
Abstract
Scholars have increasingly noted mechanisms by which religion may be detrimental to one’s health, but few have explored how individuals understand linkages between religious involvement and adverse health. Using data gathered from telephone interviews with Protestants and Catholics in North Carolina and South Carolina, we explore how individuals understand the role of religious moral failure in shaping health consequences. When asked to discuss the relationship between religion and health, 23 respondents described experiences or beliefs regarding how failing to meet the expectations of their religion corresponded with a range of reduced mental and physical health outcomes. Findings underscore the need for additional research on the role of religious involvement and life course experiences in shaping expectations that health declines result from moral failure.
Introduction
If you do not carefully observe all the words of this law that are written in this book . . . then the Lord will bring upon you and your descendants extraordinary plagues – great and prolonged plagues – and serious and prolonged sicknesses . . . (Deuteronomy 28: 58–59, emphasis added).
The salutary function of religion is well-documented. Most of the approximately 850 studies exploring the relationship between religion and mental health and the 350 studies examining the link between religion and physical health published during or prior to the year 2000 highlighted strong, recurrent associations between various forms of religiosity and positive health outcomes (Koenig, 2000). By 2012, more than 11,000 studies explored connections between religion and health (most of which, again, evidenced positive relationships) (Koenig et al., 2012). Such associations are robust (resistant to outliers) and multidimensional (indicating that religion is positively associated with health in a variety of ways that impact mental, emotional, and physical health through mechanisms ranging from the social support of fellow congregants to the feelings of peace and comfort derived from prayer). Further, these associations cannot simply be explained away by other factors (as they persist in the presence of a variety of control variables) (Behere et al., 2013; Levin, 1996).
Religion positively impacts mental and physical health directly and mental health indirectly through a variety of mechanisms. Various aspects of religion are associated directly with decreased depressive symptomatology, improved self-rated health, and recovery from mental illness (Wang et al., 2016; George et al., 2000; House et al., 1988; Huijts and Kraaykamp, 2011; Idler, 1987; Koenig et al., 1998a). Indirectly, service attendance may positively influence mental health through perceived social support, increased frequency of in-person and telephone contact with others, and increased social network size (Bradley, 1995; Krause, 2002; Taylor and Chatters, 1988). Religion may also serve as a buffer against life stressors such as cancer, the death of a child or friend, racial discrimination, or financial strain (Salsman et al., 2015; Cole and Pargament, 1999; Eliassen et al., 2005; Ellison et al., 2008; McIntosh et al., 1993; Pargament et al., 2001a; Pargament et al., 1998; Park and Cohen, 1993). Furthermore, religious activity is negatively associated with functional disability and morbidity and positively associated with prolonged survival (Doane and Elliott, 2016; Hummer et al., 1999; Idler, 1987; Klemmack et al., 2007; Koenig, 2000; Koenig et al., 1999; Levin, 1996; Seybold and Hill, 2001). 1
The multitude of persistent and strong positive associations between religion and health demonstrate religion’s potential benefits. However, their ubiquity in the literature has overshadowed the negative health effects associated with religious involvement. A growing body of research indicates religion’s potentially negative impact on health (Hayward and Krause, 2014; Hank and Schaan, 2007; Koenig et al., 2001; Koenig et al., 1998b; Pargament et al., 2001b; Pargament et al., 2000; Strawbridge et al., 1998). For example, religious rituals may encourage group suicide (as in the case of the Jonestown Massacre) (Chidester, 1990) or inspire such actions as the sending off of the dead into water used by adherents for drinking and bathing (as in the case of Hindus along the Ganges River) (Jarvis and Northcott, 1987). Additionally, religious tenets may call for the refusal of blood transfusions, surgery, or other medical interventions, resulting in extensive pain or even death (Ferraro and Albrecht-Jensen, 1991). Events as routine as service attendance can be harmful to one’s health; places of worship which routinely burn incense jeopardize their congregants’ respiratory functioning and may contribute to elevated cord blood IgE levels or allergic contact dermatitis (Lin et al., 2008).
