
Abstract
Objective
To evaluate the intraoperative efficiency and long-term outcomes of clip-assisted primary closure versus conventional suturing in classic carotid endarterectomy (CEA).
Methods
This single-center retrospective cohort study included 46 classic CEA procedures in 45 patients treated between 2013 and 2019. Procedures were divided into a clip group (n = 15) and a suture group (n = 31). The primary endpoints were carotid clamping time and intraoperative blood loss. Secondary endpoints included operative time, postoperative drainage volume, perioperative stroke, long-term stroke incidence, and all-cause mortality.
Results
The clip group had a significantly shorter carotid clamping time than the suture group (12.67 ± 5.74 min vs. 18.26 ± 7.84 min, P = 0.048) and significantly lower intraoperative blood loss (38.00 ± 18.97 mL vs. 56.77 ± 23.01 mL, P = 0.010). No statistically significant between-group differences were observed in total operative time, postoperative drainage volume, perioperative stroke, long-term stroke incidence, or all-cause mortality.
Conclusions
In this exploratory retrospective cohort study, clip-assisted primary closure during classic CEA was associated with shorter carotid clamping time and lower intraoperative blood loss than conventional suturing. No signal of increased perioperative or long-term adverse outcomes was detected; however, the study was not powered to establish equivalence or non-inferiority for rare safety endpoints. These findings support the technical feasibility of clip-assisted primary closure in selected patients, but larger prospective studies are needed to further evaluate its safety and long-term effectiveness.
Keywords
1. Vascular clips significantly shortened carotid clamping time during classic carotid endarterectomy. 2. Intraoperative blood loss was significantly lower in the clip group than in the suture group. 3. No signal of increased long-term stroke or loss of patency was detected in the clip group during follow-up. 4. Clip-assisted primary closure was technically feasible in selected patients undergoing classic carotid endarterectomy. 5. This is the first long-term exploratory cohort study evaluating clip-assisted primary closure in carotid endarterectomy.Highlights
Introduction
Stroke remains a leading cause of mortality and disability worldwide. In China, stroke rose from the third to the first leading cause of death between 1990 and 2017, with an average mortality rate of 149 per 100,000 people in 2017. 1 Carotid endarterectomy (CEA) has long been established as the gold standard for treating carotid artery stenosis, supported by large-scale randomized trials such as NASCET, ECST, and ACAS. 2 While the surgical technique is now mature, efforts continue to refine operative efficiency and minimize perioperative complications.
A key step in CEA is vascular closure, traditionally performed with needle-and-thread suturing. However, this method penetrates the vessel wall, potentially damaging the intima and introducing foreign material into the lumen, which may trigger thrombosis, intimal hyperplasia, or restenosis.3–5 Vascular clips have emerged as a promising alternative, offering advantages such as reduced vessel trauma, elimination of intraluminal foreign bodies, and shorter anastomosis time.6–12
Currently, these clips are primarily used in dialysis access creation and peripheral vascular bypass procedures. Unlike those contexts, CEA inherently involves intimal disruption, potentially diminishing the theoretical advantage of clip-based closure techniques. Moreover, earlier attempts to use clips in CEA were limited by reports of severe complications, 13 leading to ongoing controversy regarding their suitability in this setting.6,7,13
Based on our prior surgical experience with vascular clips in arterial and venous procedures—including thrombectomy reconstruction, AV graft and fistula creation, and peripheral bypass—we cautiously extended their application to selected cases of carotid endarterectomy (CEA).
This exploratory retrospective study analyzed a carefully selected cohort of classic carotid endarterectomy (CEA) patients treated at our institution between 2013 and 2019. All procedures were performed by a single experienced surgeon, with consistent surgical indications and technique selection to minimize bias. We compared vascular clips and traditional sutures in terms of clamping time, intraoperative blood loss, postoperative complications, and long-term outcomes, including 5-year follow-up data. The goal was to assess the feasibility of clip-assisted primary closure in selected cases of classic carotid endarterectomy.
Methods
Research subjects
This retrospective study included all patients who underwent classic carotid endarterectomy (CEA) at the Department of Interventional and Vascular Surgery, Peking University First Hospital between January 2013 and November 2019. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki of 1975, as revised in 2024. All patient details were de-identified and anonymized prior to analysis and reporting. Patients were identified through the hospital’s electronic medical record system.
To ensure procedural consistency and reduce confounding from surgical technique variation, only patients who received conventional classic CEA (cCEA) were included. Because the AnastoClip GC system is intended for direct arteriotomy closure, the control group was intentionally matched using the same closure strategy (primary closure) to isolate the effect of the closure device. Patients undergoing patch angioplasty (pCEA) or eversion CEA (rCEA) were excluded, as our previous clinical experience demonstrated that the GC series of vascular clips was incompatible with the prosthetic patch materials commonly used in our institution, leading to poor mechanical fit. In our pilot experience with the synthetic patches routinely used in our center (e.g., B. Braun), deployment of GC-L clips could cause patch perforation and persistent oozing/bleeding at the closure line; therefore, clip application was not pursued in patch CEA in this cohort. According to the manufacturer’s Instructions for Use, the AnastoClip GC is intended for everting approximation when tissue penetration is desired; therefore, we applied clips only when symmetric eversion and adequate tissue thickness could be achieved. Furthermore, the VCS clip system—used in some external studies—was associated with a risk of anastomotic disruption and bleeding in CEA when used inappropriately, as reported in prior literature. 13 In light of these concerns and to maximize patient safety, we cautiously limited the clip application to cCEA procedures only in this exploratory study.
