
Abstract
Objective
To analyze the safety and efficacy of manual removal and irrigation in cerumen removal in children.
Methods
A case-control study that prospectively collected the data of 6-month to 18-year-old children who underwent cerumen removal in the outpatient Department of Children's Hospital of Chongqing Medical University.
Results
A total of 347 ears were analyzed. The success rates of the manual removal and irrigation groups were 76.8% and 66.4%, respectively, with statistically significant differences. The rates of adverse reactions in both two groups were low and the differences between the two groups were not statistically significant. Meanwhile, differences in the proportion of cerumen obstruction less than 10%, discomfort and satisfaction after removal were statistically significant between the two groups. The manual removal group has a higher success rate for dry, flaky cerumen removal, whereas the irrigation group exhibits a higher success rate for dry, packed cerumen removal. While poor cooperation affects the success of both approaches, a heavy degree of cerumen obstruction affects the success of manual removal.
Conclusions
Manual removal is quicker and more convenient, whereas irrigation is cleaner and less discomfort. Selection based on ceruminous type achieves high success rate.
Introduction
Cerumen, also known as earwax, is composed of secretions from skin glands and exfoliated epithelial cells in the external auditory canal. It serves as a self-cleaning agent with protective and lubricating effects on the external auditory canal. 1 Generally, exfoliated cerumen can be expelled by jaw movement and epithelial cell migration operations. Most cerumen is asymptomatic and harmless. Cerumen accumulation in the ear canal is caused by reduced self-cleaning function or vigorous secretion. 2 Cerumen accumulation can cause symptoms such as hearing loss, ear swelling, itching and discomfort, balance disorders, tinnitus, and infection. 3 Cerumen removal is necessary for diagnostic purposes, including otoscopy and auditory or vestibular tests. Therefore, cerumen blockage should be diagnosed by clinicians when cerumen accumulation is associated with symptoms and/or prevents the necessary evaluation of the ear. 4 Cerumen blockage is particularly common in children and the elderly, with a prevalence of 10% in children.1,3,5
The most common methods for cerumen removal in clinical practice are cerumenolytic agents, irrigation, or manual removal. 6 Cerumenolytic agents are liquid solutions that can help dilute, soften, and dissolve cerumen. Considering the drug configuration, storage conditions, effectiveness, and price, hydrogen peroxide, and sodium bicarbonate are the most commonly used cerumenolytic agents in China. A previous meta-analysis showed that the solubility of a mixture of hydrogen peroxide and glycerol was significantly better than that of sodium bicarbonate and glycerol in children. 7 As hydrogen peroxide degrades on contact with the cerumen, numerous small bubbles are formed, then the cerumen gradually softens and separates from the wall of the external auditory canal. Moreover, as an oxidizing disinfectant, 8 hydrogen peroxide is used to treat cerumen obstruction and inflammation of the external ear canal and middle ear. As a result, hydrogen peroxide is the most widely used cerumenolytic agent in China. Ear irrigation refers to irrigation of the external auditory canal with normal saline. It can be performed using different syringes or electronic irrigation devices, with manual irrigation with syringes being the most common and inexpensive technique. 9 Given the poor cooperation among children, irrigation is safer and simpler than manual removal. However, this method is often accompanied by some discomfort such as feeling of fullness, vertigo, tinnitus and even ear infection, etc. and the operation time is longer. In addition, if cerumen is excessive, hard, or adheres too tightly to the skin, ear irrigation requires pretreatment with cerumenolytic agents. Manual removal is performed using a curette, probe, cerumen hook, forceps, or ear scoops and special cotton swabs under direct visualization with a headlight, otoscope, or microscope. This technique is quick and convenient, and the external auditory canal can be visualized directly, preventing exposure to moisture. However, it requires instrumentation and specially trained medical staff. Moreover, the risk of the external ear canal and tympanic membrane injury is higher than irrigation for uncooperative children.
These three methods of cerumen removal have their advantages and disadvantages, and a combination of 2–3 methods may be used in some cases. Combined methods are often applied to children owing to their poor cooperation. The choice of the method is often determined by the nature of the cerumen, the willingness of guardians, and the experience of the medical staff; however, there is no specific standard. So far, no treatment approach has proven to be superior to another. 4 It has been suggested that cerumenolytic agents and/or irrigation should be used in primary care hospitals and referrals should be made to the otolaryngology department in case of treatment failure. 10 Nonetheless, the choice of an optimal treatment method for children who present to the otolaryngology department for cerumen removal has not been elucidated. Currently, few studies have compared different cerumen removal methods in children.
Since pure 3% hydrogen peroxide is often used in China, most cases still require irrigation and/or manual removal after using cerumenolytic agents. Previous studies found that pretreatment with cerumenolytic agents before irrigation was more effective.11,12 Therefore, the outpatient Department of Otorhinolaryngology of Children's Hospital of Chongqing Medical University banned the use of cerumenolytic agents alone and irrigation without cerumenolytic agents. The treatment methods used were manual removal or irrigation after using cerumenolytic agents to improve the success rate of cerumen removal. The case-control study sought to assess the safety and efficacy of manual removal and irrigation in cerumen removal in children.
