
Abstract
Flatfoot, a disorder defined by the flattening or loss of the medial longitudinal arch (MLA), affects approximately 15.6% of the child population. It may result from congenital or acquired dysfunction of muscles, tendons, or ligaments in the foot and ankle, as well as skeletal abnormalities. Clinically, this disorder manifests as foot pain, gait abnormalities, and compensatory injuries in lower limb joints (e.g., knee and hip), thereby affecting motor function and quality of life. Short foot exercises (SFE) as a noninvasive rehabilitation strategy enhances arch height and improves dynamic foot support by actively contracting plantar muscles. It has been confirmed to effectively improve foot morphology and alleviate pain. This is a narrative review that summarizes the impact of flatfoot on patient health and the benefits of SFE-based interventions by focusing on the morphological, functional, and biomechanical characteristics of flatfoot, the standardized intervention cycles and assessment approaches for SFE as well as the mechanism(s) by which SFE alleviates flatfoot-related symptoms.
Introduction
Flatfoot is defined as the collapse of the medial longitudinal arch (MLA) induced by physiological or pathological factors that are either congenital or acquired. The MLA evolution is pivotal for human upright walking, and its stability hinges on mechanical support from passive elastic tissues, notably the plantar fascia. 1 Individuals with flatfoot typically show hyper-pronation and diminished dynamic arch support; biomechanically, this manifests as notable decrease in foot longitudinal stiffness, directly impairing propulsion in walking and running. Tests on explosive power and dynamic balance indicate children with flatfoot perform significantly worse than normal children. 