
Abstract
Drawing on narrative interviews from a study exploring the perceptions and experiences of children and young people who have a parent with young onset dementia, this article explores the ways in which the condition impacted their life courses. Dementia is degenerative, terminal and has an unpredictable timeframe that affected young people’s time perspectives, life planning and the ways they conceptualized their lives. This article contributes to the literature around young people’s life courses by illustrating how the concept of liminality can inform understandings of the impact of parental illness on the life course. Using a constructionist perspective we explore the impact of parental dementia on life planning in relation to education/career, mobilities and personal lives. For some, the future was a source of deep anxiety, whilst others were preoccupied with the present and unable to contemplate life beyond their parents’ illness. On the whole, participants felt their lives were in ‘limbo’ until their parents’ death. The data indicate that nuanced approaches towards the life course are required in order to better understand ‘being in limbo’ and to inform support.
Introduction
Young onset dementias (YOD), i.e. dementias presenting before the age of 65, are relatively rare, affecting around 44,000 people in the UK (Burns, Issacs, & Carter, 2017). Estimates suggest that around a quarter of those with YOD have children under 18 at the onset of the condition (Haugen, 2012) but very little research has investigated how children and young people experience parental dementia. The limited evidence available indicates social and emotional upset, physical and mental ill health, financial hardship and family break up compared with children who are adults when at dementia diagnosis (Hutchinson, Roberts, Kurrle, & Daly, 2014). This study took a narrative biographical approach with a limited longitudinal element that offered insight into how parental dementia is temporally experienced.
Dementia, temporality and the life course
Dementia is the umbrella term for terminal illnesses that affect the brain causing progressive cognitive and physical impairments and significant personality and behavioural changes (Stewart, 2006) highlighting the relationship between time and health (Frankenburg, 1992). Obtaining a definitive diagnosis – and, thereby, the identity of a person/family living with dementia – is a protracted, convoluted process, often lasting years (Sikes & Hall, 2017). The condition’s unpredictable development involves multiple, unexpected cumulative declines and losses ending in death, and thus, anticipated life courses are affected as time runs out for the individuals and their families (Adam, 1995).
Theorizing the life course
The life course is the sociological concept applied to the framing of individuals’ experiences as shaped by chronological phases usually in the linear ‘birth to death’ trajectory (Hunt, 2016). Theorizing the experiences of individuals and of social and cultural groups through the life course lens illuminates how disruptions and unexpected occurrences, such as illness, are experienced (Williams, 2000). Life course phases may be biologically (e.g. puberty and reproductive capacity) or developmentally informed (e.g. cognitive abilities that enable independence). Furthermore, socially constructed ideals regarding capability and appropriate behaviour, e.g. notions of how people of different ages should behave, may manifest (Hockey & James, 2003). Such constructions permeate lay consciousness as in notions of being considered a ‘young’ or ‘old’ mum or a death that is a ‘good innings’ or ‘before one’s time’.
Illness disrupts the life course of persons with a condition and those of the people close to them (Bury, 1982; James & Hockey, 2007), highlighting that within families, and more widely, the life course is experienced collectively. As the life course is synonymous with normative conceptualizations of particular phases, and framed by landmark events and rites of passage, parental terminal illness has the potential to disrupt young people’s expected life courses. The very label of young onset dementia illustrates its perceived untimeliness.
Chronologically ordered linear life phase models such as those theorized by Elder (1994) and Erikson (1980), become culturally bound and assume dominant narrative status. This can lead to pathologization of lives which deviate ‘too far’ from the norm. When the lives in question are young people’s, the road to adulthood and the myriad of tasks associated or facilitated by advanced maturity can be compromised. Someone whose life course is deemed ‘unusual’ can experience personal identity discomfort and be stigmatized within their social contexts (Goffman, 1963). Being unable to meet age, gender, social class and faith based appropriate obligations and stages can lead to emotional distress as well as practical impacts, including financial difficulties if, for instance, education and employment are impacted.
Early sociological conceptualizations of the life course depicted it as being composed of discrete stages: childhood characterized by socialization and education, adulthood dominated by paid employment and family followed by old age at retirement. In postmodernity, these stages have been brought into question (Hunt, 2016). While postmodernity is of course a contested concept, a myriad of conceptualizations (Hunt, 2016) acknowledge that changing historical, social, technological and communications developments and trends alter the possibilities for life courses and choices (Brannen & Nilsen, 2002). Thus, people can lead very different lives to those available to their forebears. Preconceived conceptualizations of time and space influence notions and expectations of, and planning for, likely futures (Brannen & Nilsen, 2002). Nevertheless, chronological age continues to be fundamental to how lives are organized by the state and other agencies, vis-a-vis legislation (e.g. sexual consent, alcohol consumption), educational provision, fees and fares (e.g. for health care and travel). Life course related institutions and categories simultaneously shape age related expectations and respond to age related needs (Dannefer, 2012).