Materials and methods
Study population
The data of children who underwent cerumen removal in the outpatient Department of Otolaryngology of Children's Hospital of Chongqing Medical University between March 2024 and July 2024 were collected prospectively. Since children younger than 6 months sleep most of the day, assessment of cerumen-related symptoms is challenging. Besides, their guardians are more likely to reject cerumen removal because of the involved risks. As a result, only a few children under 6 months undergo cerumen removal. In addition, the guidelines from the American Academy of Otolaryngology-Head and Neck Surgery Foundation apply to children aged from 6 months to 18 years. 13 Therefore, the current study collected data from 6-month to 18-year-old children.
Inclusion criteria: (1) Aged 6 months to 18 years old. (2) Cerumen obstruction ≥ 25%. 14 (3) Before cerumen removal, the ear canal and eardrum do not exhibit abnormal changes, such as inflammation, trauma, structural deformities, etc. (4) Guardians agreed to participate in the study.
Exclusion criteria: (1) Acute and chronic ear inflammation, mastoiditis. (2) Injury of the tympanic membrane and ear canal, ear canal neoplasm, and moderate or severe stenosis of the ear canal. (3) Ear canal or middle ear surgery. (4) Blood scab, external auditory canal foreign body, applying ointment or ear drops in the ear canal. (5) Known or suspected allergic reaction to cerumenolytic agents or use of cerumenolytic agents within 1 week before the study. (6) Children with coagulopathy or those taking antiplatelet or anticoagulant drugs. (7) Children with mental retardation, autism, hyperactivity, and other disorders that may affect the degree of cooperation. (8) Children with failed cerumen removal at home or other hospitals.
Study methods
Test flow
All guardians read, fully understood, and signed the informed consent form before the study, which described the advantages and disadvantages of each removal method. The guardians voluntarily chose the manual removal or irrigation method. A combination of the two methods was applied in case manual removal or irrigation failed. The operation was stopped in case the combination treatment also failed. The guardians were instructed to use sodium bicarbonate ear drops until their return to the hospital after 3–5 days.
This study was conducted in accordance with the Helsinki Declaration of 2024. It was approved by the Ethics Committee of the Children's Hospital of Chongqing Medical University (Approval number: 2023: 564). The study is reported according to STROBE guidelines. 15
Removal methods
Cerumen removal should be performed by experienced nurses to ensure high success rate and reduce the risk of cerumen removal in children. Nurses with a work experience exceeding 6 months can perform ear irrigation, whereas those with work experience exceeding 5 years can perform manual removal.
Health education before the operation: the operation process and steps, the fixation of the child's position, possible adverse events (such as pain, injury, etc.), and the corresponding treatment measures and precautions were explained to guardians and children.
Position: The child was seated laterally with the head supported against the chair back and the affected ear oriented toward the clinician. For younger or uncooperative patients, a two-person technique was employed: one clinician and the guardian secured the child's torso and limbs using a pediatric restraint sheet, while a second assistant (either another guardian or nurse) maintained cephalic stabilization through manual head fixation.
Methods: For manual removal, the nurses wore a headlamp for cerumen removal using metal instruments (cerumen hook, forceps, or ear scoops) or cotton swabs. Before irrigation, the child's head was tilted to one side and the nurse gently pulled on the auricle and dripped hydrogen peroxide into the ear canal until it was filled. After 20 min, irrigation was performed by nurses using a homemade irrigator. The irrigator was a 20-mL syringe with a needle base connected to the front end. The excess hose was cut at 1.5–2 cm, depending on the age of the child. The syringe was filled with warm normal saline (38 °C), the hose at the front end was placed into the ear canal, and the saline was irrigated in the direction of the posterior superior wall of the ear canal. The saline solution was gently introduced along the superior wall of the ear canal, allowing its reflux force to effectively flush out the cerumen. Following removal, a cotton ball was placed at the ear canal opening while the child's head was tilted laterally to facilitate drainage of residual fluid. The canal was then carefully dried using a cotton swab. Otoscopy was performed after cerumen removal to assess the ear canal and tympanic membrane.
Preset stop rules (i.e. the operation could be terminated at any time): (1) Guardians requested to stop the operation. (2) The child indicated that he could not tolerate the procedure or the operator assessed that the child could not tolerate the procedure. (3) Repeated washing or operation for more than 20 min. (4) Serious adverse events such as ear canal injury and tympanic membrane perforation occurred during the operation. After cerumen removal, the operating nurse records the operation process and adverse events and another nurse is responsible for reassessment after the procedure. Successful cerumen removal was defined as a cerumen obstruction area of <25%, whereas failure was denoted as a cerumen obstruction area of >25% or cessation of operation.
Data collection
As this study was a prospective study, a questionnaire was designed to collect the general information (gender, age), cerumen condition (ceruminous type, cerumen obstruction, time from last cerumen removal to present), symptoms, removal conditions (methods, stopping conditions, cerumen obstruction after removal), post-removal conditions (adverse events, degree of cooperation, children's feelings), and satisfaction of guardians (comprehensive evaluation of removal results, the operational process, operational time and the children's feelings). For over 3-year-old children, data on the presence of hearing loss were collected before removal and the feelings of the children were collected after removal. The patients’ data were de-identified after data collection.
