
Abstract
Introduction
Obesity is associated with an increased risk of colorectal cancer (CRC). Unlike the indirect measures such as BMI, CT-Body composition (CT-BC) allows for the assessment of both volume and distribution of adipose tissue. Therefore, the aim of this study was to examine the relationship between host characteristics, BMI, CT-BC measurements and the incidence of colorectal neoplasia.
Methods
Patients undergoing CT Colonography (CTC) as part of the Scottish Bowel Screening Programme, between July 2009 and February 2016, were eligible for inclusion. Data were collected including demographic data, clinicopathological variables and CT-BC measurements including skeletal muscle index (SMI), subcutaneous fat index (SFI) and visceral fat area (VFA). CTC, colonoscopy, and pathology reports were used to identify CRC incidence. Associations between demographic data, clinicopathological variables, CT-BC measurements, colorectal neoplasia and advanced colorectal neoplasia were analysed using univariate and multivariate binary logistics regression.
Results
286 patients met the inclusion criteria. Neoplasia was detected in 105 (37%) of the patients with advanced neoplasia being detected in 72 (69%) of patients. On multivariate analysis sex (p < 0.05) and high VFA (p < 0.001) remained independently associated with colorectal neoplasia. On multivariate analysis a high SFI (p < 0.01) remained independently associated with advanced colorectal neoplasia. BMI was not associated with either colorectal neoplasia or advanced colorectal neoplasia.
Conclusion
When directly compared to BMI, CT derived fat measurements were more closely associated with the degree of neoplasia in patients undergoing colorectal cancer screening. In patients investigated with CT colonography, CT adipose measures may stratify the risk and grade of neoplasia.
Keywords
Introduction
The obesity pandemic has become an increasing public health concern, particularly in western society. 1 Furthermore, obesity is an established, preventable cause of cancer.2,3 Studies have shown that an elevated body mass index (BMI), is associated with an increased risk of colorectal cancer (CRC).4–7 Other surrogate markers of obesity including waist circumference and waist: hip ratio have also been shown to be associated with an increased risk of colorectal cancer.8,9 However, BMI, waist: hip ratio and waist circumference are not direct measures of adiposity or its distribution. 4
CT-derived Body composition (CT-BC) has garnered considerable interest with regards to its utility in predicting outcome in patients with established cancer.10,11 Unlike the indirect measures of body fat, CT-BC allows for the assessment of both the volume and distribution of soft tissues including muscle and fat. Specifically, body fat can be divided into subcutaneous adipose tissue, which is located below the skin in the hypodermis, and visceral adipose tissue, the intra-peritoneal fat surrounding the abdominal organs.12,13 Elevated levels of visceral adipose tissue have been associated with worse oncological and survival outcomes in those with colorectal cancer.14–16
The majority of CRC are believed to arise within colorectal adenomas, as a result of the adenoma-carcinoma sequence.17,18 Obesity, (as defined by an elevated BMI), has been associated with colorectal adenoma incidence, with several meta-analyses demonstrating a positive but inconsistent correlation between the two.5–7 Furthermore, studies have shown that increased visceral adipose tissue is also associated with an increased incidence of CRC.19–21 Although the current literature suggests that obesity is directly related to the incidence of colorectal neoplasia, the exact mechanism remains unclear.
Cancer cachexia is a multifactorial syndrome associated with a loss of weight and skeletal muscle mass as the disease progresses. 22 In addition to the assessment of adipose tissue, CT-BC allows for the measurement of skeletal muscle volume and radiodensity. There is evidence that the loss of skeletal muscle tissue is an independent prognostic factor for both cancer-specific and overall survival in patients with CRC.23,24 However, there is little evidence pertaining to the role of sarcopenia in the early or pre-malignant stage of CRC.
The present study proposed that body composition, in particular adipose tissue distribution, rather than overall adiposity (according to BMI) is an enhanced method with which to study the relationship between adiposity and colorectal neoplasia. Therefore, the aim of this study was to examine the relationship between BMI, CT-BC and the incidence of colorectal neoplasia in a bowel screening population.
Patients and methods
Study design and population
Patients undergoing CT Colonography as part of the Scottish Bowel Screening Programme in NHS GGC, between July 2009 and February 2016, were eligible for inclusion. All population members aged between 50–74 years, in Scotland, are invited to take part in the Scottish Bowel Screening Programme. 25 Patients with co-morbid disease, advanced age, deemed too frail to undergo colonoscopy, and those in whom colonoscopy is incomplete, are offered CT Colonography (CTC) as an alternative. The primary study endpoints were the incidence of any histologically confirmed colorectal neoplasia and any advanced colorectal neoplasia (advanced adenoma or adenocarcinoma), as part of the bowel screening process.
Data collection
Patients underwent thorough colonic investigation by CT Colonography as a minimum, and in most cases, an additional colonoscopy or flexible sigmoidoscopy was carried out either before or after. Following CT Colonography, patients with suspected colorectal polyps or carcinoma underwent a colonoscopy to remove, biopsy, or clarify the findings on imaging. Age, sex, smoking status, BMI and other demographic data were obtained from medical records. Patients were allocated into one of four groups according to the WHO classification for BMI: underweight (BMI <18.5), normal weight (BMI 18.5–24.9), overweight (BMI 25–29.9) and obese (BMI ≥30). 26
Colonoscopy and pathology reports for each patient were reviewed to collect data on the number, size, and histopathological subtypes of colorectal neoplasia. Colorectal neoplasia was defined as either an adenomatous polyp of any subtype or invasive colorectal carcinoma. Advanced colorectal neoplasia was defined as either an advanced adenoma (at least one of; adenoma size ≥1 cm, villous histology, high grade dysplasia (HGD)) or adenocarcinoma. In patients who had undergone colonoscopy before and after CT Colonography, the results from all three tests were combined to give an overall outcome.
