
Abstract
Introduction
Ablation has become an effective treatment for small hepatocellular carcinomas (HCC). Whilst ablation is a safe and effective technique, diaphragmatic injury is a rarely associated but significant complication.
Conclusion
Our report adds to the current available knowledge on diaphragmatic injury following hepatic ablation and demonstrates the potential for life threatening consequences associated with this complication.
Introduction
The treatment of hepatocellular carcinoma (HCC) has progressed significantly in recent years with the increased availability of targeted therapies such as trans-arterial chemo embolization (TACE), selective internal radiation therapy (SIRT) and ablation techniques. Ablation has been demonstrated to be safe and effective in patients with localised disease and is now recommended for patients with Barcelona stage A disease. 1 Unlike SIRT and TACE, ablation is carried out with curative intent and can be carried out under CT or ultrasound guidance.
A low complication rate is associated with ablation. In 2012 Koda and co-workers reported on 13,283 patients who had undergone radiofrequency ablation for liver lesions and found the complication rate to be 3.54%. 2 Similarly, in 2020 Maeda et al reported a complication rate of 2.9% in 9,411 patients. 3 Recognised complications include haemorrhage, abscess formation, biliary fistulation, and hepatic injury. As more cases are performed, rarer complications are being identified, one of which is diaphragmatic injury. Recent large series have reported the rate of diaphragmatic injury to be between 0 and 0.1%2,4,5 however the natural history of such injuries remains unclear. We report a case of diaphragmatic injury secondary to MWA which progressed to diaphragmatic herniation and ultimately perforation of the large bowel.
Case report