Patients were grouped based on the anastomotic technique: those receiving vascular clips (experimental group) and those receiving conventional non-absorbable sutures (control group). Assignment was influenced by preoperative consultation, with medical insurance coverage of the vascular clip system being a key consideration—since uninsured clips posed a significant financial burden, many patients and families opted for sutures. Despite this, baseline characteristics between the two groups showed no statistically significant differences, as verified by comparative analysis.
All surgeries were elective and performed by the same surgical team, with Professor Zhang Xiansheng as the sole operating surgeon, thereby controlling for operator-related variability.
Surgical indications were determined in accordance with the 2011 clinical practice guideline on extracranial carotid artery disease management. 14 Indications included: symptomatic carotid stenosis ≥70% on non-invasive imaging or ≥50% on catheter-based angiography; asymptomatic carotid stenosis ≥70% on non-invasive imaging or ≥60% on angiography; or unstable plaque features despite stenosis <70%. Symptomatic stenosis was defined as ipsilateral transient ischemic attack (TIA) or ischemic stroke occurring within the previous six months. Patients with uncontrolled systemic disease, abnormal routine preoperative assessments, or surgical contraindications were excluded. All procedures were elective; no emergency procedures were included.
Research materials
Nonabsorbable sutures used in this study included the Prolene® series (Ethicon, Johnson & Johnson, UK) and CV-6 sutures (GORE-TEX®, W. L. Gore & Associates, USA). The vascular clips used in this study were all AnastoClip GC® Closure System devices (LeMaitre Vascular, USA), with the GC-L model exclusively used in this study. Clip specifications were selected based on individual vascular anatomy.
Preoperative preparation
All patients underwent standard preoperative evaluations, including complete blood count, liver and renal function tests, serum electrolytes, myocardial biomarkers, glucose and lipid profiles, coagulation parameters, infection screening, urinalysis, and electrocardiogram to exclude surgical contraindications. Additional tests were performed as clinically indicated for comorbid conditions (e.g., thyroid function tests in patients with hypothyroidism). All patients had preoperative carotid imaging completed either at outside institutions or in our outpatient clinic.
For those with chronic antiplatelet therapy, medications were continued perioperatively at the original regimen. Hypertensive and diabetic patients had blood pressure and glucose levels monitored during hospitalization, with pharmacologic adjustments as needed.
Prior to surgery, all patients and/or their families received standardized counseling regarding the disease condition, procedural risks and benefits, postoperative considerations, and the potential differences between traditional sutures and vascular clips in terms of operative time, complication risk, and cost. Final selection of anastomosis method (clip vs. suture) was based on patient preference after informed consent. To minimize bias, only patients undergoing classic carotid endarterectomy by the same surgeon were included in this analysis.
Surgical procedure
All procedures were performed under general anesthesia with patients in the supine position and the head turned 45° to the contralateral side. A longitudinal incision was made along the anterior border of the sternocleidomastoid muscle to expose the common, internal, and external carotid arteries. A carotid sinus block was performed with 0.22% lidocaine, and systemic heparinization (1 mg/kg) was administered 5 minutes prior to arterial clamping. Following standard endarterectomy, the incised anterior walls of the common and internal carotid arteries were reconstructed either by continuous suturing (Prolene or CV-6 suture) or vascular clips, depending on preoperative patient/family choice. Anastomotic integrity was ensured by standard hemostasis techniques. A closed-suction drain was placed before layered closure. Representative intraoperative images of the clip-assisted procedure are provided in Figure 1. Intraoperative images of carotid endarterectomy using vascular clips.
No shunts or patches were used in any of the procedures. All patients underwent classic carotid endarterectomy without patch angioplasty or eversion techniques.
Intraoperative time was defined as the interval from skin incision to completion of skin closure. Carotid clamping time was defined as the interval from carotid cross-clamping to unclamping immediately after completion of carotid arteriotomy closure. Intraoperative blood loss was recorded based on the surgical report; if not explicitly documented, anesthesia records were used as the reference.
Postoperative management
Continuous electrocardiographic and blood pressure monitoring was performed postoperatively. For patients with a history of long-term oral antihypertensive therapy, preoperative regimens were resumed to maintain stable hemodynamics, ensuring adequate perfusion of vital organs such as the heart and kidneys. Intravenous mannitol and hydrocortisone were selectively administered to reduce intracranial pressure and provide neuroprotection. Antiplatelet therapy was initiated on the first postoperative day. Patients already on long-term antiplatelet medication resumed their original regimen. Others received 100 mg of aspirin orally once daily. Wound drainage volume and characteristics were closely monitored. The drainage tube was removed when the 24-hour output was less than 10 mL. Neurological assessments—including speech, facial symmetry, and limb motor function—were routinely performed to detect early signs of perioperative stroke.