All of the aforementioned examples document direct ways in which physical problems may arise from people adhering to religious practices that nourish the soul but damage the body. However, religion can also indirectly harm physical health through, for example, negative religious coping strategies, or ‘those which reflect an engaging in religious struggle and doubt’ (Zwingmann et al., 2006). Pargament and colleagues (2001b) found that older adults who engage in negative religious coping when faced with an illness (which includes feeling ‘interpersonal religious discontent’ or ‘spiritual discontent’ and ‘questioning God’s powers’) have higher rates of mortality.
Additionally, religion may harm mental and emotional health (Brown et al., 1992). Ellis (1986: 101) argues that ‘people who have a devout belief in dogmatic and damning religions tend to be emotionally disturbed’. Members of religious organizations which espouse that eternal damnation awaits the insufficiently religious may face such emotional disturbance most acutely when they find their faith is faltering despite the potentially dire consequences impending in the afterlife; Krause and Wulff (2004) indicate that, among self-identified religious people, 2 greater religious doubt corresponds with increases in the number of depressive symptoms experienced. Furthermore, negative religious coping is associated with higher levels of depression and an increase in the number of psychological symptoms experienced (Pargament et al., 2001b: 499).
A potentially negative aspect of religion involving health which has not been studied extensively is moral failure, which we define, in this context, as inadequately meeting the expectations of one’s religion. Specifically, we are referring to instances in which self-identified religious people associate failure to maintain sufficient belief in or connection with a deity, violating religious beliefs or doctrine, or failure to properly observe religious practices (such as failure to attend services or pray regularly) with diminished health. Sloan et al., (1999) suggest that self-identified religious people may attribute their health problems to their own moral failures. However, this claim currently lacks empirical justification.
The assumption that moral failure leads to diminished health has heretofore been largely unexplored. Thus, using interview data from self-identified religious people (including clergy, health ministry program leaders, and laity drawn from congregations in North and South Carolina) we ask: do self-identified Christians believe that religiously-based moral failure negatively impacts health? In this way, we expand the literature on the connection between religion and health and contribute to the literature on moral failure by more directly and empirically addressing moral failure within the context of religion.
Literature review
Historical uses of moral failure
Scholars have conceptualized moral failure in a variety of ways and applied it in multifarious contexts. 3 At the macro-level, moral failure has served as a descriptor for such occurrences as nations’ inattention to genocide or oppression in other countries, the continued existence of patriarchy in the United States, and declines in the quality of undergraduate teaching (Sharp, 1993; Watson, 1990; Winston, 1994). At the micro-level, moral failure is frequently presented as disconnection between personal circumstances over which a given person is assumed to have some control and societal norms. For example, people with excessive body weight and people with addictions to controlled substances are often blamed for these issues and presumed to be morally failing regardless of the extent to which environmental or societal factors may be responsible. The assumption that making better choices would prevent or reverse obesity and addiction is common; as Richard Erickson (1982: 121) argues, ‘Patients who “take the first drink” or do not take needed medications or refuse to come in for treatment are seldom if ever helped if we declare these acts an expression of “their illness”. People are responsible for the decisions they make, at least for the course of action they undertake’. People living with mental disorders face similar scrutiny for their supposed moral failure (Pride, 1999). Victims of such assumptions may then internalize this scrutiny, leading to psychological harm (Sowers, 1998; Townend, 2009; Wray and Deery, 2008).
The same manifestations of moral failure occur in a religious context but bring to bear the added weight of potential divine condemnation. Regarding moral failure within the context of religion, actions such as alcohol abuse may be characterized as not only counter-normative but also sinful (Petrunik, 1972). Ephesians 5:18 carries such a sentiment in stating, ‘Do not get drunk on wine, which leads to debauchery’ (Radmacher et al. 1997). Beyond action, Koenig and colleagues (1999:129) indicate that moral failure may also pertain to mental adherence; specifically, they present ‘insufficient faith’ as synonymous with moral failure in their characterization of Sloan and colleagues’ concerns that ‘if religion is suggested as a possible road to better health, people may begin to see illness as a result of insufficient faith or moral failure’. Indeed, research expanding on attachment theory (which conceptualizes God as a ‘parental attachment figure’) indicates that ‘anxious attachment’ (feeling insecure in one’s relationship with God) is associated with negative affect (Bradshaw et al., 2010). Further, belief in a punitive God is associated with several psychiatric symptoms, including social anxiety, depression, obsession, and paranoia (Silton et al., 2014). We expand on these concerns about the potentially negative health effects of a troubled relationship with God to examine the extent to which self-identified Christians consider moral failure (which encompasses both inadequate religious belief and practice) to negatively impact health.
