
Abstract
Objective
The technological aspects of pancreaticoduodenectomy have progressed greatly, but the risk of postoperative complications, especially postoperative pancreatic fistula (POPF), postpancreatectomy haemorrhage (PPH) and mortality, is high. Therefore, we aimed to explore the safety and feasibility of pancreaticojejunostomy (PJ) under the mucosal priority healing theory through a case–control study.
Methods
We have described in detail PJ under the theory of preferential mucosal healing (PM-PJ). In a cohort of patients based on predictors of pancreatic fistula, comparisons were made according to the type of PJ: PM-PJ (n = 312); duct-to-mucosa PJ (DtoM-PJ, n = 116); and invagination PJ (IPJ, n = 109). The primary endpoint was the occurrence of clinically relevant postoperative pancreatic fistula (CR-POPF). The secondary endpoints were PPH, secondary surgery, death 90 days after surgery, and other postoperative complications.
Results
The incidence rate of CR-POPF in the PM-PJ group was not significantly different from that in the DtoM-PJ group (13.78% vs. 6.9%; p = 0.051) or the IPJ group (13.78% vs. 11.9%; p = 0.623). However, the PM-PJ group exhibited significant reductions in serious postoperative complications (7.4% versus 30.2%; p < 0.001), PPH (1.3% versus 8.4%; p < 0.001), reoperation rates (0.6% versus 9.3%; p < 0.001) and 90-day postoperative mortality rates (0.32% versus 2.6%; p = 0.023). Multivariate LASSO regression analysis revealed that BMI, hypertension, gland texture, duct size, vascular resection and pathological type were independent risk factors for CR-POPF.
Conclusions
PM-PJ is safe and reliable. During surgery, there are fewer suture needles and less trauma, which may reduce the incidence of serious complications such as postoperative bleeding and mortality.
Keywords
Introduction
Pancreaticoduodenectomy (PD), a complex general surgical procedure, remains the mainstay of surgery for the treatment of periampullary malignancies, resectable pancreatic adenocarcinoma, distal cholangiocarcinoma, duodenal adenocarcinoma and a variety of benign and premalignant conditions. 1 Pancreaticojejunostomy (PJ) essentially involves suturing of the solid pancreas and cavity organs. The pancreas itself is soft and fragile relative to the intestine, and it also secretes a large amount of digestive juice and has peak secretion within 5–19 min after eating, 2 which inevitably affects the quality of PJ. According to data from larger pancreatic surgery centres, the overall complication rate after PJ is approximately 45%. 3 There are a variety of representative PJ methods, and their healing methods also vary. However, numerous studies and analyses still cannot answer the question of the ideal or optimal PJ method, 4 and there is still a lack of relevant anastomosis theories and consensus on anastomosis methods. The duct-to-mucosa anastomosis technique ensures that the main pancreatic duct directly drains into the intestine, thereby maintaining the continuity of the pancreatic duct and jejunal mucosa. 5 The invagination anastomosis method involves fully inserting the pancreatic stump into the lumen of the jejunum, thereby enabling drainage of both the cut surface of the pancreatic stump and the main pancreatic duct. 6 According to statistics, most PJ procedures involve duct-to-mucosa pancreaticojejunostomy (DtoM-PJ), which is by far the most frequently adopted technique (78%); conversely, both invagination PJ (IPJ) and pancreato-gastrostomy are rarely employed (3% and 5%, respectively). 7 Despite this, many surgeons continue to propose technical improvements to PJ to provide the best reconstruction after PD.8–10
In clinical practice, our team studied pathological sections of the anastomosis site during PJ for patients with pancreatic duct stenosis who underwent PD and reported that the healing process of the pancreaticointestinal anastomosis site can be divided into two connections: a mucosal connection (inner layer) and a mechanical connection (outer layer). The inner layer mainly heals with the pancreatic duct epithelium through the mucosal epithelial cells of the jejunum, whereas the outer layer heals with fibrous tissue. For different current PJ methods, such as DtoM-PJ, IPJ, or bundle PJ, the final result is the connection and anastomosis of the intestinal mucosa and pancreatic duct epithelial cells. Different anastomosis methods result in different migration distances of the intestinal mucosa, with DtoM-PJ resulting in the shortest migration distance and bundle PJ resulting in the farthest migration distance. Therefore, starting from the migration distance of the intestinal mucosa, we proposed the theory of ‘mucosal priority healing during the pancreatic intestinal anastomosis healing process’. On the basis of this theory, our research team conducted a series of PJs. Here, we describe PJ under the theory of mucosal membrane priority healing (PM-PJ), with the aim of evaluating the safety and feasibility of this surgical procedure.