Post-discharge follow-up
Telephone follow-up record form.

acomputed tomographic angiography (CTA),
bmagnetic resonance angiography (MRA).
cdigital subtraction angiography (DSA).
Statistical methods
The reporting of this study conforms to the STROBE statement for observational studies. 15 No formal sample size calculation was performed because this was an exploratory retrospective cohort study. The sample size was determined by the total number of consecutive eligible patients who underwent classic carotid endarterectomy during the study period.
The study endpoints were defined as the occurrence of stroke, patient death, or reaching the predefined follow-up cutoff point.
Continuous variables were expressed as mean ± standard deviation (range), and categorical variables as counts and percentages. The Mann–Whitney U test was used for comparisons of continuous variables between groups, while the chi-square test or Fisher’s exact test was used for categorical variables, as appropriate. Long-term stroke-free survival was assessed using Kaplan–Meier analysis and the log-rank test. Because of the limited sample size and small number of outcome events, no multivariable regression model was retained in the revised analysis. A two-tailed P-value of ≤ 0.05 was considered statistically significant.
All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Figure 3 was generated in R version 4.5.0 using the survival and survminer packages to display the Kaplan–Meier curve together with the number-at-risk table.
Results
Basic information of the patient
Basic information of patients.
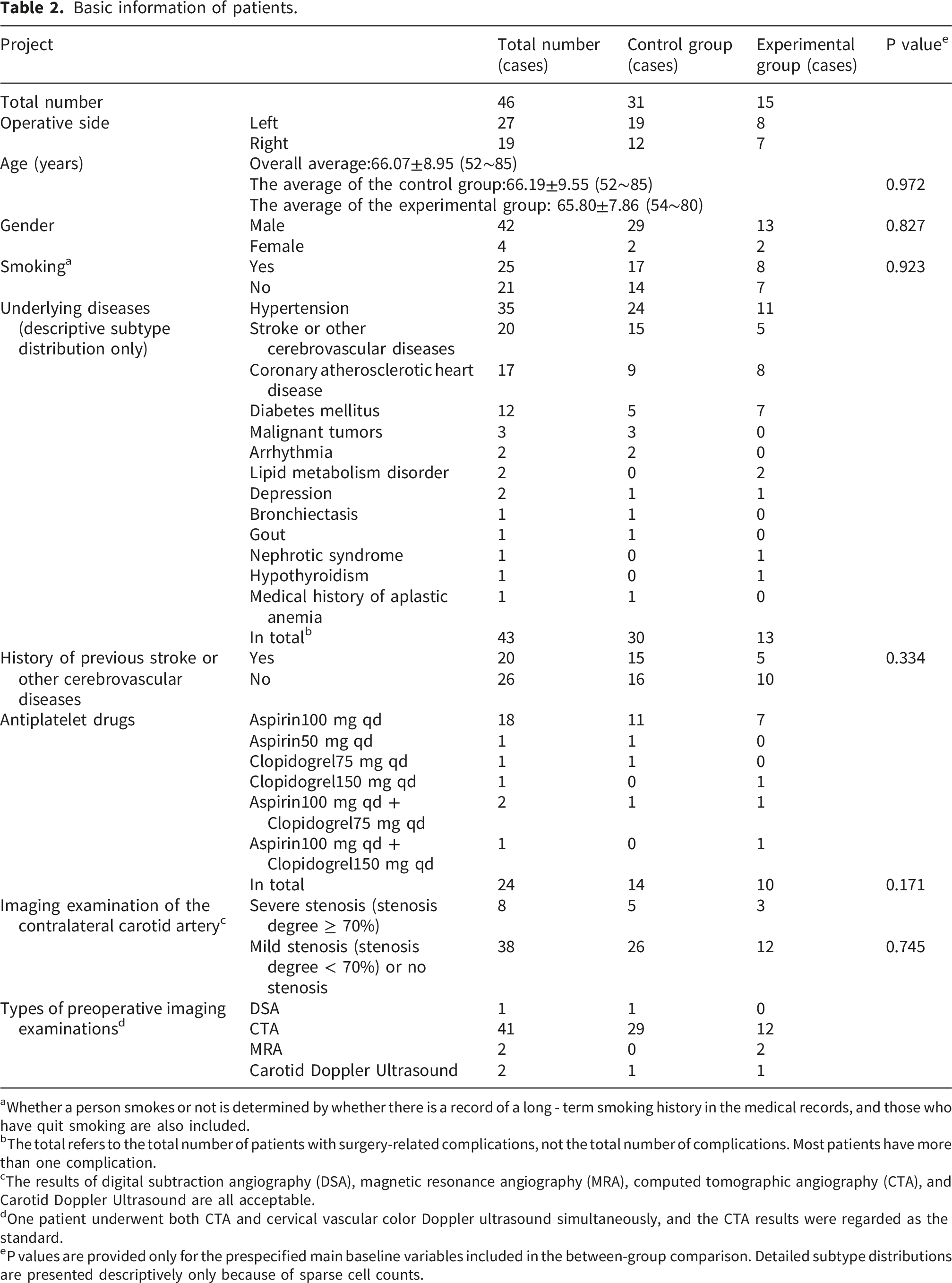
aWhether a person smokes or not is determined by whether there is a record of a long - term smoking history in the medical records, and those who have quit smoking are also included.