Giddens (1991) suggests there is increased emphasis on individual choice and this can weaken expectations around ‘standard’ biographies followed according to gender, class, ethnicity, faith group and geographical location. However, greater choice can lead to its own burdens and stresses (Bauman, 1998; Beck, 1992; Brannen & Nilsen, 2002) some of which may have particular resonance for young people with a parent with YOD. For example, over the last 40 or so years, and in the UK, changes in family roles and responsibilities include a shift from familial obligation towards family relationships based on liking and closeness (Giddens, 1991) with consequences for how caring for parents is understood. Furthermore, extended education trajectories contribute to a view that boundaries between cultural and social dimensions of youth and adult are increasingly blurred (Gilleard & Higgs, 2016). Some stages may be omitted, others postponed or brought forward (Brannen & Nilsen, 2002; Kohli, 2007; Widmer & Ritschard, 2009). Life planning is challenging, and low income and job insecurity hinder markers of adulthood, leading to conceptualizations of ‘emergent adulthood’ (Arnett, 2000, 2014; Brannen & Nilsen, 2002). However, long established expectations persist, and among children and young people ‘when the future is imagined, it is depicted through traditional rites of passage in the life course – getting married, getting a job, having children’ (James, 2005, p. 256). Additionally, emergent rites of passage, or significant life landmark events, such as attending school proms and university graduations have acquired a deeper significance (Bodnar, 2015; Tinson & Nuttall, 2010). Being unable to achieve landmark events or to experience them in the way that one had hoped and in accordance with expectations and dreams can be painful – particularly when peers are following the life course anticipated.
The impact of illness on the life course is well documented (James & Hockey, 2007). In this article, we draw on two sociological concepts: temporality and liminality, which are each outlined below.
Temporality
Adam’s theorizations of time (1995) posit that it infuses our everyday lives. Lives are lived in the context of the irreversible direction of time with terminal illness forcing ‘premature’ awareness of death. Temporality is a mediator for relationships, thus facing limited time may affect family relationships, with implications for young people’s life courses. The data presented illustrate how a significant consequence of parental dementia and the nature of dementia itself can be a state of liminality.
Liminality
Turner’s (1969) work on liminality is helpful here. When an individual is ill, they may feel and be seen as ‘neither here nor there; they are betwixt and between’ (Turner, 1969, p. 95), if, for example, they do not neatly fit into particular categories or definitions and are thus, liminal. Those experiencing symptoms of ME may find that their symptoms are contested, meaning they experience illness without being afforded the status of being ill (Brown, Huszar, & Chapman, 2017). Similarly, those living with an incurable form of cancer do not occupy the space of being in treatment or having survived the disease (Broom, Kenny, & Kirby, 2018). Young people with a parent with dementia are in the in between space of being bereaved as a result of their parents’ symptoms, and yet not afforded the considerations attributed to those who are conventionally bereaved (Sikes & Hall, 2017).
Young people’s accounts of parental dementia indicate continued relevance in viewing life phases as accomplished over time, framed by familial relationships. However, the data show that the extent to which the life course as proceeding in a particular sequence or trajectory correlates with lives as lived, on account of liminality, can be called into question. Individuals’ time perspectives may be informed by social scripts of other people’s life courses and life expectancy. An experience such as parental illness and early death may contradict dominant narratives of the life course.
Our data explore the ways in which young people’s perspectives regarding their lives, their plans, choices, decisions and envisaged futures were affected by parental YOD and in so doing we seek to contribute to the sociology of young people’s life courses, using concepts of liminality and temporality as lenses.
The study
The study employed a life history approach to this endeavour which sought a narrative auto/biographical, specifically life history approach, to elicit and analyse the in-depth, personal stories of children and young people who had experienced parental dementia. This approach, grounded in the work of members of the Chicago School (e.g. Shaw, 1930; Thomas & Znaniecki, 1918–1920) privileges ‘stories of action in theories of context’ (Stenhouse, 1975), thus illustrating links between biography and society (Bertaux, 1981).