CT- body composition
CT images were obtained at the level of the third lumbar vertebra as previously described. 27 Scans with significant movement artefact or missing region of interest were not considered for inclusion. Each image was analysed using a free-ware program (NIH Image J version 1.46, http://rsbweb.nih.gov/ij/) shown to provide reliable measurements. 28
Region of interest (ROI) measurements were made of total fat (TFA), visceral fat (VFA), subcutaneous fat (SFA), and skeletal muscle areas (SMA) (cm2) using standard Hounsfield Unit (HU) ranges (adipose tissue −190 to −30, and skeletal muscle −29 to +150). The SFA and SMA were then normalised for height2 to create indices; subcutaneous fat index (SFI, cm2/m2), and skeletal muscle index (SMI, cm2/m2).
A high VFA was defined as an area >160cm2 for male patients and >80cm2 for female patients according to established thresholds. 13 A high SFI was defined as ≥50 cm2m2 in men and ≥42 cm2m2 in women using thresholds defined by Ebadi et al. 12 A low SMI was defined as an SMI <45.6 cm2m2 (if BMI≤30) or SMI <56.8 cm2m2 (if BMI >30) in male patients and SMI <39.1 cm2m2 (if BMI ≤30) or SMI <44.6 cm2m2 (if BMI >30) in female patients, as described by Dolan and colleagues.29,30
Statistical analysis