bThe total refers to the total number of patients with surgery-related complications, not the total number of complications. Most patients have more than one complication.
cThe results of digital subtraction angiography (DSA), magnetic resonance angiography (MRA), computed tomographic angiography (CTA), and Carotid Doppler Ultrasound are all acceptable.
dOne patient underwent both CTA and cervical vascular color Doppler ultrasound simultaneously, and the CTA results were regarded as the standard.
eP values are provided only for the prespecified main baseline variables included in the between-group comparison. Detailed subtype distributions are presented descriptively only because of sparse cell counts.
In 31 cases, primary closure was performed using traditional suture during surgery, which served as the control group. In 15 cases, primary closure was carried out using vascular clips during surgery, which served as the experimental group.
The mean age of the 45 patients was 66.07 ± 8.95 years (range, 52–85 years). The average age of the control group was 66.19±9.55 (52 - 85) years, and that of the experimental group was 65.80±7.86 (54 - 80) years. Among them, 25 patients had a smoking habit before surgery. A total of 43 patients had different types of chronic underlying diseases that might affect the surgery before surgery. Among them, 35 patients had hypertension, 20 had stroke or other cerebrovascular diseases, 17 had coronary atherosclerotic heart disease, 12 had diabetes, 3 had malignant tumors, 2 had arrhythmia, 2 had lipid metabolism disorders, 2 had depression, 1 each had bronchiectasis, gout, nephrotic syndrome and hypothyroidism. In addition, 1 patient had a history of aplastic anemia, which had been cured, and the hemoglobin was normal at admission. A total of 24 patients had been taking anti - platelet drugs orally for a long time due to underlying heart or cerebrovascular diseases before surgery, and the drugs included aspirin and clopidogrel. Preoperative imaging examinations indicated that 8 patients had severe stenosis (≥70%) of the contralateral carotid artery to the surgical side.
Surgical-related information of patients
The mean operation time for all patients was 126.02 ± 25.11 minutes (range: 82–197 min), with 125.26 ± 26.70 min in the suture group and 127.60 ± 22.25 min in the clip group.
Surgical-related information of patients.

aBoth the operation time and the clamping time shall be based on the records in the anesthesia record.
bThe intraoperative blood loss shall be based on the records in the surgical record. If the surgical record does not clearly state it, the records in the anesthesia record shall be used as the basis.
c1 mmHg=133.3 Pa。.
dP values are provided only for the prespecified main perioperative variables included in the between-group comparison. Other rows are presented descriptively only.
Perioperative complication occurrence, mortality, and follow-up results
A total of 46 carotid endarterectomy procedures were performed in 45 patients, with one patient undergoing contralateral surgery 21 months later. Among these, 41 patients completed follow-up, while 5 were lost to follow-up—all from the suture group.
The median follow-up duration was 88 months (IQR, 74–116; range, 60–143 months), with 114 months (IQR, 83–124; range, 60–143 months) in the suture group and 79 months (IQR, 66–87; range, 60–93 months) in the clip group.
Perioperative and long-term events
During the perioperative period, one patient died. Over the course of the long-term follow-up, a total of seven patients died. Perioperative stroke, defined as stroke occurring within 30 days after surgery, was observed in 4 of 46 procedures (8.7%). One additional stroke occurred beyond the 30-day postoperative window. Throughout the entire study period, no cases of reoperation, wound infection, or major bleeding were observed.