The narrative, auto/biographical ‘turn’ has lacked prominence within child and youth studies (James, 2005; Riessman, 2008) which can be considered to have contributed to silencing and hiding young people’s lives (McLaughlin & Tierney, 1993). Whilst acknowledging the problems around claims to ‘give voice’ articulated by such authors as Jackson and Mazzei (2009) and Gullion (2018), the decision to use narrative auto/biography was based on a commitment to recording and using what the young people said to ‘force a confrontation with other people’s subjective perceptions’ (Goodson & Sikes, 2001, p. 7).
The study was shared on a project website, across social media and by leading dementia organizations. The 23 participants, from throughout the UK, aged 6–31, ‘found’ us when they were seeking YOD information and support for themselves or, in two cases, for their children. We initially wished to seek the views of those aged 7–25, reflecting United Nations and WHO definitions of youth. Although a broad age range, this facilitated an exploration of the impact of parental dementia throughout childhood and youth. We included four older volunteers because we regarded exclusion unethical. Furthermore, their retrospective accounts of having grown up with a parent with dementia offered useful insights into the impact from a life course perspective, and one which is largely absent in dementia studies.
Participants’ parents had a diagnosis pending; a ‘recent’ diagnosis (under a year); were several years post diagnosis; or had died from dementia. We have categorized participants as: primary school children; adolescents; students; and young adults, who were largely in employment. Age categories are of course arbitrary, and this information merely provides some context. The older sample comprises 17 women and 3 men. This representation of women’s narratives is pertinent given that burdens of care fall to and are socially expected to be assumed more by women than men (Sharma, Chakrabarti, & Grover, 2016). Such responsibilities may be particularly concentrated among lower socio-economic groups. We did not collect data pertaining to social class, so we cannot explore this in depth. However, the narratives do suggest a middle class bias if we take class to be equated with markers such as university education and property ownership (although this is problematic [Reay, 1998]). As such, there may be access to certain resources. That said, young onset dementia corresponds with working age, forcing parents into early retirement or redundancy, and their offspring may find that their careers and education are curtailed, so may not benefit from their apparent class status compared with families from a similar background. Familial structure was critical. In the five cases where participants were charged with their relatives’ care, parents were divorced (4) or widowed (1) and three of these participants were also singletons. Caring thus required the financial means to fund private care (home help/care home) or demonstrating eligibility for state care, which is itself a problematic process.
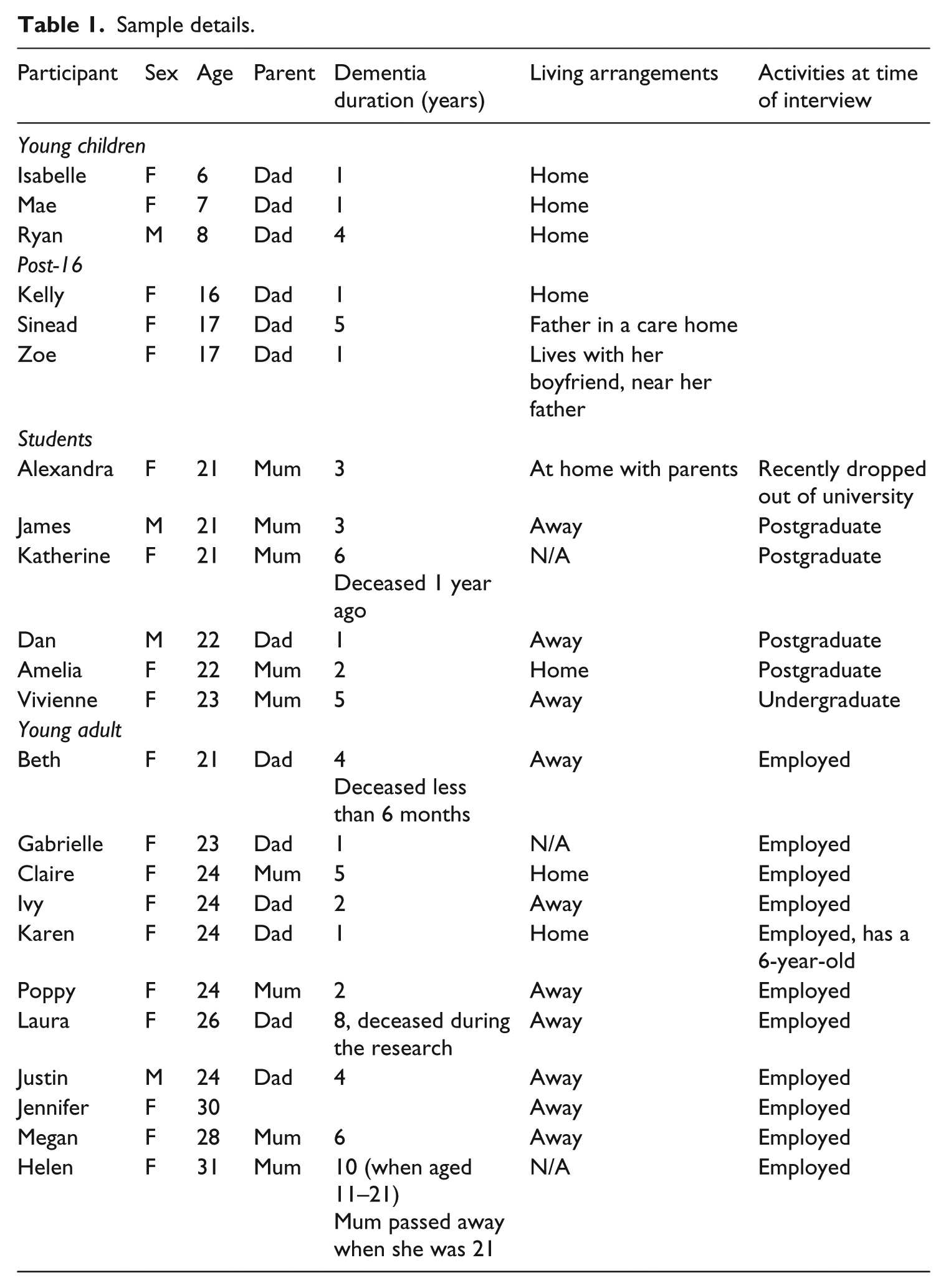
Participation entailed up to three unstructured conversations over 12 months, each lasting 45 minutes to two hours. This fostered participant–researcher familiarity and captured developments in participants’ narratives and lives. Table 1 provides an overview of the sample. Whereas older participants were simply invited to tell their story of living with parental dementia, sessions with under-10s involved play, drawing, family tree and ‘my day’ storytelling activities (James, 2005). Ethical approval was granted by our university. Participant consent, plus parental consent for under-18s, was ongoing before and throughout interviews.