Statistical analysis
All data were analyzed using SPSS 23 (IBM, Armonk, NY, USA). Normally distributed measurement data were expressed as mean ± standard deviation (x̄ ± s) and mean differences between the two groups were compared using the t-test. Non-normally distributed measurement data were expressed as median (interquartile range) [M (P25, P75)] and compared using the Mann-Whitney U test. Categorical data were compared between groups using the chi-square test. For analysis of the risk factors of cerumen removal failure, variables with statistically significant differences in the comparison between groups were subjected to a logistic regression analysis to calculate the odds ratio (OR) and 95% confidence interval (CI). All the tests were two-tailed. Notably, multiple comparisons were not performed due to space limitations.
Results
General characteristics
A total of 209 children (347 ears) were recruited, with 198 ears in the manual removal group and 149 ears in the irrigation group. No statistically significant differences in gender, ear side, and age were found between the two groups (P > 0.05) (Table 1).
General characteristics of patients in manual removal and irrigation groups.

Chi-squared test was used for variables.
Mann–Whitney U test was used.
Cerumen condition and clinical symptoms
No statistically statistical significances were observed between manual removal and irrigation groups regarding the time from last cerumen removal to present, ceruminous type, degree of cerumen obstruction before removal, and symptoms (Table 2).
Cerumen condition and clinical symptoms of patients in manual removal and irrigation groups.
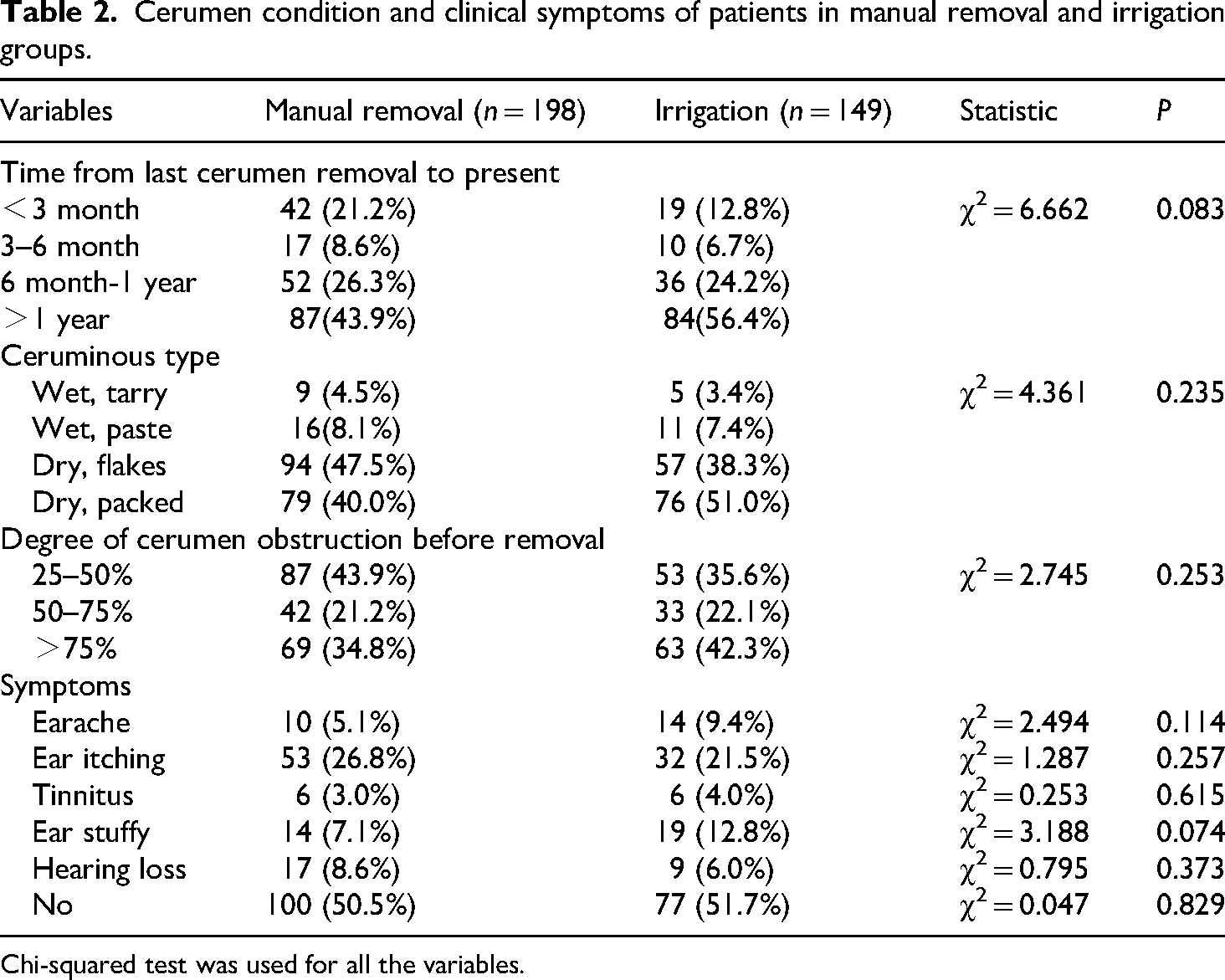
Chi-squared test was used for all the variables.