Scholarly concerns about belief in a connection between moral failure and diminished health
Exposure to research findings may lead religious people to attribute a health advantage to religious activity (Frenk et al., 2011). Social scientific findings indicate a robust association between religious involvement and overcoming or avoiding mental health problems (George et al., 2000; House et al., 1988; Idler, 1987; Koenig et al., 1998a) and improving physical health (Powell et al., 2003). The emergence of belief in a health differential based on degree of religious adherence has raised concerns among scholars; Sloan and colleagues (1999: 666) decry beliefs ‘within any individual religion [according to which]…the more devout adherents [are] “better” people, more deserving of health than others…’, going so far as to compare such beliefs to ‘now discredited research suggesting that different ethnic groups show differing levels of moral probity, intelligence, or other measures of social worth’. Sloan and colleagues then suggest that studies linking religion to positive health effects may be unintentionally harming religious people who view their own health problems as resulting from insufficient religiosity (Sloan, 2008; Sloan et al., 1999).
Neither Sloan and colleagues (1999) nor Koenig and colleagues (2001) empirically address whether religious people actually do harbor beliefs involving the connection between moral failure and health problems or explore their substantive character, making it difficult to ascertain the extent to which concern over such beliefs is warranted. To address this evidence gap, we present a pilot study investigating Christian experiences of and belief in a connection between moral failure and diminished health.
Methods
Data
Data for this study come from the 2004–2005 Caring Communities Health Ministries Program Assessment, which evaluated the effectiveness of health ministry programs in North and South Carolinian congregations and is supported through funding from the Duke Endowment. The Duke Endowment is a private foundation that is unaffiliated with Duke University and supports education, healthcare, children’s healthcare, and spiritual programs in North and South Carolina. Health ministry programs include a wide array of health-related programs meant to serve congregations as well as people in congregations’ surrounding communities including weight loss classes, preventative medical care, and health fairs (often under the leadership of parish nurses). Researchers drew a convenience sample of thirty-seven congregations from a list of congregations which had received funds from the Duke Endowment and sent each congregation a cover letter and a letter of endorsement from the Duke Endowment specifying the purpose of the assessment. A week later, the researchers contacted the congregations’ clergy to determine their willingness to participate in the study.
Twenty-five clergy agreed to participate in the study and were subsequently mailed questionnaires. After they returned the questionnaires, clergy participated in a semi-structured telephone interview with a member of the research team that lasted approximately thirty minutes. Upon agreeing to participate in the study, clergy provided contact information for their health ministry coordinator and/or their health program leaders. The researchers administered questionnaires to the health coordinators and program leaders and conducted 30-minute semi-structured telephone interviews with them. The mailed questionnaires that clergy completed asked for the names of two ‘recruiters’ who would provide contact information for church members. Researchers contacted twenty members of congregations with fewer than 200 members and 10% of the members of congregations with more than 200 members for 30-minute semi-structured telephone interviews. 4 Members of the research team transcribed the interviews, obtaining complete data for 700 respondents, including 22 clergy, 139 health coordinators/health ministry program leaders, and 539 lay members from the 37 congregations. Researchers allowed respondents to interpret terms on their own and answer accordingly without clarification.
Respondents reported their age, race, marital status, education, congregational role, and denominational affiliation, and frequency of religious attendance. We use the scheme devised by Steensland and colleagues (2000) to classify respondents’ religious preferences. Table 1 reports descriptive sociodemographic characteristics for all respondents. Respondents’ mean age is 59, and the sample consists primarily of female, white, married, well-educated, lay members of mainline Protestant congregations who attend religious services at least weekly. 75% of respondents are women, 95% are white, and 76% are married. 19% of respondents received a high school education or less, 26% completed some college but have not received a bachelor’s degree, 35% received a bachelor’s degree, and 21% received a graduate degree. 5 Additionally, 3% are clergy members, 20% are health ministry program leaders or coordinators, and 77% are lay members of a congregation. 63% attend mainline Protestant congregations, 26% attend conservative Protestant congregations, and 11% attend Catholic congregations. Fewer than 1% of respondents attend religious services several times a year or less, 3% attend monthly, 63% attend weekly, and 33% attend more than once per week.
