
Abstract
Objective
This study investigated whether endobiliary radiofrequency ablation (eRFA) performed before stent placement benefited the patency of self-expandable metal stents placed in patients with unresectable malignant biliary obstruction.
Methods
The study included 94 patients with biliary malignancies who underwent percutaneous biliary stent placement. The mean age of the patients was 66.9 ± 10.7 years, with 60 males (63.8%). Forty-five patients (47.9%) underwent eRFA (ELRATM, STARmed, Republic of Korea) before stenting. The patients’ age, gender, type of cancer, laboratory values (alanine aminotransferase [ALT], aspartate aminotransferase [AST], and gamma-glutamyl transferase [GGT]), Bismuth-Corlette classification of tumors, and stent patency were retrospectively analyzed. The study's primary objective was to evaluate the impact of pre-stenting ELRA therapy on stent patency. Secondary objectives included comparing changes in post-procedural biochemical parameters, complication rates, and other parameters between the ELRA and non-ELRA groups.
Results
The median follow-up was 17 months. Technical success was 100% in both groups, with no procedure-related major complications or mortality. Minor complications included fever and mild abdominal pain, with no significant difference between the groups. Post-procedure total bilirubin, ALT, AST, and GGT levels significantly decreased compared to pre-procedure values in the ELRA group. In contrast, no significant difference was observed in the non-ELRA group. The median duration of primary patency was 6 months for all patients, significantly longer in the ELRA group compared to the non-ELRA group (8 vs. 6 months, p < 0.001).
Conclusion
eRFA performed using the ELRA catheter before biliary stenting is a technically successful, minimally invasive, and safe procedure that can potentially increase the duration of stent patency.
Introduction
Malignant biliary obstruction (MBO) occurs due to tumors affecting the bile ducts (biliary) or due to the local extension of tumors into adjacent structures or compression by lymph nodes (extra biliary).1,2 The most common causes of MBO are cholangiocarcinoma (CCA) and pancreatic cancer, with other causes including gallbladder cancer, ampullary cancer, and metastases. 3 Surgical resection is the standard curative treatment; however, most patients are in advanced stages and unresectable at diagnosis. The efficacy of conventional radiotherapy or chemotherapy is limited. MBO can lead to jaundice, coagulopathy, impaired immunity, opportunistic infections, and hepatic failure. 4 Metallic or plastic biliary stents placed percutaneously or endoscopically are the most commonly used palliative treatments in clinical practice. Patients with palliative stent placement typically have an expected survival of 6–9 months. 5 The primary issue with biliary stents is the development of occlusion due to biliary sludge, stent migration, or tumoral ingrowth. Self-expandable metal stents (SEMSs) offer a favorable treatment option with wider luminal diameters and increased patency rates. 1 Although SEMS have better patency rates than plastic stents, their initial occlusion rates remain high, with median patency typically around 6–9 months.4,6,7 The classic treatment for stent occlusion involves replacing a plastic or metal stent. 4 In recent years, advancements in anticancer therapies have increased the life expectancy of patients with MBO, leading to higher rates of stent occlusion. Consequently, new treatments have been developed to improve stent patency rates. 1 The endobiliary radiofrequency ablation (eRFA) treatment, implemented in 2011 for this purpose, aims to enhance stent patency and, thus, improve patient survival.
eRFA aims to create local necrosis in tumor tissue using thermal energy. Ablation results in histological coagulation necrosis, protein denaturation, and cellular desiccation. Death of superficial epithelial cells in the stenosis area slows down tumoral and epithelial overgrowth and prolongs the patency of the stent. 8 It is typically performed percutaneously or via endoscopic retrograde cholangiopancreatography (ERCP) immediately before or after stenting. The active tip of the catheter is placed at the stricture site, where one or multiple consecutive ablations are performed depending on the length of the stricture. The Habib™ Endo HPB (Boston Scientific, USA) and ELRA™ (Starmed, Republic of Korea) are the two most commonly used catheters for ablation. 9 By primarily causing localized damage to tumor tissue, ablation aims to prolong stent patency. Therefore, it is expected to be more effective in patients with intra-biliary MBO (e.g. extrahepatic CCA and ampullary cancer). 10
Furthermore, due to its potential to reduce tumor burden and alter tumor immunity, eRFA is anticipated to benefit survival. 5 This study aimed to demonstrate the impact of eRFA performed before SEMS placement on stent patency in patients primarily undergoing SEMS for MBO. Secondary objectives included investigating the clinical success and safety of the procedure based on clinical and laboratory findings during patient follow-up. In addition, as existing literature primarily relies on power-controlled catheters used via ERCP, using percutaneous eRFA with a temperature-controlled catheter, such as ELRA, will significantly contribute to scientific knowledge on ablation outcomes.