2 Besides MLA collapse, flatfoot is also intricately associated with arch functional deficiencies: via intermetatarsal tissues, the transverse arch adds over 40% to the foot longitudinal stiffness. 3 Flatfoot patients have excessive weight-bearing pronation due to insufficient transverse metatarsal arch curvature or pathological metatarsal mobility,4,5 which causes lower limb mechanical alignment deviation, imposes torsional stress on knee/hip joints, and escalates risks of foot pain and secondary knee arthritis.6,7
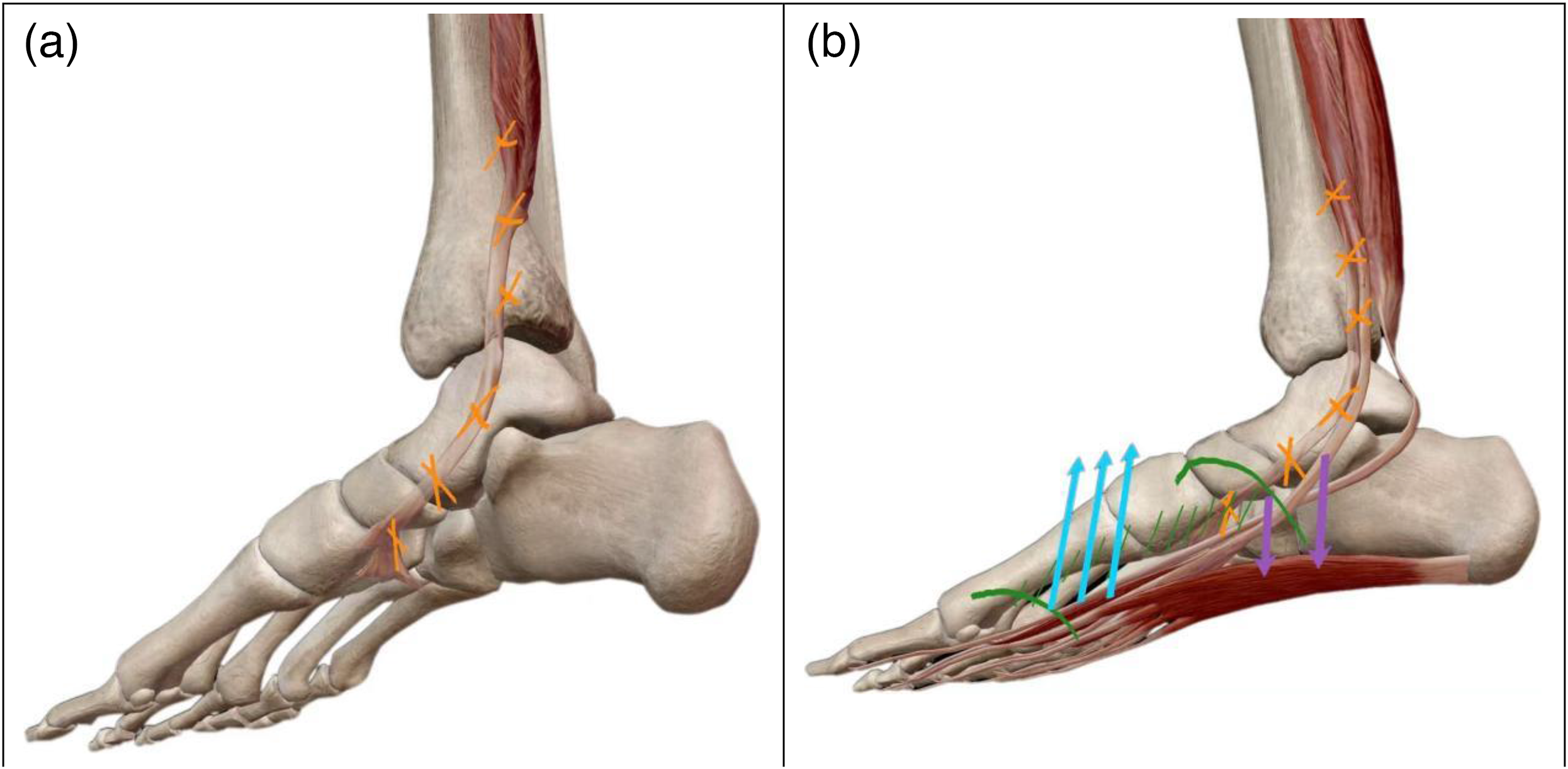
Short foot exercise (SFE) is a therapy to boost medial arch support by strengthening intrinsic plantar muscles. Its key mechanism involves voluntary contraction of the foot's deep muscles, shortening metatarsals toward the calcaneus to lift the arch. As shown in Figures 1 and 2, it is crucial to avoid toe flexion for achieving independent muscle control.8,9 The training includes the basic and advanced stages: the basic stage requires participants to sit or stand with their feet flat on the ground, 10 contracting the plantar muscles to sustain arch shortening effect for 5 to 10 seconds (repeating in 3 sets with 10 repetitions/set) ; the advanced stage incorporates squats or single-leg standing to further enhance functionality. Real-time feedback from electromyography (EMG) or musculoskeletal ultrasound should be utilized to adjust the exercise focus and boost the accuracy of muscle activation.11,12

Short foot exercise (SFE) training approaches. Perform active plantar muscle contraction to draw the metatarsal toward the calcaneus, lift the foot arch, inducing the “short foot” effect. ①: Tibia, ②: Talus, ③: Navicular, ④: Medial Cuneiform, ⑤: Metatarsal, and ⑥: Calcaneus.
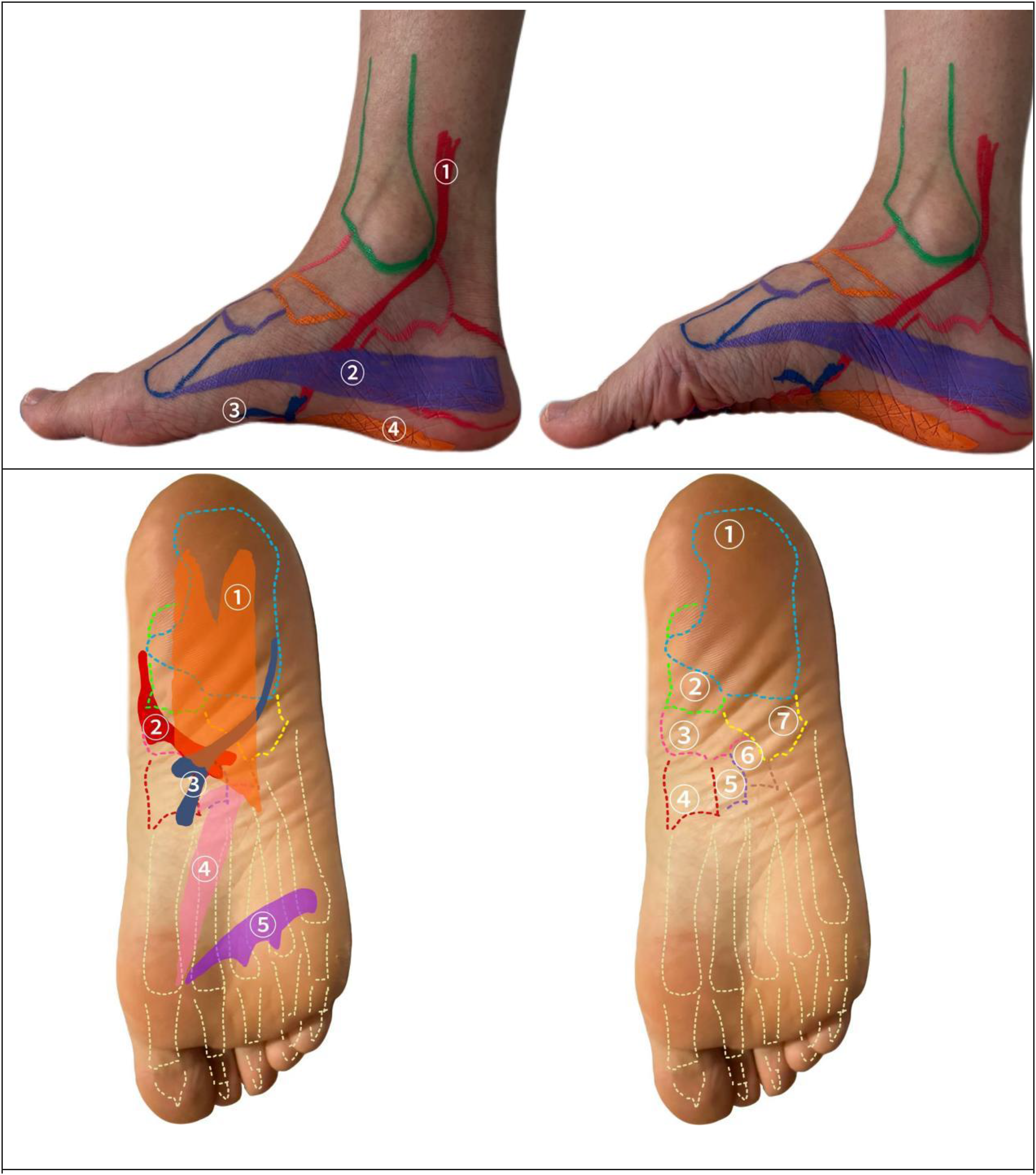
Muscles activated in SFE. Strengthening plantar muscles leads to an increase in the strength and height of the MLA.
