
Abstract
Objective
This study aims to analyze anatomical parameters of the transmission route of sigmoid sinus tinnitus (SST) to explore its mechanism and speculate on possible responsible anatomical abnormalities.
Methods
Clinical data were retrospectively collected from SST and sigmoid sinus wall dehiscence (SSWD) patients suggested by temporal bone high resolution computed tomography (HRCT), with and without tinnitus, at the First Affiliated Hospital of Chongqing Medical University from January 2015 to August 2022. Patients were divided into SSWD tinnitus (n = 61), and non-tinnitus (n = 60) groups based on HRCT features. Mimics Medical 22.0 and 3-matic Medical 13.0 software measured curvature of the sigmoid sinus bone wall, defect distribution, related parameters, distance to the tympanic sinus and cochlear window, degree of mastoid pneumatization, temporal bone air chamber surface area, volume, and S/V value. Mechanisms were analyzed by comparing clinical data and imaging anatomical parameters between groups.
Results
The tinnitus group was significantly younger and had more severe low-frequency hearing loss (P = 0.002). The degree of mastoid pneumatization was significantly lower in the tinnitus group (P = 0.032). The volume of the temporal bone air chamber was smaller (P = 0.020), and the S/V value was higher in the tinnitus group (P = 0.001). Bone wall defects in the lower curvature were protective against tinnitus (P = 0.007, OR = 0.071). Larger maximum transverse diameter of the defect increased tinnitus risk (P = 0.030, OR = 1.875). Higher S/V value was also a significant risk factor (P = 0.009, OR = 24.210).
Conclusions
SST patients exhibit significant female and right-sided predominance, with low-frequency hearing loss. Defects in the superior curvature and descending part of the sigmoid groove are more likely to cause tinnitus. Larger transverse diameters and higher S/V values are independent risk factors for tinnitus. Over-pneumatized temporal bones do not facilitate transmission of sigmoid sinus blood flow murmur, highlighting the importance of specific anatomical features in SST development.
Keywords
Introduction
Tinnitus refers to the conscious auditory sensation produced by the patient when there is no corresponding external stimulus, often accompanied by irritability, anxiety, or depression, affecting work and life. Severe tinnitus can even lead to serious consequences such as suicide. 1 According to the characteristics of tinnitus, it can be divided into pulsatile tinnitus (PT) and non-PT. PT is characterized by the rhythm of blood flow or turbulent blood flow sounds. 2 Clinically, PT is more common than non-vascular PT. Among cases of PT, venous-origin tinnitus caused by abnormalities in the sigmoid sinus and mastoid structures is the most common, which is referred to as sigmoid sinus tinnitus (SST). The main imaging characteristics of SST are sigmoid sinus diverticulum (SSD) or sigmoid sinus wall defect (SSWD). As a kind of tinnitus with real physical acoustic vibration and can be detected by others or recorded by instruments, the two important conditions for causing SST are the sound source and the transmission path. Some scholars have proposed that SSWD is the main cause of SST. However, the incidence of SSWD is about 0.6% to 5% in people without PT,3,4 indicating that it is inaccurate to determine SST by only imaging characteristics of bone wall defects. 5 The temporal bone air chamber and tympanic cavity are located between the inner ear and the sigmoid sinus, which are the only way for the sound from the sigmoid sinus to the inner ear. Many factors related to transmission route, such as size and location of bone wall defect, degree of mastoid pneumatization and distance of transmission route, may be related to SST, and it is possible that the occurrence of SST is caused by the joint action of multiple factors. 6 Transmastoid approach has become the main treatment for SST, and its main purpose is to block the transmission route of SST, namely the bone wall of sigmoid sinus and mastoid air chamber. However, at present, there are few relevant studies on the transmission route of SST, and there are certain shortcomings, such as few subjects included and one-sided analysis of image anatomical parameters, leading to certain limitations in the relevant conclusions. 4 Therefore, it is important to systematically analyze the imaging characteristics of SST transmission path. Temporal bone high resolution computed tomography (HRCT) can clearly show the complex anatomical structure of temporal bone and bone changes, such as sigmoid sinus bone wall defects, which is the most non-invasive, fast and cheap imaging examination method. 7
The aim of this study is to systematically analyze the clinical features and imaging characteristics of transmission route of SST through the clinical data and HRCT of different types of SST and healthy controls, and to clarify the possible responsible lesion site and its mechanism in SST, so as to further guide clinical diagnosis and treatments.
