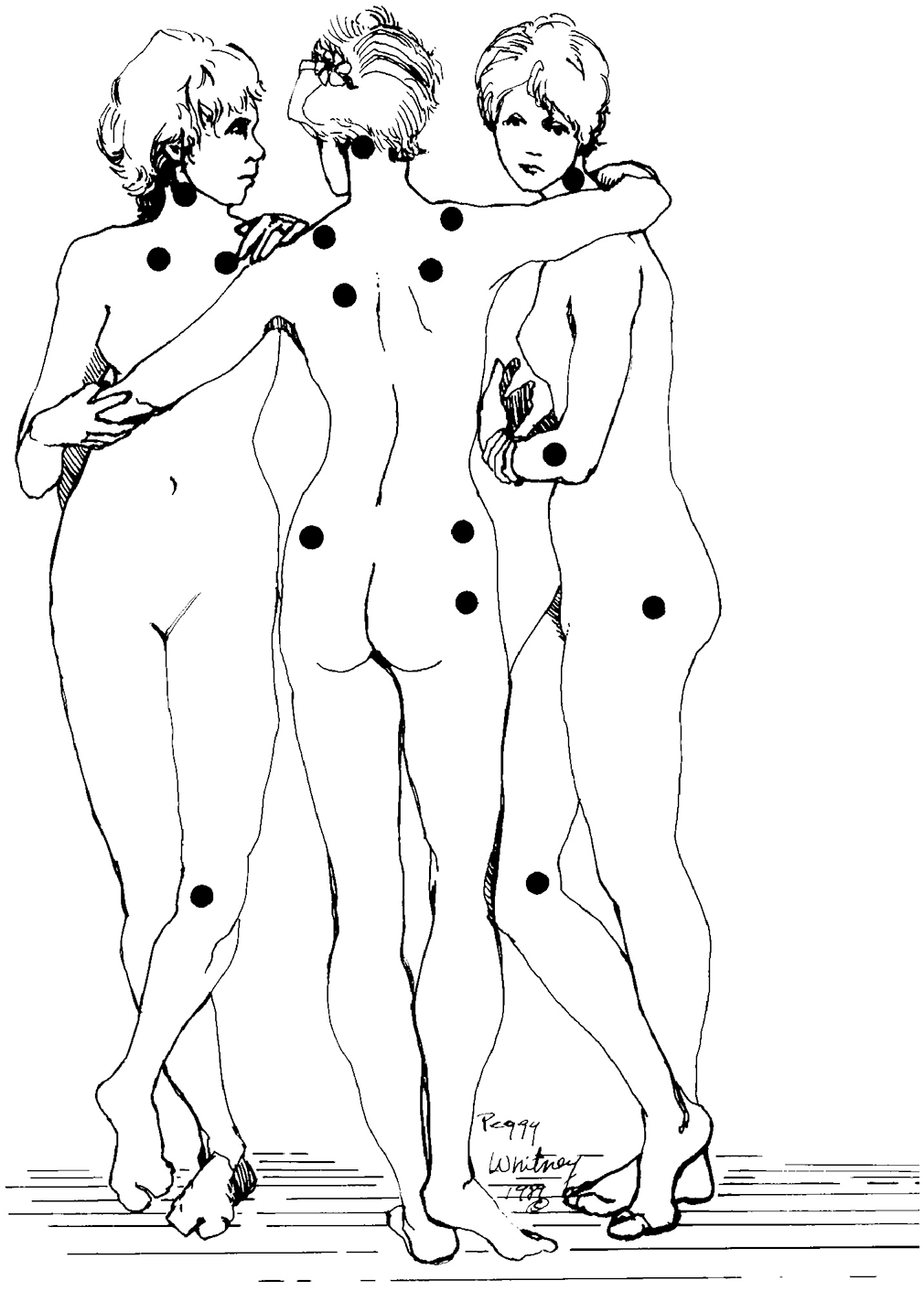
Figures representing fibromyalgia tender points. Originally printed in Wolfe et al. ‘The American college of rheumatology 1990 criteria for the classification of fibromyalgia,’ Arthritis and Rheumatology, 33(2), 160–172. https://onlinelibrary.wiley.com/doi/10.1002/art.1780330203 Reproduced with permission from John Wiley and Sons.