Sample details.
Thematic analysis considered narratives in their complete form, acknowledging context and developments in the story over time, highlighting key themes (Riessman, 2008). The first stage entailed ‘open coding’ where transcripts were read and initial themes identified. These were then organized into themes and sub-themes which were refined (Braun & Clarke, 2006).
Findings
Accounts demonstrated that participants considered that within a temporal framework their life courses had been shaped by their parents’ illness. Time was a resource, with hindsight helping make sense of what had happened (Freeman, 2010; Hall & Sikes, 2018b; Williams, 1984), meanwhile terminal illness rendered time a limited commodity (Adam, 1995). At a broader level, analysis draws on Holstein and Gubrium’s (2007) conceptualization of the individually constructed nature of the life course. A unique aspect of parental dementia concerns the tangible losses of parental abilities over time (e.g. communication, memory, mobility) and the way in which children must manage and reconstruct their life course as death approaches and indeed, beyond. Concepts of liminality and waiting further contribute to understandings of this experience. The research suggests an imperative for more nuanced approaches to the life course. Data are explored in relation to how participants constructed the life course in light of their parents’ illness. This is followed by an exploration of ‘liminality’ experienced by those who have a parent with dementia. Finally, we consider how participants manage this liminal space.
Constructing the life course
Participants’ narratives were characterized by two paradoxical, yet complementary, temporalities. On the one hand, time with the parent was considered finite. However, in the absence of a definitive prognosis of life expectancy, exacerbated by unpredictable decline, living with dementia stretches into an unknown, unbounded future. Unlike other illnesses, scans and tests do not accurately indicate progression and prognosis, so the outlook is simultaneously definite, yet unpredictable and this required management. This made planning for the future a challenge.
Planning for the future
Participants described how they needed to plan for their parents’ care. Vivienne, for example, spoke of the effect on her everyday life of more than two years of preparing for her mother’s imminent death: A year ago [doctors] were saying it could be no longer than a month and she’s still on that basis . . . I have her life expectancy like a month’s rolling contract . . . I know there will be something drastic but I don’t know when . . . Anytime someone calls and I don’t know the number, I’m like something has happened . . . usually it’s PPI [an automated call]. (Vivienne, student)
Yet, in the face of apparent uncertainties and the ‘not knowing’, young people accommodate to the future. For example, Megan was anticipating both her mother’s death and her care needs: I hope it’s [death] a long way off because it will be a traumatic experience . . . it could be in a couple of months, or the other thing is that something happens to Dad and Dad becomes suddenly unable to deal with Mum . . . You just don’t know what’s around the corner. (Megan, young adult)
The excerpt from Megan’s interview describes planning relating to her parents. Other data described the implications of parental dementia for the considerable efforts required to plot one’s own life, as we will now discuss.