Demographic data, clinicopathological variables and CT-BC measurements were presented as categorical variables. Categorical variables were analysed using χ2 test for linear-by-linear association.
Associations between demographic data, clinicopathological variables, CT-BC measurements, colorectal neoplasia and advanced colorectal neoplasia were analysed using univariate and multivariate binary logistics regression with a backward conditional approach. A p < 0.1 was applied to inclusion at each step in the multivariate analysis.
Missing data were excluded from analysis on a variable-by-variable basis. A two-tailed p-value <0.05 was considered statistically significant in this study. All statistical analyses were carried out using IBM SPSS statistics version 24.0, IBM Co, Armonk, NY, USA.
Results
Study group characteristics
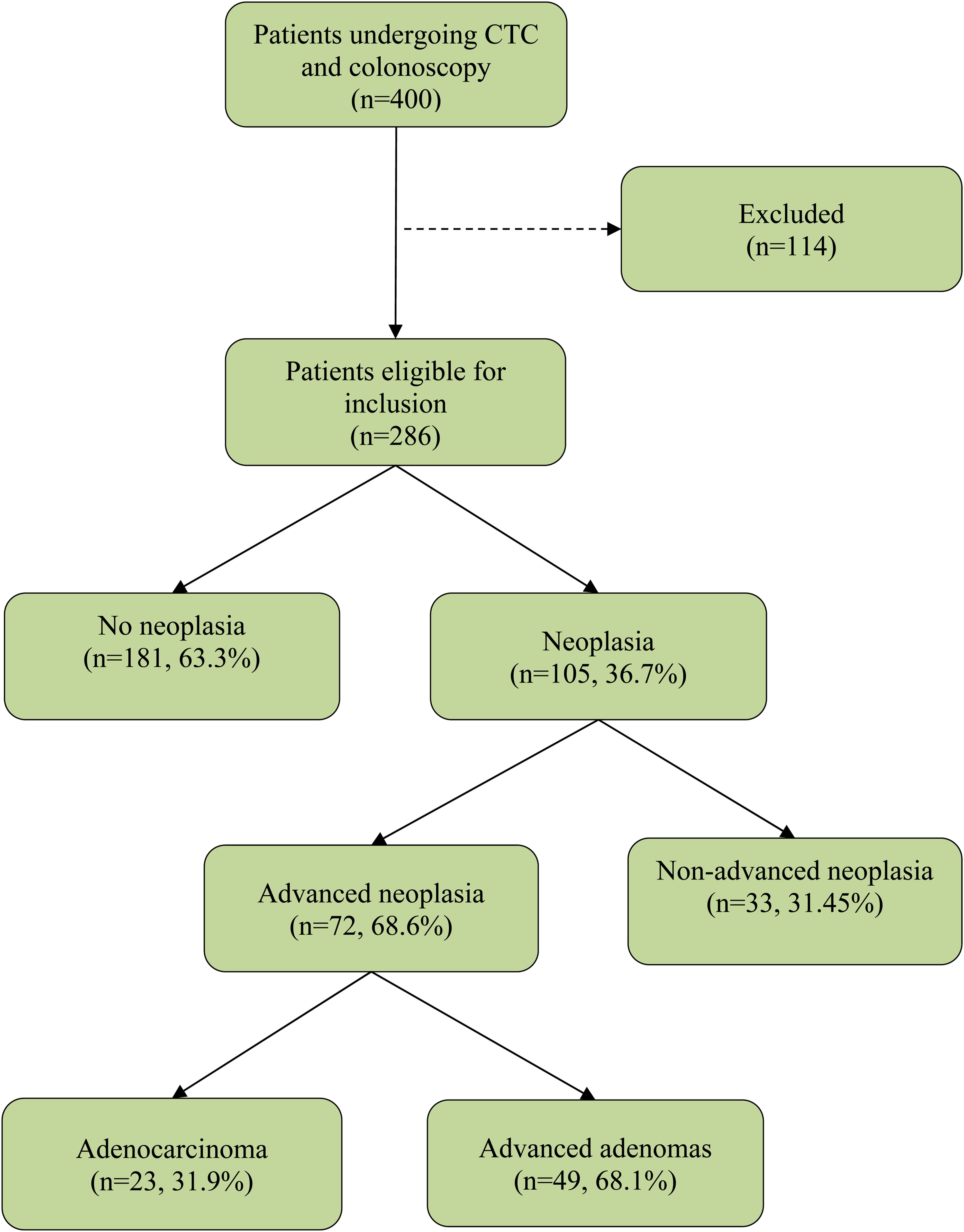
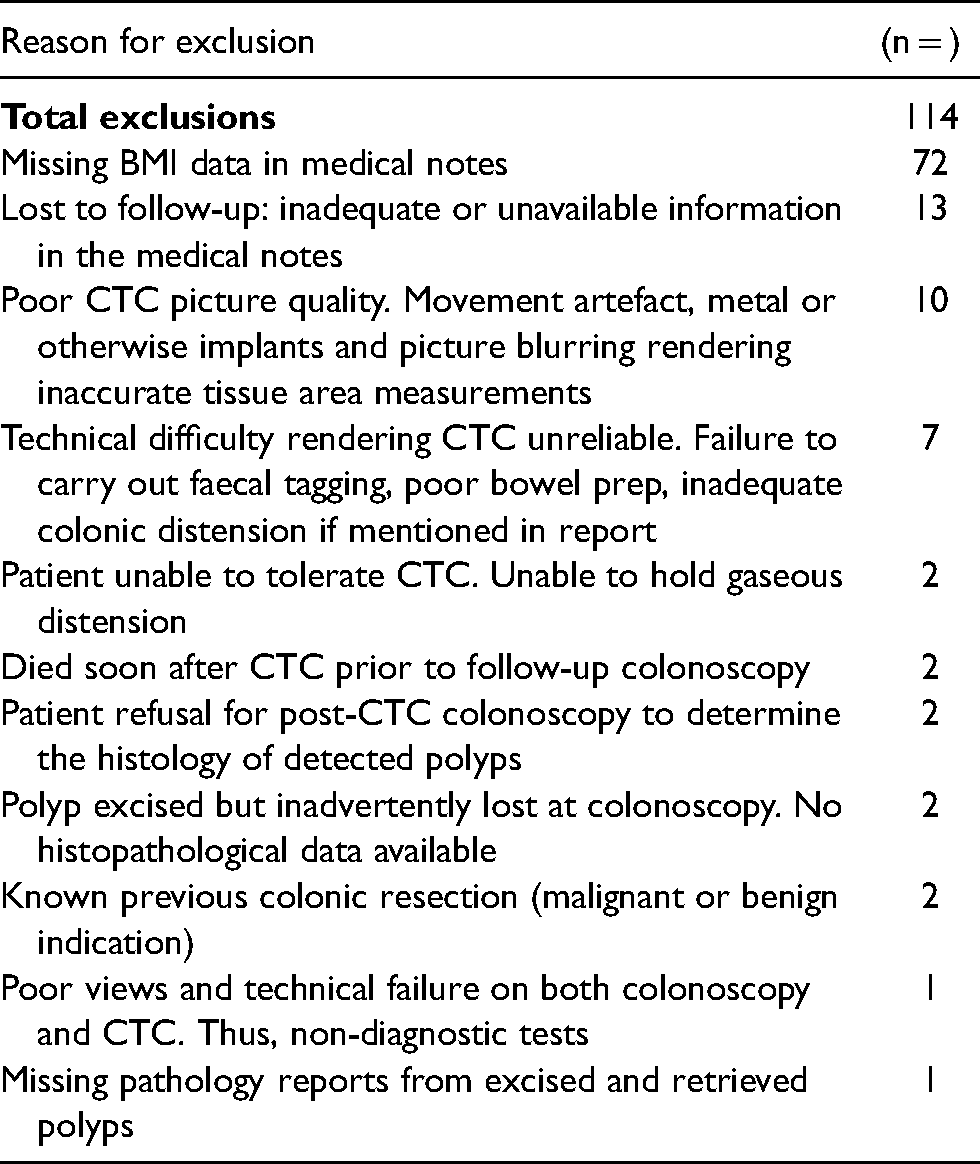
Between July 2009 and February 2016, 400 patients underwent CT Colonography following a positive screening test as part of the Scottish Bowel Screening Programme (Figure 1). Eighty-nine (22%) were allocated directly, while 311 (78%) underwent CT Colonography due to incomplete colonoscopy. One hundred and fourteen (29%) patients were excluded from the study
Outcomes following colonoscopy and CT colonography.
Reasons for exclusion from the study.