Materials and methods
Patients
Patients who underwent PD in the Department of Hepatobiliary Pancreatic Surgery at the Fifth Affiliated Hospital of Xinjiang Medical University between 2012 and 2024 were retrospectively reviewed using a prospectively maintained database. Pancreatic texture was defined as soft or hard according to the intraoperative judgement of the operating surgeons. This study was approved by the Ethics Review Committee of our hospital (approval number, XYDWFYLSK-2024-136). The requirement for informed consent was waived because of the retrospective nature of the study. Alternatively, an opt-out approach was used with the permission of the Ethics Review Committee. We have de-identified all patient details.
Study design
This was a retrospective study based on a prospective database. A total of 312 patients who underwent PJ under the theory of preferential mucosal healing (PM-PJ) since March 2018 at our hospital were included in the experimental group. The historical group consisted of 116 patients who received DtoM-PJ treatment and 109 patients who received IPJ treatment at our hospital from January 2012 to August 2017. All operations were open surgeries performed by the same surgeon through a midline incision. Patient data were collected through the electronic pathology system of our hospital, and patients were followed after discharge.
The inclusion criteria were as follows: the perioperative data were complete, and the diagnosis was confirmed by pathological results. The exclusion criterion was patients whose intraoperative records and postoperative treatment data were insufficient. Patients who underwent total pancreatectomy were excluded. We conducted our study in accordance with the Helsinki Declaration of 1975 as revised in 2024. The reporting of this study conforms to the STROBE guidelines. 11
Collection of clinical data
First, the general data of the patients included sex, age, height, weight, symptoms, history of coronary heart disease, hypertension, diabetes, etc.; pathological diagnosis type; American Association of Anaesthesiologists (ASA) score; postoperative pancreatic fistula (POPF) clinical risk score (CRS); portal vein resection; pancreatic texture; and pancreatic duct diameter (dilated > 3 mm; no expansion≦3 mm). Postoperative outcomes included clinically relevant POPF (CR-POPF), postpancreatectomy haemorrhage (PPH), serious complications, total length of stay, reoperation rate, 90-day mortality, and amylase in the abdominal drainage tube on the 3rd and 5th days after surgery. The pathological diagnosis was based on the pathological and immunohistochemical results of the paraffin section. Intraoperative blood loss in patients was estimated via Mercuriali's method. 12 The pancreatic duct was measured using CT scan and was considered dilated when its diameter was greater than 3 mm.
The primary endpoint was the occurrence of CR-POPF. The secondary endpoints included PPH, secondary surgery, death 90 days after surgery, and other postoperative complications.
Surgical methods
The surgical procedure involves standard pancreaticoduodenectomy, followed by pancreaticointestinal anastomosis, biliary intestinal anastomosis, and gastrointestinal anastomosis. The surgical procedure involves standard pancreaticoduodenectomy, followed by pancreaticointestinal anastomosis, biliary intestinal anastomosis and gastrointestinal anastomosis. The pancreatic stump was treated in three different ways: DtoM-PJ, IPJ and PM-PJ.
The theoretical basis of pancreatic intestinal anastomosis in the PM-PJ experimental group was preferential healing of the mucosa, and the specific surgical procedure was called PJ (Figure 1): the jejunum was intermittently sutured with two stitches to the upper and lower edges of the pancreatic stump so that the jejunum and the pancreatic stump were close and connected. Then, a similar opening to the pancreatic duct is cut in the jejunum, and the muscular layer of the jejunal opening is sutured to the pancreatic stump centred on the pancreatic duct. The anterior and posterior walls of the anastomotic site were sutured with 3–5 stitches using 5/0 or 4/0 polydioxanone sutures (PDSs), and a support tube was inserted into the pancreatic duct. Complete mucosal anastomosis with the pancreatic duct and jejunum is not needed; for small pancreatic ducts, tearing should be avoided as long as it facilitates close migration and connection between the intestinal mucosa and the pancreatic duct epithelium. Inserting a support tube into the pancreatic duct not only facilitates smooth drainage but also facilitates healing of the connection between the intestinal mucosa and the pancreatic duct epithelium. 13 A preventive drainage tube is placed above the pancreaticointestinal anastomosis and leads out of the body from the midline of the clavicle below the right rib margin. Another preventive drainage tube is placed below the pancreaticointestinal anastomosis and is led out of the body from the anterior axillary line below the right rib margin.

