
Abstract
With this article we present European Union (EU) and non-EU nurses’ lived experiences of feeling ‘unwelcomed’ and ‘unsettled’ in a heightened xenophobic environment, in the workplace and elsewhere, following the 2016 EU Referendum. Brexit has exposed long-standing structural inequalities which oppress and disempower the NHS migrant labour force. Migrant nurses, a highly mobile and skilled workforce, were feeling increasingly disenfranchised and insecure in their employment. Drawing on notions such as tolerated citizenship and the contested political boundaries of belonging, and taking a situated intersectionality approach, we examine everyday bordering practices in the UK where the cultivation of a hostile environment is becoming increasingly prevalent. We contribute to the debates on forms of othering in post-Brexit Britain and question the instrumentality of policy interventions, closely connected to the ‘dangerous politics of immigration control’, which have far-reaching implications for long-term settlement of migrant nurses and other healthcare migrant workers.
Keywords
Introduction: Disruptions to migrant NHS nurse recruitment and retention post-2016 EU Referendum
Brexit signifies a ‘revival’ of cultural politics, a ‘heredity redux’, with its racial nationalism rehashing old arguments over benefits exclusively open to white, ‘legitimate’ British citizens (Fitzgerald et al., 2020, p. 1165). Moreover, Brexit has also sought to privilege Englishness: with its right-wing populist campaigns evoking ‘nostalgia for empire’; a silencing over racism in the British empire; and with the overwhelming percentage of pro-Brexit voters residing in England (Virdee & McGeever, 2018). It is in this xenophobic climate that we seek to examine the positioning of migrant EU and non-EU National Health Service (NHS) nurses in post-Brexit Britain, alongside connotations of ‘tolerated’ citizens and the impact of bordering practices in everyday life (Anderson, 2013; Cassidy et al., 2018a, 2018b). The NHS provides an illustrative example of anxieties over British citizenship and access to resources, as it featured so prominently in the Brexit campaigns and has featured frequently in moral panics over exploitation from those deemed outsiders (Fitzgerald et al., 2020). In this revival of Englishness post-Brexit and inherent nostalgia for Empire, the NHS continues to function as an ‘imperially-resourced service’, relying on colonial nurses to meet its staffing needs, evident in the current NHS recruitment drives. The volatility of immigration policies and their effects on NHS recruitment allow for an in-depth exploration of the inherent contradictions in post-Brexit Britain immigration policies – over-reliant on EU/EEA (European Economic Area) and overseas nurses but creating an unwelcoming, ‘hostile’ environment towards migrants.
From 2016 to 2018, the mass media reported extensively on the dwindling numbers of EU nurses working for the NHS as a direct result of the Leave result. Reports such as ‘NHS “haemorrhaging” nurses as 33,000 leave each year’ (Triggle, 2018), or ‘Brexit blamed as record number of EU nurses give up on Britain’ (Campbell, 2018), accentuated ongoing fears over nurse labour shortages. The outward mobility of EU NHS nurses and the decreased interest of new EU nurses joining the NHS have been attributed to factors such as: uncertainty connected to the position of EU citizens post-Brexit (Nursing and Midwifery Council [NMC], 2018); increased incidents of xenophobia and racism (Johnson, 2016; Quinn, 2019); and changes to the NMC regulations, mainly the introduction of English language requirements for EU nurses by the NMC in 2017, already in place for non-EU nurses (Lintern, 2017; NMC, 2019). Thus the period of July 2016 to April 2017 saw a dramatic fall in the number of EU nurses registering with the NMC, a 96% drop, from 1304 to 46 (Siddique, 2017). Shortages of nursing staff were compounded further by more than 4000 EU NHS nurses choosing to leave the UK between October 2016 and September 2017 (Matthews-King, 2017). Spanish NHS staff were the most affected by Brexit, with a 19% decrease in numbers – from 7240 to 5580 – since 2016 (Baker, 2020).
In dealing with this crisis of nursing staff shortages, the NHS has sought to recruit from outside Europe. NMC (2019) figures showed a 126% increase in new international nurse and midwife registrants, from 2720 in April 2018 to 6157 in March 2019, mostly from the Philippines and India. This latest push to recruit internationally is further compounded by ongoing challenges to recruiting ‘homegrown’ nurses (Rafferty, 2018), such as retirement and work-related stress (NMC, 2019), and cuts to bursaries for nursing students, announced in 2016 (Johnston, 2016).
