
Abstract
Background and Aims
Testicular Germ Cell Tumours (TGCTs) are the commonest young adult male cancer, with excellent survival outcomes even with metastatic disease. Chemotherapy, radiotherapy, and surgery are international guideline-dictated standard of care (SOC) treatments for International Germ Cell Cancer Collaborative Group (IGCCCG) “good risk” TGCT, but are associated with significant toxicities. Therapy de-escalation aims to reduce treatment morbidity whilst preserving cure rates, and has been adopted by some centres for stage IIA/B seminoma. Here, we report on the contemporary UK treatment landscape for stage IIA/B seminoma.
Methods
A questionnaire-based survey of NHS England-designated specialist cancer centres hosting supra-regional specialist multi-disciplinary team (sMDT) services (n = 13) as well those within NHS Scotland, NHS Wales and Health and Social Care Northern Ireland. Respondents were asked to order preferences of SOC and therapy de-escalation treatments for stage IIA/B seminoma.
Results
We identified significant geographical heterogeneity in treatment preferences. Whilst up to a third of centres have adopted a treatment de-escalation regimen, the majority deliver combination chemotherapy or radiotherapy.
Conclusion
A wider recognition of UK treatment heterogeneity and consideration of therapy de-escalation strategies at supra-regional sMDTs will increase stage IIA/B seminoma treatment options as part of clinical trials with oncological and quality of life endpoints.
Keywords
Brief piece
Testicular Germ Cell Tumours (TGCTs) are the commonest young adult male cancer with 2300 cases per annum in the UK. 1 Chemotherapy, radiotherapy, and surgery have transformed survival outcomes, rendering many patients cured from metastatic disease. Standard of care (SOC) treatments for the International Germ Cell Cancer Collaborative Group (IGCCCG) “good risk” TGCTs 2 comprises of orchidectomy with either bleomycin, etoposide and cisplatin (BEP) combination chemotherapy or external beam radiotherapy (30–36Gy in 2Gy fractions) or primary retroperitoneal lymph node dissection (RPLND) for marker negative non-seminoma. 3 However, these treatments are associated with early toxicities and late effects which adversely impact a younger patient disease demographic.
Therapy de-escalation strategies aim to reduce treatment morbidity whilst preserving cure rates, and have promising outcomes for stage II seminoma in cohort studies. Reduced field radiotherapy with neoadjuvant carboplatin AUC7 with for stage IIB disease yields excellent results. 4 Adjuvant Carboplatin AUC7 following primary robot-assisted RPLND for stage IIA/B seminoma is associated with low relapse rates/morbidity. 5 Oncological outcomes of carboplatin AUC10 for stage II seminoma match SOC but with a lower toxicity profile. 6
We surveyed (Supplementary Data) 16 designated UK cancer centres hosting supra-regional services to determine clinician treatment preferences for stage IIA/B seminoma. The response rate was 94% from either medical (n = 11) or clinical (n = 2) oncologists, or surgeons (n = 2) representing each centre. The median number of cases treated per year was 5 (Range, 2–30). For stage IIA disease, radiotherapy was the preferred treatment (53%) whilst BEP and radiotherapy were most frequently adopted (40%, each) for stage IIB disease (Figure 1). Up to a third of all centres adopted a treatment de-escalation strategy.