Materials and methods
Patient selection
This is a retrospective study in which we continuously collected data on 221 patients diagnosed with SST in our department between January 2015 and August 2022. We excluded 100 patients based on incomplete insufficient data (n = 31), infeasible image quality (n = 22) and preoperative brain MRI and otoscopy showed other organic diseases of the ear, such as history of temporal bone trauma, otitis media, middle ear tympanoma, acoustic neuroma, and so on (n = 47); finally included 121 patients in this study (Figure 1). To ensure privacy and confidentiality, all patient information was de-identified before analysis. This study is based on existing clinical data, and all data usage complies with the ethical principles outlined in the 1975 Declaration of Helsinki and its 2013 revision. The research protocol was reviewed and approved by the relevant ethics committee. This study is reported in accordance with STROBE guidelines. 8 The data were collected with the approval of the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (2024SC10613-1). And all patient details have been de-identified Criteria for inclusion in the SSWD tinnitus: (a) unilateral PT; (b) positive neck compression test 7 : when the internal jugular vein of the patient was pressed or the head turned to the tinnitus side, the tinnitus symptoms were weakened or disappeared; (c) confirmed SSWD on HRCT, and complete data required. Exclusion criteria: (a) preoperative brain MRI and otoscopy showed other organic diseases of the ear, such as history of temporal bone trauma, otitis media, middle ear tympanoma, acoustic neuroma, and so on; (b) the HRCT image quality of temporal bone does not meet the diagnostic requirements. All patients included in the study had signed informed consent.

Flowchart of subject enrollment and study design.
Pure tone threshold audiometry
The Clinical Diagnostic Audiometer (Astera, Natus, Denmark) was used for hearing assessments. The patient was tested for a pure-tone hearing threshold in a noise <15 dB soundproofed room, the test method was explained to the patient, and the test was started after confirming the patient's understanding, and the pure-tone hearing threshold at 250, 500, 1000, 2000, 4000, and 8000 Hz was tested, and all patients were PTA at the initial visit. And the low-frequency hearing calculated as the average threshold at 250 and 500 Hz. 6
Acquisition and analysis of temporal bone thin-section CT
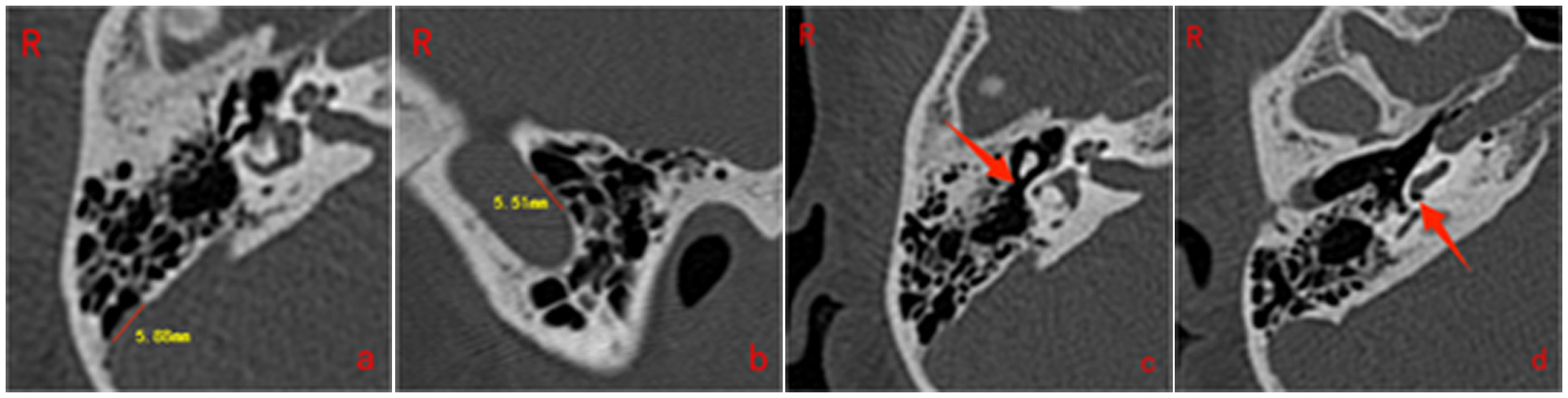
A 64-slice spiral CT scanner (Philips Brilliance, Netherlands) was used to acquire volumetric data with the patient in a supine position and no tilt angle. The scanning range was from above the frontal sinus to below the maxillary sinus. The scanning parameters included a slice thickness of 0.6 mm, slice distance of 0.3 mm, tube rotation time of 0.75 s, screw moment of 1.01, matrix of 512 × 512, and field of view ranging from 18 cm × 18 cm to 24 cm × 24 cm. The tube current was 300 mA·s per layer and the tube voltage was 130 kV. The HRCT data of the temporal bone were analyzed by radiologists with extensive experience. SSD and SSWD were determined following the methodology outlined by Zhao et al. 4 The Temporal bone HRCT image of SSWD and SSD is shown in Figure 2.The classification of the sigmoid sinus sulcus bone wall region was based on the criteria established by Essibayi et al. 9 A diagram of bone wall division and a schematic representation of sigmoid sinus wall Angle measurement are shown in Figure 3. Measurements of the maximum transverse diameter of SSWD, the maximum longitudinal diameter of SSWD, the distance between SSWD and the tympanic sinus inlet, and the distance between SSWD and the cochlear window were conducted using the techniques detailed in Table 1 and Figure 4. The degree of mastoid pneumatization was categorized according to the criteria presented in Table 2 and Figure 5, drawing upon the methodology described by Han et al. 10

Temporal bone HRCT image of SSWD and SSD.