Cerumen removal
The success rates of the manual removal and irrigation groups were 76.8% and 66.4%, respectively, and the difference was statistically significant (Table 3). After successful removal, the proportion of cerumen obstruction less than 10% for the manual removal and irrigation groups was 81.6% and 92.9%, respectively, and the difference was statistically significant. This showed that cerumen removal was cleaner when the irrigation technique was used in cases who achieved successful removal. No significant difference in the degree of cooperation was found between the two groups. There were 9 cases each of adverse reactions in the manual removal group (3 cases of cough, 5 cases of external auditory canal injury, and 1 case of tympanic membrane injury) and the irrigation group (3 cases of feeling of fullness, 2 cases of cough, and 4 cases of external auditory canal injury), the incidence was not statistically significant. For children aged over 3 years old, the proportion of discomfort in manual removal and irrigation groups was 27.3% and 15.7%, respectively, with a statistically significant difference, indicating that the discomfort of irrigation was lower. Notably, satisfaction was significantly different between the two groups, with the manual removal group exhibiting higher satisfaction. The combination of the two methods was used for children who failed manual removal or irrigation alone. The success rates of the two methods combined with manual removal and irrigation groups were 99.0% and 96.0%, respectively, with no statistically significant difference (P > 0.05).
Cerumen removal in manual removal and irrigation groups.
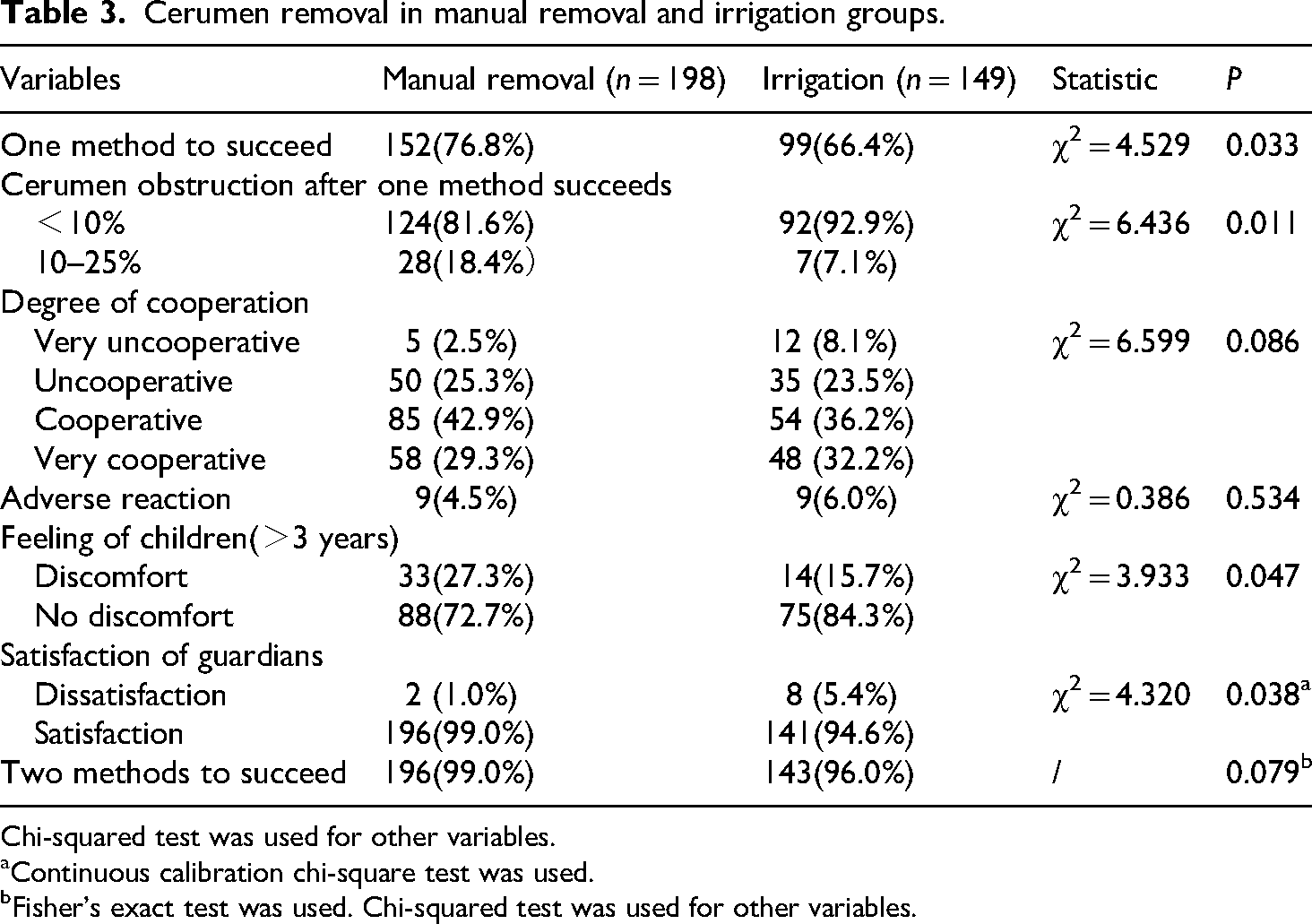
Chi-squared test was used for other variables.
Continuous calibration chi-square test was used.
Fisher's exact test was used. Chi-squared test was used for other variables.