Alternately transfixed and bemused by the presence of this threesome in this context, I was compelled to look again at the original from which this drawing was made. Their hair-dos have been modified and their voluptuousness curtailed, but that figure on the right still gazes straight out at the viewer, and the neo-classical nude form is retained, if abstracted. In Regnault’s precise style, the Three Graces with arms linked together (Figure 2) can also be viewed symbolically as a single figure depicted from three different angles, and this may be one reason the authors chose the image. In the medical version, the nymphs’ positioning enables the authors to depict all 18 tender points, pictured here as black orbs, in a single frame. I find myself obsessively counting the points, coming up short, and starting again. I explore their figures, hunting only for this one specific marker: the correct number of black points. The process interpellates me into a clinical gaze: I ignore everything but those dots, those imaginary signifiers for an illness with no signified. It’s a compulsive calculus: the Graces have been reduced from 3 to 1, and the 1 has been split into 3. While her/their pains have multiplied, I keep count. When I reach 18, I seek to verify and start again, like a good empiricist. Sometimes I find 17, sometimes only 15. I start the count again, like a doubting Thomas. I am looking at this drawing for reassurance, for concrete certainty that my pains match up to this map, and thus achieve a certain existence beyond my own perceptions. But somewhere between the image and my brain, the points flicker in and out of my field of vision; I lose faith in the entire enterprise.

Jean-Baptiste Regnault (1754–1829). The Three Graces. [Oil on canvas]. Musée de Louvre, Paris, France. Reproduced with permission from © RMN-Grand Palais/Art Resource, NY.
The Three Graces, or Charities, come to us from Greek mythology. They are sisters, daughters of Zeus and Hera, named Euphrosyne, Thalia, and Aglaia. Together they signify ‘charm, grace, and beauty’; they are eternally beautiful and eternally young (Cartwright, 2016). Artists have drawn inspiration from these classical sisters for millennia, from Botticelli’s Primavera to Kehinde Wiley’s Three Graces (2005) and Yinka Shonibare’s headless Three Graces (2001). In Regnault’s neo-classical version, conventions of idealized representation are on full display, their effortless contrapposto emphasizes a sense of ease and a dynamic liveness. Maybe the article authors are art lovers, maybe they admired Da Vinci’s anatomical drawings or paintings of operating theaters and vivisections. For whatever reason, they borrow Regnault’s Graces and install them into a situation of chronic pain. Charm, beauty, and creativity are made to occupy a black and white world entirely abstracted from their joyful existence. Those opaque blots start to look like bullet holes on a shooting target, and I search for any indication that their bodies have been impacted, but these tender points seem not to have affected them: there is no grimacing, no subtle lean from one foot to the other, no cradling of a bad shoulder. Even the figure on the right, who gazes out so mysteriously in the Regnault, seems utterly impervious to these holey impressions. These three beauties are now eternally youthful and eternally in pain, but you’d never know it from looking at them.
Walking after diagnosis
Diagnosis kicks off a new set of relations to the medical and para-medical establishments, and a new kind of research that much later I will come to identify as analogous to the religious seeker. In the immediate aftermath of diagnosis, I learn that fibromyalgia requires a specific approach to bodily discipline: routine sleep and waking times, careful attention to diet, and the correct amount of exercise. Exercise must be consistent, but not too intense. If I overdo a workout, I will pay for days. If I fail to maintain a baseline level of activity, I will ache like I’m 90. High-impact exercise is verboten, but cardio is important. I begin with walking. I find the courage to do this from my father. This marathon man gathers me into the car every night after dinner, drives us 30 seconds down the hill to a short, flat stretch of road, and we walk for 10 minutes. 5 minutes out, 5 minutes back in ugly running shoes taking their time. Once a day, 10 minutes silence. 18 points. My feet, still in agony, begin to trust the security of 5-minute arcs and 10-minute loops.