Methods
Study population and design
The reporting of this study conforms to STROBE guidelines. 11 Data from 94 patients who underwent biliary stent placement due to biliary malignancy between April 2020 and November 2023 were retrospectively reviewed. Ethical approval for the study was obtained from the Non-Interventional Ethics Committee of the Sakarya University Faculty of Medicine (date and number: 26.03.2024-E.349247). The inclusion criteria were patients with histopathologically proven MBO and ECOG grade 0-1. The exclusion criteria were patients who received liver-directed intra-arterial therapy (transarterial chemoembolization, transarterial radioembolization, or hepatic artery infusion pump chemotherapy) or ECOG grade 2 and above. Patient demographics, type of cancer, preoperative (24 h before) and postoperative (6 h after) laboratory values (total bilirubin, alanine aminotransferase [ALT], aspartate aminotransferase [AST], and gamma-glutamyl transferase [GGT]), Bismuth-Corlette classification of tumors, and stent patency during follow-up were examined.
The mean age of the patients was 66.9 ± 10.7 years, with 60 males (63.8%) and 34 females (36.2%). Biliary pathologies included 53 cases of CCA (56.4%) and 41 cases of pancreatic adenocarcinoma (43.6%).
Equipment and technique
An interventional radiologist performed all procedures with 10 years of experience in biliary interventions. All procedures adhered to standard sterile conditions. An anesthesiologist administered sedation during the procedure. All patients received prophylactic antibiotics 2 hours before the procedure. Under ultrasound and fluoroscopy guidance, a micro-biliary access set (AccuStick, Boston Medical, Ireland) was used to access the peripheral bile duct, and a vascular sheath (Flexor, Cook Medical, Ireland) was placed. A contrast agent was administered, and then imaging was performed. After identifying the obstruction site, a 0.035-inch standard hydrophilic wire (Zipwire, Boston Medical, Ireland) and a 4F vertebral catheter (Glidecath, Terumo, Japan) were used to cross the site. In the non-ELRA group, balloon dilatation was performed using a 10-mm-diameter balloon (Mustang, Boston Scientific, USA), followed by the placement of a 10-mm-diameter uncovered SEMS (Wallstent, Boston Scientific, USA). In ELRA-treated patients, an 18-mm ELRA probe (STARmed Co., Goyang, Korea) was advanced over the wire to the obstruction site before balloon and stent placement. The energy was delivered using a radiofrequency generator (VIVA Combo™, STARmed Co., Goyang, Korea) with controlled energy transmission and maintained at a target temperature of 80 °C. Ablation was performed for 2 min with 10 watts of energy for each 18-mm segment (Figure 1). Cholangiography was obtained immediately after the ablation to exclude complications such as perforation. Subsequently, balloon dilation and stenting were performed similarly to the non-ELRA group. In all patients, a single biliary stent was placed using a transpapillary approach, meaning that the papilla was stented regardless of the tumor's location.

(A–D) Fluoroscopy images of a 57-year-old male patient with Bismuth-Corlette type 2 cholangiocellular carcinoma who underwent percutaneous transhepatic cholangiography, revealing an obstructed segment (A, arrow). ELRA was first applied to the relevant segment (B, arrow), followed by ballooning (C) and metallic stenting (D).