Managing professional and personal lives
Educational careers temporally structure young people’s lives: chronological age dictates educational stage, for example, primary or secondary school attendance, GCSEs or going to university. However, the pathways of those whose parent has dementia can be disrupted. Sinead was studying for her ‘A’ levels as a distance learner to give her time to spend with her Dad as her school wouldn’t permit a flexible timetable, while Alexandra had dropped out of university due to the stress of the situation (Sikes & Hall, 2018). Others considered that their lives were ‘on hold’ and so education filled that time in a purposeful way. Long term, Amelia hoped to relocate to pursue a graduate career, but felt this was rendered impossible by her mother’s illness, and so embarked upon postgraduate study: I needed to give myself some sort of direction, a distraction, something to focus on that I could work towards. If I hadn’t done it, I would be working full time at a restaurant and thinking ‘This isn’t what I’d be doing otherwise’. If Mum hadn’t been ill, I would have had a year out and then moved away from home and then done a Master’s. (Amelia, student)
This shows how education, an established phase of the life course can be destabilized by parental dementia. This disruption was evident upon leaving education and entering the labour market too. For example, Megan, who lived far from the family home, accepted a job because it entailed travel near her parents. However, others perceived the negative impacts upon careers, as was the case for Poppy, an only child of divorced parents, who considered that her responsibilities had hindered her career progression. She was working, but had struggled to hold down a graduate job while supporting her mother because her employers could not accommodate her responsibilities: I’m intelligent, I should be in a career . . . I’m not going to really have a career. My CV doesn’t look great, I’ve had a few jobs . . . I’ve been okay . . . then a crisis with Mum . . . a month afterwards, I’m not there anymore. (Poppy, young adult)
It was challenging for someone in Poppy’s position, without a parent or sibling to share the support with, to pursue the trajectory a university graduate might expect. Conversely, other participants were able to, and had been motivated towards careers. James, the son of a housewife, feared inheriting dementia, motivating him to seek a career teaching languages.
I look at Mum, in the years leading to diagnosis, it was all monotonous . . . would a different lifestyle have kept it off longer? They say languages is one of the things . . . [it was] always something I was interested in but Alzheimer’s strengthened my desire. (James, student)
Katherine, a biologist, whose father had also died, reported that her mother’s condition stimulated her academic interest, and she subsequently registered for a doctorate involving clinical dementia research. She highlighted the considerable price to be paid for this notionally positive achievement: I don’t think I’d be doing the PhD on a type of dementia I’m doing if it wasn’t for that . . . It changes the course of your life. But that was tinged with sadness . . . I would have loved for my parents to know I’d got a PhD. (Katherine, student)
Marriage, parenthood and leaving home are considered defining features of the life course in transitioning to adulthood (Hockey & James, 2003; Kenyon, 1999). Having a parent with dementia and living with an unpredictable timeframe impacted young people’s navigation of their intimate lives such as marriage or family planning. This echoes research on parental cancer which indicates a concern with time running out (Puterman & Cadell, 2008). Claire wanted (and went on) to have her wedding sooner rather than later and planned to have children earlier: I would like to get married quite soon because I want mum to be there and to
There was a particular need to plan having families in terms of what was practical or desirable. Megan, however, was deterred from having the family that she did eventually want which posed a dilemma: I wanna think about having kids but . . . I just can’t face caring for another human being right now . . . I need a break . . . We’ll put it off a couple of years but I don’t want to run out of time. (Megan, young adult)
The desire to plan could be exacerbated by the condition’s genetic potential. Katherine’s mother had an inheritable form of dementia, and she felt this required discussion with her partner about genetic counselling, were they to decide they wanted children: The whole genetic implication, has meant I’ve had to talk to him about it and when you talk in the early stages of the relationship, it all seems far away, but it’s getting more serious . . . I would want to think about [genetic counselling] before any kind of engagement. (Katherine, student)
Thus, there are tangible impacts of having a parent with dementia, with participants citing the direct impact of their parent’s illness on the direction their life has taken. Holstein and Gubrium’s (2007) framework suggests that the life course is a resource which individuals deploy to conceptualize their lives and this was seen in the data.