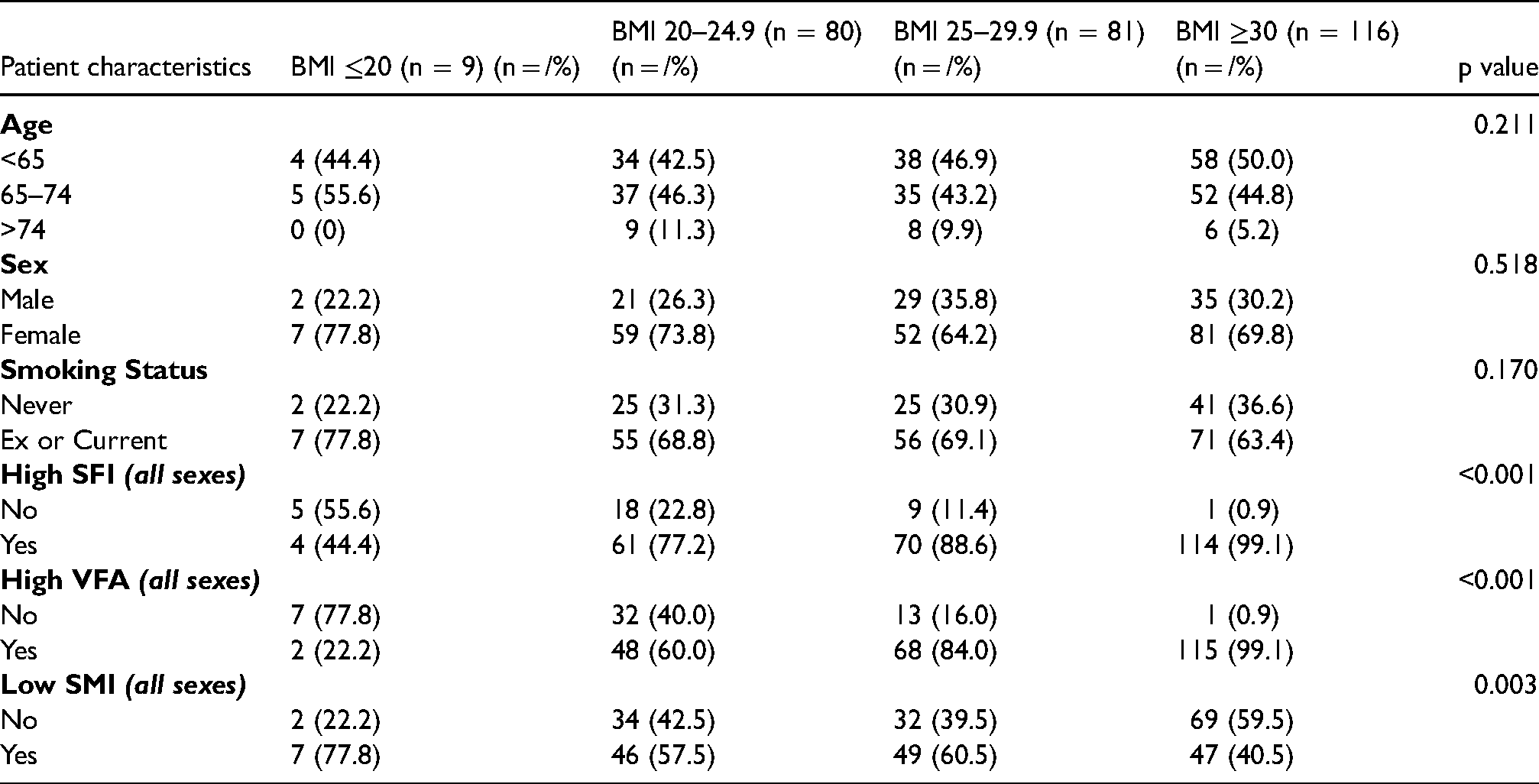
Patient characteristics stratified by BMI (n = 286).
Study outcomes
The study outcomes are displayed in Figure 3. Of the 286 patients included, 105 (37%) were diagnosed with colorectal neoplasia. Among these, 72 (69%) had advanced neoplasia. Of those with advanced neoplasia, 23 (32%) had adenocarcinoma, and 49 (68%) had an advanced adenoma (in the absence of CRC).
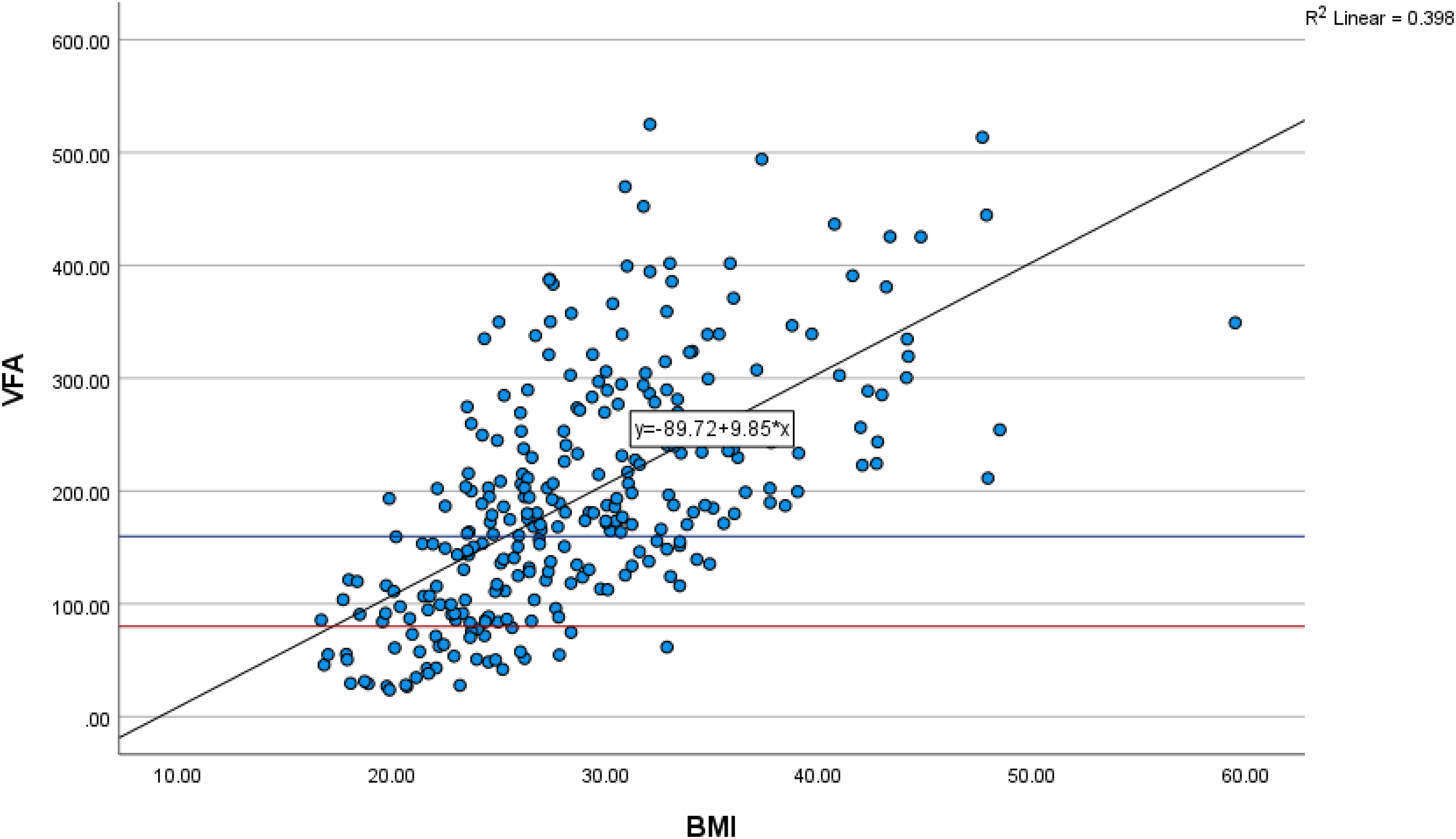
The relationship between BMI and VFA in those with undergoing CT colonography. N.B. Blue and red lines indicate thresholds of VFA for males and females respectively.
