
Abstract
Introduction
Periodontal diseases affect 3.5 billion people globally. The 2019 Global Burden of Disease report lists dental caries as the most common health issue. 1 In the United States, 42% of adults had periodontitis in 2009 to 2014, and tooth loss among adults aged 65 and over was 12.9% in 2015 to 2018.2,3 In South Korea, 17.4 million cases of gingivitis and periodontal diseases were reported in 2021. 4 Although periodontal diseases are often mild and preventable, 5 they have been linked to chronic conditions like cardiovascular disease, 6 diabetes, pulmonary disease, and cancer.7,8 In 2020, there were 19.3 million new cancer cases and 10 million deaths worldwide. 9 Cancer is a leading cause of death before the age of 70 globally. 10 In South Korea, cancer resulted in 82,204 deaths in 2020 (age-standardized rate: 69.9 per 100,000). 11 The causes of cancer include smoking, alcohol consumption, dietary habits, genetic factors, and environmental pollution. Ongoing research continues to investigate additional causes and mechanisms for cancer prevention.
Common oral diseases include dental caries, gingivitis, periodontitis, and tooth loss. Dental caries begins with bacterial activity fueled by sugar and poor oral hygiene habits, where acids produced in combination with sugars damage the teeth, leading to decay. This process can destroy the enamel of the teeth and result in structural damage to the teeth. 12 Gingivitis is inflammation of the gums surrounding the teeth and typically begins with the accumulation of dental plaque, a biofilm of bacteria formed on the tooth surface. If plaque is not adequately removed, inflammation continues to occur, and buildup can progress beneath the gumline, invading the tissues surrounding the teeth. 13 Tooth loss can occur due to various reasons, with the most common causes being dental caries and periodontal diseases. Structural damage to the teeth resulting from dental caries or periodontal diseases can destabilize the teeth, leading to their loss. 14 In the progression of these dental and periodontal damages, pathogenic microorganisms such as Porphyromonas gingivalis (P. gingivalis), Treponema denticola, and Tannerella forsythia contribute to persistent inflammation and degradation of periodontal tissues, both soft and hard. 15 Tooth loss often ensues as a consequence of severe oral disease accompanied by chronic inflammation. 16
Growing evidence suggests a link between periodontal disease and cancer, but the strength of the association and the specific types of cancer affected are still unclear. Previous studies investigating periodontal disease and cancer risk had several limitations, such as use of self-reported diagnosis of periodontal disease,17,18 a small number of cancer cases, 19 lack of information on multiple confounding factors,18,20 or population of specific age groups.16,17,19,20 Furthermore, studies have addressed the impact of periodontitis and tooth loss on cancer, but the extent to which each oral disease affects cancer remains incompletely understood.
This study aimed to investigate the impact of different oral diseases, including dental caries, gingivitis, and tooth loss, which represent varying degrees of inflammation, on the incidence and mortality of cancers in different sites. Including early-stage oral diseases such as dental caries and gingivitis, as well as severe progression stages like tooth loss, may provide a more sensitive indicator in evaluating cancer-related risk factors in the early stages of oral disease. Using standardized data collected from the National Oral Health Examination Survey conducted by dentists, three oral diseases were defined for the entire population aged 20 and above who underwent national oral health examinations. The association between oral diseases and overall cancer, as well as site-specific cancer risk, was investigated by combining the examination data of these individuals with National Health Insurance claim data and cause-of-death statistics from the Statistics Korea.
