
Abstract
Objective
In recent years, the pericapsular nerve group (PENG) block and anterior quadratus lumborum block (aQLB) have emerged as regional anesthesia techniques commonly used for pain control after hip surgery. This study compared their analgesic efficacy during the first 48 hours following surgery under spinal anesthesia.
Methods
In this prospective, randomized, single-blinded study, patients were assigned to either the PENG (n = 43) or the aQLB group (n = 30). The primary outcome of the study was the total tramadol consumption within the first 48 hours postoperatively. Secondary outcomes included time to first rescue analgesia, resting and dynamic NRS pain scores at 2, 12, 24, and 48 hours postoperatively, and the incidence of complications.
Results
In this study, postoperative tramadol consumption within the first 48 hours was significantly lower in the PENG (96.74 ± 77.36 mg) compared to the aQLB group (196.33 ± 157.43 mg) (p = 0.004). Additionally, the time to first rescue analgesia was significantly longer in the PENG (9.03 ± 7.67 hours) than in the aQLB group (6.81 ± 6.70 hours) (p = 0.048). NRS scores were similar between the groups at all time points. Quadriceps weakness was not observed in any patient.
Conclusion
The PENG block provides effective postoperative analgesia without causing motor blockade, making it advantageous for early mobilization in patients undergoing hip surgery. It can be used as a part of multimodal analgesia.
Keywords
Background
Hip fractures are common in elderly patients and are often associated with high morbidity, mortality, and the need for surgical intervention. 1 These fractures typically result from falls and are frequently associated with osteoporosis and immobility. Intertrochanteric and femoral neck fractures are the most common types.
In this frail population, comorbidities and the risk of postoperative complications make effective pain management essential. Inadequate analgesia may increase the risk of cardiopulmonary complications, thromboembolic events, and delirium. 2 Effective pain control is also critical for early mobilization, a key component of enhanced recovery after surgery (ERAS) protocols. 3 Multimodal analgesia commonly includes paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs), opioids, and peripheral nerve blocks. Techniques such as epidural analgesia, femoral nerve block, and fascia iliaca compartment block provide effective analgesia and reduce opioid consumption. Consequently, they may help minimize opioid-related adverse effects such as nausea, vomiting, sedation, and respiratory depression. 4 However, these techniques may also cause motor blockade, thereby delaying patient mobilization.
To avoid these complications, motor-sparing regional techniques have gained increasing interest. Among them, the pericapsular nerve group (PENG) block and the anterior quadratus lumborum block (aQLB) have emerged as promising options for providing sensory analgesia in hip surgery.
The PENG block, first described by Girón-Arango et al. 5 targets the femoral, obturator, and accessory obturator nerves to relieve anterior hip joint pain. 6 The hip joint is a synovial joint formed by a ball-and-socket articulation between the femoral head and the acetabulum. A fibrocartilaginous structure called the labrum covers the articular surfaces. Joint stability is maintained by the fibrous capsule, ligaments, and surrounding muscles. The hip is one of the largest and most mobile weight-bearing joints in the human body. It receives innervation from both the lumbar and sacral plexuses. The sensory innervation of the anterior joint capsule is primarily provided by the femoral nerve, obturator nerve, and accessory obturator nerve. 7 The posterior capsule is innervated by the L4–S1 nerve roots and may also receive branches from the superior gluteal and sciatic nerves. 8 The anterior capsule is considered the primary source of hip joint pain due to its higher density of nociceptors and mechanoreceptors. 9
The anterior QLB, introduced by Borglum et al., 10 has been shown to provide both somatic and visceral analgesia.11–15 Although QLB has been widely used in cesarean sections and gynecological procedures to provide effective analgesia for lower abdominal surgeries, cadaveric studies have shown that anterior QLB may potentially provide analgesia across the T10 to L3 nerve roots.16–17 In the literature, lateral, posterior, and anterior QLB approaches have been used for hip surgeries.18–21
In this study, the anterior QLB approach was chosen due to its anatomical proximity to the lumbar plexus and its potential for more effective analgesia in hip surgeries. The anterior QLB enables local anesthetic spread toward the L1–L3 nerve roots, which contribute to the innervation of the hip joint. Moreover, this region is richer in mechanoreceptors, and the anterior approach lies in a deeper fascial plane compared to lateral or posterior techniques. These characteristics may result in more consistent and effective postoperative analgesia, as supported by previous studies. 22
However, the evidence comparing the efficacy of these two blocks remains limited, and there is no clear consensus on which technique provides superior pain relief.