The anastomosis process of pancreaticojejunostomy based on the theory of mucosal priority healing (PM-PJ). (A) Intermittently suture the jejunum and pancreatic stump in a U-shape, bringing them close together without tightening, and then cut open an opening similar to the pancreatic duct in the jejunum. (B) Suture 2–3 stitches between the mucosa of the posterior wall of the jejunum and the mucosa or vicinity of the pancreatic duct. (C) Insert a support tube into the pancreatic duct and secure it slightly. (D) Complete the suturing of the mucosa of the anterior wall of the jejunum with the mucosa of the pancreatic duct or near the pancreatic duct. (E) Tighten the U-shaped suture and knot it on the surface of the jejunum to complete the anastomosis.
The DtoM-PJ procedure is carried out in the following manner. The initial step involves placing interrupted sutures with 3-4/0 polypropylene thread to connect the posterior surface of the pancreatic remnant to the jejunum. Next, a duct-to-mucosa anastomosis is performed using interrupted 5-6/0 PDS, which are placed both posteriorly and anteriorly, to join the Wirsung duct with a small incision on the jejunal loop. Finally, interrupted 3-4/0 polypropylene sutures were used to sew the anterior surface of the pancreatic remnant to the jejunum (Figure 2). The procedure of IPJ involves several steps. Initially, an outer layer is created with interrupted sutures using 3–4/0 polypropylene thread, which are placed between the posterior surface of the remaining pancreas and the jejunum. The incision on the jejunal loop should be made slightly smaller than the pancreatic remnant. Following this, a double-layered inner continuous suture is applied using 5–6/0 PDS thread for both the posterior and anterior aspects. To conclude, the outer layer of the anterior row is completed with interrupted sutures of 3-4/0 polypropylene thread, connecting the anterior surface of the pancreatic remnant to the jejunum (Figure 3).

The anastomosis process of Duct-to-mucosa pancreaticojejunostomy (DtoM-PJ). (A) The initial step involves placing interrupted sutures with 3-4/0 polypropylene thread to connect the posterior surface of the pancreatic remnant to the jejunum. (B) A duct-to-mucosa anastomosis is then performed on the posterior side. (C) On the anterior side, interrupted 5-6/0 polydioxanone sutures are used to connect the Wirsung duct to a small incision made in the jejunal loop. (D) Finally, interrupted 3-4/0 polypropylene sutures are placed between the anterior surface of the pancreatic remnant and the jejunum to complete the anastomosis.

The invagination pancreaticojejunostomy (IPJ). (A) The outer layer consists of interrupted sutures using 3-4/0 polypropylene thread between the posterior aspect of the pancreatic remnant and the jejunum. (B and C) The jejunal loop is incised to a length slightly shorter than that of the pancreatic remnant, followed by a double-layered continuous suture (B) on the posterior side and (C) on the anterior side, utilizing 5-6/0 polydioxanone thread. (D) The outer layer of the anterior row is formed by interrupted sutures with 3-4/0 polypropylene thread between the anterior surface of the pancreatic remnant and the jejunum.
Postoperative management and complications
Low-grade broad-spectrum antibiotics such as cephalosporins and penicillin should be routinely applied after surgery, and total parenteral nutrition support should be given. The retention time of the gastric tube, nutrition tube and abdominal drainage tube after surgery should be based on the actual situation and the experience of the operator. Somatostatin analogues are not used routinely. The determination of postoperative abdominal fluid accumulation and percutaneous drainage is based on the results of abdominal imaging (B-ultrasound or CT). Postoperative abdominal infection depends on whether the abdominal drainage or blood culture bacteria are positive, and high-grade antibiotics need to be replaced. PPH is defined as blood drawn from an abdominal drainage tube or stomach tube after surgery, accompanied by a continuous decrease in haemoglobin that requires the input of suspended red blood cells and plasma. The determination of POPF was based on the ISFGPS2016 standard, 14 and the risk of POPF was estimated via the CRS system. 15
Statistical analysis
Statistical data were analysed via GraphPad Prism 9.5 software. The Shapiro normality test was used to determine the normality of the sample data for continuous variables, which was represented by the mean ± standard deviation of the normal distribution. Independent sample t-tests were used for comparisons between two groups. The median (interquartile distance) was used for those that did not conform to the normal distribution, and the Wilcoxon test was used for comparisons between the two groups. The categorical variables are statistically described as frequencies (percentages), and the significance of the differences was tested via the chi-square test or Fisher's exact probability method for comparisons between groups. A logistic regression model was used to analyse the factors closely related to the occurrence of POPF. Furthermore, LASSO multiple regression analysis was conducted. The likelihood ratio test of partial maximum-likelihood estimation was used to screen independent variables. In this study, when the bilateral p value was less than 0.05, the difference was considered statistically significant.