Methods
Study design and participants
This population-based retrospective cohort study used data from the National Health Insurance Service (NHIS) database (2006–2019) and National Statistics via the Micro Data Integrated Service (MDIS) (2010–2019) in Korea. The NHIS, Korea's compulsory single health insurer, provides coverage to all citizens. The NHIS includes demographic variables, health behavior variables, and healthcare utilization variables. In South Korea, adults aged over 20 must undergo health screenings every 2 years according to the National Health Insurance Act. Screenings include physical measurements, questionnaires, and oral examinations. Annually, around four million individuals receive oral examinations. The Statistics Korea collects results based on death certificates nationwide in accordance with the Statistics Act and the Act on the Registration of Family Relationships. The cause of death is compiled based on the underlying cause (the primary factor leading to death) according to the guidelines of the World Health Organization (WHO) for the International Classification of Diseases (ICD). The retrospective cohort included 3,845,280 adults aged 20 and older who had oral examinations between 1 January and 31 December 2009. Data integrated oral exam findings from 2009 with NHIS medical records, health exams, and MDIS death records. The index date was set at the 2009 initial oral examination, followed by a 10-year observation (Figure 1). The NHIS data used in this study was provided after undergoing an anonymization process to prevent personal identification. The data was securely managed and analyzed through the NHIS’s internal data analysis system, and security measures were applied to prevent external leakage of the data. This study received approval from Korea University Institutional Review Board (KUIRB-2021-0131-02 (2022.07.06)). The authors conducted this study in accordance with the Declaration of Helsinki (1975, revised in 2024), and the reporting of this study conforms to STROBE guidelines. 21
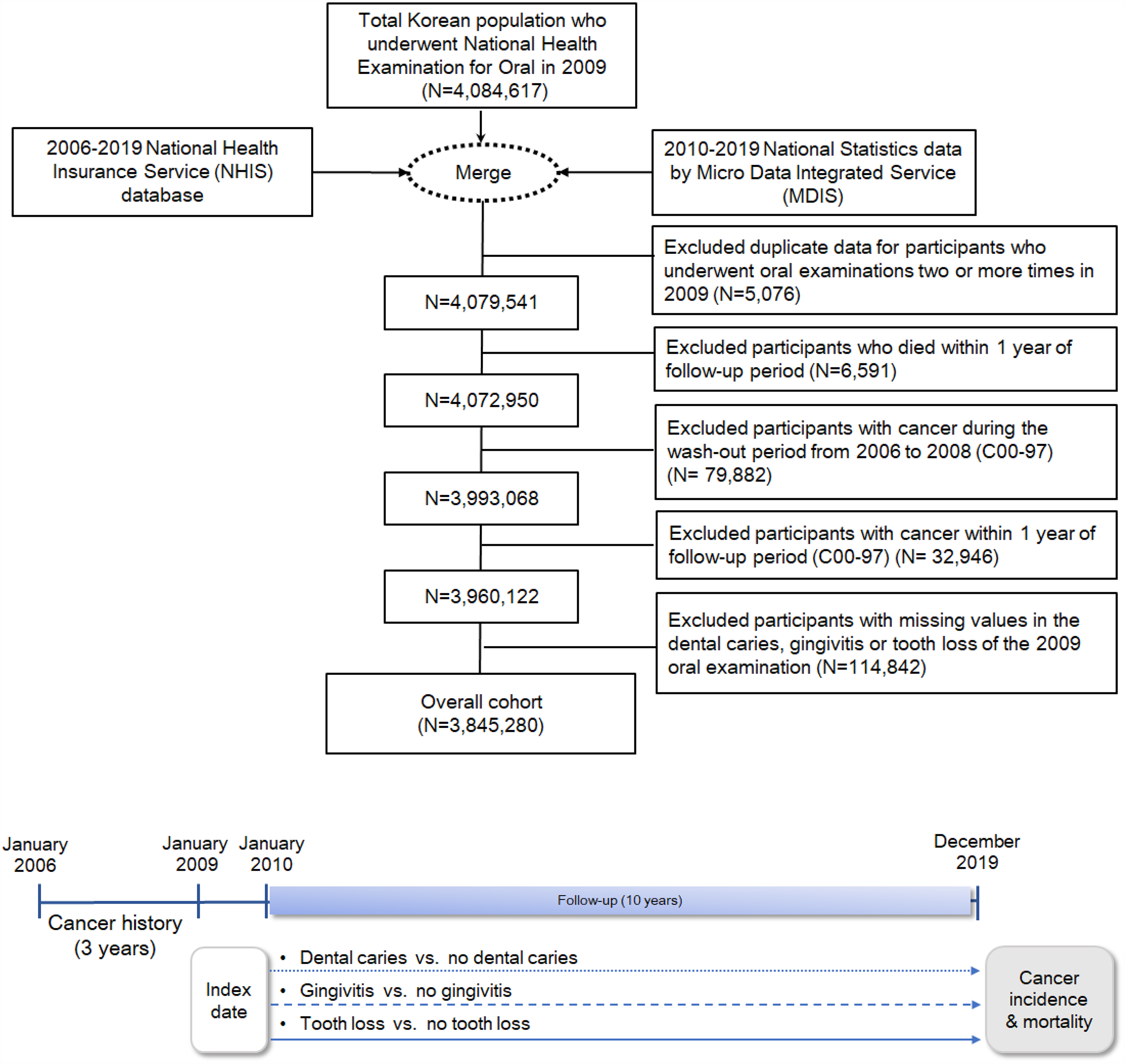
Study design and population (n = 3,845,280).
Evaluation of oral disease
Oral examination data conducted by dentists were utilized to identify oral conditions such as dental caries and periodontal disease among adults in Korea. During these examinations, dental caries, gingivitis, and tooth loss were diagnosed through tactile probing and visual inspection by dental professionals. Adults who underwent nationwide oral examinations between January and December 2009 were assessed for each oral condition based on the following criteria.
Dental caries
Participants were deemed to have dental caries if they exhibited one or more of the following criteria: (1) presence of clearly identifiable carious lesions characterized by extensive black discoloration accompanied by dentin destruction, visible blackened dentin through enamel in the lower part of the fossa; (2) confirmation of softened dentin upon minimal probing pressure, even if not initially detected during examination; (3) loss or temporary filling of permanent restoration; (4) simultaneous presence of filling and caries in a single tooth, or occurrence of secondary caries.
Gingivitis
Gingivitis was identified through visual inspection for signs of gingival bleeding or enlargement, with the following indicators: (1) mild redness and bleeding upon probe insertion; (2) severe overall inflammation, color alteration, loss of stippling, and spontaneous bleeding. Absence of visible inflammation or bleeding indicated the absence of gingivitis.