This study aimed to compare the postoperative analgesic efficacy of the PENG and anterior QLB blocks in patients undergoing hip fracture surgery. Total analgesic consumption, time to first rescue analgesic requirement, and NRS scores within the first 48 postoperative hours were evaluated. These findings may contribute to guiding clinical practice in optimizing pain management following hip surgery.
Material and methods
The study protocol was approved by the Clinical Research Ethics Committee of Gaziosmanpaşa Training and Research Hospital (Chairperson: Prof. E. Kimiloglu), Istanbul, Turkey, on June 7, 2023 (Approval No: 66). Detailed written and verbal information was provided to all patients, and written informed consent was obtained prior to participation. There was no patient or public involvement in the design, conduct, or reporting of this trial. The study was registered in the ClinicalTrials.gov database (Registration No: NCT06653894).
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki (1975), revised in 2024, and was designed as a prospective, randomized, single-blind trial. It took place in the orthopedic operating room of Gaziosmanpaşa Training and Research Hospital between October 25, 2024, and April 3, 2025. The reporting of this study conforms to the CONSORT guidelines. 23
Patients aged 40 years or older, classified as ASA I–III, who were scheduled to undergo surgery under spinal anesthesia for either intertrochanteric or femoral neck fractures were included in the study. Surgical procedures consisted of open reduction and internal fixation, intramedullary nailing, or hemiarthroplasty, depending on the type of fracture and the surgeon's preference. To minimize the potential effects of anemia, ensure more reliable results, and maintain group homogeneity, only patients with a preoperative hemoglobin level of 10 g/dL or higher were included.
Patients were excluded if they refused to participate; required general anesthesia or peripheral nerve blocks, such as a combination of femoral and parasacral sciatic nerve blocks for anesthesia; had a history of allergy to local anesthetics; sustained multiple trauma; had severe hearing or visual impairment; or presented with a local infection at the block application site. Additionally, patients with a clinical diagnosis of neurocognitive disorders, such as dementia or Alzheimer's disease, who were under active neurological follow-up, were excluded. Other exclusion criteria included a body mass index (BMI) greater than 35 kg/m² and a history of severe neurological, cardiovascular, renal, or hepatic disease. Patients requiring intensive care unit (ICU) admission for more than one day due to the need for close hemodynamic monitoring or sedation were also excluded. Furthermore, patients who developed postoperative complications requiring intervention—such as reoperation, postoperative hemorrhage, or the need for advanced cardiovascular or respiratory support—were not included in the study.
Randomization was performed postoperatively—immediately after the surgical procedure and prior to block application—to prevent bias from intraoperative factors. The randomization sequence for the two groups was generated using SPSS version 25.0 with a simple randomization method. An independent researcher, who was not involved in patient recruitment or data collection, prepared the sequence. Group assignments were concealed in sequentially numbered, opaque, sealed envelopes. Upon enrollment, each patient was assigned to a group by opening the next envelope in sequence. Patients who received the aQLB were assigned to the aQLB group, while those who received the PENG block were assigned to the PENG.
All patients received standard monitoring (i.e. electrocardiography, non-invasive blood pressure measurement, and pulse oximetry) and a standard anesthesia technique. Spinal anesthesia was administered in the L3–L4 or L4–L5 interspace using a 25G Spinocan needle (Braun, Melsungen AG, Melsungen, Germany) with intrathecal 12 mg bupivacaine.