Hysterical echoes
Unless it’s accompanied by an external signal like blood or a broken limb, pain does not present itself to outsiders. Chronic pain is often invisible: to be in pain like this is to be split between the howling immediacy of an interior state and the necessity of getting along in the world. I might wake up with a hammer in my hip. As the day progresses, I could find a knife in my heel or witness the spread of a dull, diffuse ache in my legs and shoulders. I will smile at you on the street while my feet weep in their shoes. I think of my body like a crime scene – I look for clues that might point me to reasons, or even a culprit. If I could find a reason, I think, then I could find a way to change it. Some days I wake up and can’t move my neck. It might last for days. So far as I can tell, there is no reason for any of this; it just comes and goes.
The medical literature describes this particular pain experience as nomadic: ‘the pain may move – a process called the migratory phenomenon – from one part of the body to another over time’ (Mayo Clinic, n.d.). For anyone familiar with the history of psychoanalysis – and the broad history of hysteria in the West – the reverberation between fibromyalgia’s description and this most ‘protean’ of illnesses is palpable: migratory pain; tender points; the uncertain role of trauma; and symptoms without obvious causation. . . each of these elements show up in the medical literature on hysteria and neurasthenia. 6 Had I been born 20 years earlier, I may have been diagnosed as having fibrositis, or as being just another hysterical woman in need of Valium; 100 years earlier – malingerer or drug abuser; 150 years earlier – hysteric or neurasthenic; early modern period – witch.
The tender points described by Smythe in his 1972 discussion of fibrositis (an earlier term designating FMS) coincide uncannily with what Charcot called ‘hysterogenic zones,’ discrete areas on the body that Charcot asserted could elicit pain under palpation. The clinician can either stimulate or arrest an hysterical attack by applying pressure to these zones. 7 In a 2015 issue of the journal Neurology, three physicians re-publish the fibromyalgic Three Graces in order to compare it to a nineteenth-century illustration of hysterogenic zones from Charcot’s case histories. The location of these points, they exclaim, overlaps perfectly (Teive et al., 2015). 8 They make a composite image by way of illustration (Figure 3), and I find myself, once again, getting lost in all these dots.