Descriptive statistics for caring communities’ respondents (n = 700).
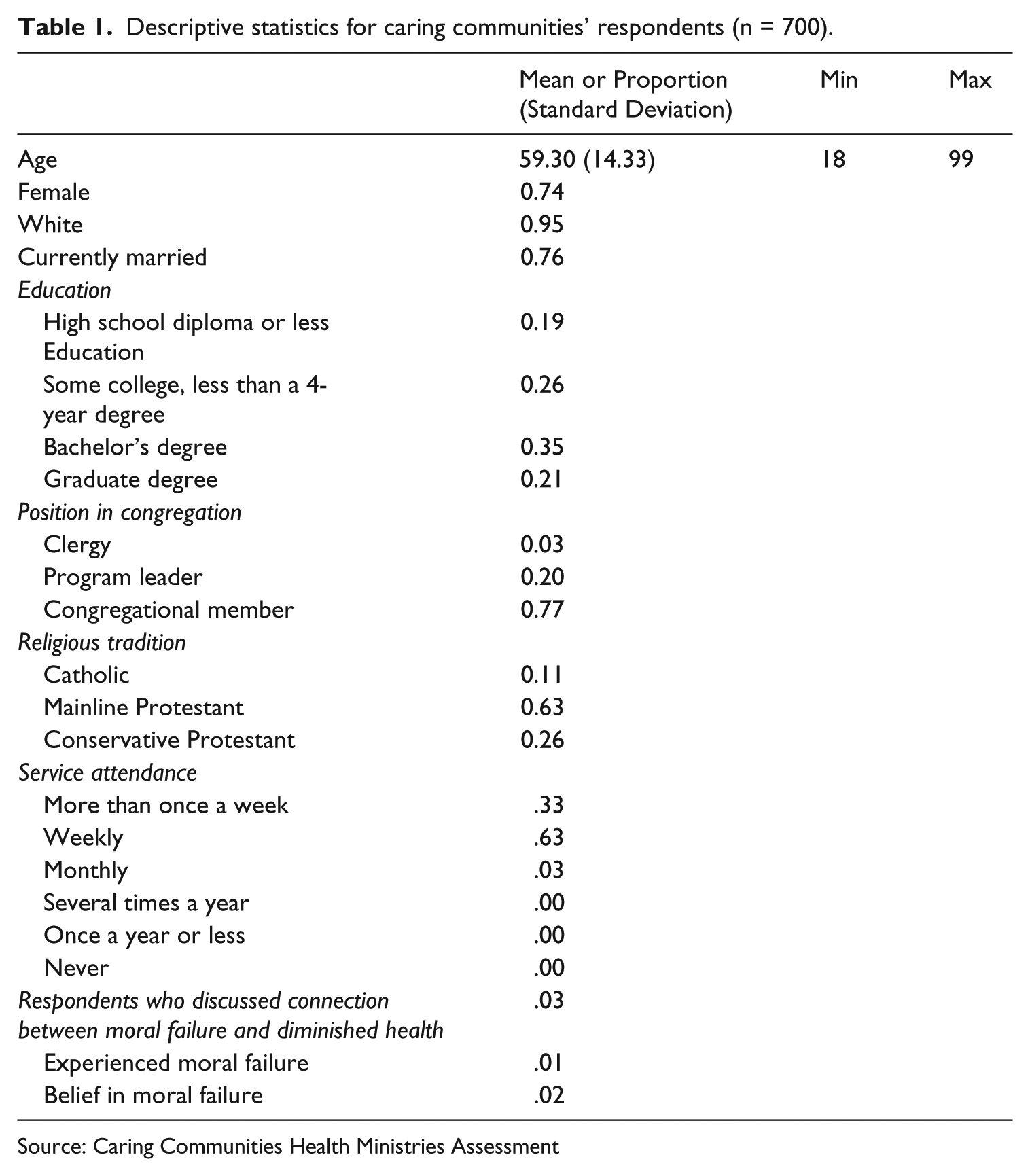
Source: Caring Communities Health Ministries Assessment
Coding strategy and selection of key cases
We selected the subset of cases linking moral failure to health for the present study. Due to the sampling frame of the Caring Communities Health Ministries Program Assessment and the general terms in which respondents were asked about the connection between religious belief and health, these cases provide a logical starting-point for an inductive inquiry into how moral failure is understood in the relationship between religion and health.