The relationship between BMI, SFA and VFA in those with undergoing CT colonography
BMI was positively associated with SFI (r2 = 0.478, p < 0.001, See Figure 2) and VFA (r2 = 0.398, p < 0.001, See Figure 3). SFI was positively associated with VFA (r2 = 0.106, p < 0.001, See Figure 4).
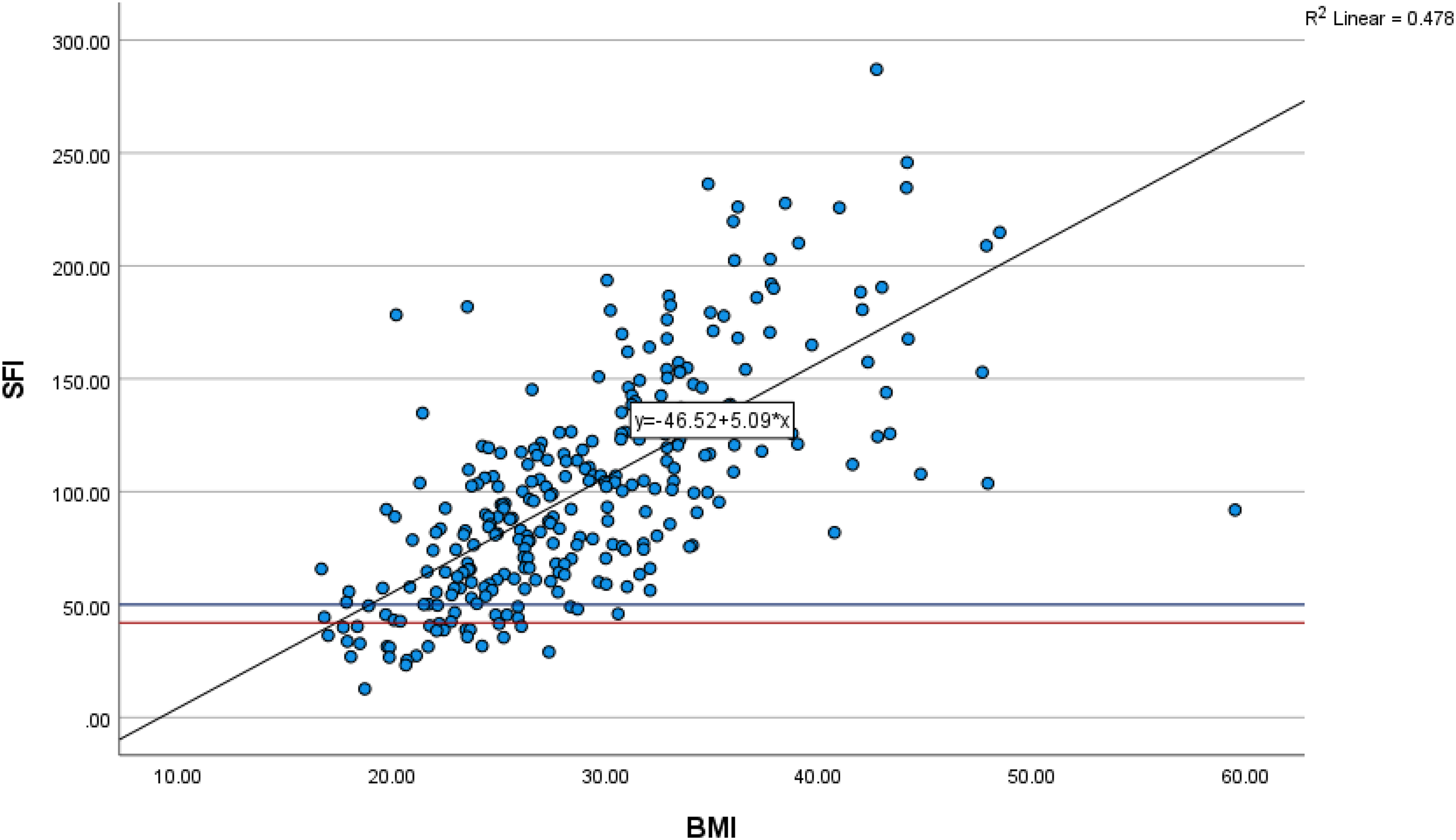
The relationship between BMI and SFI in those with undergoing CT colonography. N.B. Blue and red lines indicate thresholds of SFI for males and females respectively.