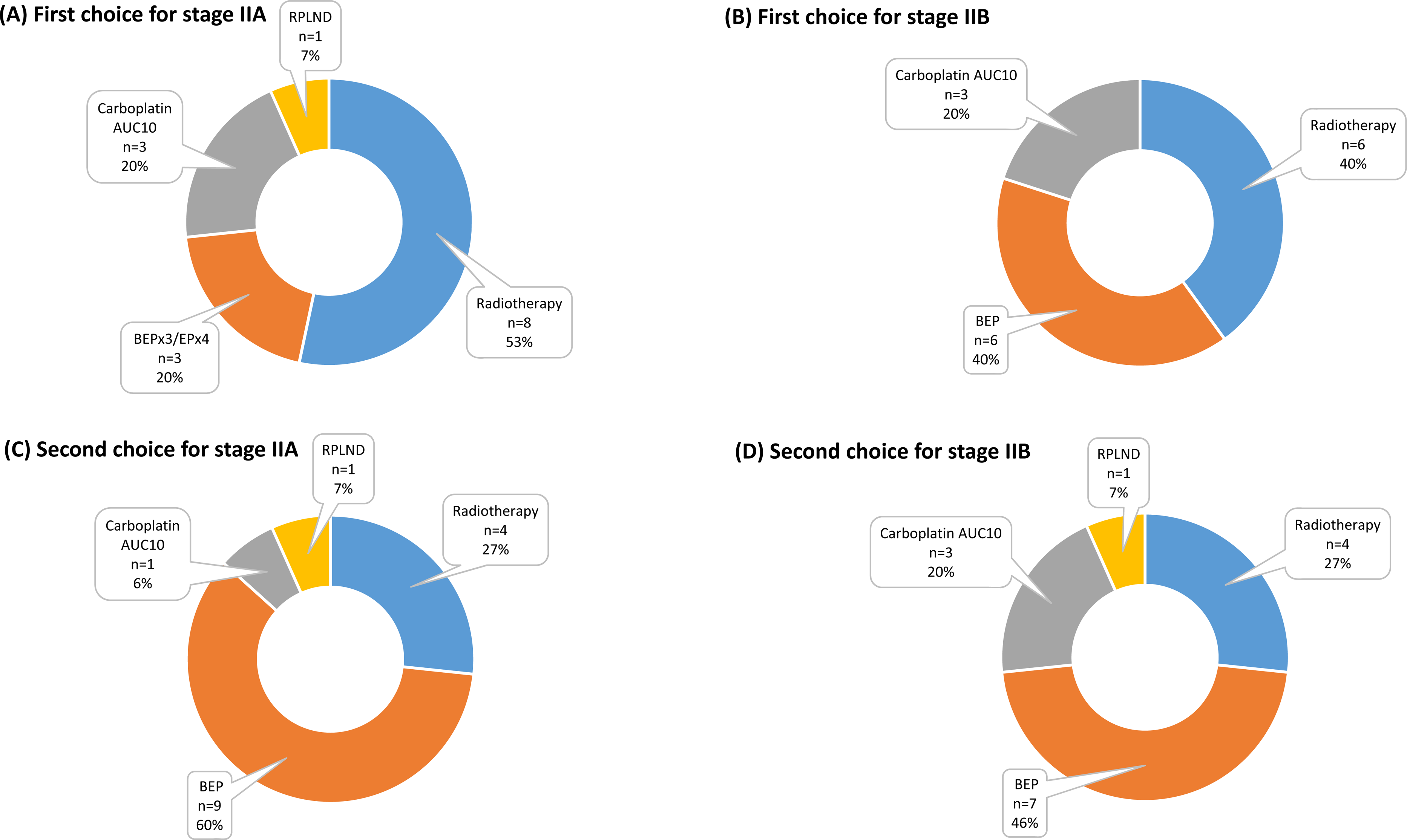
Results of UK national survey of clinician treatment preferences for stage IIA/B seminoma at specialist centres for (A) Stage IIA and (B) Stage IIB seminoma.
Of a total of 16 cancer centres, we received 15 responses (94%) from either medical (n = 11) or clinical (n = 2) oncologists, or urological surgeons (n = 2) representing each centre. The median number of cases treated by each centre was 5 (Range, 2–30/year). For stage IIA disease, radiotherapy was the preferred treatment (53%) followed by BEP or carboplatin monotherapy AUC 10 (Figure 1). BEP and radiotherapy were most frequently adopted (40%, each) for stage IIB disease followed by carboplatin monotherapy AUC 10. Whilst up to a third of all UK centres adopted one or other treatment de-escalation regimen, the majority deliver radiotherapy or combination chemotherapy which are associated with the greatest toxicites.
A lack of large-scale randomised trials data in stage II seminoma has led to disparate contemporary practices adopting chemotherapy, radiotherapy and surgery based on institutional preferences. Our survey highlights UK treatment heterogeneity for stage IIA/B seminoma. Whilst some have adopted therapy de-escalation strategies, the majority centres utilise combination chemotherapy or radiotherapy. Future prospective therapy de-escalation trials should capture patient preferences, oncological and quality-of-life outcomes, and toxicity data to support the evidence base for such approaches and aid patient-physician shared decision-making.
Summary
Therapy de-escalation aims to reduce short and long term treatment morbidity whilst preserving high cure rates
Metastatic (stage IIA/B) seminoma, which has excellent cure rates, has been a major focus for therapy de-escalation
De-escalation strategies are yet to be recognised as standard of care in international guidelines due to a lack of randomised studies
Within the UK, there appears to be some adoption of de-escalation strategies for stage IIA/B seminoma, but heterogeneity in standard of care treatments
Future clinical trials are needed to explore the use of de-escalation as part of shared patient-physician decision-making with oncological and quality of life outcomes
Footnotes
Acknowledgements
The questionnaire-based survey was designed, approved and communicated on behalf of the National Cancer Research Institute (NCRI) Teenage and Young Adult and Germ Cell Tumour Research Group members: Dr Dan Stark (Chair), Dr Mathew Murray, Mrs. Nicola Pettitt (Trainee), Dr Ben Carpenter, Dr Sarah Pratap, Dr Anna Castleton, Dr Andrew Protheroe, Dr Julia Chisholm, Mrs. Carla Reid, Dr David Cutter, Dr Alison Reid, Richard Feltbower, Dr Naveed Sarwar, Dr Lorna Fern, Professor Adam Glaser, Dr Hadeel Hassan (Trainee), Dr Louise Soanes, Prof. Mike Hawkins, Dr Sara Stoneham, Ms. Bethan Ingram, Miss Lara Veitch, Dr Angela Jesudason, Dr Graham Wheeler, Mr Max Williamson, Mr Vincent Wolverson, Dr Matthew Wheater, and Dr Clare Verill. We are grateful to NCRI Research Group Coordinators Christiana Ogunbote and Lucy Barwell for their help with survey dissemination, and all respondents for completing questionnaires.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.