Tooth loss
Tooth loss was defined as the presence of one or more missing teeth due to dental caries, requiring prosthetic intervention for functional restoration. This variable was recorded in a binary manner, indicating whether any tooth loss was present, rather than the exact number of teeth lost. Cases involving implants or teeth previously treated and not requiring further treatment were not classified as tooth loss. In the national oral health examination program of South Korea, the evaluation of tooth loss excludes third molars (wisdom teeth) because they are often congenitally absent or electively extracted without significant functional impact. Evaluation of abnormalities in the third molars is conducted as a separate item. Therefore, the assessment focuses on the loss of 28 permanent teeth, excluding third molars.
Outcome measures
New cancer incidence and cancer-related mortality were identified during a 10-year follow-up period. Cancer incidence was defined as cancer diagnosis (C00-97 according to the ICD-10) with a new claim for primary registration code (V193 or 194) between 1 January 2010 and 31 December 2019. Cancer death cases were obtained from death certificates with cancer as the cause of death using MDIS data according to the WHO guidelines for classification of cause of death from 2010 to 2019. We further analyzed the 10 most common site-specific cancers and oral cavity/pharynx cancer in Korea,11 which are oral cavity/pharynx (ICD-10: C01-14), stomach (C16), colorectal (C18-20), liver (C22), gallbladder/biliary tract (C23-24), pancreatic (C25), lung (C33-34), breast (female; C50), prostate (male; C61), kidney (C64–65), and thyroid (C73) cancers.
Potential confounders
The detailed data were adjusted for demographic factors (age, sex, and income level), clinical factors (body mass index (BMI), FBS, Charlson comorbidity index, (CCI)) and health behaviors (smoking history, alcohol intake per week, and physical activity per week). The CCI was classified based on the ICD-10 codes using weights for 17 comorbidities. 22 Comorbidities were calculated within 1 year prior to diagnosis including inpatient and outpatient claim data. 23 Variables were categorized as Supplemental Table S1.
Statistical analysis
The independent t-test for continuous variables and Chi-square test for categorical variables were performed to compare the general characteristics of participants with and without oral disease. Continuous variables were expressed as means ± standard deviation, while categorical variables were presented as counts and percentages. The Kaplan–Meier curves with log-rank tests were used to illustrate differences in cumulative cancer risk among the three oral disease groups, using the group without any oral disease as the reference. The Cox proportional hazards model, a commonly used semiparametric method for analyzing time-to-event data, was applied. A multivariable Cox proportional hazards regression model was employed to estimate the adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) for total and site-specific cancer incidence and mortality associated with the three oral diseases. Covariates adjusted in the model included age, sex, income level, BMI, FBS, CCI, smoking history, alcohol consumption, and physical activity. Additionally, subgroup analyses were conducted to explore differences by age group (≥50/<50), income level (top 20%/middle/bottom 20%), and smoking status (never smoker/smoker). All statistical analyses were performed using SAS Enterprise Guide version 7.15 (SAS Institute, Inc., Cary, NC, USA), with statistical significance set at a two-sided P < 0.05.
Results
General characteristics
At baseline, 413,852 participants had dental caries (11.3%), 1,005,916 had gingivitis (26.2%), and 706,019 had tooth loss (18.4%). Those with tooth loss were older (mean age 62.0 ± 13.2), mostly male, in the lowest income (16.3%), and had higher blood pressure, BMI, FBS, and total cholesterol. They were also more likely to smoke (32.9%), drink alcohol frequently (≥3 times per week, 15.7%), be physically inactive (no exercise per week, 47.9%; 1–2 per week, 19.6%), and had more comorbidities (CCI score ≥3, 20.6%) compared to those without tooth loss. The oral disease group (dental caries and gingivitis) showed similar trends to the tooth loss group compared to the nonoral disease group (Table 1).
Baseline characteristics of 3,845,280 participants according to oral diseases.