Policy responses to the growing nursing staff shortage and pressures to recruit internationally, however, remain ‘knee-jerk’: short-term reactions fuelled by political propaganda (Spiliopoulos, 2021), with the added complications of rising xenophobia and double standards towards ‘wanted’ and ‘unwanted’ migrant healthcare labour. Recent phenomena, such as the 2019 election campaign, where all political parties’ manifestos placed much emphasis on tackling nurse shortages (Campbell & O’Carroll, 2019), and the ‘clap for carers’ social movement during the height of the Covid-19 pandemic (Addley, 2020), come into sharp contrast with policies towards immigrant healthcare workers, such as the 2015 Immigrant Health Surcharge (IHS) for overseas healthcare staff (Marsh & Grant, 2020). Immigrants have been labelled as ‘health tourists’, abusing NHS services without contributing through taxation (Campbell & O’Carroll, 2019). This xenophobic rhetoric led to the introduction of the 2014 Immigration Act, which stipulated migrants using NHS services would need to have Indefinite Leave to Remain (ILR) (Vickers, 2019) or, since 2017, pay £400 per year (Campbell & O’Carroll, 2019), otherwise their visa would automatically be refused (Vickers, 2019). The impact of such measures is detrimental to the health and wellbeing of UK migrants whose data were shared with the Home Office in 2016 without their consent and has led to those in need not seeking medical healthcare in fear of visa implications. The 2018 Windrush scandal led to unlawful detentions, deportations or denial of citizenship rights, such as accessing NHS services, and subsequent loss of lives of the Windrush generation members (Vickers, 2019). The ‘hostile environment’ measures, introduced in 2012 by the Home Secretary at the time, Theresa May, portraying a tougher stance towards illegal migrants, added to the rising xenophobic sentiment, and have serious implications in normalising discrimination and divisions based on race, class, ethnicity and other signifiers of perceived difference (Yuval-Davis et al., 2018).
In one of the most recent examples of the contradictions inherent in the UK immigration policies and their detrimental effect on migrant healthcare staff, in the lead up to the 2019 elections, the Conservative Party announced an increase of the IHS to £625 per person. This move was criticized by the Royal College of Nursing (RCN) as ‘immoral’ (Campbell & O’Carroll, 2019). Under much pressure, the government announced in May 2020 that it would scrap the IHS for health and social care staff (Bodell, 2020). With the introduction of the new ‘Health and Care Worker Visa’, non-EU migrants who are deemed eligible, and their dependants, are exempt from paying the IHS, alongside EU migrants who reside in the UK through the EU Settlement Scheme (Gov.uk, n.d.).
This article focuses on the othering and subsequent disenfranchisement of EU (from Spain, Italy and Greece) and non-EU (from the Philippines) nurses, working for the NHS in England, in this turbulent period of ‘EU Exit’ negotiations. We seek to capture the effects of Brexit on the EU nurses who were still employed by the NHS in 2019, to explore any added challenges and also factors which could mitigate their outward mobility. Importantly, we also seek to explore the effects of EU nurses’ departure on non-EU nurses, in terms of additional workloads and their own experiences of increased xenophobia and discrimination. We locate discrimination and increased othering practices based on social divisions and normative expectations of belonging (Anderson, 2013; Anthias, 2013; Virdee & McGeever, 2018; Yuval-Davis, 2011) intersecting in ‘critical locations’ (Acker, 2006), and creating advantages and disadvantages for the migrant nurses of our study, who were experiencing a form of ‘tolerated citizenship’ (Anderson, 2013). We take a situated intersectionality approach (Cassidy et al., 2018a, 2018b; Yuval-Davis et al., 2018), including the experiences of migrants, EU and non-EU nurses, and non-migrant NHS nursing managers. The NHS, as an emblematic British institution, is an important ‘site in which racial and ethnic inclusion and British diversity [are] . . . recognized and portrayed, . . . often regarded as embodying core national values . . . [and] imbued with meaning in and for British culture’ (Bivins, 2017, p. 87). Crucially for this study, it is a ‘“typically British” institution (in a restrictive white sense rather than an inclusive sense)’ (Simpson et al., 2010, p. 392).
Our article is divided into the following sections: a historical overview of the unequal positioning of international nurses in the NHS, and in particular post-Brexit; methodology; bordering practices impacting on the migrant nurses’ everyday lives and their long-term stay; and finally, concluding remarks on ‘new’ forms of othering and policy implications.
The NHS as a site of contradictions: The unequal position of migrant nurses
The NHS employs over 200 nationalities, with one in eight workers being non-British (King’s Fund, 2019). The history of nurse migration, however, shows the volatility of immigration policies in Britain (Buchan, 2004, 2009; Buchan et al., 2019; Deeming, 2004; Spiliopoulos, 2021; Vickers, 2019). While the NHS has been dependent on international recruitment of nursing staff since its foundation, it has been ‘slow’ in recognizing their contributions (Bloch et al., 2013; Kramer, 2006), with such lack of recognition being termed as ‘collective amnesia’ (Simpson et al., 2010). Moreover, the intersection of social divisions such as gender, class, race and ethnicity, which have affected migrant nurses’ unequal positioning in the UK (Adhikari & Melia, 2015; Allan et al., 2004, 2009; Bloch et al., 2013; Ryan, 2007; Solano & Rafferty, 2007), is evident throughout the history of NHS nurse recruitment.
Overseas nurse recruitment has a deeply entrenched ‘imperialist’ history, with colonial nurses recruited to fill the gaps in health service provision but expected to return to the colonies after their training, while holding lower status positions in comparison to their British counterparts. The presence of colonial nurses sparked xenophobic reactions, for example, in the Nursing Times in 1960 (Solano & Rafferty, 2007), at a time when Britain was grappling with anxieties over national identity, and racial and ethnic diversity within its shores (Solomos, 2003).