A 67 year old gentleman with chronic liver disease secondary to hereditary haemochromatosis, Child’s Pugh score A and AFP of 3 had a liver lesion detected in segment VIII (antero-superior right lobe) of the liver on routine surveillance sonography. The lesion was indeterminate on initial MRI, however a further MRI after 6 months confirmed the lesion to be a hepatocellular carcinoma (LIRADS 5).
Following MDT discussion, ultrasound-guided MWA was performed under general anaesthesia (Figure 1). A single antenna microwave system (Emprint™, Covidien, Boulder, CO, USA) was utilised and 140 watts was delivered to the tumour for 6 minutes. The procedure was well tolerated, and no immediate complication was detected.
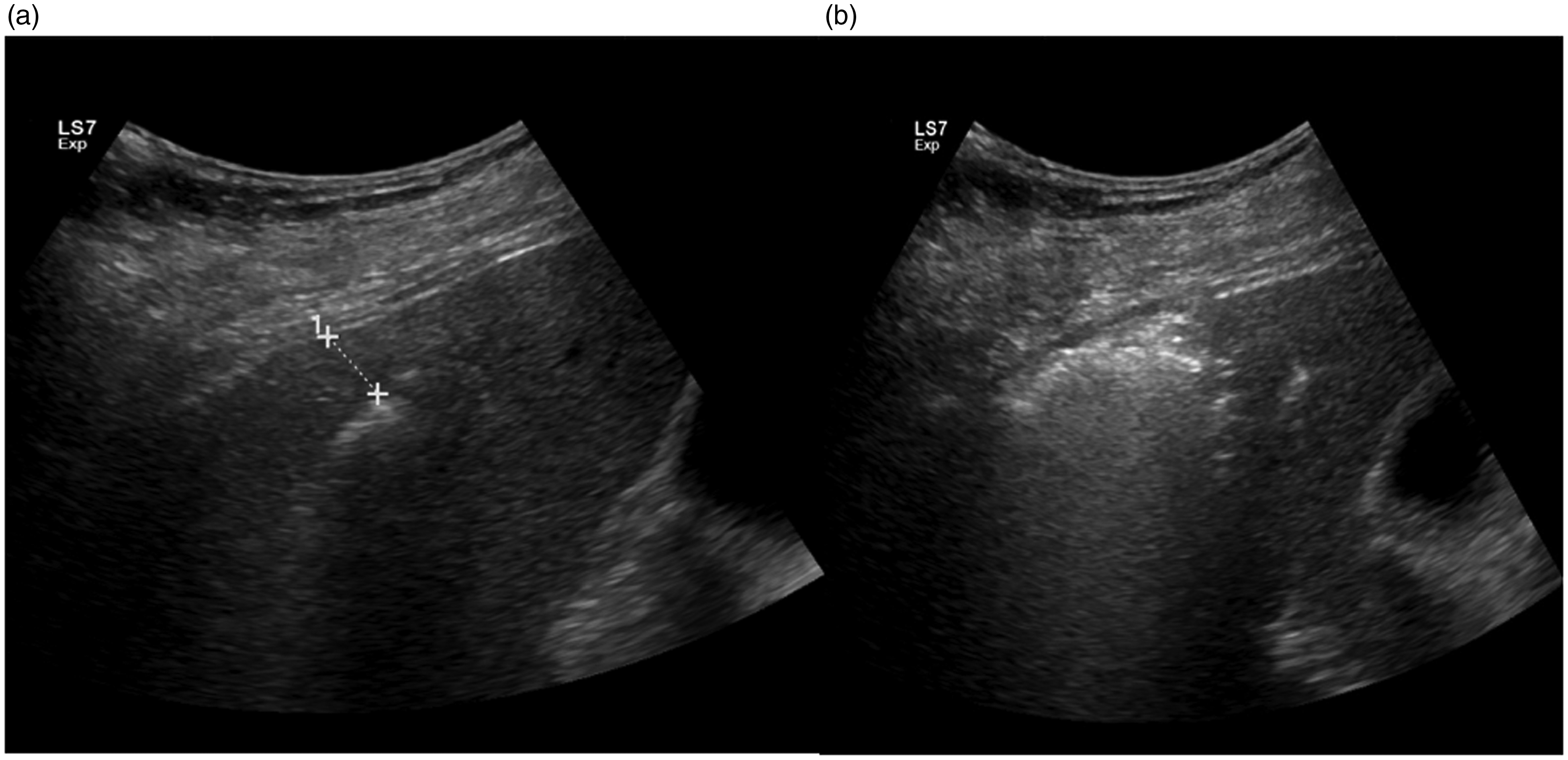
(a) Ultrasound imaging of the ablation probe crossing the segment VIII lesion. (b) Post ablation ultrasound image, demonstrating gas around the ablation zone.
Routine imaging follow up was carried out at 1 month, 6 months, 12 months, 15 months and 21 months following the procedure none of which demonstrated tumour progression. On the 15 month scan, a defect in the lateral aspect of the right hemidiaphragm was noted (Figure 2).
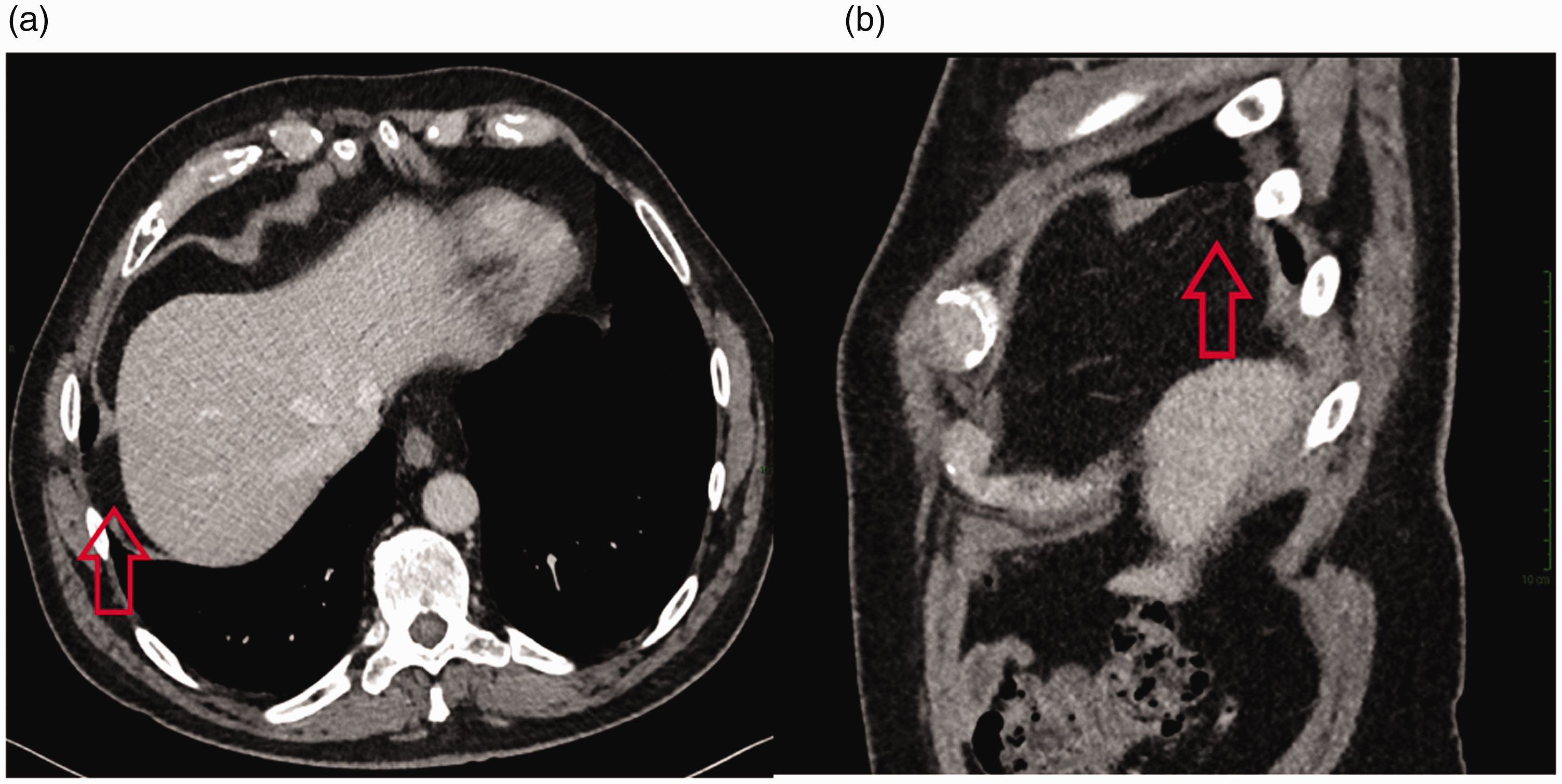
15 month follow-up contrast CT demonstrating axial (a) and sagittal views (b) of the diaphragmatic defect (red arrows) within the lateral aspect of the right diaphragm. No fat or bowel herniation is seen at this stage.
At 22 months, the patient presented to the emergency department with shoulder tip pain and shortness of breath. A chest radiograph demonstrated bowel loops within the right thoracic cavity and a CT was performed (Figure 3). This demonstrated herniation of the superior ascending colon and right transverse colon through the diaphragmatic defect into the right thoracic cavity. Emergency laparotomy revealed the transverse colon had perforated. An extended right hemicolectomy was performed with an ileostomy and mucous fistula. The diaphragmatic defect was closed.
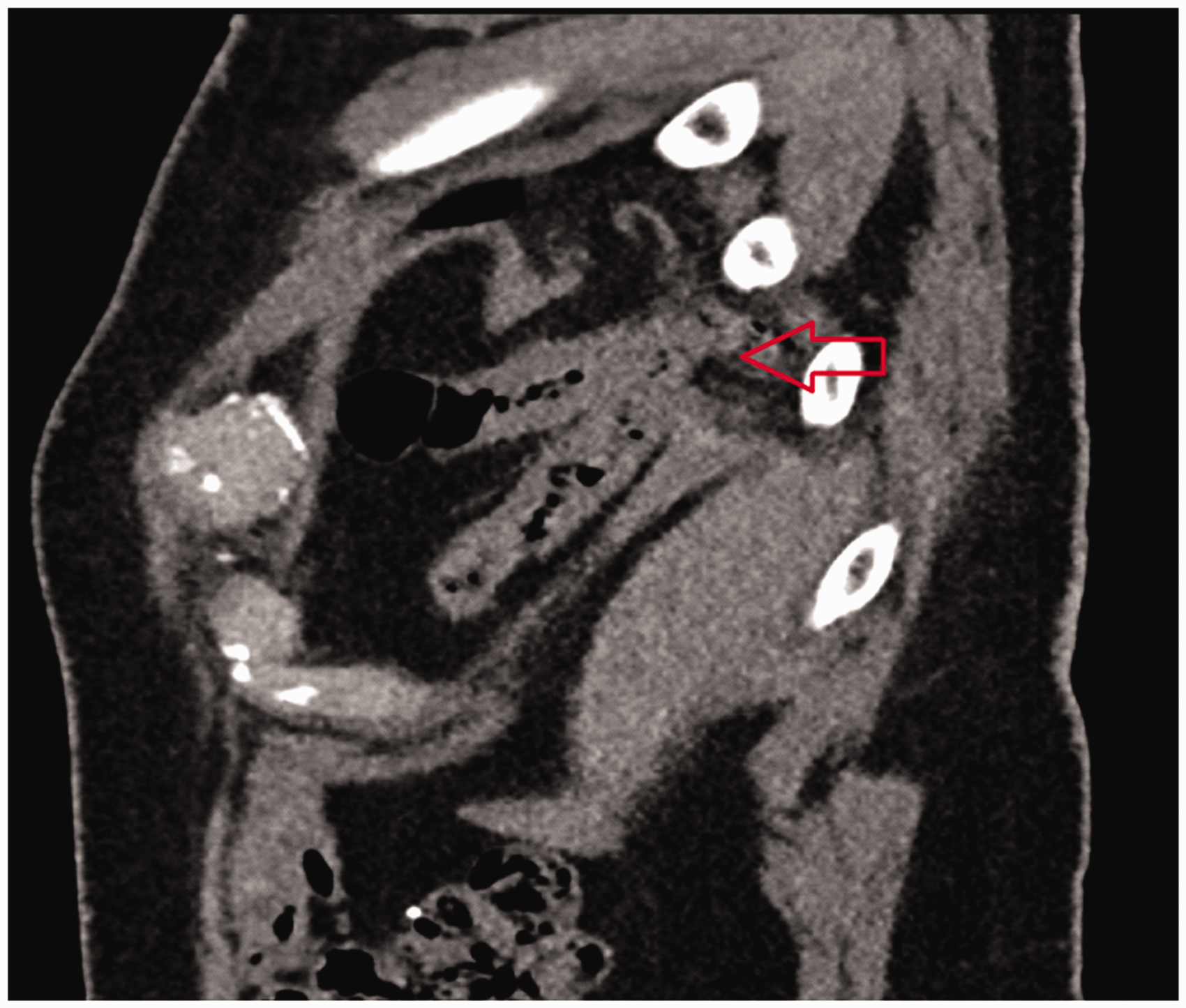