Intraoperatively, all patients received tranexamic acid at a dose of 10 mg/kg via slow intravenous infusion following the administration of spinal anesthesia. Additionally, 8 mg of intravenous dexamethasone was administered to all patients, and at the end of the surgery, tramadol hydrochloride at a dose of 1 mg/kg was given intravenously.
At the end of the surgical procedure, all patients were transferred to the block room. After standard monitoring, patients scheduled to receive the anterior QLB were placed in the lateral decubitus position with the surgical side facing up. Following aseptic preparation, a convex ultrasound probe (2–6 MHz) (MyLabseven; Esaote Europe, The Netherlands) was positioned in the subcostal area above the iliac crest. The quadratus lumborum and psoas major muscles, along with the transverse process of the L4 vertebra, were visualized in the midaxillary line using an in-plane technique. A 22G, 100-mm peripheral block needle (Stimuplex® Ultra; B. Braun Melsungen AG, Melsungen, Germany) was advanced into the subfascial plane between the quadratus lumborum and psoas major muscles, and 1–2 mL of 0.9% saline was injected to confirm correct placement via hydrodissection. Following this, 20 mL of 0.25% bupivacaine was injected incrementally, with aspiration performed every 5 mL. Proper spread of the local anesthetic was confirmed by ultrasound visualization of a hypoechoic distribution between the fascial planes.
In the PENG, patients were placed in the supine position. A convex ultrasound probe was positioned under sterile conditions on the operated side, aligned with the iliac bone below the anterior superior iliac spine (ASIS). The anterior inferior iliac spine (AIIS), iliopubic eminence (IPE), iliopsoas muscle, and its tendon were identified. Using an in-plane technique, a 22G 100-mm peripheral block needle was advanced toward the IPE, targeting the space between the iliopsoas muscle tendon and the IPE. Proper placement was confirmed via hydrodissection. Subsequently, 20 mL of 0.25% bupivacaine was administered slowly, with aspiration performed every 5 mL to avoid intravascular injection. The correct spread of the local anesthetic was verified via ultrasound, confirming elevation of the iliopsoas tendon.
All blocks were performed by the same experienced anesthesiologist, who did not participate in the postoperative follow-up of the patients. After the block procedure, all patients were monitored in the block room for 30 minutes. ASA I and II patients were then transferred to the ward, while ASA III patients were observed in the ICU for one day for close hemodynamic monitoring before being transferred to the ward.
The patients received intravenous paracetamol at a dose of 1 g four times daily, starting from the first postoperative hour. Additionally, diclofenac 75 mg was administered twice daily. At the postoperative follow-up, patients with an NRS score ≥ 4 were administered intravenous tramadol hydrochloride 1 mg/kg as rescue analgesia in the ward or ICU.
Patients were evaluated at 2, 12, 24, and 48 hours postoperatively by a different anesthesiologist who was blinded to the block procedure. Analgesic consumption, resting and dynamic (during coughing) Numeric Rating Scale (NRS) scores (rated from 0 to 10; 0: no pain, 10: worst pain imaginable), time to first rescue analgesia, and postoperative side effects (quadriceps weakness, nausea, and vomiting) were recorded. Postoperative quadriceps function was assessed at the 4th hour using a straight leg raise test in the supine position. The ability to actively extend the knee against gravity was considered indicative of preserved motor function.
The primary aim of this study was to compare the effect of an anterior QLB and PENG block on total opioid analgesic (tramadol) consumption within the first 48 hours postoperatively. The secondary aims were to compare the resting and dynamic NRS scores at 2, 12, 24 and 48 hours postoperatively, the time to first rescue analgesia, and side effects such as nausea, vomiting and quadriceps weakness.