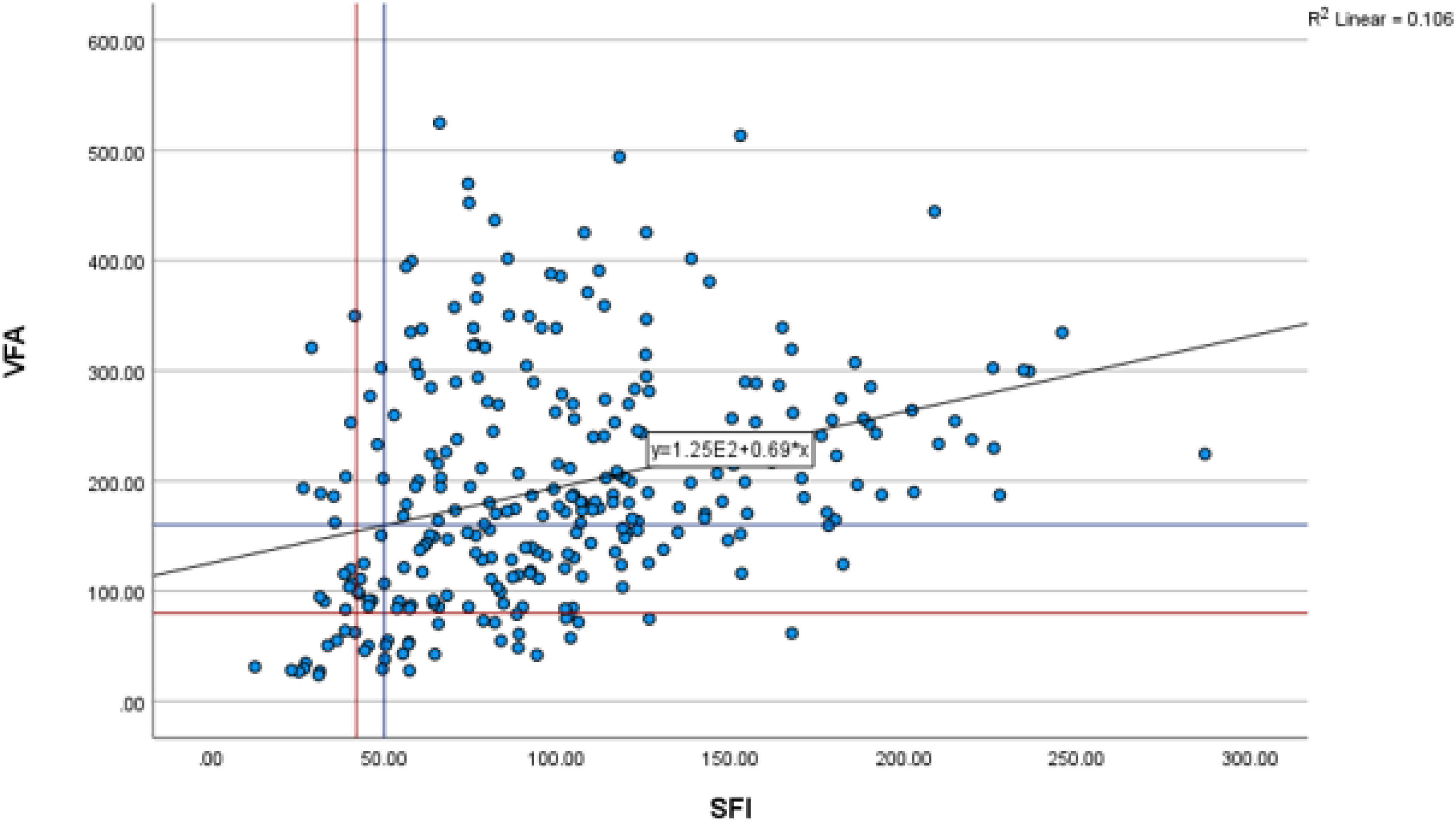
The relationship between SFI and VFA in those with undergoing CT colonography. N.B. Blue and red lines indicate thresholds of VFA and SFI for males and females respectively.
The relationship between host characteristics, BMI, CT-BC measurements and colorectal neoplasia incidence in those with undergoing CT colonography
On univariable analysis, sex (p < 0.001) and high VFA (p = 0.044) were significantly associated with colorectal neoplasia. When adjusted for age and sex, both sex (p < 0.001) and high VFA (p < 0.05) remained significantly associated with the incidence of colorectal neoplasia on multivariable analysis (See Table 3).
The relationship between host characteristics, BMI, CT-BC measurements and colorectal neoplasia incidence in patients undergoing CT colonography (n = 286).