Such imperialist practices are evident in the history of Caribbean and Irish nurses joining the NHS. Caribbean nurses were recruited by the NHS from 1949. Between the early 1950s and late 1960s, the number of Caribbean NHS nurses rose from 3000 to nearly 6500. However, they faced bias from senior staff; limited social mobility in comparison to their white British counterparts; insufficient training; and discrimination in and outside hospitals (Kramer, 2006). Irish nurses have been employed by the NHS since the 1940s (Ryan, 2007), however the practice of recruiting Irish nurses was already established, with Britain relying on a much-needed supply of trainee and trained Irish nurses during World War II and throughout the post-war period (Ryan, 2008). By the 1970s the number of Irish-born nurses in the UK was over 30,000, accounting for 12% of all nursing staff (Daniels, 1993, in Ryan, 2007). Irish nurses, predominantly white, in Britain ‘occupy an ambiguous position as white, European insiders, but cultural outsiders’ (Ryan, 2007, p. 416). Accounts of othering practices towards Irish nurses in the UK (Hickman & Ryan, 2020), termed as the ‘racialization of Irish’ (Walters, 2001, in Ryan, 2007, p. 421), provide important insights in how the intersection of divisions such as ethnicity, race, gender and class in particular time and place contexts can demarcate contested political boundaries of belonging (Yuval-Davis, 2011).
With previous attempts at recruiting ‘home-grown’ nurses largely failing, recruitment drives have targeted nurses from former British colonies, such as Zambia, Zimbabwe and Kenya. Black African nurses have been disadvantaged, subjected to racism, discrimination, downward social mobility and deskilling (Likupe, 2013; McGregor, 2007; Thondhlana et al., 2016). Criticisms over a ‘brain drain’ of nurses from developing countries led to the introduction of the 2001 ‘Code of Practice’. Adherence to the ‘Code of Practice’ has been problematic, however, as private recruitment agencies were encouraged to join but the ‘Code’ was not enforced, and it did not include penalties (Deeming, 2004). As a result of introducing the 2001 Code on ethnical recruitment, pre-existing agreements with the Philippines and India were seen as crucial in providing overseas nurses (Solano & Rafferty, 2007). Additionally, the 2004 EU enlargement facilitated EU nurse recruitment, with mostly Polish nurses entering the UK for employment in the health and social care sector (Deeming, 2004; Jayaweera, 2015). The Eurozone crisis subsequently brought even larger numbers of EU nurses to the UK, particularly from Southern Europe. From September 2010 to September 2017, the number of EU NHS nurses increased from 7895 to 21,237, with the number of nurses from Greece, Italy and Spain increasing 10-fold in this period (NHS Digital, 2018).
Since the 2016 EU Referendum result, NHS Trusts have recruited primarily from outside the EU (NMC, 2019), principally the Philippines and India (Baker, 2020), a practice confirmed by the NHS nursing managers interviewed in June 2019. More recent statistics have shown that: the number of non-EEA NHS nurses has risen, from 67,345 in March 2017 to 92,260 in March 2021; and that the top five countries that NHS nurses come from outside the EEA were trained in the Philippines, India, Nigeria, South Africa and Zimbabwe (NMC, 2021). The NHS therefore continues to embrace ‘imperialist’ practices, and to play a key role in current fears and anxieties over citizenship and belonging (Fitzgerald et al., 2020). This clearly has consequences for migrant NHS nurses.
(Dis)advantage as defined by imperialism and increased bordering practices: The ‘tolerated’ citizen in post-Brexit Britain
The long history of unequal positioning for migrant nurses working for the NHS invites an interrogation of structural factors which create ‘inequality regimes’. For Acker (2006, p. 441) it is these ‘interlocked practices and processes . . . result[ing] in continuous inequalities’ within ‘critical locations’ which create differential positionings based on social divisions. Embedded hierarchical systems in workplace environments, ‘usually gendered and racialized, especially at the top’ (p. 445), allow thus for differential access to: resources, promotion opportunities, pay, influence in decision-making and security. These disparities are configured around gender, class, race, ethnicity and other social divisions.
For Yuval-Davis (2006, p. 195), although social divisions intersect and have a relational character, nevertheless, they have their own ‘ontological basis’. Such divisions cannot be ‘essentialize[d]’, which could then lead to the ascribing of hierarchical, normative positionings and the subsequent marginalization of those not belonging to such groupings. Social categories create advantageous and disadvantageous belongings which can change, shift and reconfigure positionalities (Yuval-Davis, 2011). Whilst belonging is construed as an emotional attachment to a safe place, through ‘selective’ processes of ‘identifications and emotional attachments’ (p. 13), the politics of belonging encompass the exercise of hegemonic power which delineates boundaries of belonging, of citizenship and entitlements (Yuval-Davis, 2011). Moreover, by taking a ‘situated intersectional’ approach (Cassidy et al., 2018a), we include in the study both EU and non-EU nurses, and NHS nursing managers, thus ‘avoiding homogenising members of collectivities’ (Yuval-Davis et al., 2018, p. 232), and offering a more nuanced account of the effects of Brexit on NHS nurses.