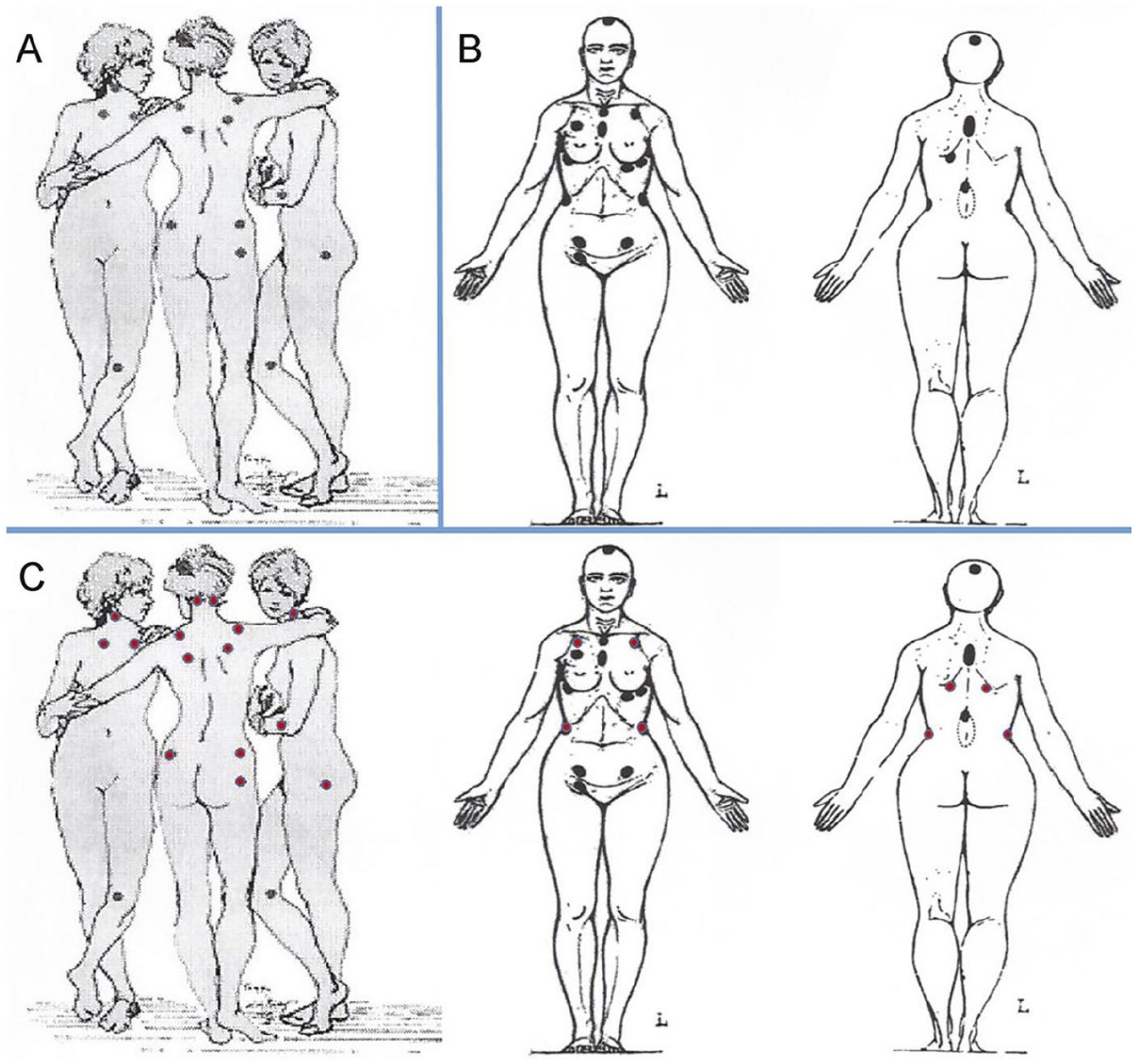
Overlap between fibromyalgia tender points and Charcot’s hysterical zones. Reprinted with permission from Teive et al., ‘Overlap between fibromyalgia tender points and Charcot’s hysterical zones,’ Neurology, 84(20), 2096–2097. https://n.neurology.org/content/84/20/2096 Reproduced with permission from Wolters Kluwer Health, Inc.
I notice how different the bodies are in this comparative figure. Regnault’s Graces exude a breezy, feminine sensuality in contrast to Charcot’s hysteric with her blocky, wide-hipped and bald body. She reminds me of medico-scientific photography of the period, in which medical subjects, colonized and enslaved peoples, and criminals, were all framed using this pseudo-scientific, matter-of-fact frontal view. Regnault’s beauties, who are primarily interacting with each other, seem as though they have just arrived in this intimate circle. I imagine them walking from disparate points in a secret garden to meet each other – the contrapposto of the central figure suggests they have all stopped, mid-step. They step gaily, without worry, without guile. Charcot’s hysteric, by contrast, is rooted and stationary. I can’t imagine her walking anywhere, ever. While the Graces seem not to even notice their tenderness, the outstretched arms of Charcot’s hysteric call attention to her hysterogenic zones. The longer I look, the more she reminds me of paintings of St. Francis of Assisi with arms extended, displaying his stigmata. St. Francis had five miraculous wounds to echo the ones Christ received from the crucifixion. I count 17 on Charcot’s figure, and those points over her pelvic zone resist Charcot’s rejection of gynecological etiology: in women with ovarialgia, hysterogenic zones over their ovaries, Charcot would press on these points to arrest an hysterical attack. 9 When I press on my ovary points, nothing happens.