Definitions
Technical success was defined as the successful placement of the biliary stent in all patients and the completion of ablation in the ELRA group. Stent occlusion was defined as clinical and laboratory evidence consistent with cholestasis or cholangitis during the follow-up period and/or dilation of intrahepatic bile ducts on follow-up imaging. Stent patency was defined as the time from stent placement to occlusion. Complications were classified as minor or major according to the Society of Interventional Radiology reporting standards. 12 Minor complications required observation without treatment or hospitalization, while major complications necessitated prolonged hospitalization, an unplanned increase in patient care level, or resulted in sequelae or death. 12
End points
The study's primary objective was to evaluate the impact of pre-stenting ELRA therapy on stent patency. Secondary objectives included comparing changes in post-procedural biochemical parameters, complication rates, and other parameters between the ELRA and non-ELRA groups. Subgroup analyses were conducted to investigate factors affecting stent patency.
Statistical analysis
MedCalc (version 12, Ostend, Belgium) was used for statistical analyses. Descriptive statistics were presented as median (minimum-maximum) and mean ± standard deviation values. Categorical variables were expressed as frequencies and percentages. Fisher, Pearson's chi-squared, and Yates’ corrected version of Pearson's chi-squared tests were used to compare categorical variables. The independent-sample t-test was used for the comparison of continuous variables with a normal distribution, and the Mann–Whitney U test was for the data that did not conform to the normal distribution according to the Kolmogorov–Smirnov test. The Kaplan–Meier analysis was used to evaluate primary patency. A p-value of <0.05 was accepted as statistically significant.
Results
The median follow-up period was 17 (range, 11–33) months. Forty-five patients (47.9%) received pre-stenting eRFA (ELRA group), while 49 (52.1%) were managed with stenting alone (non-ELRA group). No significant differences were detected between the ELRA and non-ELRA groups in terms of age, gender, type of cancer, or Bismuth-Corlette classification (Table 1).
Comparison of basic characteristics between the patient groups.
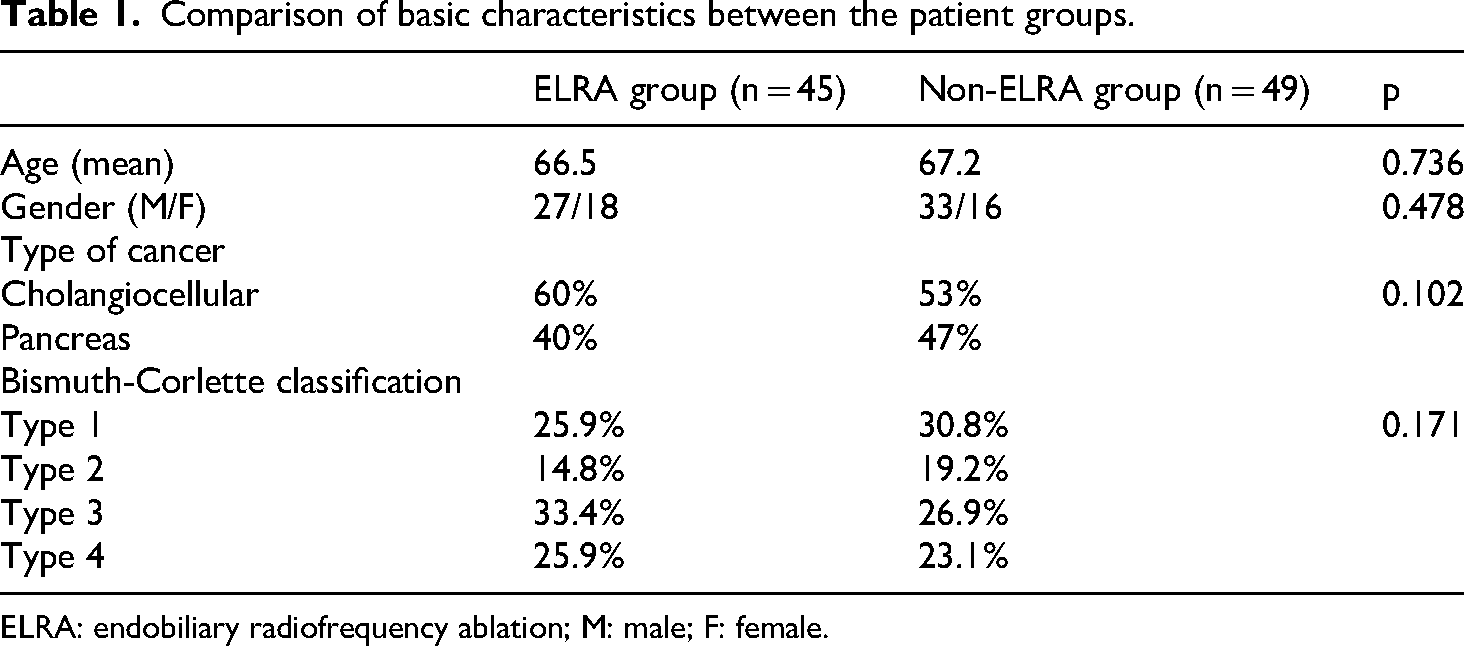
ELRA: endobiliary radiofrequency ablation; M: male; F: female.