Life course phases and rites of passage
Social processes see people move through identities (Hockey & James, 2003) and having a parent with dementia affected participants’ perceptions of their life course. Age is a marker of social identity, associated with social obligations, and families are the context through which aged related identities are realized (Hockey & James, 2003). As parental dementia affects familial roles, it shapes personal identities. Participants lamented having grown up quickly or ‘losing’ childhood. For example, in her retrospective account of being a 10-year-old with a parent with dementia, Helen reflected: ‘You have to try and grow up. You do lose a bit of your childhood.’ Participants felt they were missing out on experiences associated with youth. For example, a period of travelling, particularly after university, is increasingly a rite of passage (O’Reilly, 2006). However, being away from parents at this time was not considered feasible or desirable: I want to go travelling but I’ll go when the time is right. I could live with the regret of not going travelling at this age, but I couldn’t live with the regret at not being there for mum . . . I was meant to go to Ibiza but I couldn’t because she had a fall. (Vivienne, student)
Similarly, Laura didn’t travel during her father’s illness but following his death, she planned to: Travelling was one thing that had gone on the back burner because I didn’t want to go when Dad was ill . . . see that map on my wall. It took two months when I realized . . . I can go travelling! (Laura, young adult)
Aspects of the life course were considered unattainable, but conversely, some had achievements that were out of the bounds of their peers, for example, property ownership. Rising house prices have resulted in an increase in the average age of first time buyers (Office for National Statistics [ONS], 2018). Some participants had inherited money on their parent’s death: Katherine, Vivienne and Beth owned property at what they perceived to be a young age. This was an economic privilege that distinguished them from their peers and their homeowner status was a source of discomfort, juxtaposed with the considerable emotional loss. They articulated that this marked them out as different, and the sense of discomfort with this privilege: I’ve inherited an awful lot of money . . . That has massively set me apart from other people my age . . . I’ve just bought a house. Everyone my age, they’re saving to have a mortgage . . . it’s going to be a struggle in 10 years and I’ve just cash bought a house . . . I’m embarrassed . . . People react like ‘where has she got that money from?’ (Katherine, student) I got my inheritance and that’s how we were able to afford this house. Everything has been bittersweet . . . It makes me feel uneasy, the price that life comes at. (Beth, young adult)
Such data show how comparisons with others come into play, and that preconceived notions of the life course are informing perceptions of the situation. This might be comparisons with peers, as the above has shown. It might also be with others experiencing dementia later in life. Laura, describing conversations with an older colleague with a parent with dementia, perceived key differences on account of life course phases: She’s ready to let go of her Mum . . . she says ‘I’m in my fifties, I’ve had my childhood with her, my teenage years, marriage, children, grandchildren’. I want to have all those moments – [Dad] walking me down the aisle, meeting my children and my partner. I won’t get that anymore and it’s a loss in that way as opposed to being 50. (Laura, young adult)
The life course as a concept was relevant. Nine-year-old Ryan perceived that his adulthood might incur responsibility. In his first interview, he thought that when he ‘grew up’, he might ‘help out a bit more with Dad, drive him places like my sister does’, indicating his perceptions of adulthood. Vivienne describes how parental death jarred with her expectations of youth: My life would be so much easier if my mum wasn’t ill and I could do what I wanted . . . I’ve missed out on being young . . . I have a
These accounts illustrate normative understandings of particular phases of the life course – young people should not be making funeral arrangements, that is for those in middle age; families expect to experience particular phases of the life course together, for example, parenthood and grandparenthood; young people go travelling; young people do not own property. The data illustrate that these young people were thrust into later stages of the life course ahead of schedule, and anticipated parental absence from other phases. Narratives also reveal a perception that young people are prohibited from phases of the life course. Established anchors of the life course – education, career, personal relationships, having children and property ownership – can be disrupted by parental dementia. This echoes research on young carers by Hamilton and Adamson (2013), which revealed impacts on education, employment, health and social life. Our participants were not experiencing the life course in the conventional way of their peers. And yet nor were they afforded the social sanctions that are given to the conventionally grieving. They are in between.
Being betwixt and between
The discord with peers’ life course phases of childhood, adolescence and young adulthood shows how these were disrupted and everyday lives impacted. Some articulated that their focus was limited to the short term and that their lives were on hold confirming research on caring generally and in relation to dementia (Age UK & Carers UK, 2016; Zimmerman, 2010). In addition they found themselves in the space between socially recognized categories and that which is beyond the realms of ‘normal’. They were ‘betwixt and between’ (Turner, 1969) and in a multitude of ways: principally, in terms of life course phases, and in between griefs. They were neither bereaved and afforded the social exemptions that might ordinarily incur, but nor do they have their parent, as we will now illustrate.