Charcot’s attention to this part of the female body was not random. The word hysteria derives from hyster, Greek for uterus. For the Ancient Greeks, nomadic uteruses were the sensible explanation for migratory pain. The wandering womb was believed to travel around the body, particularly affecting respiratory health and causing an impressive range of other symptoms. The Greeks seem not to have used the word hysteria to designate a recognized disease, but they certainly referred to an erratic womb kicking up all kinds of trouble inside women’s bodies.
10
As one Hippocratic text states: ‘the womb is the origin of all diseases’ in a woman (King, 1993, pp. 12–13). Symptoms vary depending on whether the womb is deemed to be lacking in essential moisture, or suffering from an excess of heat. In one case history, for instance, the womb of a woman lacking moisture:
. . . ‘throws itself’ on the liver because this organ is full of moisture. This causes sudden pnix, by interrupting the route of the breath through the belly. During this pnix, the whites of the eyes are turned up, the woman is cold, and her complexion is livid; she grinds her teeth and has excess saliva. . . . If the womb stays on the liver or in the area of the hypochondria for a long time, however, the sufferer will be choked; if it moves to the mouth of the bladder, it will cause strangury; or it may go to the limbs or side. (King, 1993, p. 19)
However absurd this description sounds to twenty-first-century ears, what emerges most forcefully for me in these case histories is two-fold: (1) the writers’ assumptions that all these strange symptoms have a physical, or organic, cause: the womb moves around in search of better conditions; and (2) that men’s bodies are the silent standards against which women’s bodies are measured (as being too wet; too dry; too hot; too cold, etc.). As King eloquently concludes her history, which begins with Hippocrates but wends its way to the early modern period, ‘the message remains the same: women are sick, and men write their bodies’ (1993, p. 8).
It was the nineteenth-century translators of the Hippocratic texts that generated the myth of a recognized and unchanging disease called hysteria extending from Egyptian times to modern days (King, 1993, p. 8). Charcot’s rejection of the uterus as the etiology of hysteria distinguishes him both from two millennia of medical writing, as well as from the majority of his contemporaries. 11 In his view, hysterical symptoms of all sorts were believed to result from an over-excitation of nerves. Even more significant: Charcot insisted that male hysteria not only existed, he provided over 60 case histories of men he diagnosed as hysteric at the Salpetrière. Despite this neurological approach to etiology, the symptomatology Charcot describes subscribes to recognizable gender divisions of the time: female hysterics were discussed in terms of their emotional/mental states, while male hysterics tended to be described in terms of their observable physical symptoms. 12 In Charcot’s visualization of hysteria through photography, female patients played the starring roles and commandeered the visual imagination. 13 And, though wombs seem to disappear, ovaries emerge as significant hysterogenic points in women and in some men! 14 Despite the significance of Charcot’s insistent broadening of the category of the hysteric, women were understood to be more prone, at a factor of 1:20, and they were believed to be the parental transmitters of the disease (Micale, 1990, p. 406). 15 In any discussion of hysteria, it remains important to state that this was a disease attached not just to femininity, but errant femininity. 16 Charcot’s illustration, with those points on the hysteric’s ovaries, reflects the staying power of the idea of the errant womb, despite his rejection of hysteria as gynecologically induced.