Results
Research flow chart
Figure 4 shows a flow chart of the study design. Among all types of PD surgery in this study, PM-PJ, IPJ and DtoM-PJ were included. Notably, among the 312 PM-PJs in the experimental group, the total incidence of pancreatic fistula was 30.4% (95 cases), whereas the incidence of PPH was only 1.28% (4 cases).

Classification of Pancreaticoduodenectomy (PD) Into PM-PJ, IPJ and DtoM-PJ. These groups are divided into three groups based on the method of pancreatic intestinal anastomosis. The gray boxes represent PD patients who received different pancreatic intestinal anastomosis methods, the beige boxes represent the primary and secondary study objectives observed, the light green boxes represent the primary and secondary postoperative complications (POPF, PPH, 90 day mortality rate, and Reoperation), and the dark-blue boxes represent the multiple LASSO regression analysis and univariate logistic regression analysis of 537 PM-PJ patients based on whether clinically relevant pancreatic fistula occurred. CR-POPF, clinically relevant postoperative pancreatic fistula; PPH, post pancreatectomy hemorrhage; PM-PJ, pancreaticojejunostomy with priority mucosal healing; IPJ, invagination pancreaticojejunistomy; DtoM-PJ, duct-to-mucosa pancreaticojejunostomy.
Clinical characteristics and pathological data of patients
A total of 537 patients were included and divided into three groups, as shown in Table 1. Compared with both historical groups (DtoM-PJ or IPJ), the experimental group (PM-PJ) had no significant difference in mean age (p = 0.341) or sex (p = 0.884). There was no significant difference in patients with diabetes, hypertension, coronary heart disease or COPD before the operation. Preoperative ASA and CRS-POPF scores were not significantly different between the experimental group and the historical group. There was no significant difference in pancreatic texture or pancreatic duct diameter between the experimental group and the historical group. The proportions of patients with different clinical diagnoses, such as pancreatic head cancer, cholangiocarcinoma or ampullary adenocarcinoma, were compared and analysed among the groups, and the differences were not statistically significant. Different primary diseases do not affect the choice of the PJ method. The three sets of baseline data are comparable.