Imaging follow-up
A total of 36 patients underwent postoperative imaging, including CTA, MRA, DSA, or duplex ultrasound. Carotid restenosis or occlusion on the operative side was observed in three patients, none of whom developed new neurological symptoms. Representative CTA images before and after surgery are shown in Figure 2. Pre- and postoperative computed tomographic angiography (CTA) of a patient who underwent bilateral carotid endarterectomy. The red arrows indicate the locations of vascular clips used during the procedures.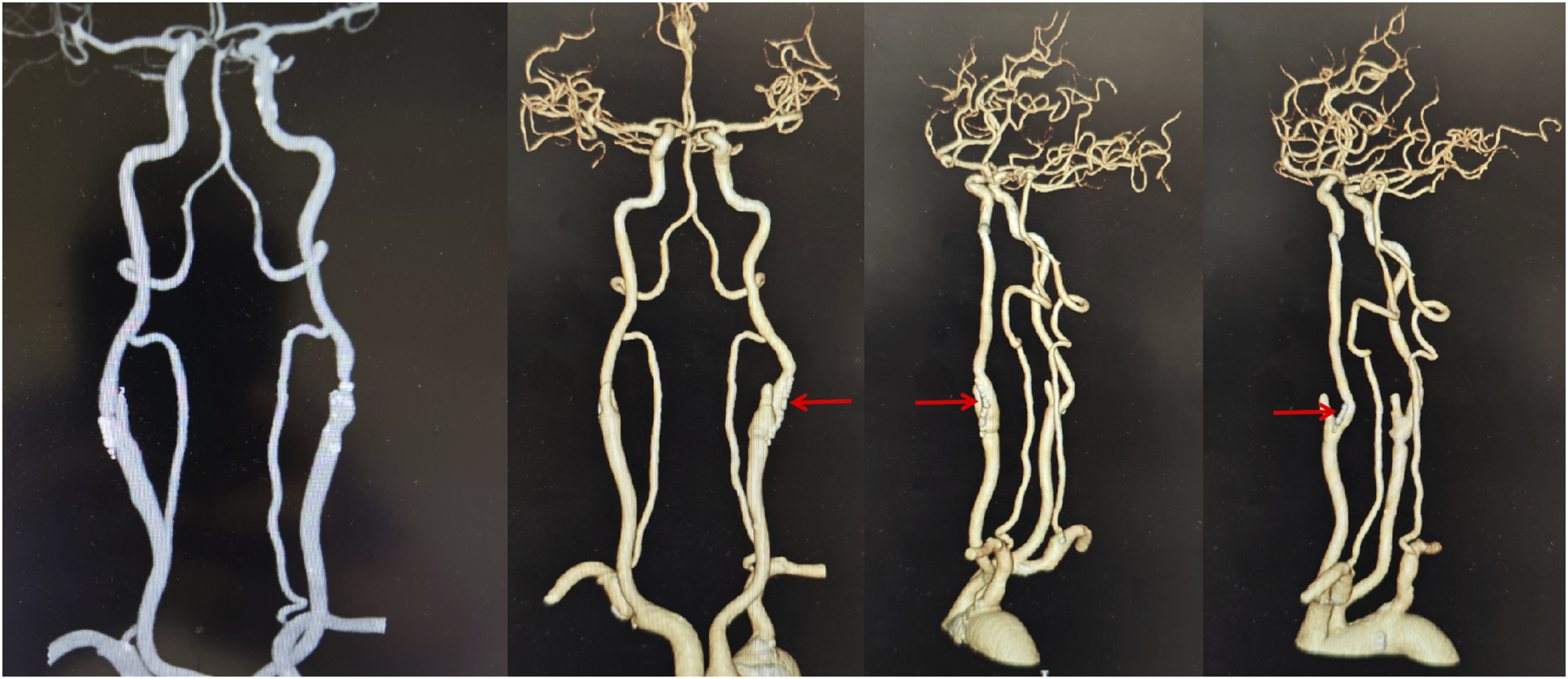
Occurrence of perioperative complications, mortality, and follow-up results.

aFollow-up time was defined as the interval from surgery to the occurrence of death or stroke; for event-free patients, it was calculated up to the study’s follow-up cut-off date, in completed months.
bPerioperative and long-term deaths were distinguished by the time of hospital discharge.
cFollow-up results included imaging conducted at both our center and external institutions.
dStroke occurring within 30 days postoperatively was classified as perioperative; events beyond 30 days were considered long-term postoperative strokes.
Statistical analysis
Variable definition and assignment
Patient prognosis following carotid endarterectomy (CEA) may be influenced by multiple clinical factors, including age, comorbidities, degree of carotid stenosis, contralateral occlusion, and preoperative cerebrovascular history. Given the limited sample size, to avoid reduced statistical power due to overparameterization, this study limited the number of covariates to: age (X1), gender (X2), smoking status (X3),underlying diseases other than cerebrovascular diseases (X4), history of stroke or other cerebrovascular diseases (X5), long - term use of antiplatelet drugs (X6), degree of carotid artery stenosis on the operative side (X7), ipsilateral external carotid artery stenosis or occlusion (X8), and severe stenosis of the contralateral carotid artery (X9).
Definitions of influencing variables, variable codes, statistical methods, and intergroup comparisons between the clip group and the suture group.