Anticipating parental death, participants’ accounts suggest that they are denied the social status and privileges that come with certain illnesses, particularly those illnesses which are contested and contradict established illness or dying narratives (Brown et al., 2017). When liminal, individuals may find themselves excluded from existing networks, or the ‘communitas’ of people one may share the experience with. Liminality can be applied to dementia, and indeed, has been to some extent (Kelly, 2008; Sweeting & Gilhooley, 1997) and on the transition from the spaces of life to death (Birt, Poland, Csipke, & Charlesworth, 2017). This applies to those experiencing dementia related grief when mourning the loss of a parent who is alive but fundamentally changed (Sikes & Hall, 2017).
The awareness of a range of future potential events then leads to anticipation of them, conceptualized as a sense of waiting. Participants described a constant sense of waiting for the next decline and, ultimately, for death, in order to plan their lives. For example, Amelia and Vivienne, both students, who might otherwise be anticipating their post-university professional lives, were waiting for death in order to be able to live their own lives: You can’t think past them being alive and you don’t know how long that will be for . . . Everything is suspended. (Amelia, student) Once Mum is not alive anymore, I’ll be able to do what I want but I don’t know, I’m not really planning anything until that happens . . . It’s just limboland. (Vivienne, student) It sounds really nasty but I’m waiting for my Dad to die . . . Waiting so I can start. (Zoe, adolescent)
This suggests a need for a ‘conclusion’ to the dementia in order to be able to move forward. Indeed, those whose parents had died described a conclusion absent from others’ accounts: I can just get on with my life . . . when you’re taking other things into account in your life plans . . . now it’s just what These horrendous diseases, they are gone. They’ve been clouding our life for the past two years . . . In having to be in the moment and not thinking about my life . . . it’s just been the disease. (Dan, student)
Amelia, Zoe and Vivienne appear to be living under the spectre of terminal illness, which occupies a constant presence. This corresponds with research by Broom et al. (2018) on cancer and waiting. Similarly, in their research with individuals with motor neurone disease, Ferrie and Wiseman (2016) posit that while waiting is often constructed as negative, they cite the hope it can sometimes invoke, a hope that is absent when illness is terminal. They go on to argue that in terminal illness, waiting (for treatment, deterioration) ‘challenges the idea of waiting as ambivalent and banal’ (Ferrie & Wiseman, 2016, p. 538). Indeed, as our participants share, the waiting is emotionally charged and far from banal.
The uncertainty and waiting draws parallels with young adults experiencing parental cancer (Puterman & Cadell, 2008). Conceptualizations of time affect the capacity to plan for the future (Brannen & Nilsen, 2002). Nowotny (1994) describes an ‘extended present’ because, for some, changes happen so rapidly that the future arrives too quickly or not at all. There is resonance here with our data insofar as dementia can progress rapidly whilst also often being long and drawn out. Understandably, young people find it difficult to plan their lives in the face of their parent’s illness. The next section, then, considers the strategies young people employ in order to help them to cope with living in a liminal space.
Managing the betwixt and between
The uncertainty provoked by dementia required young people to develop strategies to help them live with their parent’s illness. Reminding themselves of what their parent would want them to do reassured some, as did thinking of what they would be doing were their parent not ill, and is an established grieving mechanism (Walter, 1999). As Katherine describes: It’s difficult – I did what my parents would have wanted but that’s a big decision that weighs on your conscience, she was ill for years . . . if I’d have been home the whole time, that would have eradicated uni for me which just wasn’t an option. (Katherine, student)
Familial and other support networks were valuable for some in terms of affirming their actions. Amelia described the emotional support of her father: ‘Dad’s trying to emphasize that we need to live our lives
People are given leeway once someone has died but I’ve been dealing with mum dying for a long time and continually losing her and I don’t feel I get the same . . . no one would be expected to find a job just after their parent has died . . . she’s not physically dead, I’m still expected to go around living my life like a proper adult. (Vivienne, student)
The circumstances these young people found themselves in were perhaps exacerbated by the lack of a social script or template (Goodson, 2013) which might otherwise provide some pointers. As more is known about being the child of a person with YOD and as more people receive a diagnosis such scripts may become more widely available.