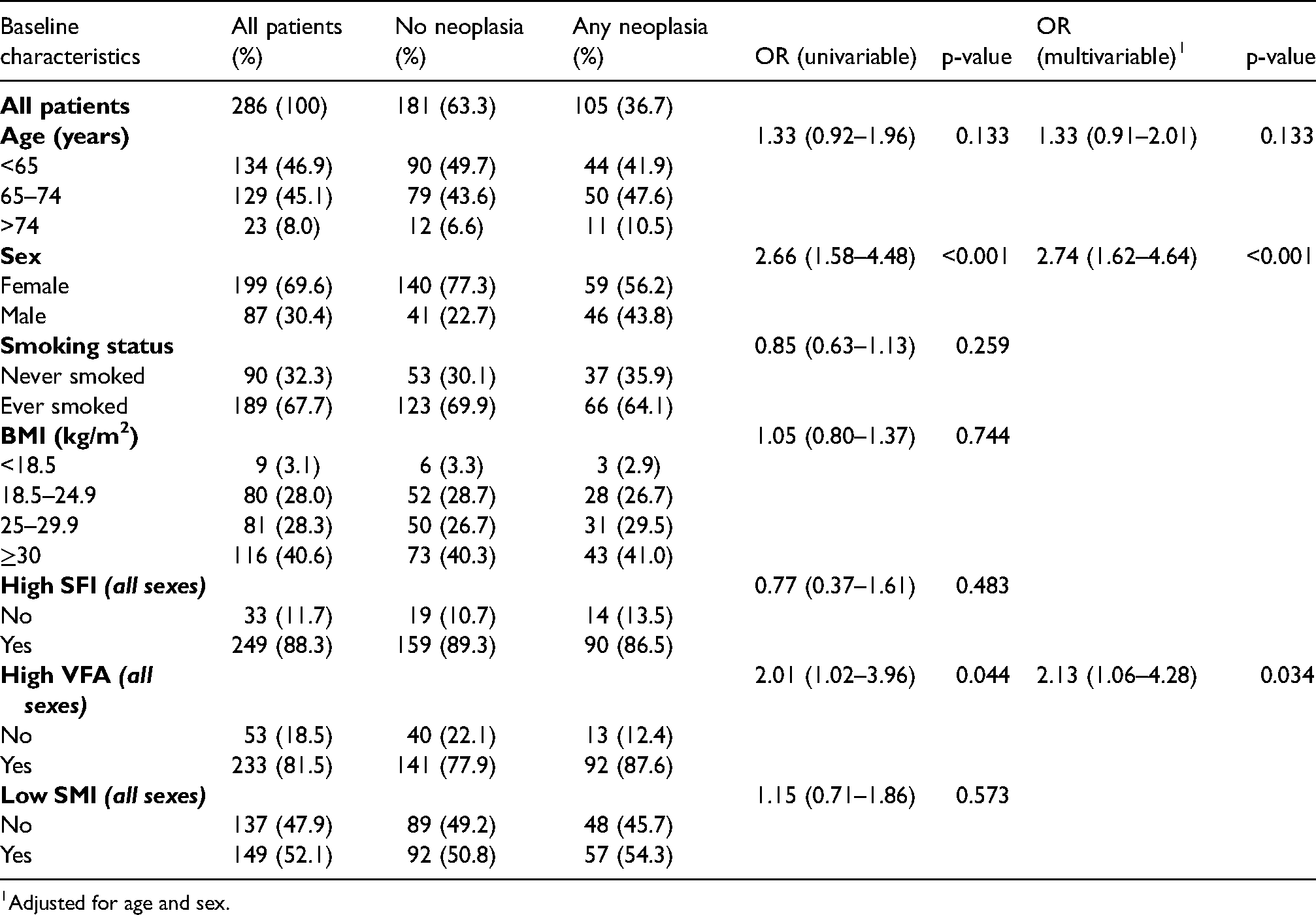
Adjusted for age and sex.
The relationship between host characteristics, BMI, CT-BC measurements and advanced colorectal neoplasia incidence in those with undergoing CT colonography
On univariable analysis, high SFI (p < 0.05) was significantly associated with advanced colorectal neoplasia. When adjusted for age and sex, high SFI (p < 0.05) remained significantly associated with the incidence of advanced colorectal neoplasia on multivariable analysis (See Table 4).
The relationship between host characteristics, BMI, CT-BC measurements and advanced colorectal neoplasia incidence in patients undergoing CT colonography with colorectal neoplasia only (n = 105).
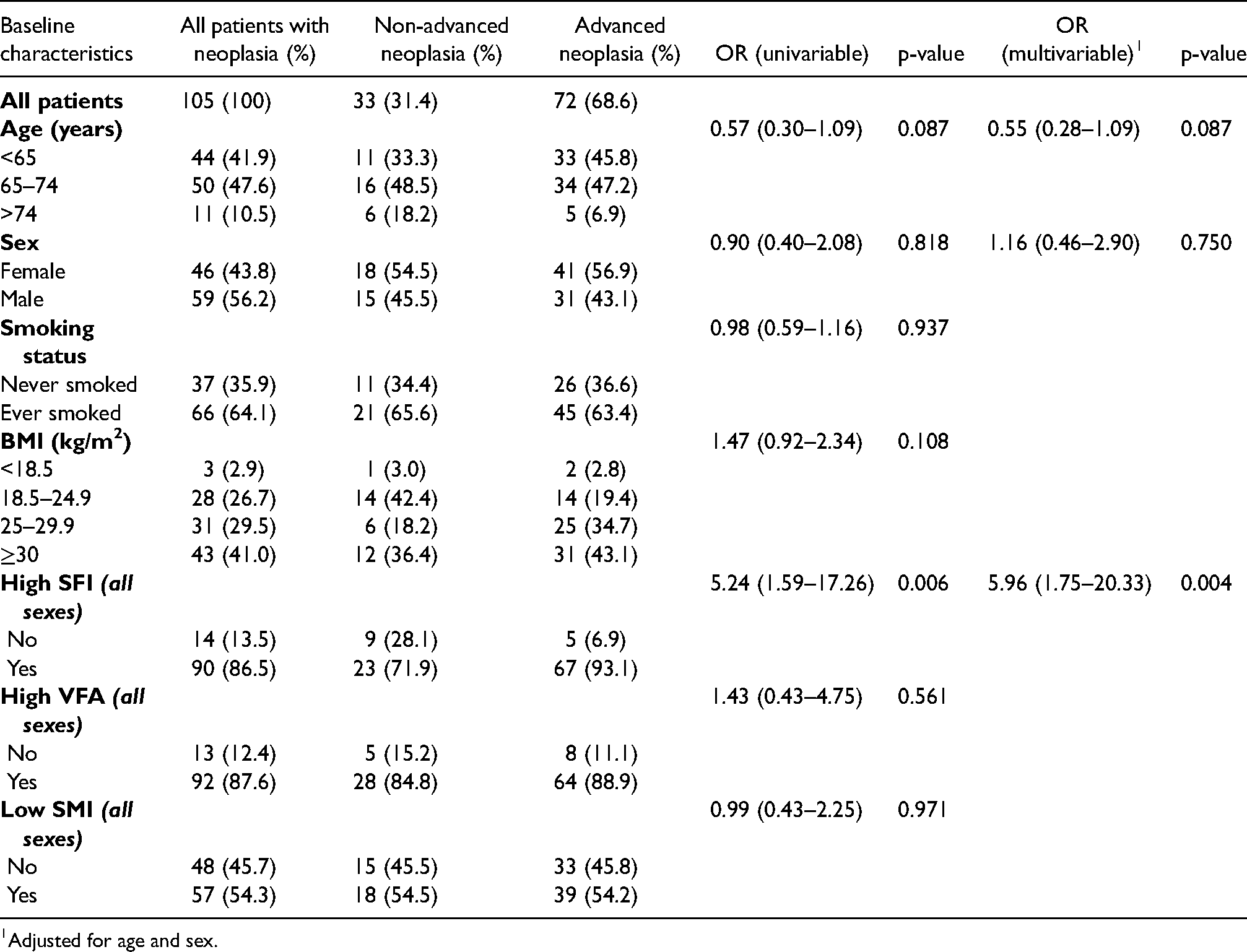
Adjusted for age and sex.