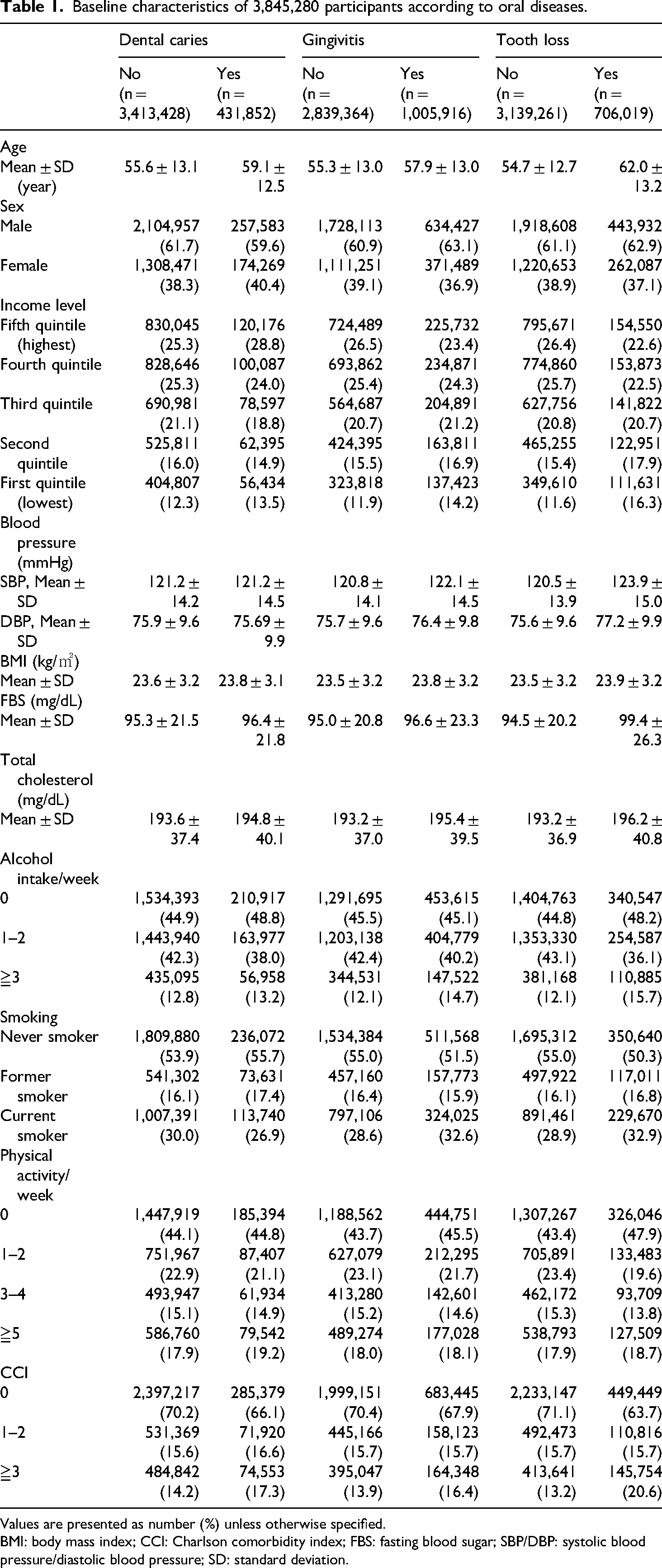
Values are presented as number (%) unless otherwise specified.
BMI: body mass index; CCI: Charlson comorbidity index; FBS: fasting blood sugar; SBP/DBP: systolic blood pressure/diastolic blood pressure; SD: standard deviation.
Cancer incidence and mortality by oral disease
A total of 3,845,280 participants with median 10.11-year follow up yielded 181,754 new cancer cases and 37,135 cancer-related deaths during 38,864,130 and 39,540,029 person-years, respectively. Cumulative total cancer incidence in the oral disease group exceeded controls, regardless of oral disease type (log-rank test, P < 0.01; Figure 2).

Cumulative incidence of total cancer in with and without oral diseases (Log-rank P < 0.01).
Adjusted for age, sex, income, BMI, FBS, CCI, smoking, alcohol, and physical activity, tooth loss significantly increased total cancer mortality (aHR: 1.12, 95% CI: 1.09–1.14). Specific cancers associated with tooth loss included stomach, colorectal, liver, and lung for incidence (aHR: 1.08, 95% CI: 1.05–1.11; aHR: 1.13, 95% CI: 1.09–1.16; aHR: 1.09, 95% CI: 1.04–1.14; aHR: 1.04, 95% CI: 1.01–1.08) and mortality (aHR: 1.21, 95% CI: 1.12–1.31; aHR: 1.14, 95% CI: 1.05–1.23; aHR: 1.16, 95% CI: 1.09–1.23; aHR: 1.08, 95% CI: 1.03–1.13). Gingivitis showed links to colorectal, liver cancer incidence (aHR: 1.07, 95% CI: 1.03–1.10; aHR: 1.08, 95% CI: 1.03–1.13), and liver cancer mortality (aHR: 1.11, 95% CI: 1.05–1.18) (Tables 2 and 3). Tooth loss and gingivitis also associated with gastrointestinal cancers (Supplemental Table S2).
Risk of total and site-specific cancer incidence of participants according to oral diseases.