SFE is primarily applied to painful conditions and enhancing kinetic chain efficiency during sports. Researches show SFE notably decreases foot valgus angle, elevates navicular height, and alleviates pain. 13 Moreover, it enhances the stability of hip and knee by strengthening foot intrinsic muscle. Combined with electrical stimulation therapy, it notably boosts the foot muscle recovery in elderly patients with severe muscle atrophy. 14 It also mitigates flatfoot-induced compensatory movement patterns and optimizes gait balance, stability, and lower limb biomechanical transmission.15–17
Intrinsic foot muscle training is key for improving flatfoot and widely used in clinical rehabilitation. There are various low-cost, noninvasive methods, including toe-spread exercises, SFE, and toe-gripping exercises. Among them, toe-spread exercises are widely used in community rehabilitation for their simplicity. Studies prove their effect on improving toe abductor strength but with weak targeted effects on the MLA. 18 This study focuses on SFE due to its unique clinically proven training advantages: it precisely targets the muscles around the MLA, enhances arch support static/dynamic arch support, and improves dynamic foot stability. These advantages offer a differentiated value from other methods. Therefore, SFE was selected as the core research object to explore its application effects in flatfoot intervention.
This is a narrative review aiming to summarize current research on SFE for flatfoot and offer guidelines for prospective research agendas. Its scope covers flatfoot's epidemiology, anatomical/pathophysiological/biomechanical traits, diagnostics, and complications—paired with the standardized protocols, therapeutic efficacy, limitations, and future directions of SFE as a targeted intervention. It is guided by the Scale for the Assessment of Narrative Review Articles (SANRA) 19 to ensure methodological quality and rigor.