Discussion
The present study explores the relationship between BMI, CT-body composition and the incidence of colorectal neoplasia, in patients investigated as part of the Scottish Bowel Screening Program. Male sex and high VFA were significantly associated with the incidence of colorectal neoplasia, while a high SFI was associated with advanced colorectal neoplasia. In contrast, when adjusted for CT-derived adipose measures, BMI was not significantly associated with the incidence of colorectal neoplasia or advanced colorectal neoplasia in this cohort. The results of the present study suggest CT adipose measurements are more closely associated with degree of neoplasia in patients undergoing colorectal cancer screening. Therefore, where CT colonography is used, VFA and SFI may be useful in stratifying patient risk of advanced neoplasia and may have a role in determining more intensive surveillance.
The results of the present study are consistent with previous studies. Summers et al., 31 found that male gender and VFA were significantly associated with colorectal adenoma incidence in 1186 patients who underwent CTC, out with a screening programme, in the USA. Furthermore, Im et al., 32 reported that VFA was significantly associated with colorectal adenoma incidence in 1163 patients who underwent CTC, also out with a screening programme, in South Korea. Although the design of these studies varied, the incidence of neoplasia was similar between the present study, and that of Summers and Im (37%, 29% and 39%). Therefore, CT body composition measurements may be useful to explore the mechanism underlying the relationship between visceral obesity and increased incidence of colorectal adenoma. It is likely that this is complex, with several biologically plausible theories proposed. It has been suggested that visceral adipose tissue (VAT) is metabolically more active than subcutaneous adipose tissue (SAT). Relative to SAT, it is thought that higher volumes of VAT results in elevated levels of circulating pro-inflammatory cytokines such as IL-6 and TNF-α. 33 Furthermore, elevated VAT volume is thought to promote insulin resistance and the bioavailability of insulin-like growth factor-1 (IGF-1). Recent work has shown a correlation between CT-derived measurements of VAT and both inflammatory and angiogenic biomarkers such as CRP and vascular endothelial growth factor (VEGF) in patients with CRC. 34 It is believed that the pro-inflammatory, pro-proliferative, insulin-resistant environment promoted by VAT may play a role in the formation and growth of colorectal neoplasia.35,36 This theory is supported by previous work, demonstrating that insulin and insulin-like growth factors are associated with the development and progression of adenomatous polyps. 37
The present study also sought to investigate the relationship between body composition and advanced neoplasia. It was of interest that on multivariate analysis, a high SFI but not a high VFA, was found to be significantly associated with advanced colorectal neoplasia. Indeed, on post-hoc univariate analysis TFA (presented as tertiles) was not found to be significantly associated with advanced neoplasia (OR 1.18, (95% CI 0.70–1.97, p = 0.531). The reason for this finding is not clear, however previous studies have reported that VAT decreases in the later stages of CRC.36,38 It may be that VAT is potentially adenoma-promoting in the early stages as per the results of the present study, but its volume and influence decrease as adenomas progress towards advanced neoplasia and cancer, such that VFA becomes less influential than SFI. Indeed, Himbert and co-workers found that in patients with CRC, the VFA:SFA ratio was positively correlated with biomarkers of inflammation and angiogenesis, which play fundamental roles in the development and progression of colorectal cancer. 34 Further work comparing body composition measures in a group of patients with pre-malignant disease and those with established CRC may be of value in examining this theory further.” Text amended accordingly in the discussion section of the manuscript.
A low skeletal muscle mass is prevalent in patients with CRC across a range of disease stages. 39 Studies have found that it is an independent prognostic factor for both cancer-specific and overall survival in patients with CRC.23,24 However, to date, there is little evidence pertaining to the role of sarcopenia in the early or pre-malignant stage of CRC. As such, the results of the present study are informative, finding that a low skeletal muscle mass was neither associated with the incidence of colorectal neoplasia or advanced colorectal neoplasia. Therefore, it may be that the prognostic value of SMI reflects its measure of the nutritional and functional reserve of the cancer patient. 39
This present study has a number of limitations. Firstly, this was a single centre study which may introduce sample bias. Also, a significant number of patients had CTC as their first-line investigation due to multiple comorbidities that rendered them unfit for colonoscopy. It could be construed that this group may be slightly less representative of standard bowel screening patients; however, the 7% cancer diagnosis rate in this group mirrors that of the Scottish Bowel Screening Programme nationally. 40
In conclusion, the results of the present study show that visceral obesity as measured by VFA, is associated with a higher incidence of colorectal neoplasia. Furthermore, it is likely that this detailed analysis of body fat distribution is a superior measure to BMI for studying the relationship between adiposity and colorectal neoplasia. Further studies comparing measures of body composition in a pre-malignant population and those with established cancer are required.
Footnotes
Disclosures
No funding/conflicts of interest to declare.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.