An assimilationist stance towards immigration has manifested throughout the recent history of post-colonial Britain (Anthias, 2013; Solomos, 2003; Spiliopoulos, 2021; Yuval-Davis, 2011). Increasing ‘bordering’ practices in post-Brexit Britain point towards place and time contexts which shape social ordering and allow for contradictory inclusions and exclusions. ‘Borderings’ are practices and processes ‘situated and constituted in the specificity of political negotiations as well as the everyday life performance of them’ and reflect ‘specific political projects of belonging. . . . Their contestations are closely related to different constructions of identity, belonging and citizenship’ (Yuval-Davis et al., 2018, p. 230). Borders are no longer exclusively external but have internal qualities. They control who can mobilize and where, create social hierarchies, and are shifted to a multiplicity of actors (Cassidy et al., 2018a, 2018b). The NHS figures as a prime example of such an institution which creates distinctions between legitimate and illegitimate patients and employees.
Anthias (2013) points towards the dangers of British politics framing multiculturalism, diversity and integration within economic parameters, favouring diversity on an individual level but viewing belonging to diverse groupings as less favourable, or even endangering social cohesion. It is within these parameters of tolerated diversity or, ‘tolerated citizenship’ (Anderson, 2013), that ‘others’ are constructed as ‘desirable and undesirable persons and groupings’ due to lifestyles and cultures seen as ‘incompatible or undesirable within Western societies’ (Anthias, 2013, p. 330). We take the position shared by Yuval-Davis (2011, p. 48), that citizenship is an embodied experience dependent on social divisions which ascribe differential access to resources and privileges, at the same time ‘de-homogeniz[ing] the notion of citizenship’.
Anderson (2013, p. 2) warns against such ‘dangerous politics of immigration control’, which place imaginary ‘borders between citizen and migrant, between us and them’, projecting these imaginary borders as ‘stable’ and thus uncontested. The exclusion of those ‘others’ purposefully cements privilege and hierarchical positions. Such belonging to a ‘community of value’ is thus framed within normative parameters of national identity and British values, ‘good’ citizens being ‘hard-working’, ‘law-abiding’, ‘rational, self-owning, and independent, with a moral compass that enables him [sic] to consider the interests of others’ (Anderson, 2013, p. 3). Migrants therefore occupy the position of ‘non-citizen’, deemed outsiders. For Anderson (2013), exclusion is manifested in the public rhetoric of who belongs and who does not belong, not only in terms of race, of being non-white, but also the right kind of ‘white’. We now turn to how we studied these phenomena.
Interrogating bordering and othering practices: Methodological approaches
Interviews with 11 NHS nurses, in the Midlands and Southwest of England, and with four senior NHS managers were conducted between January and June 2019. A snowballing technique was used to find respondents. Including respondents from two NHS Trusts was advantageous, as it allowed us to make some comparisons in terms of support offered to the migrant nurses and their positioning in their respective communities. Our study was conducted in accordance with ethical procedures, including preserving participant anonymity, participant consent and the storage of data according to data protection laws. Ethical approval was obtained by the Universities of Nottingham UK and Nottingham Ningbo China.
Demographics of the migrant nurses interviewed are shown in Table 1. We recruited nurses with less than five years’ NHS experience to gain an understanding of their career trajectories and their interest in investing long-term in a career in the NHS.
Participant demographics (information accurate at the time of data collection).
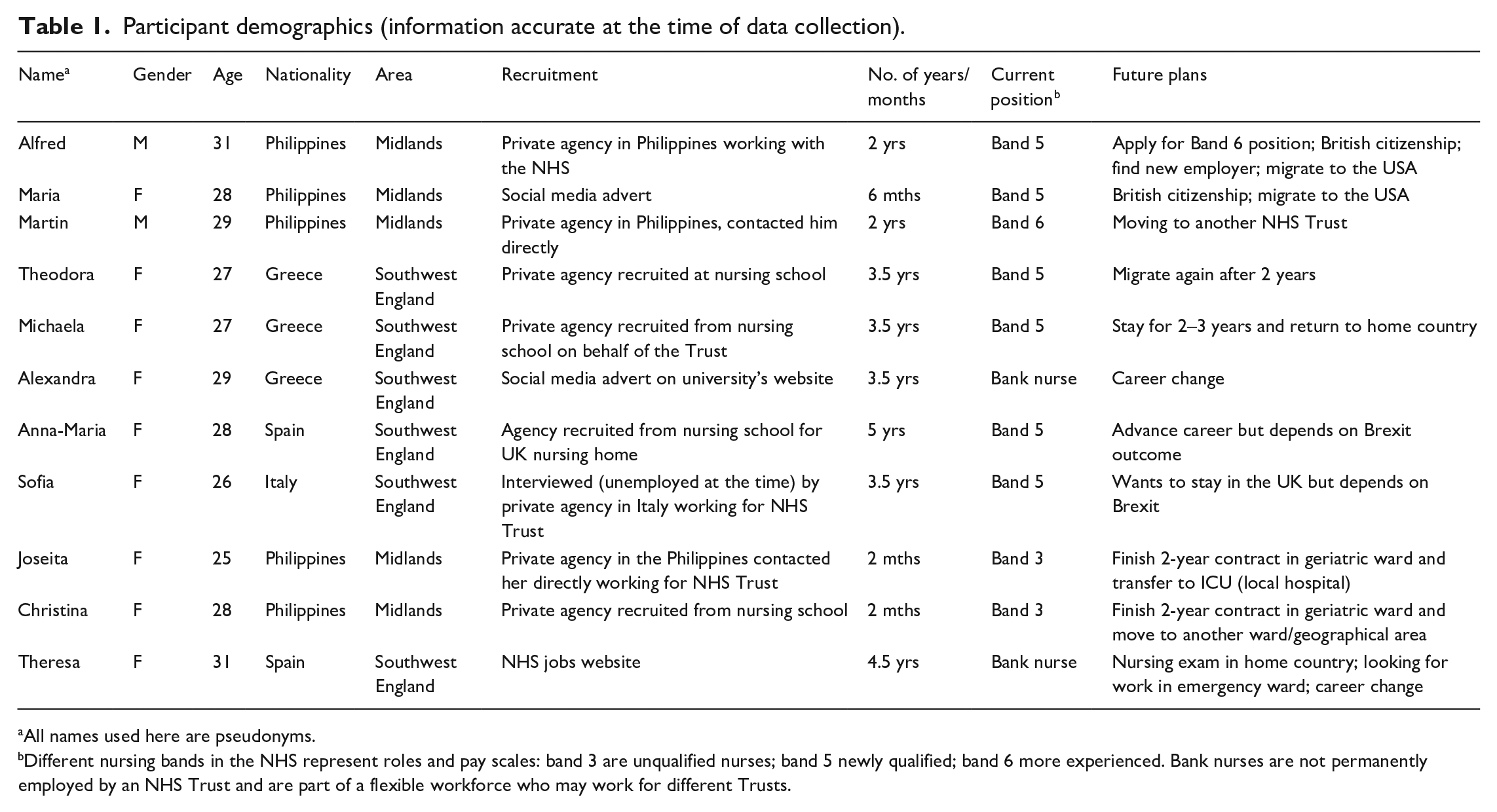