This review searched English databases including PubMed, Cochrane Library, Embase, and PEDro for evidence on SFE in flatfoot therapy, using synonyms for flatfoot and SFE (with applicable MeSH terms). Relevant English literature was included, focusing on SFE for flatfoot (with outcomes including arch height, foot pain, and biomechanics), while excluding severe rigid flatfoot, SFE + surgery studies, and duplicates.
Overview of flatfoot
The epidemiology of flatfoot
Ethnic disparities in flatfoot
Flatfoot prevalence and characteristics vary notably across ethnic groups. A senior high school survey in Beijing, China, found a 5.5% prevalence; 20 a large-scale South Korean study (sample size = 560,141) of 19-year-old male recruits showed 2.9% prevalence (with 0.9% being moderate-to-severe). 21 A multivariate analysis indicated that Asians have 2.34 times the flatfoot risk of the Caucasians, 22 possibly due to genetic reasons and/or foot morphological variations. Skeletal deformities and comorbidities are also strongly correlated. Studies also show that Black participants demonstrate more conspicuous flatfoot traits: lower arch height index, greater ankle valgus index, and higher rate of overpronation. 23
Sex and age variations in flatfoot
Concerning sex variations in flatfoot, males have a higher risk than females, 24 but conflicting studies find no sex variations possibly due to diagnostic discrepancy.20,22,25 Flatfoot affects 15% of children under 15, with boys having a higher incidence. 26 Most childhood cases are asymptomatic and flexible; only a few need intervention due to pain or gait issues. 27 Those with comorbid foot pathologies (e.g. cerebral palsy and congenital clubfoot) should be prioritized for treatment over healthy asymptomatic children. Adult-acquired flatfoot deformity (AAFD; also referred to as Progressive Collapsing Foot Deformity, PCFD—a consensus term proposed by Cesar de Cesar Netto and Scott J. Ellis et al. in 2019 to describe the progressive nature of the deformity) mainly affects middle-aged to elderly females, causing foot pain, malalignment, and dysfunction. Its main cause is degeneration of Posterior Tibial Tendon (PTT). The PTT, a key midfoot structure, normally grips arch bones and works with peroneus longus and tibialis anterior tendons for dynamic arch support. The PTT degeneration involves tenosynovitis, tendinopathy, elongation, and tendon tear. While the arch is flexible initially when collapsing, the foot stiffens as the disease advances. Sex differences of AAFD/PCFD may stem from social roles (e.g. footwear habits), hormones, and muscle strength. 28
Other risk factors related to flatfoot
Obesity is a major risk factor where a rise in body mass index (BMI) worsens arch collapse by altering foot biomechanics. Footprint analysis and clinical evaluations show that the prevalence is around 17.5% in normal-weight children, versus 26.9% to 30.8% in overweight and obese children.24,26 A study in Ethiopia shows that overweight and obese children are 2.8 and 4.1 times more likely to develop flatfoot than their normal-weight peers. 24 Almost all studies link children's flatfoot prevalence to increased BMI. 29 Moreover, lack of physical activity, prolonged use of shoes limiting foot mobility, and living at high altitudes are also risk factors for flatfoot. For instance, 11- to 18-year-old children in high-altitude and urban areas are more susceptible to flatfoot. 30 A plantar fascia disease study identified two related gene variants via genome-wide association analysis: an insertion-deletion in Tumor Necrosis Factor Alpha-Induced Protein 8 (TNFAIP8) and a single-nucleotide polymorphism in WW Domain containing E3 Ubiquitin Protein Ligase 2 (WWP2). 31 Though this study focuses on plantar fascia disorders, similar genetic mechanisms may affect flatfoot. Genetics also impact the biomechanics of flatfoot, because those with higher dynamic foot inversion respond better to customized arch supports, 32 implying that genetic factors impact foot morphology and responses to external interventions.