Technical success was 100% in both groups, with no procedure-related major complications or mortality. Minor complications included fever (seven patients in the ELRA group vs. 10 in the non-ELRA group) and mild abdominal pain (11 patients in the ELRA group vs. 14 in the non-ELRA group), with no significant difference between the groups (p > 0.005).
In the statistical analysis of biochemical markers, there was a significant decrease in post-procedure total bilirubin, ALT, AST, and GGT values in the ELRA group (Table 2). However, in the non-ELRA group, no significant difference was detected between the total bilirubin, ALT, AST, and GGT values measured before and after the procedure (Table 3).
Pre- and post-procedure biochemical results of the ELRA group.

ELRA: endobiliary radiofrequency ablation; ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma-glutamyl transferase.
Pre- and post-procedure biochemical evaluation of the non-ELRA group.

ELRA: endobiliary radiofrequency ablation; ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma-glutamyl transferase.
In the subgroup analysis, no relationship was found between stent patency time and age (p = 0.875), gender (p = 0.590), Bismuth-Corlette classification (p = 0.214), or etiology (p = 0.614) in the ELRA group.
In the Kaplan–Meier analysis, the median duration of primary patency was 6 (95% confidence interval [CI]: 5–7) months for all patients, significantly longer in the ELRA group (8 months, 95% CI: 7–9 months) compared to the non-ELRA group (6 months, 95% CI: 3–5 months) (p < 0.001) (Figure 2).

Kaplan–Meier analysis comparing stent patency between the ELRA and non-ELRA groups (p < 0.001).
Discussion
RFA is increasingly essential in treating liver and pancreas pathologies with imaging guidance (ultrasound, computed tomography, digital subtraction angiography, endoscopic ultrasound). 13 This study demonstrated that percutaneous eRFA performed with ELRA, a temperature-controlled probe before biliary stenting, increased stent patency. A significant aspect distinguishing our study is its inclusion of the largest series in the literature investigating the efficacy of percutaneous ELRA in metallic stent patency (Table 4). Moreover, no significant difference in complications between the ELRA and non-ELRA groups indicates the procedure's safety.
Comparison of the current study with similar studies in the literature.

SEMS: self-expandable metal stent.