Removal of different types of cerumen using manual removal and irrigation methods
The success rate of manual removal and irrigation methods in the removal of different types of cerumen is shown in Table 4. No statistically significant difference in wet tarry cerumen and wet pasty cerumen was found between the two methods. The manual removal group exhibited a significantly higher success rate for dry, flaky cerumen removal (93.6% vs 57.9%), whereas the irrigation group showed a significantly higher success rate for dry, packed cerumen removal (71.1% vs 54.4%), and the difference was statistically significant (P < 0.05).
Removal of different types of cerumen using manual removal and irrigation methods.

Chi-squared test was used for variables.
Fisher's exact test was used.
Analysis of risk factors for failure based on the manual removal method
Related factors in success and failure groups based on the manual removal method are presented in Table 5. Results showed that the difference of age groups, time from last cerumen removal to present, ceruminous types, degree of cerumen obstruction, and degree of cooperation were statistically significant. These variables were subjected to multivariate logistic regression analysis (Table 6). The results showed that the risk of cerumen removal failure whose time from last cerumen removal to present was between 6 months and 1 year(6m-1y) was 0.127 times (95%CI: 0.025–0.641, P = 0.012) that of whose time was less than 3 months. The risk of cerumen removal failure in cerumen obstruction of >75% and 50–75% was 115.3 and 36.1 times that of cerumen obstruction of 20–50%, respectively. The risk of failure in the uncooperative group was 5.4 times that of the very cooperative group.
Factors influencing the success and failure groups based on the manual removal method.
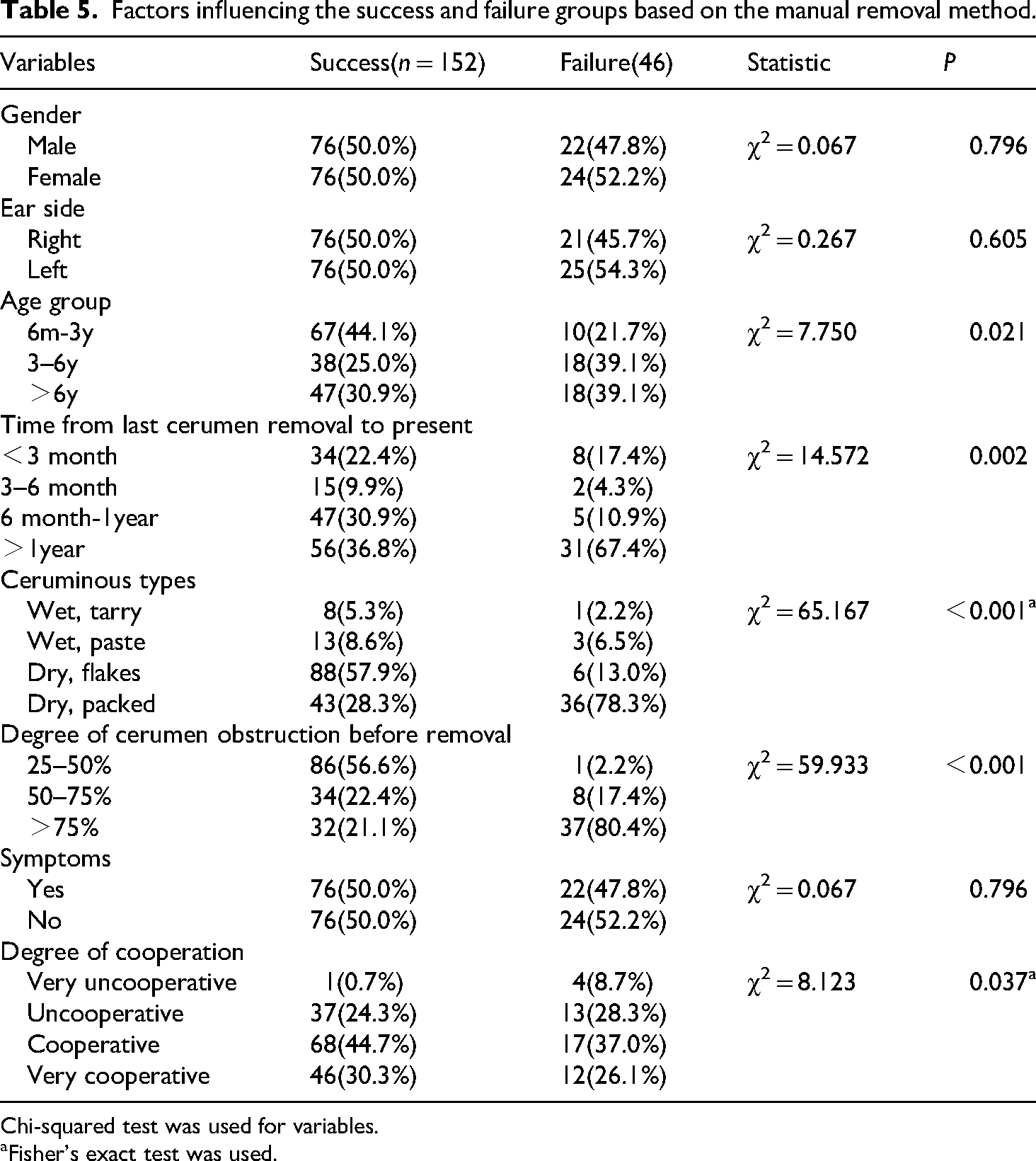
Chi-squared test was used for variables.