Anatomy, pathophysiology, and biomechanics of flatfoot
Flatfoot is a complex pathological disorder caused by the interaction of skeletal structural abnormalities, soft tissue dysfunction, and biomechanical changes. 1 Its core mechanism involves the combined effect of the MLA collapse and the PTT dysfunction, which impairs static arch support and disrupts kinetic disorders. A weight-bearing three-dimensional (3D) computed tomography (CT) scan reveals that flatfoot has significantly lower values in the calcaneal-fibular distance, sagittal and transverse calcaneal inclination angles, medial column height, sagittal and axial coverage angles, and sagittal and transverse hibb angles. Among them, the sagittal hibb angle and medial column height are key risk factors for flatfoot. 7
Flatfoot pathophysiology involves complex biomechanical anomalies and soft tissue dysfunctions, and the major ones are as below.
The PTT degeneration damages secondary support structures (e.g. plantar fascia), reduces medial arch support, and causes the collapse of talonavicular joint (Figure 3(a)). 28
Biomechanical mechanisms of flatfoot injury. (a) Injury to the tibialis posterior tendon impairs secondary support structures like spring ligament, leading to descent of the navicular and talus. (b) Descent of the talonavicular joint and midfoot collapse leads to forefoot overload, triggering a surge in pressure on the second and third metatarsals.
The 3D osseous morphological changes (e.g. abnormalities of the talus and calcaneus lead to arch collapse and subtalar joint valgus), together with kinematic abnormalities of the talonavicular joint, form a biomechanical pattern of “midfoot collapse-forefoot overload”, increasing pressure on the 2nd and 3rd metatarsals (Figure 3(b))7,33; congenital intertarsal fibrous/osseous coalitions may result in rigid flatfoot, limiting normal foot function and inducing pain.34,35
Laxity of the plantar fascia and spring ligament complex weakens the foot arch's passive support, inducing excessive pronation and typical deformity.36,37
Abnormal dynamic stability of intrinsic plantar muscles disrupts rigid lever mechanism during foot propulsion, worsening MLA collapse.38,39 Muscles like abductor hallucis and flexor digitorum brevis maintain arch rigidity via coordinated contraction, especially during gait propulsion; their atrophy/dysfunction causes MLA collapse, along with increased subtalar joint valgus and abnormal calcaneal valgus angle. 40
A finite element analysis shows that under plantar pressure, flexible flatfeet have higher biomechanical stress on the calcaneofibular ligament, posterior talofibular ligament, talocalcaneal joint, talonavicular joint, medial cuneonavicular joint, and first tarsometatarsal joint than normal feet. This accelerates degenerative lesions in ligamentous and articular surfaces. 41 With loss of dynamic stability, the foot fails to disperse stress efficiently during weight-bearing, triggering biomechanical compensation.39,42,43 Abnormal concentration of joint reaction forces and plantar stress accelerates cartilage degradation and may induce flatfoot-related complications.
Visible Body Suite (Version 4.31) [Computer software]. (2023). Retrieved January 30, 2023 from www.visiblebody.com
Categories of flatfoot
Flexible flatfoot is defined by MLA collapse and reduced elastic modulus, with reducible arch recovery in nonweight-bearing positions. Clinically, it is often asymptomatic or causes mild fatigue, with normal joint mobility that typically exceeds physiological limits due to ligamentous laxity. Anatomical findings include tibial internal rotation, calcaneal valgus, and forefoot abduction, leading to dynamic arch support failure. 44
Rigid flatfoot causes fixed deformities due to structural pathologies (such as talocalcaneal coalition or osteoarthritis). Biomechanically, joint mobility loss leads to rigid load concentration, 7 causing significant increase of posterior reaction forces, reduced energy absorption, decreased elastic modulus45,46 and a significant spike in peak knee adduction forces during gait, 47 contributing to flatfoot complications.
The key differences between flexible and rigid flatfoot lie in reducibility, etiology (muscle/ligament abnormalities vs. osseous lesions), and biomechanical effects. Clinical diagnosis combines imaging (CT/weight-bearing X-rays for osseous assessment) and ink print/pressure plate tests. Clinically, the flexibility and rigidity of the foot arch can further be assessed via arch height flexibility. A standardized classification system categorizes arch flexibility into five levels: very stiff, stiff, neutral, flexible, very flexible. 48 Biomechanically, this method has been applied to explore foot arch flexibility's correlation with ground reaction force distribution. 49
For treatment, flexible flatfoot mainly uses orthotics and muscle training, while rigid flatfoot often needs surgery for mechanical stability. In children under 6, flexible flatfoot is usually normal (incomplete arch development), but rigid flatfoot indicates congenital deformities requiring early intervention. In adults, rigid flatfoot is often linked to degenerative changes, needing surgical evaluation. Overall, medical history, physical examination, and imaging are essential to distinguish reducible from structural abnormalities for treatment planning.
