
Abstract
For patients with arteriovenous fistulas, venous stent placement is indicated when angioplasty fails to alleviate hemodialysis access stenosis. Stent migration from the peripheral vasculature into the cardiac chambers, though rare, constitutes a serious complication. We report the case of an early 70s Chinese male with hemodynamically significant venous stenosis compromising dialysis access, who underwent venous stent implantation. Two weeks later, during readmission for a fracture, transthoracic echocardiography incidentally revealed cardiac embolization of the stent. Using endovascular techniques, the stent was successfully retrieved from the heart and translocated to the left common iliac vein. Follow-up echocardiography 1 week postprocedure demonstrated no worsening of cardiac function or tricuspid regurgitation. This case illustrates that endovascular retrieval and relocation of a cardiac-embolized venous stent is a feasible, safe, and minimally invasive strategy. The application of endoscopic grasping forceps to achieve transcatheter stent translocation to the iliac vein offers a novel alternative to surgical intervention, potentially avoiding the need for sternotomy.
Introduction
Upper extremity venous stenosis represents a major contributor to hemodialysis dysfunction in patients with end-stage renal failure. To maintain access patency, stent implantation is often considered, especially for central venous lesions refractory to angioplasty. 1 A rare but consequential complication is stent migration into the right heart. Such an event poses immediate risks of cardiac injury, valvular damage (particularly tricuspid regurgitation), and thrombotic complications, potentially culminating in heart failure if untreated. 2 Management remains nonstandardized. Traditional retrieval via median sternotomy carries significant morbidity, including risks of stroke, pericardial hematoma, and valvular injury.3,4 Endovascular retrieval using a combination of a large-bore sheath, balloon, and snare has been reported as a less invasive alternative. 5 This report describes a further evolution of an endovascular approach. We present a case of subclavian vein stent migration to the right ventricle, causing significant tricuspid regurgitation, which was successfully managed by translocating the stent to the iliac vein using a novel endoscopic forceps technique, thereby averting the need for sternotomy.
Case report
An early 70s male patient was presented to Jinhua People's Hospital (Zhejiang, mid-2025) with elevated venous pressures during hemodialysis sessions. Imaging confirmed significant stenoses of the subclavian and innominate veins. He subsequently underwent a successful deployment of a 12 mm × 60 mm Wallstent™ self-expanding stent. Postprocedural hemodialysis venous pressures returned to normal.
Two weeks later, the patient was admitted to the orthopedic service for management of a traumatic fracture following a fall. A routine preoperative transthoracic echocardiography unexpectedly identified the stent lodged across the tricuspid valve, resulting in severe valvular regurgitation (Figure 1). Chest computed tomography was performed for further anatomical assessment. Following a multidisciplinary team discussion, endovascular retrieval was selected as the primary intervention, with surgical standby via sternotomy arranged in case of percutaneous failure.