So too have stigmata been tangled up with hysteria’s long history. Conventionally, stigmata signify the wounds of Christ and affirm the religious purity and fealty of the supplicant. St. Francis of Assisi was the first to claim them in 1224, and centuries since have witnessed hundreds of such declarations, many of which allege only one or two wounds. Others claim scratches on their foreheads as imitations of Christ’s crown of thorns (Dash, 2011). For believers, they commemorate the pain of the crucifixion, but also God’s blessing and the mark of faith. Like hysteria, they beggar belief: evidence for the reality of genuine God-given stigmata is ‘sketchy at best’ (Dash, 2011). Some cases have been attributed to fraud, others to psychological conditions like ‘low self-esteem’ or a ‘tendency toward self-mutilation’ (Dash, 2011). In several instances, people have confessed after the fact to self-inflicted wounds rather than divine damage. Contemporary analyses of the veracity of these claims are steeped in the medicalization of religious experience. During the early modern period, the bleed between medical and religious discourses ran both ways. Physicians of the time referred to hysterical symptoms as stigmata, steeped as they were in a demonological model and a cultural belief in witches. 17 Most stigmatics have been women, and most hysterics during this early modern period were also women. 18 As Micale traces in his history of the illness, early modern physicians saw female hysterics ‘alternately as a victim of bewitchment to be pitied and the devil’s soul mate to be despised’ (Micale, 1995, p. 20). The physical manifestations of hysteria, its ‘anaesthesias, mutisms, and convulsions’ were deemed ‘stigmata diaboli, or marks of the devil’ (Micale, 1995, p. 20). 19 In Charcot’s nineteenth-century analysis, Greek wombs recede and early modern witches morph into modern hysterics with sensory stigmata. Their bodies are the surface on which the language of ecstasy and unchecked passions is reinscribed into yet another configuration of female fragility. 20
I dwell on this history to emphasize the accretion and erasure of meanings over the years; to highlight how the discourse of a stable disease entity emerges from centuries of manuscripts travelling between ‘East’ and ‘West’ and of being translated again and then again. 21 Through all these twists and turns, the organically caused ‘suffocation of the womb’ gets hooked up to demonology, to excitable nerves, to the emergence of psychoanalysis and the idea of repressed memory, and to women whose complaints are ‘all in their heads.’ It gets funneled through feminist histories, where it comes to stand for women’s silencing under patriarchy, or women’s responses to their subjection, and it becomes an adjective to describe troublesome female patients. It appears in adjectival form in twentieth-century medical discussions of a syndrome that comes to be known as fibromyalgia.
Hysteria is not identical to fibromyalgia, but their points of contact, those tender points of overlap, superimpose wandering wombs and devil-marked witches with malingerers and nervous-nellies. The chronic pains of fibromyalgia patients, widely dismissed until recently as self-generated and psychosomatic, are sensory stigmata: symptoms for which no organic cause can be identified. I had all 18 tender points when evaluated in 1996. My bullet holes; my stigmata; my fraudulent body. But also: my constellation. Now, 25 years after diagnosis, I think of Walter Benjamin’s conception of ideas as constellations. Distant lights in the sky become meaningful as we link them together into patterns, and from patterns into stories. After gazing at these black stars on Regnault’s Graces and Charcot’s hysteric, I feel my tender points, finally, as a constellation of black holes whose gravitational pull has dragged me into the density of storytelling.
Thirty years after Biology, I roll over in bed and try to avoid brushing against the shins that shy away from touch, or the hip that has hollowed itself out from decades of sorrow. I work my way up to a careful sitting position, slip my feet into a pair of thick-soled electric pink running shoes and wonder how it will feel when I stand. Chronic pain, for me, is a structure of anticipation. I keep the laces loose, so I can slip them on and off easily enough, and I shlump around the house. My pink albatross is the only external sign of a nervous system lit up like Vegas. The genealogy from Wicked Witch pump to pink runner can’t be traced with a straight line. At 45, I walk through university hallways in squeaking winter boots – well-made, sensible Sorels that accept my orthotics – and colleagues joke they always know I’m coming.
Footnotes
Acknowledgements
Titles are my nemesis. I must acknowledge that numerous suggestions for titles of this piece were made by Patrick, my first and most important reader. I chose none of his suggestions, but wish to note them here, for posterity. First, and most compelling: heel turn (he explained this is a wrestling term, designating when a good character turns evil); anklesaurus; foot-bedridden; and another pun with the word ‘sole’ but I’ve since forgotten the exact invention. This note serves as a reminder to write things down as soon as they happen.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.