Discussion
This article has explored young people’s life courses in the context of parental dementia. A temporal lens can enhance understandings of young people’s lives and illustrate that the past, present and future are not linear concepts (Brannen & Nilsen, 2002). The findings shed light on young people’s temporal perspectives vis-a-vis dementia, illustrating the life course as socially constructed and a need for more nuanced approaches in light of the liminal space individuals enter.
It has been argued that, contemporaneously, there are more choices for individuals and fewer constraints from institutions and expectations (Beck, 1992; Giddens, 1991). However, Brannen and Nilsen (2002) suggest that the idea of the so-called choice biography is problematic when applied to young people because, while they may have agency, structural, social and material forces are pervasive and futures are perceived in diverse ways (Brannen & Nilsen, 2002). Adam (1998) states that young people’s temporal perspectives are characterized by a ‘future unknowable’ (p. 70). Research suggests that there remain constraints imposed on young people in the form of ‘bounded agency’ (Bynner, 2005; Evans, 2007) and this has notably been applied to the experiences of young carers (Hamilton & Adamson, 2013). The excerpts presented here echo these constraints. For young people like the ones whose narratives we have included, rather than having a plethora of choice, their parental health constrains them.
Parental dementia affects young people’s choices, time perspectives and life planning: the condition is ever present. Illness is known to be biographically disruptive (Bury, 1982), and dementia certainly was for our participants (Hall & Sikes, 2018b). Furthermore, young people’s agency was compromised by parental illness, illuminated by the concept of liminality (Turner, 1969), because parents were absent and present. At a broad level, the disruptions and finitude affect young people’s progression through the life course, ‘In transition to adulthood, parents and young people renegotiate their relationships on the basis of voluntarism’ (Brannen, Dodd, & Oakley, 1994, p. 181). However, here, this process of renegotiation was hindered. Young people push for independence (Brannen et al., 1994), but where a parent is ill, the ‘normal’ process is interrupted because they may feel obligated to take on responsibility out of time. This can be experienced positively or negatively. Furthermore, notions of the transition to adulthood being a linear process, in isolation from the family, are questioned, as these data indicate interconnectedness to the family (Morrow, 2013). Additionally, familial relationships pre-illness affect how people feel about the place of their parents in their present and future lives (Hall & Sikes, 2018a).
Parallel to their parent’s illness is the timeline of young people’s own lives. Holstein and Gubrium suggest that the life course is ‘constructed and used as an interpretive resource’ (2007, p. 340). Indeed, findings suggest young people’s wishes and expectations are informed by notions of life course phases. Time is of the essence here: young adulthood is an intense project when there is much to be done. For our participants, parents’ needs also had to be accommodated challenging constructions of youth as a period characterized by opportunities and being carefree. A more flexible approach to the life course is therefore vital (Bhopal, Heptinstall, & Brannen, 2000). Hamilton and Cass’s (2017) research on young carers recommend an age sensitive theory of care giving in formulating support, acknowledging that age, life course phase and gender shape caring experiences, pathways to care and social support. Schoon and Bynner (2010) suggest that there are ‘sensitive periods’ where extra support may be beneficial and Hamilton and Adamson (2013) add that services could ease the constraints on young people during these times. Further research is required that focuses on a more diverse sample in terms of social class and gender in order to ascertain the impact on the life course of men and to specifically explore the material impacts of parental dementia.
Terminal illness is always hard but in the case of this research, having a parent with dementia collides with personal crossroads, and a time associated with endless possibilities becomes bound by dementia. There is little indication of a timeframe, with decline and death the only certainties. And yet, the social support that might be afforded to the conventionally bereaved is lacking for the ‘dual dying’ (Jones & Martinson, 1992) and the concomitant grief characteristic of dementia is rarely acknowledged (Sikes & Hall, 2017). This resonates with Turner’s (1969) ‘betwixt and between’ concept.
Applying life course perspectives to the accounts of children and young people with a parent with dementia can provide valuable information to those in a position to provide support which is lacking. Such support is important given the evidence that experiencing parental dementia when a child or young person has significant health and wellbeing consequences (Svanberg, Spector, & Stott, 2011).
Highlighting the impact of a relatively unique experience, that of parental dementia while individuals are at a comparatively early phase of the life course, demonstrates how important it is not to take a rigid and prescribed approach to the life course. Constructions of childhood, youth and early adulthood are shored up by assumptions as to what these phases of the life course should consist of and these only serve to stigmatize those who do not conform to these.
Footnotes
Acknowledgements
We are grateful to Lauren White for useful feedback on an earlier version of the article.
Funding
This study was undertaken at the University of Sheffield and was funded by Alzheimer’s Society Grant No. R138585.