Sagittal view of CT performed during acute admission. Herniation of hepatic flexure through the right diaphragmatic defect.
Post operatively an empyema formed in the right pleural space, for which an ultrasound guided drain was placed. Eventually the patient was released from hospital and was able to undergo an elective closure colostomy 1 year following discharge
Discussion
Diaphragmatic injury is a rare complication of hepatic ablation. There is a spectrum of injuries which may be present, ranging from diaphragmatic defect to bowel herniation. Whilst a small defect may appear innocuous, as we have demonstrated in this case, defects may progress to herniation with potentially life-threatening complications. To the authors knowledge this is the first case in the literature in which emergency bowel resection has been required for ablation associated diaphragmatic hernia.
One common factor in the cases reported to date is the location of the lesions which were treated. The majority have been in the right lobe or close to the border between the lobes, with many of these being in segments VII (posterior-superior right lobe) and VIII.6,7 This was also the case in the present case where the initial lesion was present in segment VIII.
The use of techniques such as hydro dissection, artificial ascites or laparoscopy-assisted ablation could be considered to reduce the direct heat effect to the diaphragm. Advances in ablation probe technology will allow a more focused delivery of energy and should also reduce the risk of non-target tissue injury. 8
On follow up imaging after ablation of lesions in the superior segments of the right liver, clinicians should take particular care to assess the diaphragm for injury. Diaphragmatic defects are difficult to detect on CT and MRI and there may be a group of patients who have defects which go undetected and do not progress to herniation.