Schematic diagram of bone wall division and internal angle measurement of sigmoid sinus wall.
SSWD correlation diameter length measurement diagram.

Classification of mastoid pneumatization degree.
SSWD related diameter line name and definition. 11

Criteria for classifying the degree of mastoid pneumatization. 12

Measurement of volume and surface area of temporal bone air chamber
Temporal bone HRCT data in DICOM format were imported into Mimics Medical 22.0 software. The reconstruction threshold was set at −1024 HU to −224 HU. The region growing function was used to separate the mastoid air cells at each scanning layer, and 3D reconstruction of the separated cell was performed. The sum of their areas represented the surface area of the temporal bone air cell, and the sum of their volumes represented the volume of the temporal bone air cell. Surface area/volume (S/V) was defined as the ratio of surface area to volume. The measurement schematic is shown in Figure 6.

Schematic diagram of volume and surface area measurement of the air chamber of temporal bone.
Measurement and classification of sigmoid sinus bone wall defect area
Temporal bone HRCT data was imported into Mimics Medical 22.0 software in DICOM format for gas cell reconstruction. The threshold for reconstruction was set at greater than 335HU, with region growing used to collect temporal bone pixels. The region of temporal bone was then cut using an editing template, followed by three-dimensional reconstruction. The reconstructed air chamber and temporal bone were then copied and imported into 3-matic Medical 13.0 software. The Lasso area mark function box selected and separated the sigmoid sinus groove surface, the adaptive Remesh function refined the curved triangular elements, and the Fill hole function repaired the defect area. Defects were classified as concentrated if the maximum defect area was at least 60% of the total defect area and diffuse if it was less than 60%. The measurement schematic is shown in Figure 7.
Tinnitus rating method
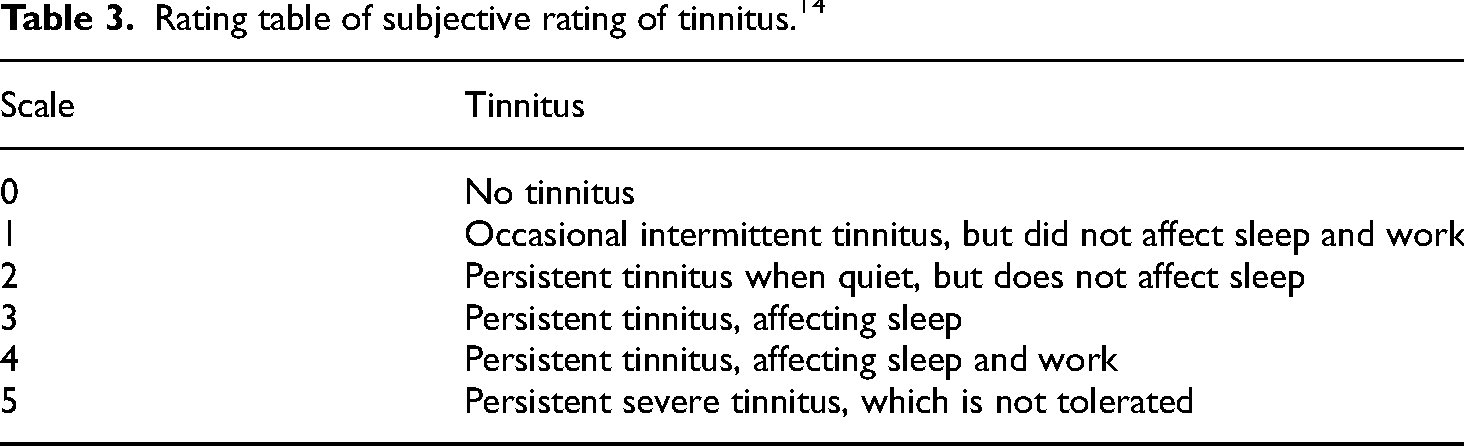
Tinnitus was subjectively rated based on the Guidelines for the Diagnosis and treatment of Ménière's disease (2017) 13 (Table 3).