Based on preliminary data (48-hour tramadol consumption: 113.0 ± 71.83 mg in the PENG and 160.3 ± 58.60 mg in the QLB group), a power analysis was conducted using G*Power (version 3.1, Brunsbüttel, Germany). 24 With an alpha level of 0.05, a power of 0.80, and an effect size of 0.72, the minimum required sample size was calculated to be 30 patients per group. However, during the pilot phase, we observed a high rate of patient exclusion due to advanced age, comorbidities, prolonged ICU stays, and postoperative sedation. To reduce the risk of data loss due to such protocol deviations and to enhance the statistical power of the final analysis, we planned to enroll 45 patients per group.
Statistical analyses were performed using IBM SPSS Statistics, version 26.0 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as frequencies and percentages, while numerical variables were summarized using descriptive statistics, including mean, standard deviation, median, minimum, and maximum values. The distribution of numerical variables was assessed using the Kolmogorov–Smirnov test. Variables such as total tramadol consumption and time to first rescue analgesia did not show a normal distribution, as their standard deviations were close to or exceeded their means. Accordingly, non-parametric tests (e.g. the Mann–Whitney U test) were applied for these comparisons. Normally distributed data were analyzed using the independent samples t-test. For repeated measures of pain scores (NRS) over time, the Friedman test was used. Relationships between categorical variables were assessed using the Chi-squared test, and Fisher's exact test was applied when the expected frequency in any cell was less than 5. A p-value of < 0.05 was considered statistically significant.
Results
In this study, 113 patients were initially scheduled for elective hip fracture surgery. A total of 23 patients were excluded: four due to an ASA classification of IV, five because they were unsuitable for spinal anesthesia, seven due to cognitive impairment (e.g. dementia or Alzheimer's disease), three due to a BMI > 35 kg/m², and four who declined to participate.
Consequently, 90 patients were enrolled in the study. Of these, 17 patients were excluded due to prolonged stays in the ICU, the need for sedation, postoperative hemorrhage, or non-adherence to the postoperative analgesic regimen during follow-up. In addition, the block could not be administered in 5 patients due to significant pain during lateral positioning. Ultimately, 73 patients were included in the final analysis, with 30 in the aQLB group and 43 in the PENG (Figure 1).