Basic characteristics of patients undergoing open PD and pancreatic anastomosis by PM-PJ, IPJ and DtoM-PJ.
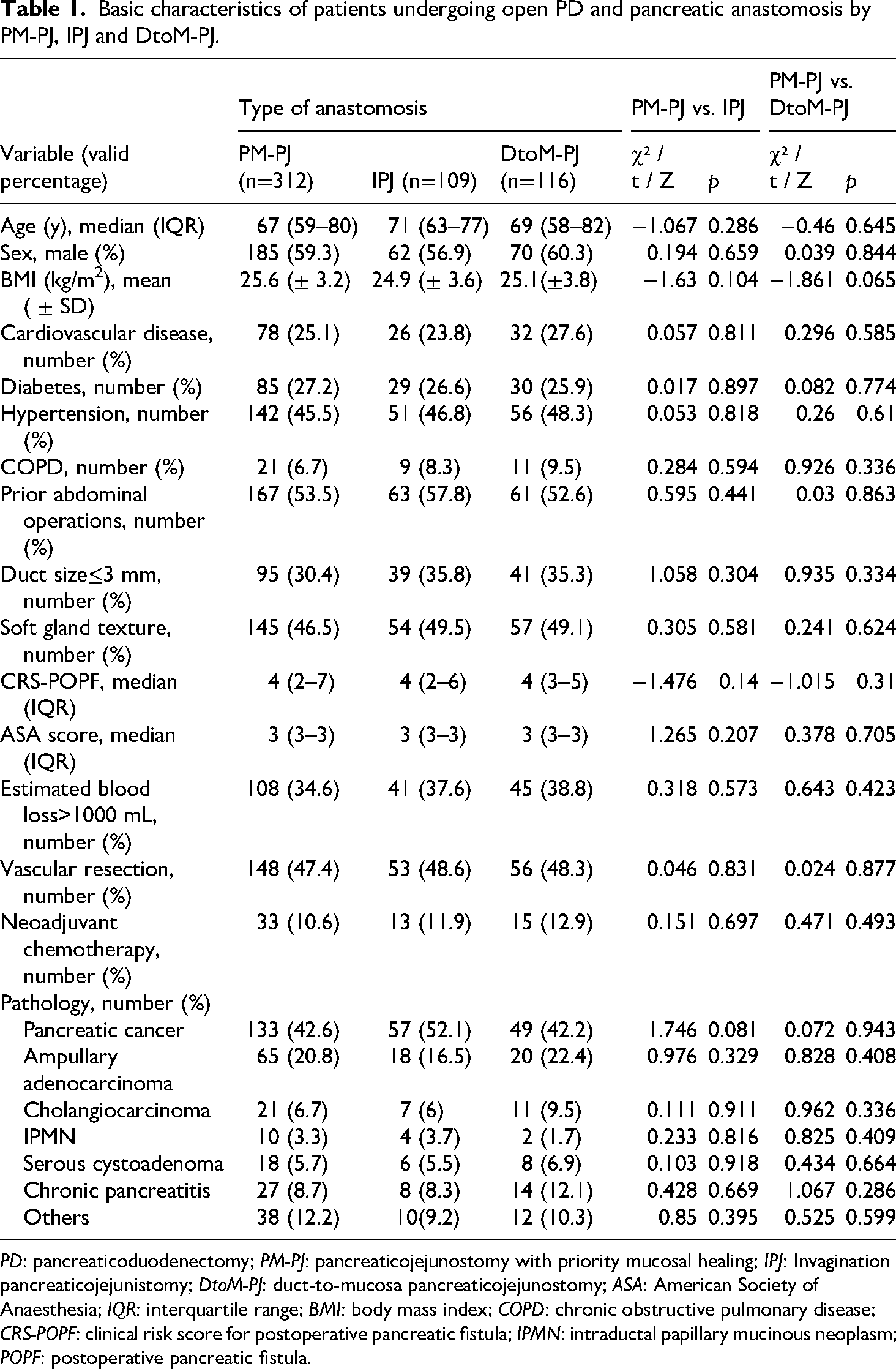
PD: pancreaticoduodenectomy; PM-PJ: pancreaticojejunostomy with priority mucosal healing; IPJ: Invagination pancreaticojejunistomy; DtoM-PJ: duct-to-mucosa pancreaticojejunostomy; ASA: American Society of Anaesthesia; IQR: interquartile range; BMI: body mass index; COPD: chronic obstructive pulmonary disease; CRS-POPF: clinical risk score for postoperative pancreatic fistula; IPMN: intraductal papillary mucinous neoplasm; POPF: postoperative pancreatic fistula.
Comparison of postoperative complications
As shown in Table 2, the incidence of POPF in the experimental group was 30.4% (95/312) compared with 27.4% (30/109) in the IPJ group, and there was no significant difference (p = 0.565); the incidence was 15.5% (25/116) higher than that in the DtoM-PJ group (p = 0.002). Similarly, the incidence of CR-POPF was 17.8% (43/312) greater than that of the IPJ group (11.9% (13/109), p = 0.623) compared with 6.9% (8/116) in the DtoM-PJ group; there was no significant difference (p = 0.704). The incidence of PPH in the experimental group was 1.28% (4/312) lower than that in the IPJ group (8.3% (9/109), p < 0.001); the incidence was also lower than 8.6% (10/116) in the DtoM-PJ group (p < 0.001). The incidence of serious complications in the experimental group was 7.4% (23/312), which was lower than that in the IPJ group (32.1% (35/109), p < 0.001); the incidence was lower than that in the DtoM-PJ group (28.4% (33/116), p < 0.001). In the experimental group, one patient died within 90 days after surgery (1.28%), which was less than the four patients (3.6%) in the IPJ group (p = 0.024). Compared with the DtoM-PJ group of two individuals (1.7%), there was no significant difference (p = 0.371). The experimental group had a postoperative reoperation rate of 0.6% (2/312), which was lower than that of the IPJ group (11.9% (13/109), p < 0.001) and lower than that of the DtoM-PJ group (7.8% (9/116), p < 0.001). The incidence of delayed gastric emptying was 11.5% (36/312) in the experimental group and 34.7% (78/225) in the historical group (p < 0.001). No intestinal or biliary fistulas occurred in the three groups after surgery.