Interviewers asked respondents, ‘Do you think your religious beliefs affect your health?’ After giving an initial response to the question (yes or no), respondents were asked to elaborate. These responses were coded to reveal themes including whether respondents suggested that moral failure had led or would lead to diminished health. Responses were coded as suggesting a connection between moral failure and health if a respondent: 1) described personally experiencing or witnessing others experience diminished health after failing to maintain sufficient religious belief in or a personal connection with a deity, violating religious beliefs or doctrine, or failing to properly observe religious practices; or 2) expressed belief in a connection between such examples of moral failure and health without indication of specific personal experience.
Twenty-three respondents expressed that not only do religious beliefs positively affect health, but also adverse health consequences follow from failure to adhere to religious teachings, beliefs, and practices. The present study focuses on these 23 cases to shed light on the range of ways in which moral failure is linked to adverse health. Among these respondents, ten indicated that they had experienced a connection between moral failure and health, while thirteen indicated that they believed in a connection between moral failure and health but did not describe any relevant personal experiences. Table 2 provides characteristics of these 23 key cases.
Respondents expressing belief in the connection between moral failure and adverse health (n=23).
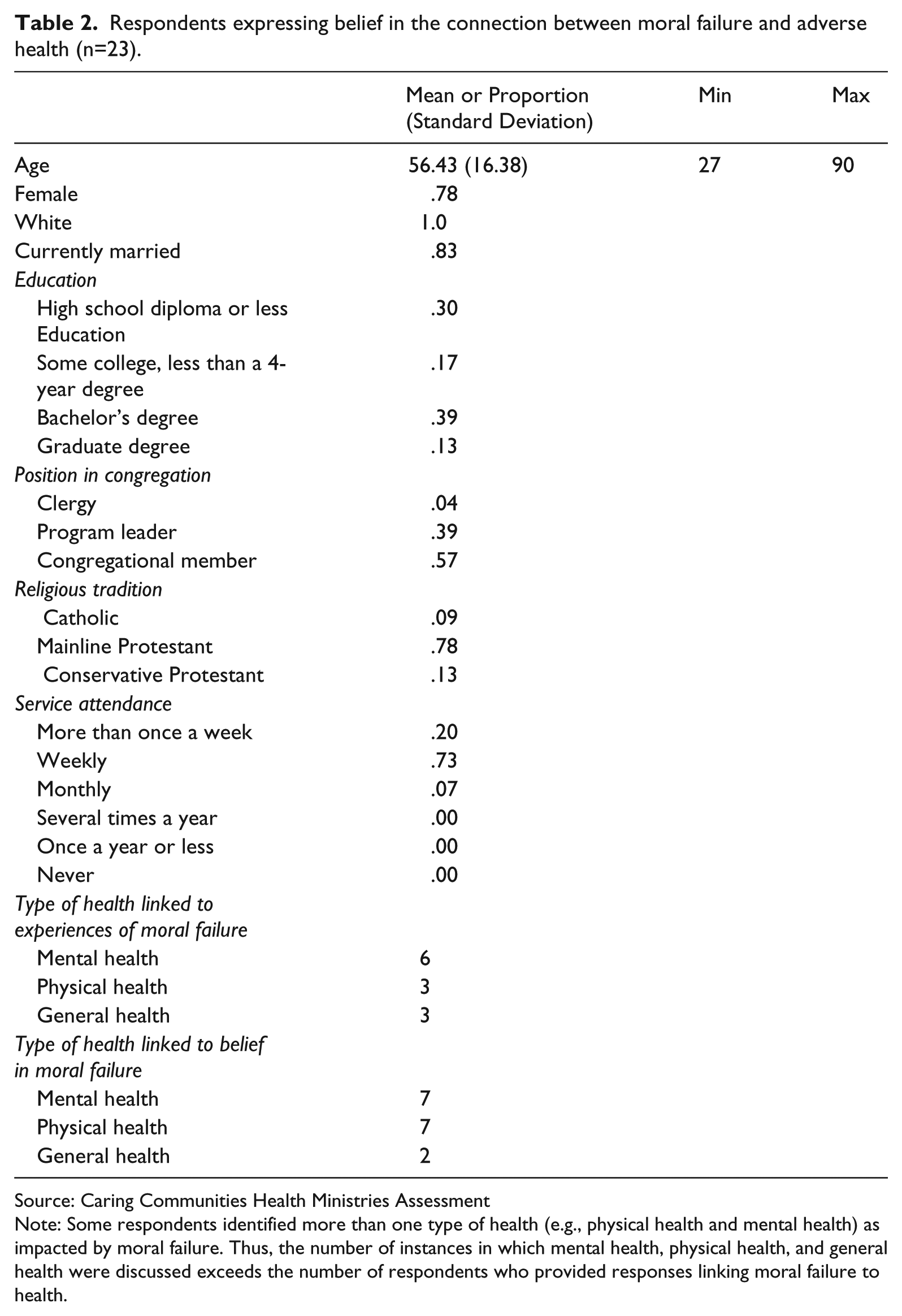
Source: Caring Communities Health Ministries Assessment
Note: Some respondents identified more than one type of health (e.g., physical health and mental health) as impacted by moral failure. Thus, the number of instances in which mental health, physical health, and general health were discussed exceeds the number of respondents who provided responses linking moral failure to health.
These cases reveal a range of religious belief, experiences, and practices in the pathways by which moral failure is understood to precede health decline. We also noted the types of health (mental, physical, or general) described as declining following moral failure in religious belief, experience, or practice. Respondents provided general remarks regarding mental health and specific mentions of depression, desire to live, ability to cope with everyday challenges, and stress level, which were also coded as mental health. Respondents mentioned physical health in general terms, and specific references to fluctuations in pain, delayed or expedited mortality, improved or impeded immune system