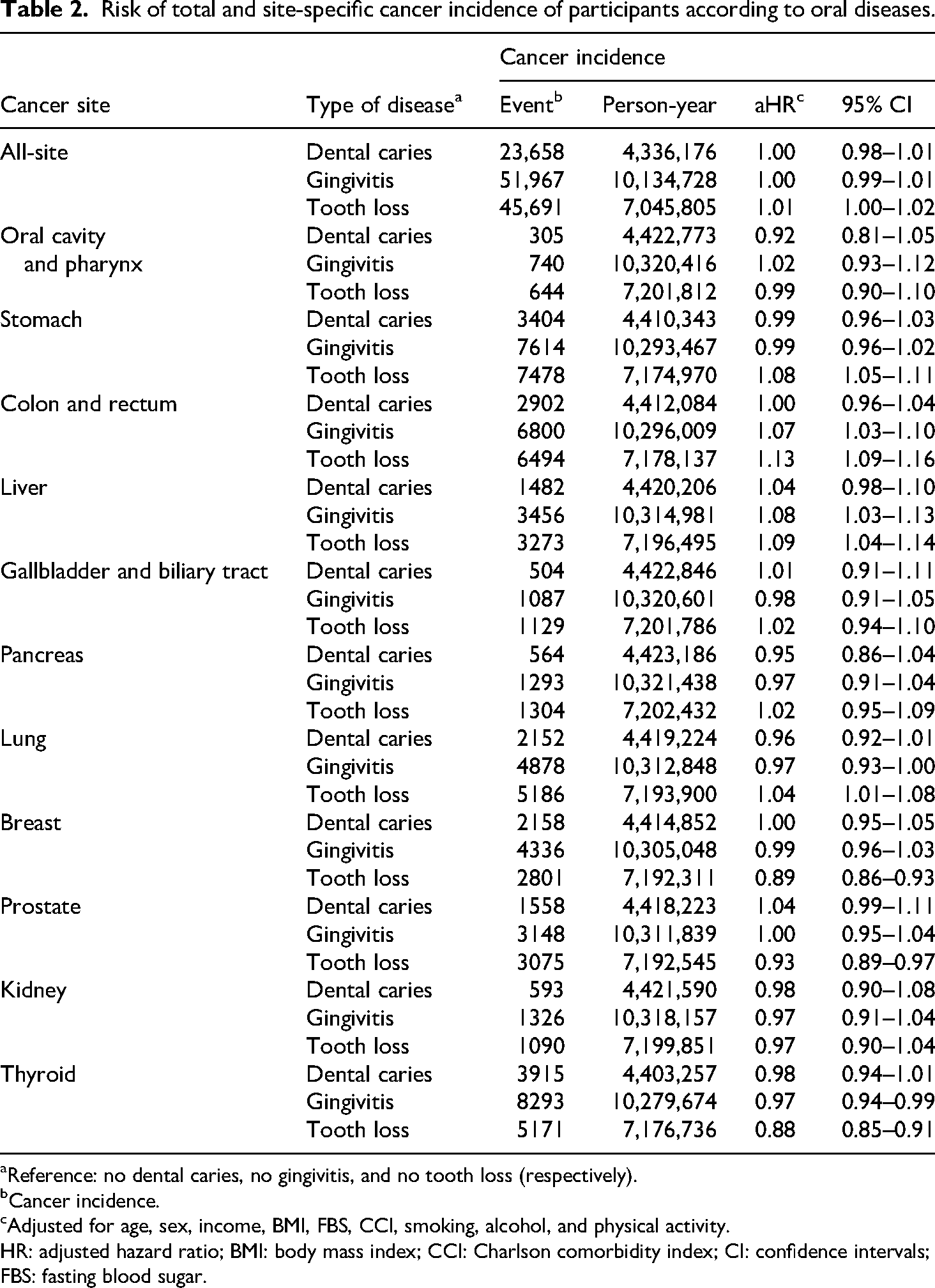
Reference: no dental caries, no gingivitis, and no tooth loss (respectively).
Cancer incidence.
Adjusted for age, sex, income, BMI, FBS, CCI, smoking, alcohol, and physical activity.
HR: adjusted hazard ratio; BMI: body mass index; CCI: Charlson comorbidity index; CI: confidence intervals; FBS: fasting blood sugar.
Risk of total and site-specific cancer mortality of participants according to oral diseases.
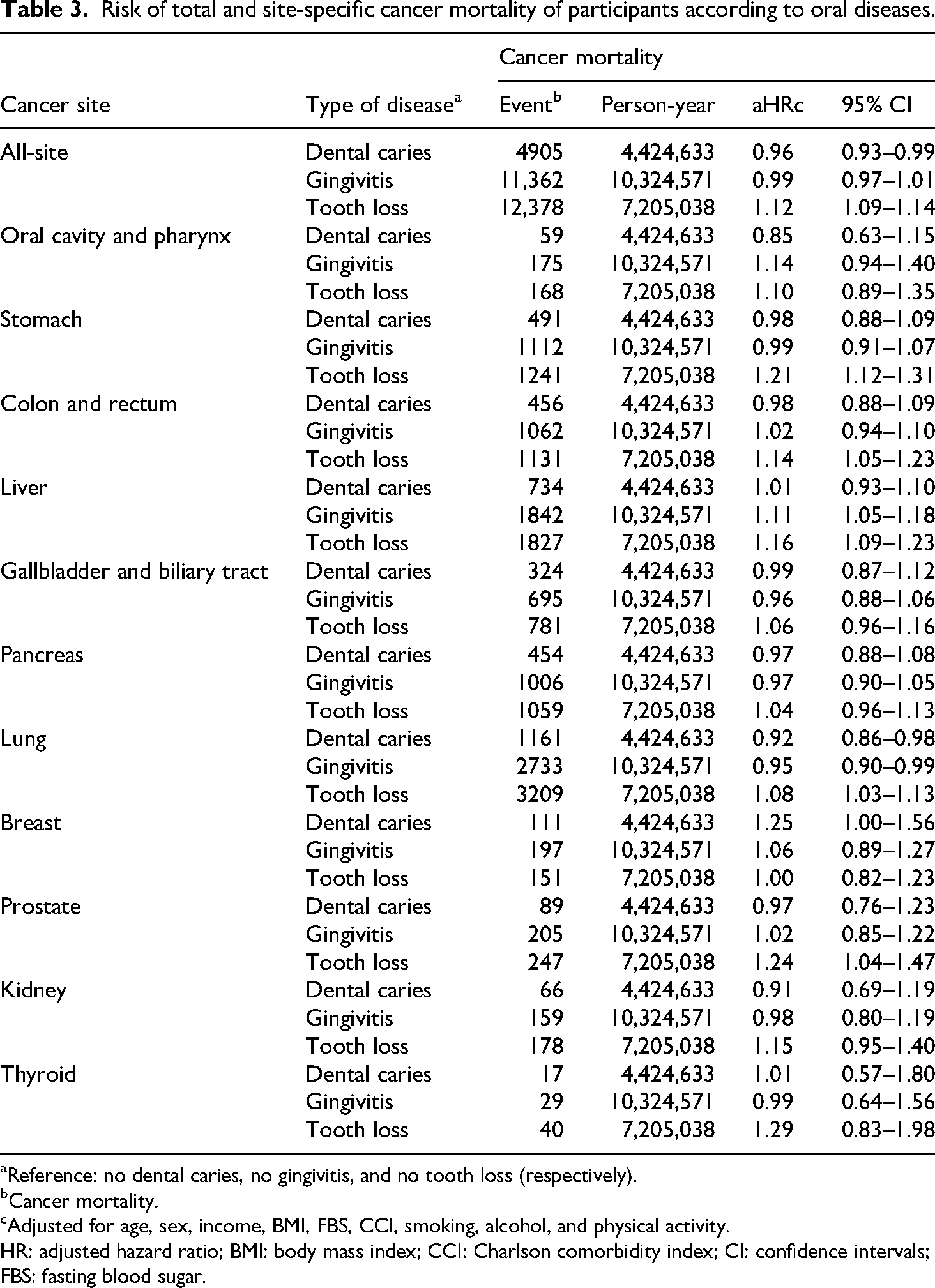
Reference: no dental caries, no gingivitis, and no tooth loss (respectively).
Cancer mortality.
Adjusted for age, sex, income, BMI, FBS, CCI, smoking, alcohol, and physical activity.
HR: adjusted hazard ratio; BMI: body mass index; CCI: Charlson comorbidity index; CI: confidence intervals; FBS: fasting blood sugar.
Subgroup analysis
We observed a stronger association between tooth loss and risk of total cancer incidence in participants over 50 (aHR: 1.18, 95% CI: 1.17–1.20) than 20 to 49 years. Over 50 s also showed heightened risk for oral cavity/pharynx, stomach, colorectal, liver, gallbladder/biliary tract, pancreas, lung, prostate, and kidney cancers (aHR: 1.16, 95% CI: 1.05–1.28; aHR: 1.31, 95% CI: 1.27–1.35; aHR: 1.36, 95% CI: 1.32–1.41; aHR: 1.27, 95% CI: 1.21–1.33; aHR: 1.32, 95% CI: 1.22–1.42; aHR: 1.26, 95% CI: 1.18–1.35; aHR: 1.34, 95% CI: 1.29–1.39; aHR: 1.29, 95% CI: 1.24–1.35; aHR: 1.11, 95% CI: 1.03–1.19). The risk of cancer in the tooth loss group tended to be higher among smokers and individuals with high income, and even among those who had never smoked, there was an increased risk of developing stomach, colorectal, and liver cancers (Figure 3).

Association between tooth loss and total and site-specific cancer incidence according to age group (A), income level (B), and smoking (C). a Adjusted for sex, income, BMI, FBS, CCI, smoking, alcohol, and physical activity (reference: no tooth loss). b Adjusted for age, sex, BMI, FBS, CCI, smoking, alcohol, and physical activity (reference: no tooth loss). c Adjusted for age, sex, income, BMI, FBS CCI, alcohol, and physical activity (reference: no tooth loss). d n = number of cancer cases among individuals with tooth loss/total number of cancer cases. aHR: adjusted hazard ratio; BMI: body mass index; CCI: Charlson comorbidity index; CI: confidence intervals; FBS: fasting blood sugar.
Discussion
Our study explored the link between cancer incidence and mortality from oral diseases in Korean adults using comprehensive data from nationwide annual oral examinations, integrated with health insurance claims and national statistics. We found that periodontal disease affects the risk of cancer incidence and mortality, especially for gastric, liver, and colorectal cancers. In addition, gingivitis increased the risk of liver cancer incidence and mortality and colorectal cancer incidence. The associations between tooth loss and cancer were stronger in participants who were older (≥50 years old) than in those under 50, and in ever cigarette smokers.