Artificial intelligence application in flatfoot diagnosis
Artificial intelligence (AI) is a transformative tool in flatfoot diagnosis, enabling automated analysis of foot X-rays and/or plantar pressure images. Vision Transformer (ViT)-based deep learning models outperform traditional convolutional neural network (CNN) in classifying “flatfoot” or “nonflatfoot” foot images.50,51 Integrated with plantar pressure scanners, AI quickly detects arch collapse and aids diagnosis by quantifying pressure patterns. 52 In measuring key foot parameters (e.g. navicular/arch height), AI's accuracy and reliability match or exceed clinical specialists’, reducing human measurement errors in foot structure evaluation and ensuring multicenter data consistency.53,54 A recent study using deep neural networks to estimate 3D foot bone kinematics reports average errors of 0.5 mm (position) and 0.6 degrees (orientation) versus actual values. This shows neural networks can noninvasively provide precise 3D kinematic data, aiding exploration of foot function and pathology in foot disorders. 55 Cost-wise, AI can diagnose via ordinary X-rays or even smartphone-captured foot images, independent of expensive professional devices. This makes it ideal for large-scale public health screenings and resource-poor regions. 51
Diagnostic investigation
Flatfoot can be diagnosed through the following core approaches: (1) biomechanical testing: it acquires ground reaction force data via force platform during patient movement, integrating with 3D motion capture (e.g. Vicon system) to evaluate gait abnormalities and muscle activity patterns; 56 (2) plantar pressure plates and ink-method: plantar pressure plates convert sensor signals to digital data, and record regional plantar pressure over time, 57 while the less sensitive ink method identifies arch collapse via footprints; (3) imaging examination: X-ray (measuring calcaneal angle, transverse arch-anterior arch angle, and transverse arch-posterior arch angle in weight-bearing position) serves as the gold standard for osseous structure evaluation,57,58 while ultrasound 59 and magnetic resonance imaging (for soft tissue lesion assessment) aid noninvasive diagnosis, and CT addresses complex malformations (e.g. tarsal coalition); (4) clinical assessment: it uses functional tests (navicular drop test/foot posture index, FPI) to distinguish flexible and rigid flatfoot, integrating symptoms and history to rule out neurogenic causes; (5) emerging technologies: finite element models simulate orthopedic intervention effects; wearable sensors monitor real-time dynamic pressure. In general, flexible flatfoot diagnosis relies on dynamic/static pressure plate analysis, while rigid flatfoot needs imaging to confirm osseous issues (e.g. vertical talus). Future trends focus on multimodal data (pressure-movement-imaging) for accuracy. (Notably, children's foot finite element models are limited due to open epiphyses and age-related skeletal heterogeneity.)
Flatfoot complications
Flatfoot complications stem mainly from its biomechanical traits. When walking or running, flatfoot patients’ navicular bone shows significant dorsiflexion, eversion, and external rotation relative to the talus, while the calcaneus has a larger eversion angle in mid-stance. These abnormal movements accelerate arch collapse, 33 concentrating stress in the mid and distal plantar fascia. Prolonged overstretching of the fascia 60 triggers plantar fasciitis and heel pain. 61 Flatfoot may reduce energy transfer efficiency during walking propulsion by lowering midfoot stiffness, 3 and its biomechanical features might enhance exercise compensatory mechanisms. 62 Chronic foot pronation further speeds up cartilage degradation in the subtalar and ankle joints, causing degenerative osteoarthritis. 28 A cross-sectional study of 95 middle-aged and elderly adults found that bilateral flatfoot is strongly linked to increased knee pain. 44 These complications impair motor function and quality of life, highlighting the need for early biomechanical intervention.