All names used here are pseudonyms.
Different nursing bands in the NHS represent roles and pay scales: band 3 are unqualified nurses; band 5 newly qualified; band 6 more experienced. Bank nurses are not permanently employed by an NHS Trust and are part of a flexible workforce who may work for different Trusts.
We used semi-structured interviews (Galetta & Cross, 2013) and thematic analysis (Boyatzis, 1998; Braun & Clarke, 2006) to examine ‘othering’ practices experienced in the everyday lives of the migrant nurses. Face-to-face interviews took place in cafes, with one interview conducted over the telephone. Average time of interviews was 40 minutes and follow-ups through telephone and email were also used to clarify any questions from the initial interview. While semi-structured interviews (Galetta & Cross, 2013) allow for the participants to discuss issues pertinent to them in more detail, thematic analysis (Boyatzis, 1998; Braun & Clarke, 2006) allowed for the examination of broader themes of ‘othering’ and bordering practices.
Interview questions focused on: how the nurses were recruited; training prior to finding employment in the NHS; job satisfaction and opportunities for career development; everyday experiences and interpretations of the Brexit referendum outcome; and their long-term plans. Recruitment strategies were an important aspect of our study, in connection to the role of the NHS as an ‘imperially-resourced service’ (Fitzgerald et al., 2020). This study builds on literature focusing on the experiences of international NHS nurses (Allan et al., 2004, 2009; Kramer, 2006; McGregor, 2007; Ryan, 2007) which have highlighted issues of racist discrimination, bias, limitations to social mobility and training for nurses. Furthermore, in previous studies we have carried out (Spiliopoulos, et al., 2021), UK public and private healthcare services rely on recruitment agencies or send their own managers to other countries to recruit directly from nursing schools or hospitals, confirmed by one of the managers interviewed for this study. These appear to be common practices and feed into the criticisms of the NHS employing imperialistic attitudes to recruitment from former colonies, and Eastern and Southern Europe. We make an important contribution to the existing literature on UK nurse migration, by examining the experiences of Southern European nurses whose experiences are not as well-documented as those of other white, European nurses (for example, Ryan, 2007; Rzepnikowska, 2019).
Findings: ‘I don’t want them to respect me because I am a nurse, I want them to respect me as an individual, for who I am’ – migrant NHS nurses wanted but merely tolerated
In this section, as seen in the quote above, we discuss the most prominent themes which reflect the participants’ precarious and differential positioning in connection to their gender, occupation, race, ethnicity and nationality, and importantly, as being merely ‘tolerated’. We focus on the two ‘critical locations’ (Acker, 2006) studied, two Trusts in the Midlands and Southwest England and the surrounding community in each location. The participants disclosed their everyday lived experiences and concerns for the future: feeling unsettled post-2016 EU Referendum; stalled career progression – new and ongoing challenges; and mitigating future challenges – the importance of institutional support.
Feeling unsettled post-2016 EU Referendum
Othering in their everyday interactions, in hospitals and communities, directly related to the Brexit xenophobic rhetoric and bordering practices, was a regular occurrence for the majority of the participants. This included bullying from colleagues, racist remarks from patients, and even remarks from members of their communities on their place of origin, questioning their legitimate presence in these English communities. For the participants, racist experiences may not have been new, however, feelings of being ‘unwanted’ and ‘unsettled’ were experienced more acutely following the 2016 EU Referendum.