functioning, and differential engagement in preventative care (such as exercising, eating healthily, or avoiding excessive alcohol intake) were also coded as physical health. Remaining non-specific remarks pertaining to health in general without specifying mental or physical health were coded as ‘general health’. Among respondents describing experiences of moral failure preceding a decline in health, six discussed mental health, three discussed physical health, and three discussed general (unspecified) health. Among respondents suggesting belief in (but not personal experience with) a connection between moral failure and health, seven discussed physical health, seven discussed mental health, and two discussed general (unspecified) health.
Results
Among respondents describing experiences of moral failure preceding a decline in health, four discussed having an insufficiently close relationship with a higher power, four discussed failing to attend church regularly, two discussed exhibiting insufficient faith or belief, one discussed lack of obedience to a deity, and one discussed participating in church ministries that violated personal religious beliefs.
Experiences of a connection between moral failure and health
Approximately one percent of respondents described experiences they had with moral failure and negative health effects or examples of when they witnessed others having such experiences. Respondents in this category most frequently discussed moral failure in the context of having an insufficiently close relationship with a higher power or failing to attend church regularly. Incorporating both of these themes, Tom, a white, 66-year-old Presbyterian program leader said, My sense of well-being is based on whether I go to church or not and if I don’t know how my relationship with God is, there was a time when I didn’t have a close relationship and it shows in my demeanor and attitude and a person can’t be healthy unless your spiritual health is just as important as your physical health.
Two respondents discussed the health effects of exhibiting insufficient faith or belief. Simultaneously addressing this and other themes, Cassidy, a white, 30-year-old Methodist member noted, I have learned, and I’m learning that if something’s not right, if I’m not there with my faith, if it’s been awhile since I’ve led a devotion or really, really gotten connected with God through prayer something is just not right and I seriously get depressed.
Jessica, a white, 27-year-old Presbyterian member cited lack of obedience, saying: . . . we all sin and I find myself . . . that if I’ve been especially ‘bad’ that week or if I have done something that I’m not so proud of and God wouldn’t be proud of, I just feel bad.