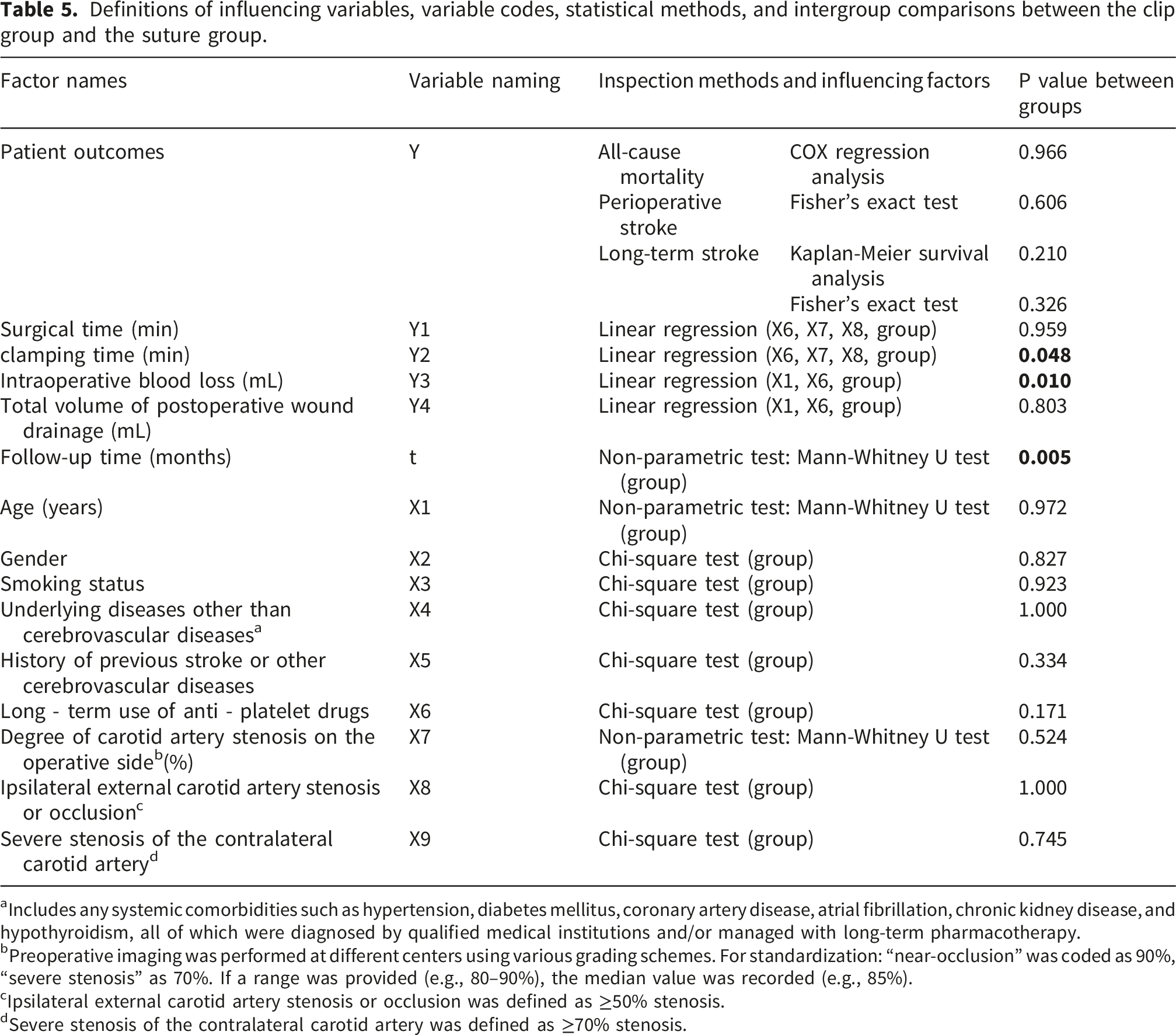
aIncludes any systemic comorbidities such as hypertension, diabetes mellitus, coronary artery disease, atrial fibrillation, chronic kidney disease, and hypothyroidism, all of which were diagnosed by qualified medical institutions and/or managed with long-term pharmacotherapy.
bPreoperative imaging was performed at different centers using various grading schemes. For standardization: “near-occlusion” was coded as 90%, “severe stenosis” as 70%. If a range was provided (e.g., 80–90%), the median value was recorded (e.g., 85%).
cIpsilateral external carotid artery stenosis or occlusion was defined as ≥50% stenosis.
dSevere stenosis of the contralateral carotid artery was defined as ≥70% stenosis.
Intergroup comparison of baseline characteristics
Age (X1) was treated as a continuous variable. The Kolmogorov–Smirnov test indicated that the age data in the experimental group did not follow a normal distribution (P = 0.009). Therefore, the Mann–Whitney U test was applied, revealing no statistically significant difference in age between the two groups (U = 231.000, z = –0.035, P = 0.972).
The degree of carotid artery stenosis on the operative side (X7) was also a continuous variable. As the data in both groups were non-normally distributed (P = 0.000 in the control group; P = 0.038 in the experimental group), the Mann–Whitney U test was used and showed no significant intergroup difference (U = 206.000, z = –0.637, P = 0.524).
Follow-up time (t), treated as a continuous variable, did not follow a normal distribution and was therefore summarized as median (IQR) and compared between groups using the Mann–Whitney U test. A statistically significant difference in follow-up duration was observed between the two groups (U = 93.500, z = –2.751, P = 0.005).
The remaining variables—gender (X2), smoking status (X3), underlying diseases other than cerebrovascular diseases (X4), history of stroke or other cerebrovascular diseases (X5), long-term use of antiplatelet drugs (X6), stenosis or occlusion of the ipsilateral external carotid artery (X8), and severe stenosis of the contralateral carotid artery (X9)—were treated as categorical variables and compared using chi-square tests.
Based on these analyses, there were no statistically significant differences in any of the baseline characteristics between the control and experimental groups, except for follow-up time (t), which was longer in the control group (P = 0.005). See Table 5 for details.