Discriminatory attitudes were expressed by patients and while senior management were supportive of the migrant staff, policies did not necessarily translate into a feeling of safety:
I had racist issues, with a family of a patient, and the husband, was like, ‘why don’t you go back to your own country?’ And I was, ‘actually, I have to look after your wife. Otherwise, nobody will do, because in this shift, we are five foreign nurses, and only one British.’ . . . Recently, the chief executive from the hospital wrote a report, in the official page of the hospital, to let us know, that as a hospital, they appreciate nurses from all of the world, and they will do everything to protect their rights. . . . So, we feel quite protected in theory, but there is still an attitude, you could feel it, in the air, that something is wrong.
In this extract, Theodora, a Greek nurse, is narrating her experience of being racialized as a white, European nurse (Ryan, 2007), and excluded from the ‘community of value’ (Anderson, 2013). In this encounter with the patient’s family, she is using her own agency to mitigate this exclusionary attitude – ‘actually, I have to look after your wife. Otherwise, nobody will do, because in this shift, we are five foreign nurses, and only one British.’ In her response she is claiming legitimacy for her role as an NHS nurse, despite being viewed as a ‘foreign’ nurse. This extract showcases how hegemonic power is expressed through the ‘politics of belonging’ (Yuval-Davis, 2011), within the parameters of a heightened xenophobic rhetoric, which delineate boundaries of (il)legitimate and (un)desirable belonging within specific time and place parameters. The social divisions intersecting here are: ethnicity, race, gender, occupation. Theodora’s presence is hence ‘tolerated’ and viewed in an instrumental way, as much-needed labour. While the Trust’s senior management has taken action to protect staff from racist attitudes, nurses like Theodora ‘feel protected’ but only ‘in theory’. The performance of othering here by the patient’s family reflects the restructuring of belonging as an everyday performance – Theodora is viewed as illegitimate due to her ethnicity and race, her whiteness is not equated with Englishness but is indicative of the wrong kind of ‘white’.
In the extract below, Theresa, a Spanish nurse, is expressing the feeling of being ‘unwanted’ more acutely because of the normalization of discrimination post-2016 EU Referendum:
The only difference I noticed with Brexit, this is my personal experience, I feel that people are more open to expressing what before they only think. . . . it gives them the entitlement to say ‘I think this’. . . . I used to work with another nurse and there was this conversation between two English nurses, she was like, ‘who are you talking about?’ ‘The one who doesn’t speak any English.’ They didn’t notice that I was in front of them.
Theresa experienced exclusion by her English nursing colleagues, because of her perceived lack of English language skills. Here language becomes a marker of difference (Allan et al., 2004) and her legitimate position in the ward was questioned. For Theresa, the Brexit result has allowed for a more explicit xenophobic attitude towards Europeans and those who do not ascribe to normative expectations of Englishness and legitimate citizenship (Anderson, 2013; Anthias, 2013; Ryan, 2007; Yuval-Davis, 2011). As discussed, discriminatory attitudes towards non-British staff in the NHS are not a new phenomenon, however, their prevalence and normalization is a worrying trend.
Economic uncertainties connected to Brexit were an important consideration for the participants of this study. For Martin, a Filipino nurse, Brexit was affecting the staff–patient ratio on the wards but also had financial implications for international nurses:
There is no specific plan for Brexit yet. . . . But, we’ll see, what, how the British economy will do. Because even if we stay here, if we are going to send money to the Philippines, it’s not that really good. . . . You can see, that, European nurses are leaving England. . . . It will always be short of staff and then it will depend on how the Trust will support the ward, for example, in my area, the only nationalities are definitely on the ward are just the British and Filipino. . . . all the Italians have left.
Economic security is a motivating factor for many migrant nurses to migrate to destinations such as the UK (Kingma, 2006) and hence, any negative impact on remittances could be detrimental on decisions to invest in long-term career plans.
As confirmed by one the NHS managers (Manager A), ‘the EU route has already dried up’, due to the introduction of stricter English language requirements for EU nurses (NMC, 2017) but also because of Brexit. For Manager C, Brexit was a detrimental factor influencing EU recruitment but also international recruitment in general: ‘I don’t know if we’re doing ourselves any favours at all. It’s nationally with Brexit. . . . I very much believe that we’re [a] globalized society and I think when people get a sense that they might not be welcomed, [this is] not going to encourage them to come work here.’ All four NHS managers confirmed that their Trusts were targeting international nurse recruits from either the Philippines or India.
Additional costs imposed on international NHS staff added to the sense of economic insecurity:
And then, with the international health surcharge, it’s really unfair because from the reasoning of the parliament, migrants who are trying to get the benefits of the NHS, need to pay double, with the IHS, because it will be unfair to them, British taxpayers. But we do pay our taxes as well.
Even though the Government announced the cancellation of the IHS during the 2020 pandemic (Marsh & Gentleman, 2020), the IHS is an example of conditional or ‘tolerated’ citizenship (Anderson, 2013). Here, Martin’s nationality intersects with other social divisions such as occupation, race and ethnicity and places him in advantageous (desirable employee) and disadvantageous (migrant) positionings, hence viewed as ‘tolerated’.