Finally, Sandra, a white, 62-year-old Methodist pastor suggested that serving in a church that violated her personal religious beliefs led to her physically losing her voice. As she described, I think your world view and your view of God directly effects every cell, every breath, and every electrical movement in your being . . . And I know that in my body because I, I got my call to ministry because I lost my voice. And I could not sing. And the reason I could not sing had nothing to do with the anything wrong with the mechanism. It had to do with the fact that I could not sing a sexist hymn another bit in my life. And I could not exist another day in a sexist church. And when I got my voice – because in the church where I worked, as a minister of music that time, the belief was women don’t, aren’t called to ministry. But I was doing music for ten years in that place, and so women had not choice, or voice in the church. I had no voice and I lost it . . .
Belief in a connection between moral failure and health
Among respondents suggesting belief in (but not personal experience with) a connection between moral failure and health, five cited lack of obedience, five cited having an insufficiently close relationship with a higher power, two cited exhibiting insufficient faith/belief, and one cited having an insufficiently strong spiritual life. Respondents in this category most frequently focused on lack of obedience and having an insufficiently close relationship with a higher power as leading to negative health effects. Descriptions of lack of obedience ranged from failing to adhere to guidelines pertaining to health behaviors to failing to forgive others. Sam, a white, 64-year-old Methodist program leader), discussed how ‘If you read the Bible making your body a temple and what you put in your body, if you put trash in, you’re going to get trash . . . ’ Delores, a white, 90-year-old Methodist member, explained that You can tear yourself up, if they hurt you and if you carry that on, you are not hurting the other person. You are hurting yourself. In the Lord ’s Prayer, if you are to be forgiven, you have to forgive.
Regarding having an insufficiently close relationship with a higher power, Casey, a gender-unidentified 41-year-old Methodist member suggested that . . . if you don’t put God first in your life, it is so easy to slip into bad habits that [are] hard on your body. Like going to bars and drinking and smoking and that sort of thing.
Two respondents focused on insufficient faith/belief. One of these respondents was Betty, a white, 62-year-old Methodist member who offered: ‘I think that not having good religious beliefs can create weakness which would affect you physically’. Finally, one respondent (Trudy, a white, 68-year-old Methodist program leader) cited having an insufficiently strong spiritual life, discussing how patients in hospice care without a strong spiritual life were ‘sort of floundering’ and had difficulty coping with their physical health problems.
Discussion
Findings reveal a range of beliefs and experiences in the connection between religious moral failure and adverse health. These results go beyond previous religion and health studies to suggest that religious involvement may not only be perceived to be positively associated with health, but that failure to maintain a subjectively-determined sufficient level of religiosity can lead to perceptions of negative health effects.
Respondents who expressed convictions in the causal link between religious moral failure and adverse health typically described religious moral failure as inadequate maintenance of a close relationship with a higher power. However, those who drew on specific experiences in their lives also often focused on failure to attend church services regularly while those with beliefs detached from specific experiences focused more on general lack of obedience to God or Biblical precepts. Respondents associated moral failure with a variety of health outcomes ranging from general health (e.g., feeling bad overall) to mental health (e.g., depression or anxiety) and physical health (e.g., getting migraine headaches).
Limitations and directions for future research
While these findings are useful to elucidate experiences of and belief in a connection between moral failure and diminished health, they are subject to certain caveats. The question wording’s focus on religious belief likely resulted in less discussion of other forms of religiosity than would occur otherwise. Given that the sample only included Christians, conclusions from this study may differ from those drawn from other religious groups. Relatedly, the sample is neither representative of the American population at large nor of people who consider themselves religious adults in the U.S., as respondents were relatively high in age and education and predominantly white, female, and Protestant. Additionally, there are no measures of socio-economic status beyond level of education for the sample. Further, the data does not include the insurance status of these respondents, limiting understanding of their access to health care, which may affect their beliefs in the connection between religion and health (Maitra, 2010; McAlpine and Mechanic, 2000). However, given that we rely on spontaneous responses (rather than answers to a direct question about the connection between moral failure and health), it is possible that at least some of the respondents who did not reveal belief in a connection between moral failure and diminished health would have done so had they been directly asked whether they believed that less religious people experience worse health than more religious people. Therefore, this study may provide a rather conservative estimate regarding the commonality of this belief. This study should not be taken as an estimate of the prevalence of beliefs in a connection between moral failure and health among Christians in America. Future studies should explore the extent to which these beliefs are held by diverse religious groups in a variety of sociodemographic contexts.