Comparison of perioperative indicators between groups
Perioperative parameters, including operative time, carotid clamping time, intraoperative blood loss, and postoperative wound drainage, were compared directly between the clip and suture groups. The clip group had a significantly shorter carotid clamping time and lower intraoperative blood loss than the suture group. No statistically significant differences were observed in total operative time or postoperative wound drainage volume. Detailed results are presented in Table 3.
Comparison of postoperative stroke incidence and all-cause mortality between groups
Perioperative stroke, defined as stroke occurring within 30 days after surgery, occurred in 4/46 procedures (8.7%). Fisher’s exact test showed no statistically significant difference in perioperative stroke incidence between the two groups.
For long-term stroke incidence, Kaplan–Meier analysis with the log-rank test showed no statistically significant between-group difference (log-rank P = 0.210; Figure 3). Kaplan–Meier analysis of long-term postoperative stroke incidence.
All-cause mortality was reported descriptively. Because of the limited number of death events, no multivariable survival regression was retained in the revised analysis.
Discussion
In this single-center exploratory retrospective cohort study of classic carotid endarterectomy (CEA) with primary closure, clip-assisted closure was associated with shorter carotid clamping time and lower intraoperative blood loss than continuous suturing. Total operative time and postoperative drainage were similar between groups. During follow-up, no statistically significant between-group differences were detected in perioperative stroke, long-term stroke, restenosis/occlusion, or all-cause mortality. However, given the small sample size, particularly the 15 procedures in the clip group, and the non-randomized design, these findings should be interpreted as hypothesis-generating rather than evidence of equivalence or non-inferiority.
Influence of vascular clips on clamping time and operative duration
Previous experimental and clinical studies have generally shown that clip-based vascular closure or anastomosis can shorten closure or anastomotic construction time compared with suturing, particularly when compared with interrupted techniques.13,16–20 Our findings are directionally consistent with this literature. In the present cohort, the clip group had a significantly shorter carotid clamping time than the suture group.
By contrast, total operative time did not differ significantly between groups. A plausible explanation is that carotid arteriotomy closure represents only one component of the overall procedure, whereas exposure, plaque removal, hemostasis, and wound closure were otherwise similar between groups. In addition, the present study may have been underpowered to detect modest differences in total operative duration. A shorter carotid clamping time may still be clinically relevant, particularly in patients with limited collateral reserve or significant contralateral carotid disease. 21
Influence of vascular clips on intraoperative blood loss and postoperative wound drainage
The lower intraoperative blood loss observed in the clip group is biologically plausible and is consistent with earlier reports suggesting that clip-based closure may reduce bleeding from repeated suture-hole punctures.3,22,23 In our cohort, however, this difference did not translate into a significant difference in postoperative drainage volume.
One possible explanation is that 24-hour wound drainage reflects not only closure-line bleeding but also soft-tissue exudation from the operative field. Therefore, reducing immediate needle-hole bleeding may not necessarily change total postoperative drainage. In addition, continued antiplatelet therapy did not significantly increase intraoperative blood loss in our regression analysis, which is consistent with contemporary carotid surgery guidance supporting continuation of antiplatelet therapy in appropriate patients. 24
Impact of vascular clips on complications, stroke, restenosis, and mortality
Prior studies in other vascular beds have generally not shown an obvious increase in complication rates with clip-assisted closure, although isolated adverse events have been reported, particularly when clip selection or application was suboptimal.13,23,25–27 In the present cohort, perioperative stroke occurred in 4/46 procedures (8.7%), with three events in the suture group and one in the clip group; one additional late stroke occurred during follow-up. Imaging follow-up in 36 patients identified three cases of restenosis or occlusion, none of which were associated with new neurologic symptoms.
No statistically significant between-group differences were detected for perioperative stroke, long-term stroke, or all-cause mortality. However, these findings should be interpreted cautiously. Because the total sample was small, particularly the 15 procedures in the clip group, the study had limited power for uncommon but clinically important safety endpoints. Accordingly, the absence of statistically significant differences should be understood as no signal detected, rather than evidence of equivalent safety or non-inferiority.
All observed deaths occurred in the suture group, but this pattern should not be overinterpreted because follow-up duration was longer in that group and the number of events was small. Given the limited number of death events, no robust multivariable analysis of mortality was retained in the revised manuscript.
Potential mechanisms underlying the observed effects of vascular clips
Mechanistically, clip-assisted closure may reduce local tissue trauma, avoid repeated needle-hole bleeding, and lessen foreign-material exposure associated with conventional suturing. Experimental studies of clip-based vascular closure have reported better preservation of endothelial integrity, less compliance mismatch, and less intimal thickening than conventional suturing in some models.18,19,22,28–30 These observations provide a plausible explanation for the shorter clamping time and lower blood loss observed in our series and suggest a potential benefit for long-term patency. However, whether such histologic or biomechanical advantages translate into clinically meaningful reductions in restenosis or stroke in CEA remains uncertain and requires larger human studies.