Fisher's exact test was used.
Multivariate analysis of the failure risks of manual removal.
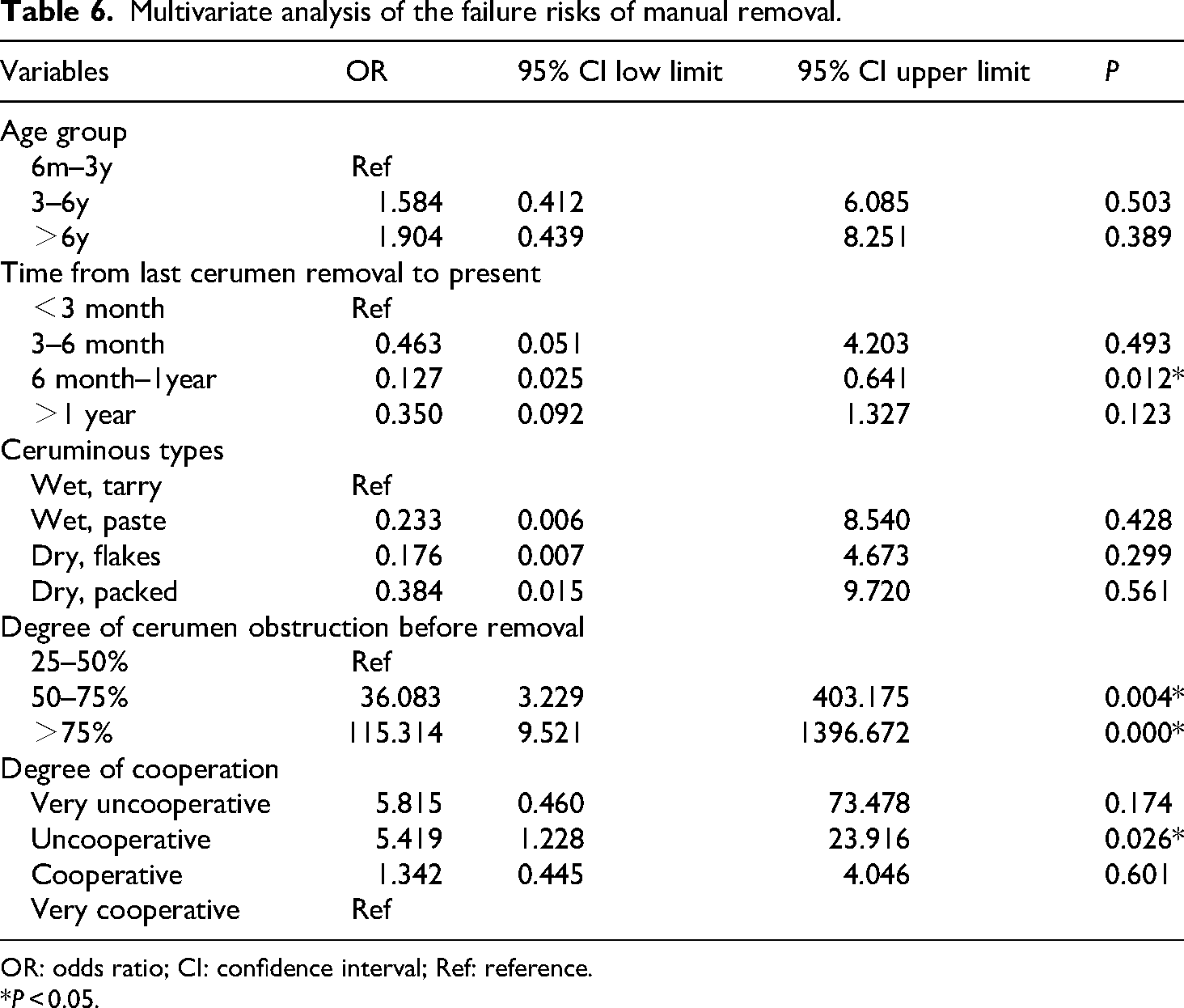
OR: odds ratio; CI: confidence interval; Ref: reference.
*P < 0.05.