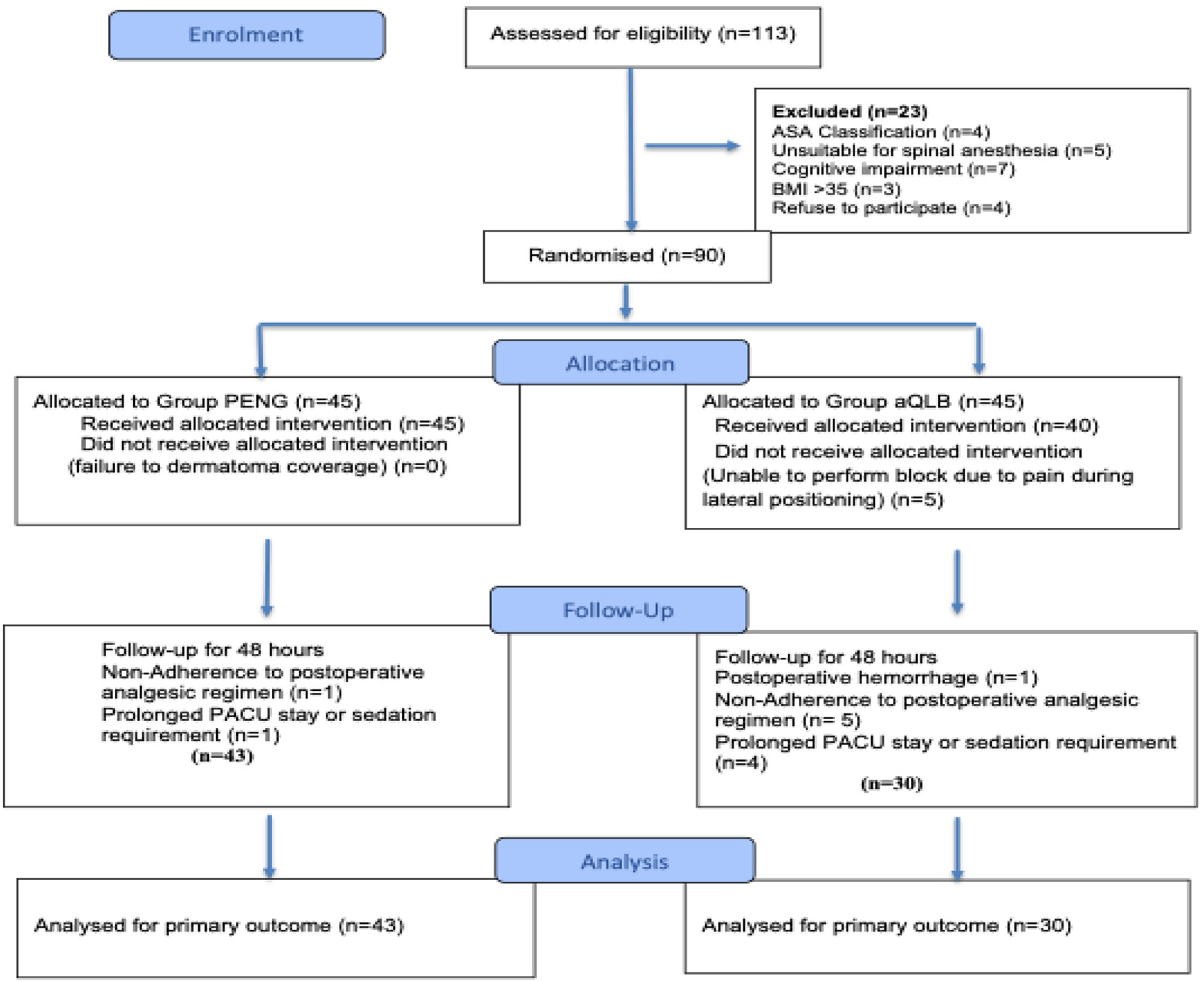
Flow diagram of the study (CONSORT diagram).
The two groups were demographically comparable (Table 1). The distribution of ASA classifications was also similar between the groups. Patients had chronic comorbidities such as hypertension, coronary artery disease, heart failure, chronic obstructive pulmonary disease, diabetes mellitus, hypothyroidism, and atrial fibrillation. There was no significant difference between the groups in terms of fracture types (intertrochanteric vs. femoral neck fractures).
Demographic and anesthetic characteristics of the groups.

Values are presented as mean ± SD. Group aQLB: anterior quadratus lumborum block group; Group PENG: pericapsular nerve group block group. BMI: body mass index; SD: standard deviation. Statistical tests: independent samples t-test, Mann–Whitney U test, Chi-squared test. p < 0.05.
Postoperative tramadol use within the first 48 hours was significantly lower in the PENG compared to the aQLB group (p = 0.004). Notably, nine patients (20.9%) in the PENG and four patients (13.3%) in the aQLB group did not require any tramadol (Table 2).
Evaluation of tramadol HCl usage between groups in the postoperative first 48 hours.

Values are presented as mean ± SD for continuous variables and as number and percentage (n, %) for categorical variables. Group aQLB: anterior quadratus lumborum block group; Group PENG: pericapsular nerve group block group. SD: standard deviation; CI: confidence interval. Statistical tests: Mann–Whitney U test, Chi-squared test *: p < 0.05.
The time to first rescue analgesia was significantly longer in the PENG (9.03 ± 7.67 hours) than in the aQLB group (6.81 ± 6.70 hours) (p = 0.048) (Table 2).
rNRS scores remained low (< 4) at all time points in both groups. There were no statistically significant differences in resting or dynamic NRS scores between the PENG and aQLB groups at any postoperative time point (Table 3). At the 2nd postoperative hour, the Cohen's d for rNRS was 0.415 and for dNRS was 0.448, indicating small to moderate effect sizes. Effect sizes at other time points were lower, suggesting minimal group differences (Table 3) (Figure 2).