Limitations of the present study
Several limitations merit emphasis
First, this was a non-randomized retrospective study. Treatment allocation was influenced not only by clinical judgment but also by patient/family preference, insurance coverage, and affordability of the clip system. This introduces a substantial risk of selection bias and confounding by indication/affordability. This issue is also clinically relevant in the broader vascular surgery literature, because cost differences between clip- and suture-based closure have been shown to influence the economic attractiveness of clip use even when short-term clinical outcomes appear similar in other settings such as arteriovenous fistula creation. 31 Although measured baseline variables were broadly similar between groups, unmeasured factors such as socioeconomic status, risk tolerance, health literacy, and decision-making preferences may have influenced both treatment choice and outcomes.
Second, the overall sample size was small, particularly in the clip group (15 procedures). As a result, the study had limited statistical power for rare but clinically important endpoints such as perioperative stroke, long-term stroke, restenosis/occlusion, and all-cause mortality. Therefore, the absence of statistically significant between-group differences should not be interpreted as proof of equivalence or non-inferiority.
Third, clip-assisted procedures were introduced later in the study period, resulting in shorter follow-up in the clip group and potential time-related confounding. Although all operations were performed by the same experienced surgeon using a standardized approach, changes in perioperative management or institutional practice over time cannot be excluded.
Fourth, only classic CEA with primary closure was included. Patch angioplasty and eversion techniques were excluded, even though patch closure has been associated with lower restenosis rates and is recommended in contemporary guidelines.24,32 This improved internal consistency for a device-focused exploratory comparison but limits generalizability. In addition, we previously observed incompatibility between the GC-L clip and certain synthetic patch materials used in our institution, which precluded safe clip-assisted patch closure in this cohort. Future studies should evaluate clip-assisted closure in conjunction with compatible patch materials and broader CEA techniques.
Fifth, follow-up was not uniform for all patients. Some long-term information was obtained by telephone, imaging was partly performed at outside institutions, and five patients—all in the suture group—were lost to follow-up. These factors may have affected event ascertainment and reduced the precision of long-term comparisons.
In summary, this study provides long-term exploratory data suggesting that clip-assisted primary closure is technically feasible in selected patients undergoing classic CEA and may improve intraoperative efficiency. However, because of the non-randomized design, small sample size, and follow-up limitations, these findings should be regarded as hypothesis-generating. Larger prospective studies are needed before broader conclusions can be drawn regarding the safety and effectiveness of clip-assisted primary closure in carotid surgery.
Conclusion
In this exploratory, non-randomized cohort study, clip-assisted primary closure during classic carotid endarterectomy was associated with shorter carotid clamping time and lower intraoperative blood loss than conventional suturing. No signal of increased perioperative or long-term adverse outcomes was detected; however, the study was not powered to establish equivalence or non-inferiority for rare safety endpoints. These findings suggest that clip-assisted closure is technically feasible in selected patients undergoing classic carotid endarterectomy.
Because of the small sample size, non-randomized single-center design, and potential residual confounding, the results should be interpreted as hypothesis-generating. Larger prospective studies are needed to further evaluate the safety and long-term effectiveness of clip-assisted primary closure in carotid surgery.
Supplemental material
Supplemental material - Vascular clips for primary closure in classic carotid endarterectomy: A 5-year exploratory retrospective cohort study
Supplemental material for Vascular clips for primary closure in classic carotid endarterectomy: A 5-year exploratory retrospective cohort study by Kang She, Xiansheng Zhang, Zhengheng Yu, Jie Yin and Gong Cheng in Science Progress.
Footnotes
Acknowledgements
During the preparation of this manuscript, the authors used ChatGPT-5.3 and ChatGPT-5.4 for language translation, English polishing, grammar checking, and improvement of sentence fluency. After using these tools, the authors carefully reviewed, revised, and verified all text. The authors take full responsibility for the content and accuracy of this publication.
Consent to participate
Informed Consent Statement: Written informed consent was obtained from all patients prior to surgery. For postoperative follow-up, verbal or telephone consent was obtained from the patients and documented in the medical records.
Author contributions
Concept construction: S.K., Z.X.S. Methodology design: S.K., Z.X.S. Resource provision: Z.X.S., Y.J., S.K. Verification and implementation: Z.X.S., Y.J., C.G., S.K. Initial draft writing: S.K. Data analysis: S.K., Y.Z.H. Manuscript review and editing: S.K., Y.Z.H. Follow - up survey research: S.K. Data management and analysis: S.K., Y.Z.H. Project supervision: Z.X.S. Project management: S.K., Z.X.S. Surgical operations: Z.X.S., Y.J., S.K., C.G. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National High Level Hospital Clinical Research Funding (Scientific Research Seed Fund of Peking University First Hospital) (No. 2023SF03).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article are not publicly available because of patient privacy and ethical restrictions. De-identified data may be made available from the corresponding author upon reasonable request and with permission from the relevant ethics committee and institution.
IRB approval
Institutional Review Board Statement: This study was approved by the Biomedical Research Ethics Committee of Peking University First Hospital, Beijing, China (approval No. 2025R0292-0002; approved on August 12, 2025). All patient details were de-identified and anonymized prior to analysis and reporting.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.