Analysis of risk factors for failure based on the irrigation technique
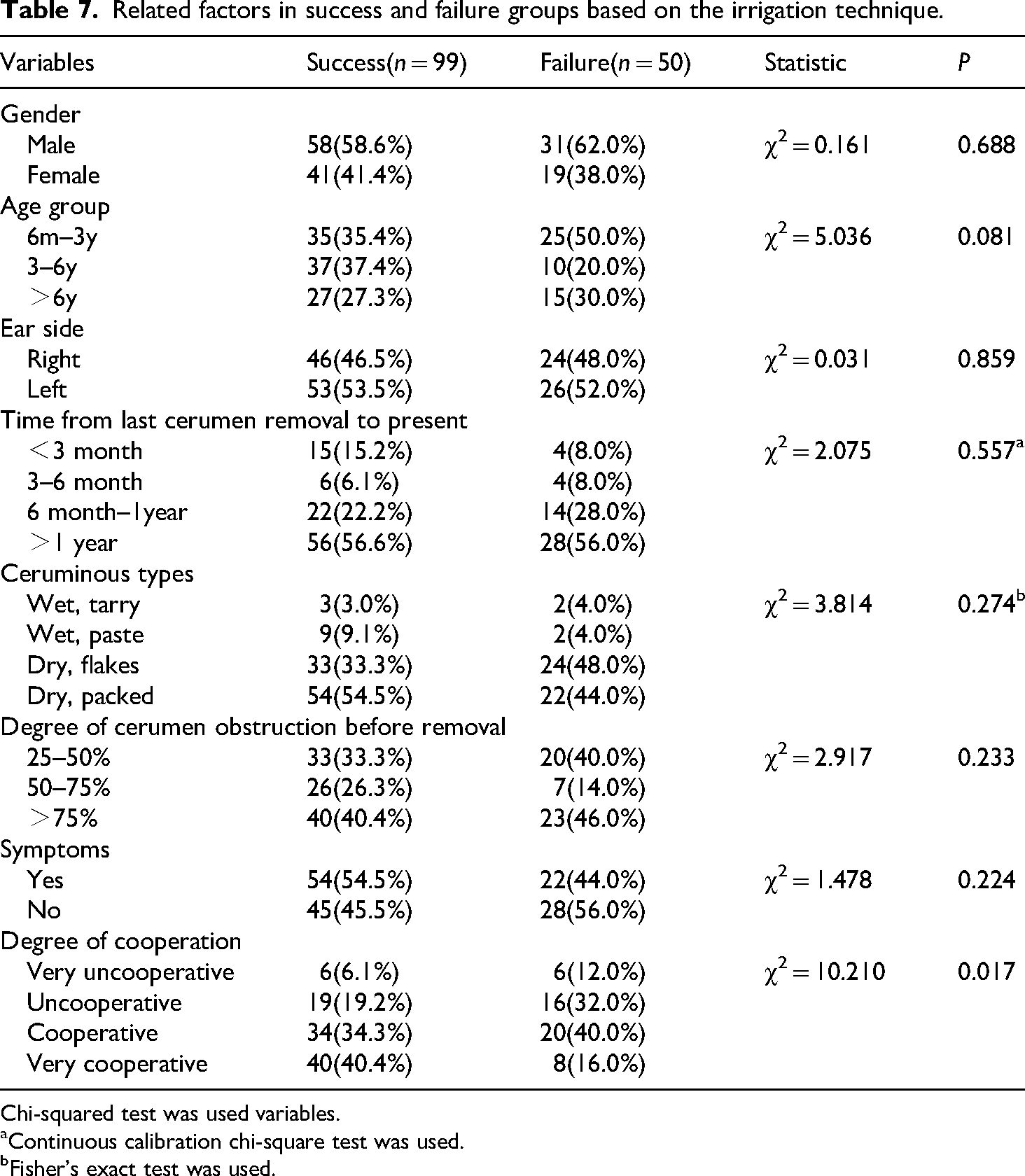
The analysis of related factors in success and failure groups based on the irrigation technique is depicted in Table 7. Results showed that only the degree of cooperation was significantly different between the two groups. Further logistic regression univariate analysis showed that the risk of failure of very uncooperative, uncooperative, and cooperative was 5.0, 4.2, and 2.9 times that of very cooperative, respectively, and the differences were statistically significant (Table 8).
Related factors in success and failure groups based on the irrigation technique.
Chi-squared test was used variables.
Continuous calibration chi-square test was used.
Fisher's exact test was used.
Univariate analysis of irrigation failure.

OR: odds ratio; CI: confidence interval.
*P < 0.05.
Discussion
Different cerumen cerumenolytic agents,12,14 ear irrigation devices,16,17 and suction devices 18 have been used in cerumen removal in various developed countries. Herein, we applied the metal instruments (cerumen hook, forceps, or ear scoops) and cotton swabs for manual removal and a simple irrigator for ear irrigation after pretreatment with hydrogen peroxide, which is cheap and readily available. This is one of the few studies exploring cerumen removal in a large sample (347 ears) of Asian children. The safety and efficacy of these two methods were analyzed to guide cerumen removal in children in economically underdeveloped areas.
Our study found that the success rate of irrigation was 66.4%, consistent with the results of Meyer et al., 12 which showed that the success rate of irrigation after using water-based cerumen cerumenolytic agents was 66.2% in 71 adults. Schwartz et al. 4 also pointed out that the success rate of irrigation was 68–92%, congruous with the results of the present study. Studies exploring the clinical application of cerumen manual removal in children are scanty due to poor cooperation among children. Shope et al. 17 reported that the success rate of manual removal using a metal curette was 65%; however, the study had a small sample size, only 17 ears. Our study found that the success rate of manual removal was 76.8%, which was higher than that of the irrigation group, with a statistically significant difference. Moreover, the satisfaction of manual removal was higher, which may be related to the high success rate, simple operation, and short operation time. Therefore, manual removal was recommended in the Department of Otolaryngology of Children's Hospital of Chongqing Medical University because of the higher success rate and higher satisfaction, due to specially trained personnel and related equipment. However, irrigation was selected in primary care hospitals owing to a lack of trained staff and related instruments, and children were referred to the otolaryngology department in the case of irrigation treatment failure. This viewpoint is consistent with previous studies.4,13
Furthermore, we found that the incidence of adverse reactions was low in the manual removal and irrigation groups, and there was no significant difference between the two groups. The incidence of the external auditory canal and tympanic membrane injuries in the two groups was 3.0% and 2.7%, respectively. This incidence is similar to the 3.7% reported in previous studies. 19 This indicates that both methods are safe for children. However, the medical staff who performed manual removal were nurses with specialized training and 5 years of experience, equipped with metal instruments and a headlamp. The incidence of adverse reactions in the manual removal group may be higher in community hospitals with no relevant equipment and inexperienced staff. Therefore, when considering the safety of different cerumen removal methods, it is also necessary to consider the experience of the operator and the related equipment.