Time-dependent changes in mean NRS scores at rest (A) and during movement (B) in patients receiving PENG or aQLB blocks. Data points represent mean values at 2nd, 12th, 24th, and 48th postoperative hours.
Comparison of postoperative resting and dynamic NRS pain scores between PENG and aQLB groups during the first 48 hours.

Values are presented as mean ± SD and median (minimum–maximum). Group aQLB: anterior quadratus lumborum block group; Group PENG: pericapsular nerve group block group. rNRS: resting numeric rating scale; dNRS: dynamic numeric rating scale; SD: standard deviation; d: Cohen's d. *: Effect size indicating small clinical relevance despite nonsignificant p-value. Statistical tests: Mann–Whitney U test and Friedman Analysis (Fr). p < 0.05.
Quadriceps muscle weakness was not observed in any patient. In the QLB group, nausea occurred in only two patients.
Discussion
The findings of this study suggest that, in patients undergoing hip fracture surgery under spinal anesthesia, the PENG block provides superior postoperative analgesia compared to the anterior QLB block. Specifically, tramadol consumption was significantly lower, and the time to first rescue analgesia was significantly longer in the PENG during the first 48 postoperative hours.
In recent years, the use of fascial plane blocks for postoperative analgesia in hip surgeries has gained popularity.25–27 We believe that the findings of the present study may contribute to clinical practice by guiding the selection of optimal analgesic techniques for postoperative pain control in hip surgeries.
Studies comparing the PENG block with FICB and femoral nerve blocks have reported that the PENG block provides more effective and safer analgesia than both techniques. 27 It has also been associated with faster onset of analgesia, fewer complications, and higher patient satisfaction. Furthermore, unlike FICB and femoral nerve blocks, which often result in motor blockade, the PENG block has a motor-sparing effect and does not cause quadriceps weakness.28,29
In this study, 43 patients were analyzed in the PENG, whereas a relatively smaller number of 30 patients were included in the aQLB group. This imbalance was primarily due to a higher number of patients in the aQLB group being excluded during the postoperative period. Patients who required ICU monitoring for more than 24 hours were excluded from the analysis. These patients were typically classified as ASA III and had multiple chronic comorbidities, such as cardiovascular, pulmonary, or metabolic conditions, which necessitated prolonged ICU care due to their clinical status rather than the study intervention. Additionally, patients who required postoperative sedation (e.g. with midazolam or dexmedetomidine) or received blood transfusions due to postoperative hemorrhage were also excluded. These patients were expected to have variable analgesic requirements due to clinical instability. Including such patients in the analysis could have compromised the generalizability and reliability of the study findings; therefore, a per-protocol analysis was preferred.
Additionally, in five patients, the anterior QLB block could not be performed due to significant pain during positioning in the lateral decubitus position. The procedure was aborted in these cases out of concern that further manipulation might aggravate pain at the fracture site or compromise surgical stability. While the PENG block has the advantage of being performed in the supine position, the QLB requires lateral positioning, which can present challenges in geriatric patients with recent hip fractures. To minimize such risks, all blocks were performed with careful support and positioning techniques, including the placement of a pillow between the legs.
Although preoperative administration of blocks may offer advantages for patient positioning, in this study, blocks were intentionally performed in the postoperative period. This decision was based on several factors: hip surgeries typically last around two hours, and peripheral nerve blocks are ideally administered approximately 30 minutes before the procedure. However, during this same period, activities such as surgical field preparation, equipment checks, and spinal anesthesia administration are carried out. Therefore, performing the blocks preoperatively would have resulted in a significant portion of their analgesic effect coinciding with the intraoperative period. To enhance postoperative patient comfort, reduce opioid consumption, and minimize opioid-related side effects through effective analgesia, the blocks were applied after surgery.