Benefits of SFE in flatfoot
Muscle strengthening
By activating intrinsic foot muscles (e.g. abductor hallucis and flexor digitorum brevis) via repetitive contractions, SFE directly enhances abductor hallucis cross-sectional area/volume, improves its mechanical properties (stiffness and elasticity), and boosts MLA static support. 63 Notably, the effectiveness of these improvements varies by arch flexibility: a study found that compared to rigid flatfoot, flexible flatfoot showed better abductor hallucis activation and arch angle improvements during SFE, supporting that SFE is more effective for flexible flatfoot. 9 It also raises navicular height, reduces foot pronation, and improves static (e.g. extended single-leg stance) and dynamic (e.g. running gait efficiency) balance. The benefits correlate with training cycles (significant effects observed in 4–8 weeks). 64 Studies show 6-week SFE training reduces navicular drop and foot inversion, while increasing midfoot plantar pressure, indicating better dynamic foot support.8,65 Another study compared exercises targeting the lateral and medial foot muscles, showing that corrective training for intrinsic foot muscles (including SFE) is more effective in improving foot muscle morphology and reducing navicular drop in boys with flatfoot. 66
Biomechanical optimization
SFE optimizes biomechanical function by redistributing plantar pressure, guiding it laterally to improve gait. 67 It reduces forefoot and hindfoot peak pressure and abnormal compensatory pressures. It lessens hindfoot eversion and forefoot abduction, thus optimizing lower limb alignment and alleviating knee and hip compensatory loads. With lower limb exercises like squats, it activates gluteal and core muscles, creating a kinetic chain synergy to boost dynamic balance. A randomized trial showed that, compared to single-foot exercises, 4-week foot-hip exercises reduced navicular drop, medial forefoot pressure and mediolateral displacement more significantly, and with a higher arch height; 8-week ones further reduced medial hindfoot pressure and anteroposterior displacement. Gluteus medius training added to foot exercises better supports MLA. 68
Improving neuromuscular control
Due to SFE's execution complexity, electrophysiological feedback (e.g. EMG-controlled stimulation) and ultrasonic feedback aid precise muscle activation and shorten the learning cycle. Electrophysiological methods monitor foot muscle activity (EMG) and joint movement, while ultrasonic feedback on talonavicular joint kinematics also shortens the cycle.11,69 High-arched athletes outperform others in the Star Excursion Balance Test (SEBT) and 40-yard dash, linking foot morphology to dynamic balance and speed. 70 SFE significantly improves dynamic balance and reduces ankle instability risk in patients with chronic ankle sprains after 4 weeks of training.71,72 It enhances lower limb motor control such as gait coordination and jump landing stability, especially in sports needing precise foot adjustments (e.g. soccer shooting, running).73,74 In stroke patients, it boosts walking speed, stride length, and dynamic balance scores (e.g. Dynamic Gait Index, DGI). 72
Pain relief and functional improvement
By strengthening foot support structures, SFE reduces excessive plantar fascia tension, relieving pain and enhancing walking ability. Randomized controlled trials confirm that SFE plus active interventions (e.g. lower limb strength training) outperforms passive approaches (e.g. orthotics). A 6-week SFE program significantly cuts foot pain scores (assessed via VAS/NPPRS); 8 pairing with insoles boosts relief and long-term function.15,75Combined with fascia release or minimalist footwear, it optimizes muscle activation—runners improve their FPI and functional movement scores after 6 weeks.17,76 Notably, flatfoot patients have higher knee pain than nonflatfoot individuals (11.3 vs. 6.58 points), 44 and SFE improves foot biomechanics to reduce knee loading, 77 enhance MLA support, and lower proximal joint compensation and second injury risks (e.g. patellofemoral pain).