The management of patients with iatrogenic diaphragmatic defects has been reported to a limited degree. Nagasu and co-workers in 2017 reported a series of 6 patients with diaphragmatic perforation, 4 of which had associated herniation. 9 All 6 of the cases were repaired surgically, and the authors advised that surgical repair should be carried out on any ablation induced diaphragmatic defect. Our case supports the treatment of patients who develop diaphragmatic defects to prevent the development of herniation.
The risk of development of herniation should be balanced with the risks of surgery. The majority of patients who undergo thermal ablation have background chronic liver disease which increases the risks associated with surgery. In addition, some patients are selected for ablation, specifically because they are not fit for surgery. Saito described a case in 2015 in which the subject died of liver failure 33 days following diaphragmatic hernia repair, caused by radiofrequency ablation. 10
Future studies should aim to characterise the true prevalence of diaphragmatic defects and the natural history of this complication to help inform whether these defects should be repaired prophylactically, prior to the development of herniation.
Learning points:
Clinicians should be aware of the risk of diaphragmatic injury and the potential sequelae when planning hepatic ablation. Readers of follow up imaging should carefully assess the diaphragm in cases where ablation has been performed in the superior right lobe of liver segments. Our case also supports the early surgical repair of iatrogenic diaphragmatic defects secondary to liver ablation.
Footnotes
Authors’ contribution
HI performed the ablation and contributed to writing the manuscript.
SL and MM contributed to writing the manuscript.
Consent for publication
Consent for publication was obtained for every individual person’s data included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Patient consent
Full informed consent was obtained from the patient described in this case.