In the management of postoperative analgesia, paracetamol was administered due to its favorable safety profile. Additionally, diclofenac was given twice daily for its anti-inflammatory properties as part of the multimodal analgesic regimen. If the resting NRS score resulted ≥ 4, we administered tramadol, which is a mild opioid analgesic with strong and reliable analgesic efficacy, as recommended in stepwise therapy.
This study demonstrated low NRS scores in both groups, with no statistically significant differences at any time point, indicating that postoperative pain management was effective overall.
Although the differences in rNRS and dNRS scores between groups did not reach statistical significance at any time points (p > 0.05), the effect sizes (Cohen's d) at 2nd postoperative hour were indicative of small clinical effects in favor of PENG block. This suggests that the PENG block may offer slightly better early pain control, despite lack of statistical significance.
Postoperative 2nd-hour NRS pain assessments were conducted two hours after the patients were discharged from the operating room. Considering that the average duration of surgery was approximately 2 hours, this corresponds to approximately 5 to 5.5 hours after spinal anesthesia. We believe that this timing accurately reflects pain levels in the early postoperative period following block administration.
Since tramadol was administered when the NRS score was ≥4, the similarity in pain scores between the groups can be attributed to the standardized rescue analgesia protocol. Although the proportion of patients receiving tramadol was similar in both groups, the mean cumulative tramadol consumption was higher in the aQLB group. This discrepancy likely resulted from multiple tramadol doses being required by some patients in the aQLB group during the 48-hour follow-up period. In contrast, patients in the PENG more frequently achieved adequate analgesia with a single dose. This finding highlights that while NRS scores were comparable, the analgesic requirements over time—reflected by total tramadol consumption—may differ between block types, suggesting variations in the duration or depth of analgesic effect.
Total tramadol consumption was 50% lower in patients who received the PENG block compared to those who received the aQLB block.
An additional finding in this study was that the standard deviation of tramadol consumption in the aQLB group was higher than both that of the PENG and the variability anticipated in the power analysis. This may reflect inter-individual differences in response to the aQLB block, potentially due to factors such as the distribution and duration of action of the local anesthetic. Although the block technique was performed in a standardized manner, anatomical variations and individual differences in tissue elasticity may have influenced the block's effectiveness. These variations could have affected the total analgesic consumption and suggest that the consistency of block efficacy may differ between the two techniques. The inherent unpredictability of fascial plane blocks—particularly in terms of local anesthetic spread and anatomical variability—may further explain the wider standard deviation observed in the QLB group. 30
Previous studies comparing PENG and anterior QLB blocks have shown inconsistent results. While many support the superior analgesic efficacy and motor-sparing properties of the PENG block, the evidence regarding which technique provides more effective analgesia in hip surgeries remains limited and inconclusive.21,27,31 Our findings are consistent with previous studies reporting the effectiveness of the PENG block in postoperative analgesia.18,28,31,32 Furthermore, the time to first rescue analgesia was longer in the PENG, supporting its superior analgesic effect and potential utility in acute pain management.
In another study evaluating postoperative analgesia with PENG and QLB blocks, quadriceps paresis was reported in 20% to 25% of patients by the 12th postoperative hour. 28 This was attributed to the use of higher volumes and concentrations of local anesthetics. In contrast, no such motor weakness was observed in our study. We believe this may be due to the use of 20 mL of 0.25% bupivacaine, which is thought to play a key role in preserving motor function. Although this volume may have contributed to the preservation of motor function, the analgesic efficacy achieved with anterior QLB might have been limited, particularly in the context of hip surgeries. Considering that quadratus lumborum blocks are fascial plane blocks, it is evident that higher volumes may result in more effective analgesia.