Rating table of subjective rating of tinnitus. 14
Statistical analysis
The data were analyzed by SPSS version 26.0 for Windows (SPSS Inc., Chicago, IL, USA). Normality of data was assessed using the K-S test for samples larger than 50 and the S-W test for samples between 3 and 50. If P ≥ 0.05, data were considered normal; if P < 0.05, they were not. Homogeneity of variance was tested with the F test. Normally distributed data were analyzed using “mean ± standard deviation” and compared with the t-test. Non-normally distributed data were expressed as median (interquartile range), and analyzed with nonparametric tests, such as the Wilcoxon Signed-Rank test for paired samples and the Mann–Whitney U test for unpaired samples. For the analysis of composition ratio, Chi-squared test or Fisher exact probability method was used according to the situation, and binary Logistic regression analysis was used for multi-factor analysis. The value of P < 0.05 was considered significant.
Results
Comparison of clinical characteristics between individuals with subjective somatic tinnitus and individuals with subjective somatic without tinnitus
In the SSWD tinnitus, there were a total of 61 cases, with a distribution of 16 cases in the left ear and 45 cases in the right ear, and the male proportion is 4.92%. The average age of onset was 33.21 years with a standard deviation of 8.93 years, and the average duration of tinnitus was 12 months with a range of 6 to 24 months. The average body mass index (BMI) was 22.59 with a range of 20.82 to 24.05, and 5 cases (8.20%) had a history of hypertension. And an average hearing level of 20 dB (range 17.5, 27.5) was observed at the low frequencies. The study included a cohort of 60 patients in the SSWD without tinnitus group, with a distribution of 13 cases in the left ear and 47 cases in the right ear, and the male proportion is 95%. The average age of onset was calculated to be 40.95 ± 11.94 years, with a BMI of 21.91 (range 19.6, 24.38). Hypertension was present in 5 cases (8.33%), and low-frequency hearing level was measured at 15 dB (range 12.5, 22.5). The age of