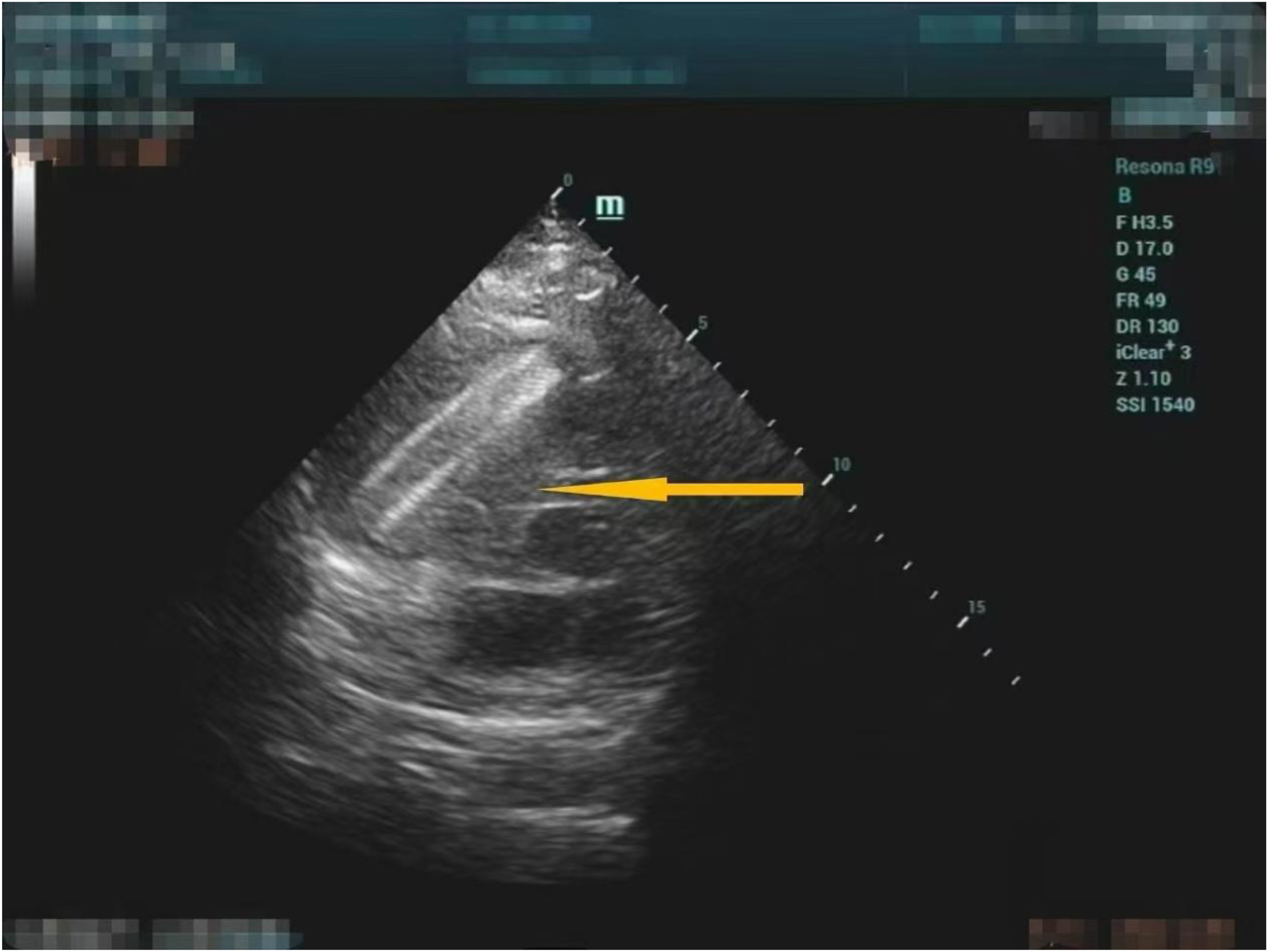
Transthoracic echocardiography showed the migrated stent straddling the tricuspid valve (stent location indicated by the yellow arrow).
The procedure was conducted in a hybrid operating room with cardiothoracic surgery on standby. Initial attempts via right internal jugular vein access, utilizing a 7F long sheath and endoscopic forceps under fluoroscopy, failed to engage the stent. The approach was then switched to femoral venous access. Despite upsizing to an 8F sheath, direct grasping attempts remained unsuccessful. The forceps tip was deemed too rigid for optimal manipulation within the cardiac chambers, raising concerns for potential tissue injury. A revised strategy was therefore adopted: a guidewire was advanced through the stent lumen, followed by a 5.5F thrombectomy catheter and inflation of a 14 mm × 80 mm balloon within the stent to provide anchorage. While traction on these devices did not fully dislodge the stent, it achieved critical positional realignment. Capitalizing on this improved orientation, the forceps were then able to securely engage the stent and retract it to the superior vena cava (Figure 2).

Under digital subtraction angiography (DSA) guidance, the stent was engaged with endoscopic grasping forceps and retrieved into the vena cava.