The positive association between periodontal disease and gastric cancer observed in this study aligns with findings from large cohort studies,18,24–26 as well as a supporting case-control study. 27 Despite varying definitions of periodontal disease as an independent variable, the risk ranged from 1.09 to 1.80. A meta-analysis indicated a stronger association in studies focusing on Asian populations compared to those on American and European populations. 28 Conversely, studies in Sweden, 29 the United States,17,30,31 and Japan 32 found no significant association with gastric cancer. These cohorts in the United States and Europe were limited to specific demographics (white males or females of certain ages),17,29,31 with insufficient sample sizes in case-control studies.30,32 Smoking and alcohol consumption were adjusted as confounding factors, while other variables such as income, comorbidities, and cholesterol were not adjusted. Korean dietary habits, including spicy and irritating foods 33 and high carbohydrate intake such as rice, 34 may influence gastric cancer development. Thus, while the link between periodontal disease and gastric cancer risk appears evident, further large-scale studies incorporating dietary habits are necessary for a more precise evaluation.
Beyond gastric cancer, positive associations between periodontal disease (including tooth loss) and colorectal cancer35,36 and liver cancer18,32,37 have been documented, though a minority of studies reported no association.17,30 In conclusion, despite ongoing debate, consistent reports suggest positive associations between periodontal diseases and gastrointestinal cancers. This association appears to be significantly influenced by Helicobacter pylori (H. pylori), a bacterium that colonizes the oral cavity and stomach.38,39 Considered a risk factor for gastrointestinal diseases, H. pylori contains virulence factors such as cytotoxin-associated gene A (CagA) and vacuolating cytotoxin A (VacA), which are oncoproteins involved in gastric epithelial colonization, damage, increased cell proliferation, chronic inflammation, and carcinogenesis.40,41 The oral cavity acts as a reservoir for H. pylori associated with gastric infections. Significantly, individuals with gastric cancer have exhibited poorer periodontal health, and H. pylori colonization has been detected in the oral cavity. 42 Consequently, oral hygiene practices aimed at eliminating H. pylori and related pathogens may contribute to the prevention of gastrointestinal cancers and diseases.
The association between certain cancers and oral diseases did not yield consistent results. In this study, the association between tooth loss and pancreatic cancer showed a weak association but was not statistically significant, with significant results observed only in individuals over the age of 50. This is similar to previous analyses, which indicated that tooth loss slightly increases the risk of pancreatic cancer in the general adult population, but the association was not significant. 32 Additionally, the significant results observed only in those over 50 may be attributed to age-related factors such as immune decline,7,43,44 increased inflammation,43,45 and chronic diseases. 46 However, considering the inconsistent or nonsignificant relationship between oral disease and pancreatic cancer even in older individuals,17,20,31 there is insufficient evidence to explain the impact of tooth loss on pancreatic cancer. More detailed results related to specific age groups are required.
Furthermore, this study showed that tooth loss was associated with a decreased risk of breast, prostate, and thyroid cancers. Our findings are similar to studies that suggest periodontal diseases may lower the risk of breast and prostate cancers, but these results were not statistically significant,16,17,32 and inconsistencies were also observed.29,31 Conflicting results between studies may stem from differences in study design, population, or the methods used to measure oral disease. Moreover, the inverse association observed in this study suggests that the impact of tooth loss on oral inflammation or the immune system may vary depending on the type of cancer. Further research is necessary to clarify these associations in future studies.
Although the biological mechanisms linking periodontal disease and carcinogenesis remain unclear, studies have suggested common pathways, including chronic inflammation induced by oral diseases. Research indicated that bacteria like P. gingivalis interact with the immune system within the microbiome, leading to inflammatory diseases.47,48 This chronic immune response can systemically impact cancer development,7,43,44 supported by evidence showing increased serum inflammation levels due to periodontal disease. 49 Furthermore, excessive accumulation of reactive oxygen species (ROS) from systemic inflammation can cause DNA damage and promote cancer. 45 Additionally, dysbiosis caused by P. gingivalis in subgingival microbiota and immune defenses may dysregulate gut health, potentially contributing to systemic diseases. 50 Chronic inflammation has been recognized as a risk factor for various cancers, such as lung, bladder, oral, colorectal, cervical, pancreatic, esophageal, and gallbladder cancers. 43 Consistent with the established link between inflammation and cancer, our study revealed an increased risk of lung, colorectal, esophageal, and cervical cancers across all age groups, and higher risk for stomach, liver, oral, pancreatic, and gallbladder cancers in individuals aged 50 and over.
Alternatively, common risk factors such as smoking, alcohol consumption, obesity, diabetes, and lack of physical activity have been proposed as reasons for the association between periodontal disease and cancer.7,8,48 Hyperglycemia activates pathways that increase inflammation, oxidative stress, and apoptosis.51,52 It also leads to advanced glycation end-products (AGEs) deposition in periodontal tissues and throughout the body, triggering local cytokine release via the AGEs receptor (RAGE) and altering inflammatory responses. Cytokine production in periodontal tissues may affect systemic blood glucose control and insulin signaling, 52 exacerbated by smoking-induced inflammation. In this study, we adjusted for these risk factors: smoking, alcohol consumption, physical activity, obesity, diabetes, and comorbidities. Despite adjustments, periodontal disease has consistently shown a positive association with cancer incidence and mortality, even in the never-smoking group.