the SSWD tinnitus group was found to be significantly younger compared to the SSWD group without tinnitus, while the low-frequency hearing loss was more pronounced in the latter group. There was no significant difference in side, gender, BMI, hypertension, air conduction, average hearing threshold, bone conduction average hearing threshold between the two groups, as shown in Table 4.
Comparison of clinical features between group SSWD with tinnitus and group SSWD without tinnitus.
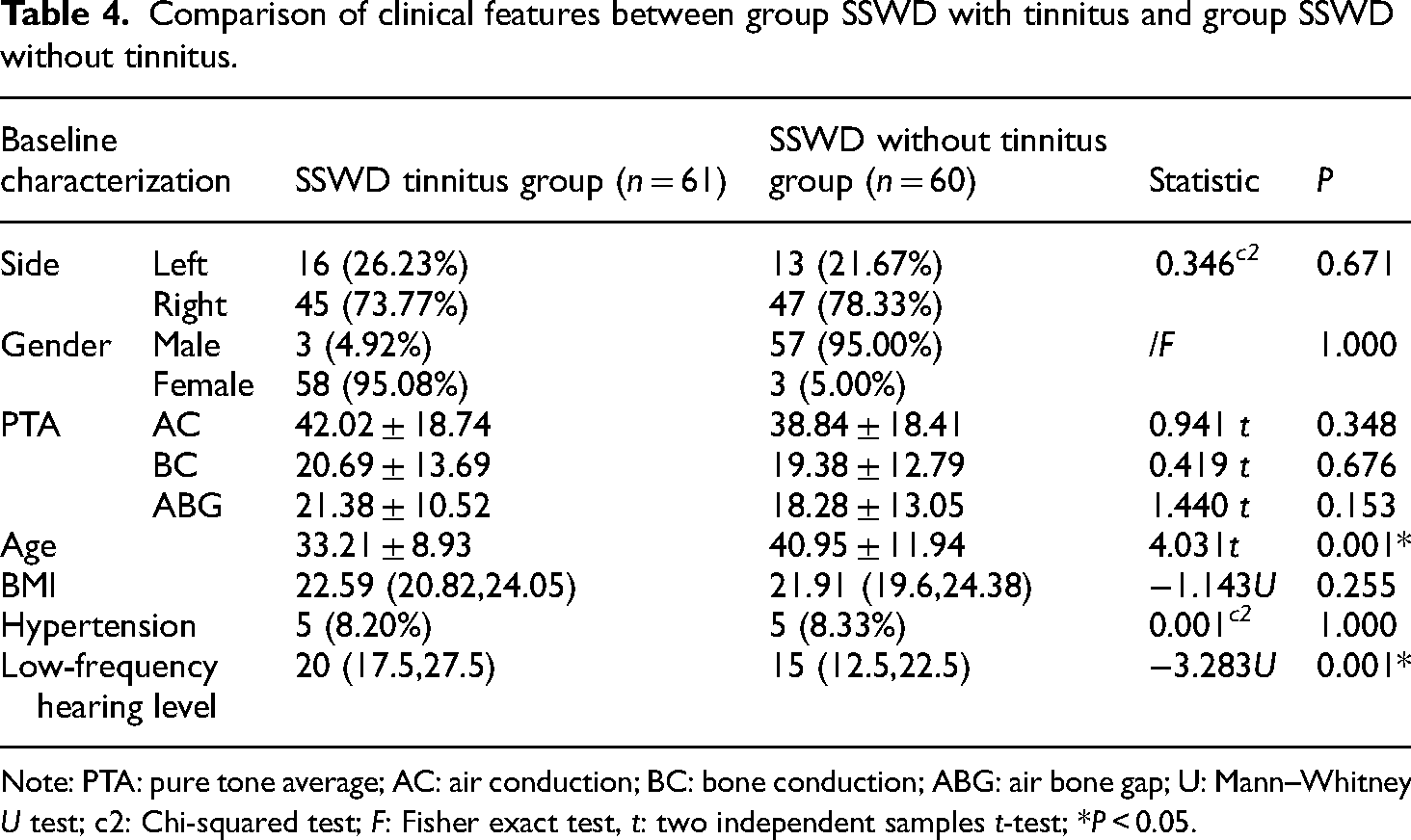
Note: PTA: pure tone average; AC: air conduction; BC: bone conduction; ABG: air bone gap; U: Mann–Whitney U test; c2: Chi-squared test; F: Fisher exact test, t: two independent samples t-test; *P < 0.05.
Comparison of imaging anatomical parameters of bone wall defects between the group of patients with SSWD and tinnitus and the group of patients with SSWD without tinnitus
Bone wall defects in the SSWD tinnitus group were mainly in the upper curvature and descending part, while the SSWD without tinnitus group had defects mainly in the lower curvature. The curvature of bone wall was smaller in the SSWD tinnitus group compared to the SSWD without tinnitus group, with statistically significant differences (P = 0.002). The tinnitus group exhibited significantly larger maximum transverse diameter (P = 0.001), maximum longitudinal diameter (P = 0.001), maximum defect area (P = 0.001), and total defect area (P = 0.001) compared to the non-tinnitus group. Conversely, there was no statistically significant difference between the two groups in terms of horizontal distribution of bone wall defects (P = 0.067), proportion of tympanic sinus communication (P = 0.240), distance between defect and tympanic sinus (P = 0.826), cochlear window (P = 0.170), and defect classification (P = 0.073) as shown in Table 5 (Figure 7).

Measurement method and classification of bone wall defect area of sigmoid sinus.
Comparison of image anatomical parameters of bone wall dehiscence between group SSWD with tinnitus and group SSWD without tinnitus.
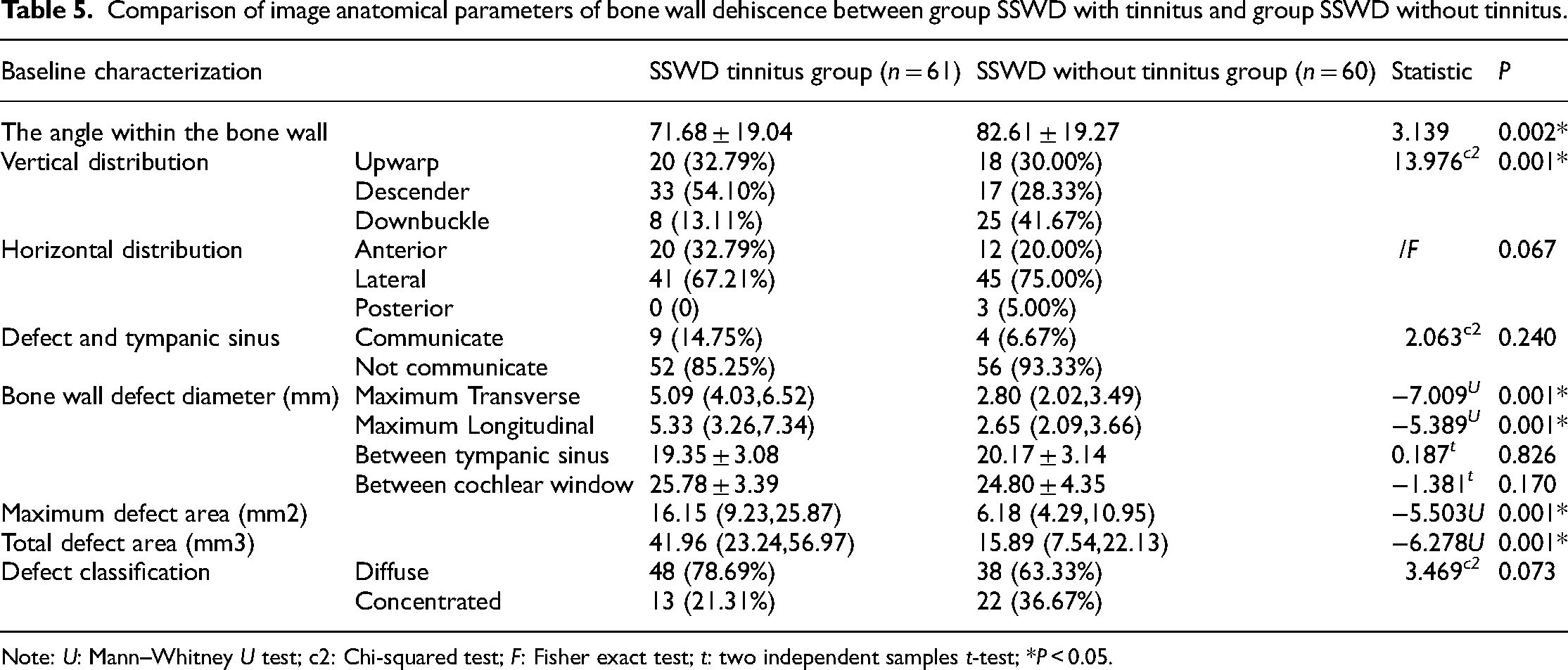