Racism and discrimination were also experienced outside the workplace. For Theodora and Theresa, socializing with friends in their local pubs would attract English locals’ attention and discriminatory comments – ‘are you lost?’ Theodora exclaimed: ‘I don’t want them to respect me because I am a nurse, I want to them to respect me individually, because I am who I am.’ Here, Theodora is verbalizing the feeling of being identified as exclusively as a ‘nurse’, merely tolerated. As discussed in the next section, these ‘Brexit’ effects need to be understood in the context of other long-standing issues with the NHS nursing workforce.
The Brexit effect on migrant NHS nurses – new and old challenges
Here we highlight the old and new challenges which the participants of this study were facing post-2016 EU Referendum, including: overwork due to staffing shortages; limited resources connected to their nationality; and increased discrimination on the wards. For Acker (2006), social divisions intersect in the ‘critical locations’ and sustain hierarchical positions and marginalization. Here we illustrate how these social divisions intersected to create differential positionings, showcasing how international staff are devalued due to institutional discrimination (Allan et al., 2004) and, increasingly, due to perceived divisions connected to the politics of belonging (Yuval-Davis, 2011; Yuval-Davis et al., 2018).
For Alfred, a Filipino nurse, the loss of EU nurses meant a heavier workload for the remaining Filipino nurses, especially when he felt much pressure to undertake responsibilities as a ward nurse and nurse in charge: ‘We are really short of nurses. When you are the nurse in charge, you are not meant to handle patients. So, basically you are doing two jobs at the same time.’
The staffing issues were further compounded for Alfred by his experiences of being ‘othered’, ignored and made to feel invisible on wards predominately staffed by British nurses:
Generally, I feel the support of my ward sister and my colleagues. Because on our ward, we are two Filipino nurses and two health care assistants are Filipinos. I would want to say that in that ward, it is not majority British staff, it is like a good mix of international nurses. So, I feel the support in our ward. . . . My ward sister called me, asking me if I can help on another ward, because that ward is really short. And . . . that’s the most horrible experience. Because that ward is the extreme opposite of my ward. There are some people that are really nice but some of them are ridiculous. I wish I can get hold of one or two ward sisters who work there, that they can just see that experience. I spoke to the ward sister of that ward and told them what my observations are. I also told them that this person made me feel like this. It’s like the feeling that you are there, but as if you are not there. And they don’t offer any kind of support, even if you are struggling.
Here Alfred mentioned two issues connected to Brexit and the subsequent loss of EU staff – understaffing and overwork; and the feeling of being undervalued by some British colleagues. Alfred’s experiences showcase how a ‘good mix’ of international staff is seen as essential for migrant nurses in order for them to feel that they belong and their position is legitimate.
Alfred’s experience of working for this Trust was one of mixed emotions in terms of access to resources. While this Trust offered advanced nurse training, which was one of the reasons that Alfred decided to take this position and move to the Midlands, he was disadvantaged in comparison with international nurses in other Trusts, who are offered longer work permits. Martin disclosed similar experiences:
One reason why I chose [town], is because the initial sponsorship was five years, and then, when I ask about why, how come that they only gave us like two years’ insurance contract, and then they said, ‘don’t worry, because we will renew everything’. But we contacted HR last December, that’s the only time that they told us that they won’t pay for the visa. I was trying to negotiate to give me three years, so that I will only need to renew once. Because it’s expensive, the visa processing fee. But then, HR doesn’t really want to compromise.
One of the findings of this study is that migrant nurses ‘shop around’ for the most advantageous positions among NHS Trusts. Being offered a two-year permit as opposed to three-year permits offered at other Trusts is a serious impediment for overseas nurses due to feelings of insecurity and the economic costs involved. This is an indication that NHS Trusts take on an ‘imperialist-resource’ character, depending on migrant nurses to fill shortages on the wards but not supporting them to stay long-term.
Conversely, participants who felt that their career aspirations were being supported by their employers were much more likely to feel valued, continue to work for the particular NHS Trust, and subsequently invest in long-term stay in the UK:
Yes, my goals are being an ACP [Advanced Clinical Practitioner] . . . if I go back to Spain, I couldn’t have the opportunities to rise, or get promoted, ACP aren’t there, because in Spain, once you are a registered nurse . . . you are just registered nurse . . . which is all right, but if you have expectations, to be promoted, this is very difficult.
However, even Anna-Maria, a Spanish nurse in Southwest England, whose career plans meant that she wanted to stay in the UK, had doubts:
. . . for long term, I’m very confused, just because we don’t know what is going to happen with Brexit. . . . all depends on Brexit . . . life is not going to be as easy as it been until now. To have bad time over here, is different to have bad time in Spain, where I have my own family’s support.
Considering the positioning of nurses such as Anna-Maria, career progression is a crucial factor in long-term commitment to working for the NHS. However, as discussed, Brexit has brought a number of uncertainties which can only be partly mitigated through social mobility.
We can surmise that not only do individual NHS Trusts offer different resources to their migrant nursing staff, which then shape their long-term investment in their NHS career, but also that there are inconsistencies between Trusts. Wards and NHS Trusts can thus be construed as ‘critical locations’ where social divisions intersect to create advantages and disadvantages. Theresa, for example, a Spanish nurse, and Alexandra, a Greek nurse, were also working for the same Trust as Anna-Maria. Both experienced discrimination in their workplaces and were therefore only undertaking bank nursing. They were so disenfranchised that they were both considering a complete career change, despite efforts by some NHS Trusts to support migrant nurses, as discussed in the following section.