Analysis of the degree of cerumen obstruction after successful removal showed that the proportion of cerumen less than 10% was higher in the irrigation group, suggesting that cerumen removal was less left using the irrigation approach. The reason may be that the removal of small and deeper cerumen using the manual removal method is difficult. However, these small and deep cerumen can be easily washed out after irrigation. Regarding the discomfort of children, the manual removal group had a higher proportion of discomfort than the irrigation group, indicating that irrigation was more comfortable. This is because manual removal can cause discomfort in cerumen that is hard, deep, or adheres too tightly to the wall of the external auditory canal, while the irrigation technique can greatly reduce the discomfort due to cerumen softening and irrigation with warm physiological saline.
Cerumen can be classified as “dry” and “wet” and is mainly genetically determined. The dry type of cerumen is mainly found in Asians and Native Americans, whereas the wet type is mainly found in Africans and Europeans. 1 Since the study enrolled an Asian population, the majority of cerumen (88.2%) was the dry phenotype. Guest et al. 3 believed that there is no strong evidence to support the treatment of cerumen obstruction tailored to the cerumen phenotypes. Therefore, we analyzed the success rates of different types of cerumen and found that the manual removal group exhibited a significantly higher success rate for dry, flaky cerumen removal, whereas the irrigation group showed a significantly higher success rate for dry, packed cerumen removal. This is because the dry, flaky cerumen was close to the external auditory canal wall, and was easily, directly manually removed. However, irrigation may reduce the success rate due to insufficient strength. Meanwhile, it is difficult to manually remove the dry, packed cerumen, which is often hard, as it can easily cause discomfort during the operation, resulting in a lower success rate. However, this cerumen can be easily removed by irrigation, which softens the cerumen and reduces the discomfort, thereby resulting in a higher success rate.
Surprisingly, the analysis revealed that patients who had undergone cerumen removal 6 months to 1 year prior were 0.127 times as likely to experience failure compared to those with a shorter interval (<3 months). This suggests that a 6-month to 1-year interval may serve as a protective factor against cerumen removal failure. One possible explanation is that cerumen in the 6 m-1 y period had clumps together and becomes inspissated over time which was easier to remove manually. Another possible reason is that since the cycle for cerumen removal is often 6 m-1 y, children and their guardians visit the hospital for cerumen removal, enhancing cooperation in children, which may increase the success rate. However, more studies are needed to explore the correlation between time and manual removal. Our data also demonstrated that poor cooperation is a risk factor for manual removal and irrigation failure. Poor cooperation among children not only increases the time and number of operations but also complicates the operation, thereby increasing the failure rate of cerumen removal. In addition, the risk of cerumen removal failure in cerumen obstruction of >75% and 50–75% was 115.3 and 36.1 times that of 20–50%, respectively. The degree of cerumen obstruction is an important factor affecting the success rate of direct manual removal. This may be because the heavier the degree of cerumen obstruction, the easier the formation of the wet, pasty cerumen and the dry, packed cerumen, which may further complicate manual removal. The success rate of the dry, packed cerumen was significantly lower than that of the dry, flaky cerumen in the manual removal group.
Our study subjects were divided into manual removal and irrigation groups according to the wishes of the guardians, resulting in incomplete randomization. Because both methods have their advantages and disadvantages, guardians’ voluntary choice of the method is in line with the actual situation. In addition, this can prevent the contradiction caused by adverse reactions following the selection of the removal method by the medical staff. However, this study has several limitations. (1) It was a single-center study. (2) Since more time and manpower are needed for children in the irrigation group, the sample size is not large enough. (3) Due to the small number of wet cerumen in the Asian population, the samples of wet cerumen are small. Therefore, to more sufficient statistical power, future research should prioritize large-scale, multi-center, high-quality randomized controlled trials. These studies would help establish reliable prediction models and accurately determine the success rate of cerumen removal in children.
Conclusions
In summary, this study offers valuable guidance for selecting cerumen removal methods in children. To maximize success rates, the choice of technique should be tailored to the type of cerumen present. By adopting the most appropriate removal method, healthcare providers can optimize medical resource utilization, enhance procedural success, and improve patient satisfaction.
Footnotes
Ethical considerations
This study was conducted in accordance with the Helsinki Declaration of 2024. It was approved by the Ethics Committee of the Children's Hospital of Chongqing Medical University (Approval number: 2023: 564). The study is reported according to STROBE guidelines.
Author contributions
Yao Lian collected data and wrote the manuscript, Ke Yuan finished statistical analysis, Linlin Nie and Ling Xiao checked statistical analysis and manuscript, and Ling Ding proposed ideas and finished project administration. All authors were involved in revising the manuscript and approved the final submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The raw data supporting the conclusions of this article will be made available on reasonable request.