Effect of endobiliary radiofrequency ablation on stent patency and survival
The mechanism by which eRFA affects biliary stent patency is unclear. Mechanisms such as slowing down epithelial overgrowth with superficial cell death, triggering an immune response against tumor cells, and causing an increase in tumor lysis activity via CD8 + cells have been suggested.21–23 The effect of ablation on biliary stent patency and patient survival has been of recent interest, with numerous studies, systematic reviews, and meta-analyses comparing outcomes between patients treated with eRFA + stent versus stent alone. In these systematic reviews, randomized controlled trials (RCTs), retrospective studies (RS), and cross-sectional studies (CSS) were included. A meta-analysis published by Hayat et al. in 2024 (comprising 1339 patients and 13 studies, including five RCTs, seven RS, and one CSS) demonstrated that stent patency and overall survival were higher in the group that received eRFA. The pooled weighted mean difference between the two groups was reported to be 43.5 days for stent patency and 90.5 days for survival. According to that meta-analysis, eRFA was performed via ERCP in 10 studies and percutaneously in only three studies. No difference in complications was observed between the two groups. Additionally, the study suggested that immunological activation triggered by ablation might have contributed positively to both patency and survival, based on the effects of RFA observed in animal experiments. 24 A recent meta-analysis by de Oliveira Veras et al. (439 patients; six RCTs) also indicated that eRFA improved overall survival but increased stent patency only in tumors located in the hilum and CCA. This was attributed to the primary biliary tumors, originating from the biliary epithelium, responding more favorably to ablation. The results of that meta-analysis revealed that eRFA was performed via ERCP in four studies, percutaneously in one study, and through a combination of ERCP and percutaneous methods in one study. No differences in adverse events were observed between the two groups. 1 Another meta-analysis by Khizar et al. (1815 patients; 15 studies including six RCTs and nine RS) concluded that eRFA increased both stent patency and overall survival in patients with MBO. The pooled mean difference between the two groups was reported to be 2.11 months for stent patency and 2.88 months for survival. Notably, the RCT conducted by Tomas et al. was the only study among those included that reported no difference in survival between the two groups. 9 It is important to note that all these meta-analyses included patients who received PS alongside metallic stents, and ablation was predominantly performed via ERCP. In our study, all patients received metallic stents, and both stenting and eRFA were performed percutaneously. The group that received eRFA exhibited an average stent patency of 2 months longer than the group that received stenting alone. These results are consistent with the findings of the meta-analyses undertaken by Hayat et al., 24 Oliveira Veras et al., 1 and Khizar et al. 9
The technique employed in ablation (percutaneous or ERCP), the catheter chosen (Habib Endo HPB or ELRA), and the type of stent (PS or SEMS) has the potential to influence the outcomes of the procedure. The current study performed ablation procedures percutaneously using the ELRA eRFA catheter and SEMS stents. Despite the perceived safety of the percutaneous approach due to its minimally invasive nature and the elimination of ERCP-related risks, insufficient scientific data compares these two methods. The meta-analysis undertaken by Khizar et al. indicated shorter average survival with the percutaneous approach compared to the endoscopic method. 9 In Andrasina et al.'s (76 patients; RCT) study, all procedures utilized the percutaneous route with SEMS and the Habib Endo HPB catheter for eRFA. The authors concluded that eRFA increased stent patency only in the CCA group and did not benefit overall survival. All patients in that study received brachytherapy before the procedure. 21 In a study by Yu et al. (70 patients; RS), all procedures employed the percutaneous route with SEMS and the Habib Endo HPB catheter for eRFA, showing positive effects on stent patency and patient survival. 25 In a single-center study by Uyanık et al. (62 patients; RS), the percutaneous route with SEMS was employed, and the ELRA catheter was used for eRFA. 18 The authors demonstrated the positive effect of ELRA on stent patency compared to stenting alone (median patency of 223 days vs. 158 days). The temperature sensor of the ELRA catheter allows for temperature-controlled ablation, potentially reducing complication risks and increasing the effective ablation zone by mitigating the heat-sink effect.26,27 Several other studies have utilized the percutaneous approach and the ELRA catheter. For example, a prospective randomized phase II trial conducted by Kang et al. with 48 patients compared ELRA and non-ELRA groups, finding no difference in patency or survival. The study primarily used ERCP as the access route, with percutaneous procedures for patients unsuitable for ERCP. 19 An RS undertaken by Yildirim et al. with 18 patients found longer stent patency in the ELRA group (median patency of 128 vs. 86 days). 17 A recent study by Kim et al. compared ELRA and control groups in patients with type 4 hilar CCA, reporting longer stent patency in the ELRA group (median patency of 188 vs. 155 days) without differences in overall survival. 14 Our study is one of the few in the literature using ELRA for eRFA percutaneously, showing results consistent with the abovementioned studies.