Primary and secondary study endpoints, and other outcome variables of patients undergoing open PD with PM-PJ, IPJ and DtoM-PJ.

Bolded values mean that statistical significance was reached.
CR-POPF: clinically relevant postoperative pancreatic fistula; PPH: post pancreatectomy hemorrhage; DGE: Delayed gastric emptying; POD: postoperative days; GDA: gastroduodenal artery; IQR: interquartile range; PD: pancreaticoduodenectomy; POPF: postoperative pancreatic fistula; PM-PJ: pancreaticojejunostomy with priority mucosal healing; IPJ: invagination pancreaticojejunostomy.
Risk factors for clinically relevant postoperative pancreatic fistula
As shown in Table 3, in patients who developed CR-POPF, age and sex were not risk factors for clinical pancreatic leakage (p = 0.87 and p = 0.615, respectively). The BMI of the CR-POPF group was 25.7 (± 3.1), and the difference was statistically significant compared with that of the non-CR-POPF group (24.3 ± 1.8, p = 0.006). Among the preoperative complications, the proportion of hypertension in patients with POPF was 60.5%, which was greater than that in patients without POPF (p = 0.034). However, diabetes, coronary heart disease and COPD are not clinically relevant factors for POPF. Preoperative abdominal pain and jaundice did not have a definite effect on the occurrence of pancreatic leakage, with p-values of 0.969 and 0.324, respectively. The numbers of patients with PDAC or pancreatitis among those with POPF were 13 (30.2) and 150 (55.8), respectively, which were significantly different from those of patients with other pathological types (p = 0.005). The number of patients with vascular resection was 12 (27.9) among the patients with POPF and 136 (50.5) among the patients without POPF, which was significantly different from that of patients without vascular resection (p = 0.006). The numbers of patients with POPF that displayed a residual soft pancreas were 25 (58.1) and 120 (44.6), suggesting that patients with a soft pancreas were more prone to POPF (p = 0.02). There were 14 (32.6) patients with POPF and 203 (75.5) patients without POPF who had a main pancreatic duct diameter greater than 3 mm, which were significantly different from the 29 (67.4) and 66 (24.5) patients with a main pancreatic duct diameter less than or equal to 3, respectively (p < 0.001).
Univariate logistic regression analysis of the factors predictive of CR-POPF in PD.

Bolded values mean that statistical significance was reached.
ASA: American Society of Anaesthesia; BMI: body mass index; COPD: chronic obstructive pulmonary disease; CRS-POPF: clinical risk score for postoperative pancreatic fistula; IQR: interquartile range; PDAC: Pancreatic Ductal Adenocarcinoma; PD: pancreaticoduodenectomy; POPF: postoperative pancreatic fistula; PJ: pancreaticojejunostomy; PM-PJ: pancreaticojejunostomy with priority mucosal healing; DtoM-PJ: duct-to-mucosa pancreaticojejunostomy; CR-POPF: clinically relevant postoperative pancreatic fistula.
Table 4 presents the results of multivariate LASSO regression analysis for predicting risk factors for CR-POPF after PD. The results showed that for every 1 kg/m² increase in BMI, the risk of CR-POPF increased by 16%. The risk of CR-POPF in hypertensive patients is 2.23 times higher than that in patients with normal blood pressure. The risk of CR-POPF in patients with soft pancreatic texture is twice that of patients with hard texture. The risk of CR-POPF in patients with a main pancreatic duct diameter less than or equal to 3 is 4.48 times higher than in patients a main pancreatic duct diameter greater than 3 mm. The risk of CR-POPF in patients who undergo vascular resection is 3.32 times higher than in patients who do not undergo vascular resection. The risk of CR-POPF in patients with pancreatic cancer/pancreatitis was 2.72 times higher than that in other patients.
Multivariate LASSO regression analysis of the factors predictive of CR-POPF in PD.

BMI: body mass index; SE: standard error; β: regression coefficient; OR: odds ratio; PD: pancreaticoduodenectomy; POPF: postoperative pancreatic fistula; CR-POPF: clinically relevant postoperative pancreatic fistula.