Additionally, nausea was observed in only two patients in the QLB group. We believe this may be attributable to both our multimodal analgesic regimen and the intraoperative use of dexamethasone. No other adverse events were observed in the present study. Upon reviewing the literature, a case series was identified in which three patients with hip fractures experienced blood aspiration through the catheter following PENG catheter placement for analgesia. 33 The authors reported that they had ruled out the presence of vascular structures in the area using Doppler ultrasound. They suggested that the source of blood could have been due to the spread of intra-articular bleeding into the iliopsoas bursa following the hip fracture, or secondary to a hematoma within the iliopsoas muscle caused by trauma. In our study, no blood aspiration was encountered during local anesthetic injection following hydrodissection. In both block procedures, we ensured that local anesthetic was administered only after confirming adequate hydrodissection. We believe that the use of an in-plane technique, along with continuous real-time visualization of both the needle advancement and the injection of the local anesthetic, plays a critical role in minimizing the risk of such complications.
In this study, the absence of rescue analgesic requirements in some patients and the relatively low average total analgesic consumption over 48 hours not only suggest the effectiveness of these blocks in providing postoperative analgesia, but may also be influenced by the advanced age of the study population. In elderly individuals, postoperative or acute pain management differs from that in younger patients due to altered pain perception, changes in pharmacokinetics, and increased sensitivity to opioids. These factors may contribute to lower analgesic requirements and prolonged drug effects resulting from reduced metabolic clearance. 34
In the PENG block, cutaneous sensory blockade is not expected, as sensory coverage is limited to the anterior capsule of the hip joint. In contrast, QLB blocks may provide sensory coverage of the T10–L3 dermatomes, potentially offering some benefit in managing incisional pain. However, based on our findings, postoperative pain following hip surgery appears to originate more from the joint capsule than from the incision site.
One of the major limitations of this study is the unequal number of patients between the groups, which may have affected the statistical power and the external validity of the findings. This imbalance was primarily due to technical difficulties encountered during the aQLB procedure and patient losses in the postoperative period. A per-protocol analysis was preferred, as including patients lost to follow-up could have compromised the internal validity and interpretability of the results. Although an intention-to-treat approach could enhance generalizability, the per-protocol method was considered more appropriate for evaluating the analgesic efficacy of the interventions under standardized conditions. However, this approach may limit the generalizability of the findings and should be taken into account when interpreting the results.
One of the limitations regarding blinding is the possibility that some patients might have inferred the type of block they received due to differences in positioning (i.e. supine for PENG vs. lateral for QLB). However, since the blocks were performed in the postoperative period while the sedative effect was still present, and patients were assessed only for their analgesic status without being asked about the type of block administered, blinding was largely preserved. In addition, the types of surgical procedures were not analyzed separately; comparing surgical approaches could have provided additional insight into analgesic outcomes. Another notable limitation is that dermatomal sensory assessments could not be performed in the aQLB group due to the residual effects of spinal anesthesia in the early postoperative period. An additional concern is the lack of evaluation for chronic postoperative pain, which could have offered important insights into the long-term efficacy of the blocks in preventing chronic pain. A further limitation is the high degree of inter-individual variability in tramadol consumption observed in the aQLB group. This may reflect variable responses to the block and could limit the generalizability of the analgesic outcomes. Finally, the lack of comparison with higher volumes represents another limitation, as it restricts the ability to fully assess the potential efficacy of the technique.
Conclusion
This study demonstrated that the PENG block may offer more effective postoperative analgesia compared to the anterior QLB block in patients undergoing hip fracture surgery under spinal anesthesia. The PENG block was associated with lower opioid consumption and a longer time to first rescue analgesia, suggesting better pain control in the early postoperative period. Given its motor-sparing nature and technical feasibility in the supine position, the PENG block appears to be a valuable component of multimodal analgesia protocols in elderly patients.
Footnotes
Acknowledgments
Th authors would like to thank Omer Kaplan for his contributions to the statistical evaluation of this study.
Authors’ contributions
Data collection, data analysis, writing, revising, study design, and patient recruitment were done by SŞ, DGM. All authors contributed equally to this work.
All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available but are accessible from the corresponding author upon reasonable request.