Mitigating Brexit challenges – supporting nurses on site but also bringing from abroad
For some of the participants, Brexit did not affect their long-term settlement plans. Sofia, an Italian nurse in Southwest England, welcomed the Trust’s support on securing EU settlement status:
I noticed that the hospital started a trial to make the new settlement programme easier for us nurses, so they’re going to pay for it, and they are setting up services to help us, which makes me think probably they still want us here. Because of that, I don’t think it’s going to affect us in the health care professions at all, because if we have to, if all the nurses from overseas had to go back to their countries, I am not sure where the NHS would be.
Sofia’s experience comes into contrast with the experiences of nurses such as Alfred and Martin in the Midlands, who did not feel valued by their HR department. For Sofia, this support received by her Trust was proof that EU nurses were valued. Additionally, she was claiming her professional standing, worth and legitimate position by stating that the NHS would not be able to function without migrant nurses. Her response is seeking to counter the Brexit bordering practices and stresses NHS reliance on migrant staff.
The NHS managers shared many of the migrant nurses’ concerns in terms of long-term challenges post-Brexit:
You cannot bank on any one option and you have to value and recognize the staff that you have, recognize their potential. So uncertain times for workforce, and I’m worried. (Manager A) With Brexit there was significant[ly] more difficulty to recruit from Europe. It is certain that all Trusts will look to the same areas [of specialization] where there is the problem and that will increase competitive tension in those areas. (Manager D)
Furthermore, the managers appreciated that it would not be straightforward to substitute nurses from outside the EU for those who they were unable to recruit from the EU post-Brexit:
The point is we no longer readily recruit from the EU, so we are recruiting internationally. And at the moment, there is international supply. But obviously when the pinch point comes, when everybody’s going international, and there’s a global shortage of nurses and health care workers, we cannot be reliant on international supply. So, we have to look at our own pipelines and grow our own workforce. We’re doing a bit of everything. (Manager D)
Continuing reliance on overseas nurses was clearly a topic of intense consideration for the NHS nursing managers. ‘Bring[ing] in from abroad’ was promulgated by bodies such as NHS England and NHS Improvement (2019, p. 5) as one of the pathways to deal with ‘[T]he most urgent challenge [being] the current shortage of nurses, who are critical to delivering the 21st century care set out in the NHS Long Term Plan’. The managers recognized the importance of pastoral care, offering educational opportunities and crucially, a sense of community, both inside and outside the hospital, and recognition of their contributions in order to retain international nursing staff. While all managers recognized the implications of Brexit in meeting their staffing needs, support mechanisms already in place included: building trust and communication in person and on social media; newly employed staff being included in the nursing communities of British, migrant and co-ethnic staff; and introducing newcomers to life in Britain via local community events. As Manager D explained: ‘we try to take equal attention to the clinical aspect as we do the integration into the wider society perspective. . . . We can’t underestimate the impact of the pastoral aspect on the positive outcomes of integration of international nurses into the organization.’ Such practices cannot entirely mitigate exclusionary practices but can offer a much-needed supportive environment.
Concluding remarks and policy implications
For the migrant NHS nurses in this study, racism, discrimination and bias were not new phenomena. However, Brexit brought these to the fore and intensified feelings and practices of othering. Citizenship, as an embodied experience (Yuval-Davis, 2011), for the EU and non-EU nurses was interpreted as framed within economic contributions (Anthias, 2013). The migrant nurses were merely ‘tolerated’ citizens (Anderson, 2013), increasingly feeling unwanted, unsettled and racialized (Ryan, 2007). By using a situated intersectionality approach and examining everyday bordering practices (Cassidy et al., 2018a; 2018b; Yuval-Davis et al., 2018), migrant NHS nurses are placed in sometimes advantageous but more often disadvantageous positionings, creating contradictory inclusions and exclusions in post-Brexit Britain. The volatility of immigration policies (Anderson, 2013) and instrumentality of policy interventions, such as the IHS (Gov.uk, 2015), cannot be underestimated in their effects on nurse retention and recruitment, and on the long-term settlement of migrants.
The shadow of Britain’s colonial past continues to affect the positioning of migrants and more widely, of its ethnically diverse populations. The NHS is an institution which exemplifies the bordering practices increasingly at play. Some positive, albeit slow-paced, steps are taken through initiatives such as the NHS Workforce Race Equality Standard (NHS WRES, 2020), which seeks to identify racial inequality and discrimination, and provide indicators (bullying, harassment, discrimination, abuse and bias in promotion) for NHS Trusts. We argue that further research into the gendered, racial and ethnic inequalities of the healthcare workforce is needed, if ethnic and other diversities are to be celebrated and embraced, outside the constraints of economic contributions, imposed assimilation and increased borderings.
Footnotes
Acknowledgements
We would like to thank the participants of this study for their time, trust and disclosure – their support has been invaluable. We would also like to thank our anonymous reviewers for their very supportive comments and feedback. Finally, we sincerely thank our funders for their financial and overall support.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University of Nottingham Research Priority Area Development Funding (Research Priority Area: Rights and Justice); and the School of International Studies, University of Nottingham Ningbo China.