Post-procedural follow-up
Follow-up is recommended to assess the clinical success of eRFA after the procedure. The literature shows varied follow-up intervals and diagnostic tests, including phone calls, planned visits, routine blood tests, liver function tests, and imaging (commonly abdominal ultrasonography and computed tomography; less frequently magnetic resonance imaging, magnetic resonance cholangiopancreatography, and endoscopic ultrasound). 10 All imaging examinations can be performed routinely or only in patients with ongoing/emerging clinical findings or those with elevated bilirubin levels. 18 If there are suspicious findings regarding biliary obstruction in these preliminary examinations, percutaneous or endoscopic intervention should be performed, and if necessary, repeat eRFA or stenting should be undertaken. 10 Yang et al. used intraductal ultrasound during ERCP to repeat eRFA if the bile duct wall thickness exceeded 6 mm at the previous lesion site. 28 Postoperative follow-up intervals varied across studies: first month, followed by every three months in the study of Gao et al.; every 3 months in those of Albers et al. and Xia et al.; first and third months, followed by every 3 months in that of Kim et al.; and every 2 weeks in that of Yang et al.28–30 In our RS, patient follow-up was carried out based on the clinical and laboratory findings and radiological images in the hospital records.
The role of bilirubin level in follow-up and clinical response assessment
The studies show that bilirubin levels are monitored during follow-up to evaluate stent patency. In the study of Özer et al., 25 patients who underwent eRFA and metallic stenting due to MBO were examined, and a significant decrease in total bilirubin values was observed in the patients after the procedure compared to before the procedure. A decrease of more than 50 percent in bilirubin values was defined as clinical success in the study. In addition, the authors stated that the bilirubin values before the procedure were significantly higher in their patients compared to publications in the literature and may have affected the study results. 16 Our study found no significant difference between the bilirubin values before and after the procedure. As in many other studies, bilirubin values were also evaluated to monitor stent patency. In our study, we examined laboratory parameters during the early postoperative period. We interpreted our findings to suggest that the biochemical response in patients who underwent e-RFA was faster than in the other group. This may have contributed to a significant decrease in these parameters in the ELRA group, unlike the other group.
Procedure-related adverse events
The incidence of procedure-related side effects and complications ranges from 4.2% to 35%. 10 The most common complication following eRFA is abdominal pain, occurring in approximately 21% of cases and typically resolving spontaneously within 1–5 days.10,31 The meta-analysis undertaken by Khizar et al. found no increase in the frequency of abdominal pain when comparing eRFA with stenting alone. 9 In our study, minor complications, namely abdominal pain and fever, were observed. Other common complications include pancreatitis, cholangitis, cholecystitis, ampullary stricture, and bleeding, which can be related to the ablation and the ERCP procedures. The effects observed in patients undergoing eRFA may be attributable to the ablation itself or to the ERCP procedure performed via the endoscopic route. Several meta-analyses addressing this issue have indicated that eRFA does not increase the risk of complications or side effects when added to conventional ERCP. 10 Cholangitis associated with the procedure is generally considered to arise from inadequate biliary drainage or stent occlusion caused by necrotic tissues. This condition is observed more frequently in hilar obstructions compared to distal regions. Following eRFA, the risks can be mitigated by stenting, external drainage, or using a balloon to remove necrotic tissues. 10 In a study by Kang et al., a patient who underwent eRFA died due to sepsis; however, the presence of bacteremia in blood cultures taken before ERCP suggested that the sepsis was not directly related to the procedure. 19 Pancreatitis risk is primarily associated with eRFA targeting the pancreatic or ampullary regions. Prophylactic stenting of the pancreatic duct is recommended for prevention. 10 It has been suggested that cholecystitis can result from cystic duct damage during eRFA of the hilar region. 29 Bleeding is frequent in the ampullary region due to incomplete ablation or tissue necrosis involving major tumor vessels. 9 Most reported bleeding complications in the literature have resolved with conservative treatment, although Tal et al. documented fatalities in two of three patients who developed hemobilia. 32 In addition to these complications, the thermal effects of eRFA can cause partial liver infarction, biliary tract perforation, liver abscess, and bile leakage, albeit rarely.33–36 These complications also generally respond to conservative treatment. 10 In the study by Zhou et al., biliary perforation occurred in two patients, resulting in one death due to peritonitis. 36 Avoiding overlap and normal biliary tract ablation is crucial to preventing such complications.