Discussion
PJ is the main method for treating residual pancreas after PD and partial pancreatectomy. The selection of a suitable PJ method is very important for determining the prognosis. Clinical and experimental studies on PJ have been carried out, but there is no universally recognized ideal anastomosis method. 16 Especially in the case of a soft pancreas texture and a thin pancreatic duct diameter, traditional anastomosis methods are time-consuming and inaccurate, and the incidence of POPF is relatively high. 17 Over the years, many scholars have made various improvements to PJ and proposed more intuitive methods, such as ‘Hong's one-needle method’, the ‘five-needle method’ and the ‘301 method’.18–20 These methods achieve biological healing by precisely fitting the cut pancreatic section to the jejunal serous layer while the pancreatic fluid is discharged into the jejunal cavity through the stent tube, thereby preventing pancreatic fistula. The gradual acceptance of simplified and safe PJ depends on the development of technology and the surgeon's understanding of the importance of physical healing of the anastomosis.
The physiological healing and repair of the pancreatic intestinal anastomosis site share common characteristics with the classic wound healing process of the skin and other tissues.21,22 The process of epithelialization plays an important role in anastomotic healing, especially for intestinal metaplasia. Animal experimental studies on mucosal anastomosis of the bile duct and jejunum mucosa have shown that the mucosal epithelial tissue covers the proliferative connective tissue without a submucosal tissue layer, and the resulting anastomotic section shows intestinal mucosal epithelialization. 23 In conclusion, intestinal metaplasia is the pathophysiological basis of mucosal migration healing at the anastomotic stoma, and the inner layer of the anastomotic stoma is mainly healed by jejunal mucosal epithelial cells and the pancreatic duct epithelium, that is, cell–cell junction healing, which may be the basic mechanism of pancreatic tissue repair and healing at the pancreato-enteric anastomosis to maintain the smooth flow of pancreatic fluid into the intestinal cavity. Studies have shown that cell–cell connections play an important role in gap closure during wound healing, with cell migration mediating the collective migration of cells to close undamaged epithelial spaces. 24 At present, there are different PJ methods. Regardless of whether it is the IPJ, DtoM-PJ or binding PJ (BPJ) method, the intestinal mucosa and pancreatic duct epithelial cells are connected and anastomosed. Different anastomosis methods lead to different migration distances of the intestinal mucosa, with the shortest migration distances resulting from DtoM-PJ and the longest migration distances resulting from BPJ. On the basis of the migration distance of the intestinal mucosa, the anastomosis theory of preferential mucosal healing is proposed, which is very consistent with the wound repair theory. Our proposed PJ method is an improvement on the basis of the theory of preferential mucosal healing. The improvement of the theoretical anastomosis method simplifies the surgical operation, avoids the inaccuracy of the operation in a narrow space, reduces the stenosis of the pancreatic duct caused by suturing the pancreatic duct and jejunal mucosa to a certain extent, and makes the small intestinal wall more tightly wrapped and more firmly anastomosed to the pancreatic stump. The method does not require complete mucosal-to-mucosal anastomosis with the pancreatic duct jejunum. Instead, a pancreatic duct support tube is placed and secured with silk, and the suture is reduced to 3–5 stitches.
The results of this study revealed that, compared with the IPJ group and the DtoM-PJ group, the PM-PJ group presented a greater incidence of overall POPF, mainly grade A and grade B POPF (grade A POPF was 16%, grade B POPF was 12.5% and grade C POPF was 1.25%). However, there was no significant difference in the incidence of CR-POPF. In terms of secondary outcome measures, the surgical method significantly reduced the rate of PPH, the rate of serious complications, the rate of reoperation and 90-day postoperative mortality, but there was no significant difference in other complications. The incidence of POPF in the experimental group was high, but the incidence of PPH was low, which was an abnormal phenomenon compared with traditional research results. On the other hand, patients with IPJ are significantly more likely to require additional intervention due to serious complications (grades IIIa, IIIb, IV and V), including bleeding. 25 Although the incidence of POPF after BPJ is low or even zero, postoperative morbidity and mortality are still high, and the technical requirements are high. 26 Therefore, we speculate that PPH after PJ may not be closely related to POPF or that POPF may not be the main cause of bleeding. Studies have reported 27 that complicated POPF is one of the major independent risk factors for PPH, especially for delayed bleeding. However, in a recent retrospective study of 3040 postoperative bleeding sites and response strategies for PD at the Sloan Kettering Cancer Research Center, William A et al. 28 suggested that gastroduodenal artery bleeding (16.7%) was associated with vascular corrosion caused by POPF and other factors; nongastroduodenal artery bleeding (83.3%) was mainly secondary to iatrogenic injury (other abdominal blood vessels) or vascular injury (anastomotic ulcers). The conclusion that pancreatic fistula is not the main cause of bleeding after PD surgery confirms our hypothesis.