Limitations of SFE
SFE needs precise activation of intrinsic foot muscles (e.g. abductor hallucis and flexor digitorum brevis) to shorten the foot and elevate MLA, but this is challenging for beginners due to muscle complexity. Inadequate activation causes excessive use of calf muscles (e.g. tibialis posterior and peroneus longus) and movement distortions (e.g. toe clawing and ankle inversion). 78 SFE also requires arch elevation only via plantar muscle contraction (no toe abduction or excessive plantar flexion), demanding good neuromuscular coordination—harder for those with poor foot proprioception (e.g. flatfoot patients). Around 30% of healthy subjects need multiple practices to master the correct pattern.10,79
Meta-analysis reveals disputes on SFE's efficacy in improving arch morphology, due to initial arch morphology (e.g. FPI), foot flexibility (e.g. rigid flatfoot), or training compliance.15,76,80 Current research shows moderate effects on flatfoot's arch height/plantar pressure, but via short-term (6–8 weeks) interventions; long-cycle prospective studies are essential.76,81 SFE works for mild flexible flatfoot (FPI 4–6) but not structural deformities or PTT dysfunction. Large-sample long-term follow ups are insufficient. Six-week trials show 30% to 40% pain reduction, but long-term data are lacking.7,52
Studies vary in outcome metrics (e.g. FPI, navicular height, and pain scores) and training methods, leading to high heterogeneity in meta-analyses. 80 Prospective follow ups are insufficient; traditional assessments miss dynamic gait fluctuations. Integrating 3D tech with plantar pressure monitoring would boost assessment validity. 11
Individual variations in SFE are evident: flexible flatfoot children benefit more than rigid flatfoot patients.9,82 Furthermore, efficacy is affected by deformity severity, age, routines, and neuromuscular control; SFE alone fails for Posterior Tibial Tendon Dysfunction. Most use 4- to 6-week cycles (3–5/week) but intensity differs; no adjustment consensus hinders use.8,63 Foot morphology and compliance impact outcomes,64,75 requiring personalized treatments.
SFE's biomechanical mechanisms are unclear, and there are debated SFE effects on foot kinetic chain (e.g. windlass mechanism and inconsistent evidence on gait arch stability), unstandardized training, costly inaccessible biofeedback,10–12 and limited SFE effects on healthy people's lower limb kinetics (in need of combination with other training).
Future directions
SFE can improve arch structure and lower limb alignment by enhancing the autonomous contraction of plantar intrinsic muscles, with clear efficacy in treating flexible flatfoot—and these structural improvements further translate to enhanced foot function, such as more stable foot movement during walking and optimized plantar pressure distribution. However, it faces challenges such as the lack of standardized training protocols, suboptimal efficacy in rigid flatfoot, no unified assessment tools, and insufficient long-term high-quality research. Further exploration of its application potential and resolution of these challenges are required.
First, standardized protocols should be developed. Determine training intensity for flatfoot based on weight-bearing X-rays, FPI, etc.; construct an intelligent monitoring system (integrating insole pressure sensors and machine learning), incorporate real-time biofeedback to improve movement precision; and establish treatment protocols and frequencies through qualitative–quantitative analysis. Second, conduct large-sample follow-up studies (≥6 months) to explore the sustained effects of SFE on arch stability (e.g. dynamic changes in navicular height) and gait; combine surface electromyography (sEMG) and ultrasound to analyze the synergistic activation patterns of plantar intrinsic muscles and lower limb kinetic chains. Third, integrate foot morphological features, electromyography data, gait characteristics, and genetic factors to build a therapeutic effect prediction model; combine orthopedic insoles and neuromuscular electrical stimulation (NMES), and use motion capture and pressure sensing to establish a “monitoring-feedback-adjustment” closed-loop. It is necessary to improve AI's ability in flatfoot diagnosis and dynamic foot function assessment. Fourth, develop stratified intervention strategies according to arch flexibility and needs of special populations (e.g. diabetic patients with microcirculatory disorders and athletes with plantar load requirements); extend research to overall lower limb function to explore SFE's compensatory effects on knee valgus and pelvic tilt, and quantify its advantages for motor performance. Lastly, multicenter randomized controlled trials are urgently needed to unify efficacy evaluation criteria, especially the weight allocation between FPI and pain scoring systems; expand application to the full cycle of flatfoot, implement early and comprehensive intervention, and build a “prevention-treatment-rehabilitation” pathway. Additionally, future research can further explore the application of SFE in managing AAFD/PCFD—investigating how stratified SFE protocols can target its progressive structural changes, and verifying the long-term effects of SFE on slowing deformity progression and improving functional outcomes.
In summary, the multidisciplinary integration of AI, biomechanics, etc., will promote the transformation of SFE from an empirically based practice to a precision-driven foot health optimization paradigm.
Footnotes
Acknowledgements
The authors would like to thank all participants in the literature retrieval process and the reviewers for their valuable comments.
ORCID iDs
Authors’ contributions
HY drafted the work, CL collected and analyzed data, KY and JY analyzed data, YW and CS interpreted data, PL revised the work, and HD designed the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
No datasets were generated or analyzed during the current study.