Note: U: Mann–Whitney U test; c2: Chi-squared test; F: Fisher exact test; t: two independent samples t-test; *P < 0.05.
Comparison of temporal bone air chamber anatomical parameters on the side with defects in individuals with SSWD tinnitus versus those without tinnitus
SSWD tinnitus group had worse mastoid pneumatization compared to SSWD without tinnitus group, with statistically significant differences (P = 0.032). The Tinnitus group had a smaller volume (P = 0.020) and higher S/V value (P = 0.001) than non- tinnitus group, also with statistically significant differences. No significant difference in cell surface area between the two groups (P = 0.361) (Table 6).
Comparison of image anatomical parameters of temporal bone pneumatization between group SSWD with tinnitus and group SSWD without tinnitus.

Note: U: Mann–Whitney U test; t: Two independent sample t test; *P < 0.05.
Regression analysis of clinical and imaging anatomical parameters of SSWD
Binary logistic regression analysis was employed to examine the anatomical parameters of the SSWD tinnitus and non-tinnitus groups. The dependent variable, tinnitus, was coded as “1,” while the non-tinnitus group was coded as “0.” An array of anatomical features, including bone wall curvature, upper, middle, and lower bone wall measurements, degree of mastoid pneumatization, air chamber volume, S/V ratio, maximum transverse and longitudinal diameters of bone wall defects, total defect area, and maximum defect area, were considered in the analysis. Dummy variables were created for bone wall distribution and mastoid pneumatization levels, with values assigned to each category. The contrast mode indicator was used with the first category as reference. After multivariate analysis, only the vertical distribution, S/V value, and maximum transverse diameter of the defect showed statistically significant differences between the two groups (Table 7).
Binary logistics regression analysis of clinical and imaging anatomical parameters of SSWD.

Note: β: regression coefficient; SE: standard error; Df: degrees of freedom; OR: odds ratio; CI: confidence interval; *P < 0.05.