The goal of pancreatic surgical experts has always been to eliminate or reduce the incidence of pancreatic fistula. 29 Previous studies focused on dense suturing of the pancreatic stump but failed to reduce POPF, PPH or mortality, indicating that close suturing is not reliable. 30 Therefore, we should consider the histological characteristics of the pancreas itself and shift the focus to its potential complex pathophysiological mechanism, accounting for not only the individual characteristics of the patient, surgeon and surgical team but also the importance of biological healing at the anastomotic site. 31 Owing to the small number of PM-PJ suture needles used, the degree of damage to the mucosal and serosal layers is mild, and the blood flow at the anastomotic site is normal. At the same time, the pancreatic duct and jejunal mucosa are directly anastomosed, the mucosal migration distance is short, and healing is prioritized, thus achieving biological healing while ensuring the integrity of the serosal fibre connection. Although the overall POPF rate after PM-PJ is greater, owing to the proximity of the intestinal mucosa to the anastomosis and the short mucosal migration distance, the intestinal mucosa can more easily repair the needle eye, and POPF recovery is faster, which may be more consistent with the pathophysiological mechanism of pancreatic duct jejunal anastomosis healing. Moreover, ensuring that the drainage tube flows smoothly after the operation can reduce or eliminate the vascular bleeding caused by damage to and corrosion of the pancreatic fluid in the pancreas and anastomosis. Dr Cameron of Johns Hopkins University believes 3 that open drainage after PD surgery can greatly reduce PPH, infection and mortality, which is reported to be approximately 1%. The research results are similar to our findings. Although relatively little research has been conducted on the pathophysiological aspects of POPF, research on its risk factors has been extensive. In the present study, we did not find a significant correlation between sex, age, diabetes mellitus, coronary heart disease or intraoperative blood loss and the occurrence of POPF through univariate analysis. As independent risk factors affecting pancreatic fistula, pancreatic texture and pancreatic duct diameter are consistent with the conclusions reported by Casciani et al. 7
From the perspective of the completion time of the surgery and the complexity of the anastomosis process, the pancreaticointestinal anastomosis we performed is relatively simple and has the same safety as other anastomosis methods. From both security and universality perspectives, this method can be performed as a routine operation. However, this study has several limitations. First, although the data were obtained through a prospectively maintained database, there is a risk of bias associated with primary patient selection due to the limited retrospective analysis. Second, although a relatively large number of PJ procedures have been reported, our research results may not be sufficient to describe all the complications and severity after PM-PJ surgery. Third, although all surgeries were performed by the same surgical team, significant differences in sample size among the three groups may have led to various biases in the data analysis. Finally, this study presents the preliminary research results of PM-PJ, revealing that this anastomosis theory can significantly reduce PPH and mortality. However, it also reveals the shortcomings of this type of anastomosis, and the reasons for the increased incidence of pancreatic fistula need to be summarized and improved upon in future clinical work.
Conclusion
The PM-PJ ensures that the outer fibrous tissue of the anastomosis site is intact and that the inner mucosal migration distance is short, which is beneficial for healing the anastomosis and guarantees complete healing of the PJ. During anastomosis, there are fewer suture needles and less trauma, and the incidence of serious postoperative complications is comparable to that of other anastomosis methods. Therefore, the PJ we used may be considered safe and reliable.
Footnotes
ORCID iDs
Ethical considerations and consent to participate
Ethical approval for this study (number: XYDWFYLSK-2024-136) was provided by the Ethical Committee of the Fifth Affiliated Hospital of Xinjiang Medical University on 28 August 2024.
Author contributions
SW and JL wrote the manuscript; BZ performed the formal analysis; CW and AA performed the data aggregation; JZ and SZ collected the clinical data; CG performed the writing – review and editing of the manuscript; XX performed the conceptualization and methodology and obtained funding.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Natural Science Foundation of China (![]() ), China (Award Number: 82160497) and the Natural Science Foundation of Xinjiang Uygur Autonomous Region (Award Number: 2021D01C424).
), China (Award Number: 82160497) and the Natural Science Foundation of Xinjiang Uygur Autonomous Region (Award Number: 2021D01C424).
National Natural Science Foundation of China, Natural Science Foundation of Xinjiang Uygur Autonomous Region, (grant number 82160497, 2021D01C424).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.