It is also unclear from the data whether those who express belief in a connection between moral failure and health explicitly blame themselves. Even outside of a religious context, self-blame for illness is not uncommon; researchers have documented self-blame on the part of mothers of infants with perinatal problems (Tennen et al., 1986), women with breast cancer (Taylor et al., 1984), and people living with HIV/AIDS (Mak et al., 2007). It is possible that respondents who expressed acceptance of a connection between moral failure and health could blame themselves for their health problems as well if they saw those health problems as resulting from their failure to meet religious expectations. Although explicit self-blame was uncommon in our sample, certain respondents said things that indicated the potential for self-blame, such as one respondent’s comment that ‘we all sin, and I find myself . . . that if I’ve been especially “bad” that week or if I have done something that I’m not so proud of and God wouldn’t be proud of, I just feel bad’.
If some of those who believe in a connection between moral failure and diminished health might blame themselves, another possibility warranting investigation is whether they might also see others they deem inadequately religious as responsible for their own health problems. Sloan and colleagues (Sloan, 2008; Sloan et al., 1999) raise the possibility that religious people might see devout adherents as more deserving of health than others. Although one respondent did suggest that other Christians she knew experienced poorer health because they ‘don’t believe as much as I do’ or ‘are as close to God [as I am],’ we found little evidence to support blame for others resulting from beliefs in the connection between moral failure and health. Moreover, attempting to directly tie belief in the connection between moral failure and diminished health to self-blame or blame of others should be approached with caution. As noted by Chaves (2010), belief is not always consistently tied to behavior or subsequent belief, and attempts to frame such connections as stagnant and absolute result in the commission of the ‘religious congruence fallacy’.
Conclusion
These findings extend empirical analyses of moral failure to the context of religion and, in so doing, add to existing research on connections between religion and health by illuminating the ways in which religious people on the ground conceptualize the potential health pitfalls attendant to insufficient religiosity. A number of previous studies indicate that religious involvement can positively influence health such that, by extension, those who are not religious or are less religious may receive fewer health benefits (Koenig et al., 2012). However, those who are not religious or who are less religious may be receiving forms of social, emotional, and material support in other contexts that enable them to maintain good health despite a lack of active involvement in religion. Thus, saying that less religious people experience fewer health benefits from religion is not the same as suggesting that religious people perceive an explicit penalty to declining in religious involvement. Our study addresses this nuance.
The consequences of belief in a connection between moral failure and health remain insufficiently specified. Although our results do not appear to explicitly confirm concerns that belief in moral failure impacting health will lead to self-blame or other-blame for sickness, more targeted questions are needed to assess whether holding such a belief results in self-blame. It is also important to determine whether harboring such belief results in diminished mental health through self-blame. In general, our discovery of respondents who discussed a connection between moral failure and diminished health necessitates further quantitative and qualitative research to unpack both the factors which lead religious people to view religiously-based moral failure as leading to health problems and the results of such views.
Footnotes
Acknowledgements
The authors would like to thank Keith Meador, Whitney Arroyave, and Alexis Franzese for their assistance with the Caring Communities Health Ministries Assessment Project, and Steven Frenk, Linda George, Mark Chaves, and Edward Tiryakian for reviewing earlier versions of the manuscript. The authors thank the clergy, congregation members, and program leaders who participated in the study. The content of this article is solely the responsibility of the authors and does not reflect the views or opinions of The Duke Endowment. Finally, the authors would like to thank the Duke Endowment for financial support of the Caring Communities Health Ministries Assessment from which these data are drawn.
Notes
Author biographies
Email:
Address: Department of Sociology and Anthropology, SBSC 344, 1201 W. University Dr., Edinburg, TX 78539 USA.
Email:
Address: Social Science Research Institute, Duke University, 140 Science Drive, Durham, NC 27708, USA.