Discussion
Somatic tinnitus, specifically subjective somatic tinnitus (SST), is contingent upon the presence of both a sound source and a transmission pathway. Various acoustic actors, such as SSD, stenosis, thrombosis, and unilateral reflux dominance, can alter local hemodynamics, leading to audible turbulence through changes in blood flow dynamics. 15 Prior research has indicated that turbulence may not be the primary factor contributing to superior semicircular canal dehiscence (SSCD). In SSCD patients, tinnitus was alleviated following repair of the sigmoid sinus bone wall, despite the persistence of turbulence, 16 a finding supported by Wang et al.'s study. 17 Several scholars have additionally suggested that the sound generated by the bone wall defect may not be attributed to turbulence, but rather to the vibration of the thinning blood vessel wall at the bone wall defect, resembling the resonance of a wind instrument reed. 6 The compromise of the integrity of the sigmoid sinus wall diminishes its ability to dampen blood flow murmurs, a critical factor in the development of sigmoid sinus thrombosis.4,16,18 Some scholars have summarized the imaging characteristics of SST as one or more defects on the sigmoid sinus wall of the dominant side of venous reflux. 4 Bone wall repair alone is sufficient to relieve tinnitus, and interventions aimed at eliminating sigmoid sinus blood flow disturbance are not necessary, 18 but may lead to sigmoid sinus reflux obstruction, causing increased intracranial pressure, and bleeding related risks. 19 In addition, Essibayi et al., 9 through finite element simulation analysis of models with different sigmoid sinus bone wall thickness, found that under the same stimulation, the vibration amplitude of monitoring nodes in the model with bone wall absence (0 mm) was 100–1000 times that of models with other thicknesses, that is, SSWD would lead to a significant weakening of the shielding effect of sigmoid sinus bone wall on vascular murmurs. The above multiple research results indicate that SSWD can be considered as the primary factor for the occurrence of SST. However, epidemiology shows that the incidence of SSWD in people without PT is approximately 0.6% to 5%,9,20 which suggests that although SSWD may be associated with tinnitus, it is not a common cause of tinnitus, and SSWD is not the only condition for SST to occur. Therefore, judging SST based solely on SSWD is not comprehensive. The possible reason is that SSWD varies greatly among individuals, and factors such as distribution location, defect size and morphology may play different roles in sound conduction or shielding, which needs further analysis. Due to the variety of shapes of SSD, which can be sac-like, fingered, and lobulated, 21 bone wall defects are mostly located on the diverticulum bone wall, and it is difficult to develop a unified standard for regional distribution. Therefore, this study only analyzed the distribution of bone wall defects in simple SSWD. The defects in the SSWD tinnitus group were mainly distributed in the lateral wall of the superior curvature and descending part of the sigmoid sinus sulcus, which was consistent with previous research reports. 4 In the SSWD without tinnitus group, the defects were mainly distributed in the inferior curvature of the sigmoid sinus, and through binary logistics regression analysis, we found that the bone wall defects distributed in the inferior curvature of the sigmoid sinus were the protective factor of PT. The reason may be that there were obvious hemodynamics in the sigmoid sinus in the superior and descending parts of the sigmoid sinus, the blood flow shear stress was larger than that in the inferior curvature, and the vibration of the vessel wall was more obvious. 22 At the same time, the distribution of air cells around the inferior curvature of the sigmoid sinus groove is different from that in the superior curvature and descending parts, which may be not conducive to low-frequency acoustic conduction, but the specific mechanism needs to be further verified in vitro.
In most people, especially women, the right side of the brain venous drainage system is larger than the left side, and the bone wall of the sigmoid sinus will be compressed due to the increase of intra-sinus or intracranial pressure. Over time, the bone wall of the sigmoid sinus will become thin or even dehissed, resulting in SSD or SSWD. 3 That is, patients with SST are mainly young and middle-aged, and tinnitus occurs without obvious causes, and the tinnitus gradually gets worse with the progress of the disease. At the same time, it is confirmed that SST is more common in women with increased BMI. 23 We found that there were differences in gender, left and right ears, age and BMI between the two groups, but only the difference between age was statistically significant. We suspect that the reason for the deviation from the epidemiological results may be that the sample size of the included studies in this paper is not as large as the sample size of the epidemiological statistics.
The maximum transverse and longitudinal diameters of SSWD can be directly measured and read by HRCT of temporal bone, which is simple and feasible, and can objectively reflect the size of the defect. In previous studies, the above diameters were used to quantify SSWD. In this study, based on measuring the above diameter line, the inner angle of sigmoid sinus as used to measure the curvature of sigmoid sinus bone wall. At the same time, the visualization of bone wall defect was realized by image post-processing software, and the area of the defect was accurately measured, and the defect was classified.
This study found that the maximum transverse diameter of the defect in the SSD group was smaller than that in the SSWD tinnitus group, but the proportion of concentrated defects was higher. We speculate that the above differences were closely related to the vascular turbulence formed locally in SSD, 24 and the bone wall at the turbulent site was compressed, thus forming localized and concentrated defects, but the specific mechanism still needs to be further studied. In addition, in the comparison between the SSWD tinnitus group and the SSWD without tinnitus group, we found through binary logistics regression analysis that the maximum transverse diameter of sigmoid sinus bone wall defect was an independent risk factor for tinnitus. For every 1 mm increase in the maximum transverse diameter of sigmoid sinus bone wall defect, the risk of tinnitus increased by 1.922 times. Considering that the shielding effect of the bone wall of the sigmoid sinus groove on blood flow gradually weakens with the increase of the transverse diameter of the defect, when the defect is small, the blood flow sounds cannot be perceived by the inner ear, and when the defect reaches the critical value, the blood flow sounds are perceived by the inner ear, resulting in tinnitus. Within a certain range, the intensity of tinnitus noise increases with the increase of the transverse diameter of the defect. 25 Therefore, we conclude that SSWD without tinnitus group may develop tinnitus over time, but it still needs to be further confirmed by prospective studies. At present, transmastoid sigmoid sinus bone wall reconstruction has achieved good clinical results in the treatment of sigmoid sinus bone wall defects and related PT, and has gradually attracted the attention of domestic experts.26,27
No matter whether the inner ear function of the patient is normal or not, when the bone wall is defective, the sigmoid sinus blood flow murmur enters the temporal bone air cells, passes through the temporal bone air cells into the tympanic sinus, enters the tympanic sinus from the tympanic sinus inlet, and vibrates the round window membrane. Finally, the sigmoid sinus blood flow murmur is perceived by the inner ear as tinnitus. 28 In this study, the entrance of tympanic sinus and round window were selected as reference points, and the distance from the midpoint of the maximum transverse diameter of the bone wall defect to them was used as the quantitative index of the length of the propagation path. In this study, there was no significant difference in the quantitative index of the length of the propagation path in each group. Considering the variety of bone wall defects, the origin center of the sound source was not the midpoint of the maximum transverse diameter of the bone wall defect, but the edge of the defect or the most disordered blood flow. At the same time, the temporal bone air chamber was divided by the atrial septum, the shape of the air chamber was irregular, and the propagation path of blood flow murmur was tortuous. It could not effectively reflect the real transmission path length, and the relevant parameters that can more effectively quantify the length of transmission path still need to be further studied.