The leading explanation is chronic inflammation triggered by bacteria such as P. gingivalis, impacting the systemic immune response and subsequent cancer development. However, unlike the findings for digestive cancers in our study, no association was observed with cancers of the oral cavity/pharynx, which are direct contact sites. In a prospective cohort study of adult males, periodontal disease did not significantly raise the risk of oropharyngeal cancer. 17 Similarly, in a prospective cohort study of adult females, self-reported periodontal disease showed no link to cancers of the lip, oral cavity/pharynx. 31 Case-control studies conducted in the United States, Japan, and Europe also indicated that tooth loss did not elevate the risk of head and neck cancers, consistent with our findings.32,53,54 Conversely, a retrospective cohort study reported a 1.17-fold increase in oral cancer risk due to chronic periodontitis, although this study did not adjust for major confounding factors such as smoking, drinking, physical activity, BMI, and comorbidities. 55 Given these diverse findings, it is essential to consider the interplay of various etiological factors and confounders in the development of oral cancer. Therefore, the inferences drawn from our study need to be considered with caution.
This study's strengths include its large participant base of adults of all ages, the integration of oral examination and health insurance claim data, and the diagnosis of oral diseases by dentists. It evaluated the association between cancer incidence and mortality with various oral disease severities, such as dental caries, gingivitis, and tooth loss, while adjusting for common risk factors. However, several limitations are noted. First, oral disease variables such as tooth loss were recorded in a binary format, indicating the presence or absence of the condition rather than quantifying the exact number of missing or filled teeth. Caution is warranted when comparing the findings to studies that categorized continuous measures.17,24,27,32 In addition, interpretation of the findings should take into account the methodological differences in the assessment of oral diseases. This study found that the prevalence of dental caries was 11.3%, which is similar to the 11.9% reported by the Health Insurance Review and Assessment Service (HIRA). However, the prevalence of gingivitis in this study was 26.2%, while the HIRA statistics combined both gingivitis and periodontal disease, resulting in 35.2%, indicating a difference in the definition used. 56 The prevalence of tooth loss in our study was 18.4%, but because the National Health and Nutrition Examination Survey only reports the number of remaining teeth, direct comparison with national estimates was not possible. Although the diagnosis of oral diseases in this study was made through clinical examinations by dental professionals, considering that the data was obtained from the mandatory national health screening, there may be potential for underreporting or incomplete capture of cases. Third, although nine confounding factors, including age, sex, BMI, FBS, comorbidities, and health behaviors, were adjusted using health insurance data, variables such as overall quality of life, stress, eating habits, and other potential confounders specific to each type of cancer were excluded due to data limitations. Furthermore, the analysis did not account for differences in cancer severity across cancer types. As observed in both previous studies and the present study, considering the inconsistent or potentially adverse effects, further research is needed, particularly regarding the role of periodontal disease in oropharyngeal, breast, prostate, and thyroid cancers.
Conclusions
Overall, our results suggest that periodontal disease affects the risk of cancer incidence and mortality, especially for gastric, liver, and colorectal cancers. We found that not only advanced oral disease tooth loss, but even early-stage gingivitis increased the risk of liver and colorectal cancer. Considering differences among cancer types, further experimental studies are needed to specifically prove the mechanism for the association and clarify other unknown potential risk factors.
Supplemental Material
sj-docx-1-sci-10.1177_00368504251345632 - Supplemental material for Association of oral disease with cancer incidence and mortality among adults in South Korea: A nationwide retrospective cohort study
Supplemental material, sj-docx-1-sci-10.1177_00368504251345632 for Association of oral disease with cancer incidence and mortality among adults in South Korea: A nationwide retrospective cohort study by Seung Yeon Lee and Kyae Hyung Kim in Science Progress
Footnotes
Abbreviations
Acknowledgements
We gratefully thank Professor Hyung Sik Ahn (1959–2023) for his devoted teaching and commemorate his efforts in research in the fields of preventive medicine and public health with the goal of improving evidence-based medical services.
Ethics considerations
This study was conducted in accordance with the Declaration of Helsinki, Good Clinical Practice guidelines, and national policy on the Personal Information Protection Act. This study was approved by the Institutional Review Board at Korea University (KUIRB-2021-0131-02). The methods were performed in accordance with relevant regulations.
Author contributions
KKH was involved in writing—review & editing, methodology, data curation, and supervision. LSY was involved in writing—review & editing, writing—original draft, conceptualization, methodology, formal analysis, data curation, and visualization. All authors reviewed the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available from the Korea National Health Insurance Sharing Service Institutional Data Access/Ethics Committee (![]() ) for researchers who meet the criteria for access to confidential data. However, in accordance with Korean law, the study authors are not permitted to transfer any data files to a third party.
) for researchers who meet the criteria for access to confidential data. However, in accordance with Korean law, the study authors are not permitted to transfer any data files to a third party.
Informed consent
Informed consent was waived because the NHIS or MDIS database contains publicly available anonymized data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.