Subsequent attempts to capture and retrieve the stent entirely via a left common femoral approach using an AngioJet™ system and a snare were thwarted by the snare's inadequate size for the stent diameter. As a result, a 6 cm oblique incision was made in the left groin to expose the common femoral vein under direct vision. Applying traction via the forceps under fluoroscopic guidance, the stent was successfully translocated distally and anchored within the left common iliac vein, where further advancement was prevented by its expansion (Figure 3). Completion venography confirmed patent venous flow with mild focal stenosis at the stent site. No device fragmentation occurred.

The stent was ultimately translocated and anchored within the left common iliac vein using endoscopic grasping forceps.
Postoperative echocardiography showed residual moderate tricuspid regurgitation. The patient remained asymptomatic, and surveillance echocardiography at 2 weeks demonstrated stable valvular function without progression (Figure 4). Serial Doppler studies confirmed stable stent position in the left iliac vein. The patient was discharged on a lifelong anticoagulation regimen to prevent stent thrombosis. Postoperatively, the patient was administered low-molecular-weight heparin 0.3 mL subcutaneously every 12 h until discharge, was then transitioned to rivaroxaban 15 mg orally once daily for 3 months, and subsequently maintained on lifelong anticoagulation with rivaroxaban 10 mg orally once daily.

Follow-up echocardiography at 2 weeks demonstrated preserved valvular function without worsening of tricuspid regurgitation.
Informed consent was obtained for the treatment and publication. Patient anonymity has been preserved. This case report adheres to CARE guidelines. 6
Discussion
Patients with end-stage renal disease depend on reliable hemodialysis access, typically via an arteriovenous fistula. The development of central venous stenosis is a major cause of access dysfunction, often necessitating stent placement when angioplasty fails to sustain adequate flow.
Stent migration to the heart, while rare, represents a serious complication of venous stenting. Although less common with upper extremity than with iliac or renal vein stents, 7 it can lead to severe consequences such as arrhythmias, 8 heart failure, 9 and cardiac perforation. 10 Management has traditionally involved a choice between percutaneous retrieval with endovascular tools5,11 and open surgical extraction for complex cases.12,13
In our elderly patient with multiple comorbidities, sternotomy was considered high risk. Our initial plan to use a combined snare–balloon technique was limited by the lack of sufficiently large snares (≥25 mm) at our institution. We therefore employed endoscopic grasping forceps. While complete retrieval was not achieved, we successfully translocated the stent from the tricuspid valve to the iliac vein, avoiding open surgery. This procedure, though minimally invasive, carries inherent risks of cardiac or valvular injury, demanding extreme caution.
Intraoperatively, the forceps provided excellent grip on the stent fabric, suggesting particular utility for retrieving covered stents. However, their sharp jaws pose a significant risk of iatrogenic injury, requiring very controlled manipulation. When a stent is entangled in the tricuspid apparatus, we recommend first passing a guidewire through its lumen to create a stable rail. Wire selection is critical: an overly stiff wire may propel the stent deeper into the ventricle, while a soft one may not support safe traction.
For future cases, a multimodal endovascular approach—perhaps combining a large snare with grasping forceps—may improve success rates. Patient selection remains paramount. Endovascular retrieval may be prohibitively risky for very large stents or those that have migrated deeply into the right ventricle or pulmonary artery, where complication risks are substantially higher.
Conclusion
In conclusion, maintaining a high index of suspicion for stent migration is crucial following venous stenting for hemodialysis access. When migration occurs, endovascular retrieval offers a safe, minimally invasive alternative to surgery. This case illustrates a novel application of endoscopic grasping forceps to achieve controlled translocation of a cardiac-embolized stent into the iliac vein. This approach successfully avoided sternotomy and provides a valuable paradigm for managing this rare but serious complication.
Footnotes
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Author contributions
XQW and PZ—concept or design; PZ—acquisition of data; PZ—analysis or interpretation of data; PZ and XQW—drafting of the article; XQW—critical revision for important intellectual content. Both authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Key Program of Jinhua Science and Technology Bureau (Grant No 2023-3-088).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data generated in the present study may be requested from the corresponding author.