It has been suggested that using temperature-controlled catheters, such as ELRA, may further reduce the risk of complications. 18 In a study by Uyanık et al., percutaneous ELRA was used for ablation, and no significant differences in minor or major complications were found between the patients who underwent eRFA with metallic stent placement and those who underwent metallic stenting alone. 18 Similarly, Kim et al. concluded that using ELRA in conjunction with biliary stenting did not increase the risk of adverse events. 14 Our study also employed ELRA for eRFA, finding no differences in minor complications between the groups. However, more comprehensive research is needed in this area.
In-stent occlusion: role of endobiliary radiofrequency ablation
eRFA has also emerged as a therapeutic option in cases of metallic stent occlusion. 37 Nayar et al. were the first to employ a temperature-controlled catheter for this purpose (nine procedures; pilot study), reporting its safety. 8 Similarly, in a study by So et al. (11 patients; pilot study), eRFA using a temperature-controlled catheter in patients with CCA who presented with metallic stent occlusion achieved a technical success rate of 100% and a clinical success rate of 72.7%. 38 In a recent study by Inoue et al. (30 patients; pilot study), clinical success rates were similarly high, highlighting good long-term patency without stenting. The authors also noted a positive correlation between clinical success and the ratio of the recanalized diameter within the occluded stent to the stent diameter exceeding 51.1%. 34
Combination therapies and future perspectives
Endobiliary ablation therapy has recently been combined with other anti-tumor treatments. An RCT conducted by Yang et al. showed a positive effect of combination therapy (5-fluorouracil compound + eRFA) on overall survival and stent patency compared to eRFA alone. 28 In addition, two studies comparing combination therapy with chemotherapy alone found superior median survival and progression-free survival with combination therapy.34,39 The extent to which the use of various chemotherapy regimens or the incorporation of immunotherapies into combination treatments will alter therapeutic efficacy remains a subject for future investigation. In a study conducted by Andrasina et al., brachytherapy was administered to all patients with MBO, regardless of whether ERFA had also been applied prior to the procedure. 21 Given that all patients received brachytherapy, there was no control group, indicating a need for further studies to evaluate the combined outcomes of these two treatments.
Study limitations
Our study has certain limitations. Despite being the largest series in the literature investigating the effect of percutaneous ELRA on metallic stent patency, the number of patients was small. In addition, the retrospective design and single-center nature of the study were limiting factors. Another limitation of our study is that we did not present any data on overall survival. Future studies should consider multi-center, prospective designs with larger patient groups.
Conclusion
In conclusion, eRFA with ELRA represents a promising therapeutic option for improving stent patency in patients undergoing biliary stenting due to MBO. It has a high technical success rate and can be applied percutaneously in the same session as biliary stenting, making it minimally invasive. Our study supports the safety of the procedure, aligning with literature data.
Footnotes
Ethical considerations
Ethical approval for the study was obtained from the Non-Interventional Ethics Committee of the Sakarya University Faculty of Medicine (date and number: 26.03.2024-E.349247).
Author contributions
EA and OT contributed to the conception and design of the study. OFT, FYA, and OFS acquired the data. ABK and MC conducted literature searches. AS and ATE analyzed and interpreted the data. MHO and MO drafted and revised the article. Each author made a substantial contribution to the forthcoming work. The final version of the manuscript was reviewed and agreed to be submitted by all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and analyzed during the current study are available from the corresponding author upon reasonable request.
Informed consent
Informed consent is not required due to the retrospective nature of the study.