The role of gas chambers in the temporal bone in the pathogenesis of SST has been controversial. Some scholars believe that the degree of pneumatization, of the temporal bone has little effect on the formation of SST, 11 and some scholars believe that the distribution of gas chambers in the temporal bone plays an important role in the conduction and amplification of tinnitus. 12 The temporal bone gas chamber with a small average volume can be regarded as a porous medium. This structure has sound absorption performance, and within a certain range, the smaller the aperture, the better the sound absorption performance. 14 Therefore, the small air chamber can block the vibration from the sigmoid sinus to a certain extent, while the large air chamber can increase the sound resonance and form a resonance cavity, which can amplify and filter the sigmoid sinus blood flow murmur and conduct it to the cochlea, eventually causing tinnitus. 12
In this study, the classification standard of mastoid pneumatization proposed by Han et al. 10 was used to determine the relative pneumatization degree of each temporal bone HRCT with the help of sigmoid sinus. At the same time, this study uses the threshold method to measure the surface area and volume of the temporal bone air compartment by the image post-processing software Mimics. The S/V value provides a quantitative measure to describe the morphological characteristics of the temporal bone air compartment by calculating the ratio of surface area to volume. Mimics software can provide accurate three-dimensional reconstruction and measurement. Then, the calculation process of S/V value is automated to reduce human error and improve efficiency. The accuracy of this method has been confirmed by Luntz et al. 29 Pneumatization classification and gas cell volume can reflect the degree of temporal bone pneumatization to a certain extent but cannot reflect the size of the internal gas cell. The surface area of the temporal bone is the sum of the area of the atrial septum, the area of each surface of the tympanic sinus and the area of each surface of the tympanic cavity. The more the atrial septum, the smaller the average volume of the temporal bone, and the larger the surface area of the temporal bone. Therefore, the surface area/volume (S/V) can reflect the average size of the temporal bone cell to a certain extent.
In univariate analysis, there were statistically significant differences in the degree of mastoid pneumatization, cell volume and S/V value between the SSWD tinnitus group and the SSWD without tinnitus group, but through binary logistics regression analysis, only the S/V value was the influencing factor of tinnitus, and the larger the S/V value, the smaller the average cell volume, and the higher the risk of tinnitus. However, we know that small air chambers have the characteristics of airway resistance in acoustics, which is not conducive to sound transmission. Meanwhile, Liu et al. 30 found that gasless temporal bone honeycomb will hinder sound transmission through in vitro experiments with high-simulation vascular tinnitus solid model. According to the data analysis of this study, the S/V value is positively correlated with the risk of tinnitus. We infer the following two reasons: From the data, the pneumatization of the SSWD without tinnitus group was better than that of the SSWD group, which was not caused by the poor pneumatization of the latter, but by the excessive pneumatization of the former. The optimal sound conduction frequency of temporal bone with different degrees of pneumatization is different. The well-gasified temporal bone can conduct 200 to 600 Hz sound, while the over-gasified temporal bone is more suitable to conduct 400 to 800 Hz sound and the sigmoid sinus vascular murmur is less than 600 Hz. 31 Therefore, with the increase of the average volume of the air chamber, the risk of tinnitus may increase first and then decrease. It's not just linear. The well-pneumatized temporal bone is most conducive to the transmission of sigmoid sinus vascular murmurs to the inner ear, and over-pneumatization is not conducive to low-frequency sound transmission.30,32 As the chamber dysplasia is mostly caused by otitis media lesions, 33 otitis media can lead to tinnitus and hearing impairment, the subjects with organic ear diseases were not included in this study, so it was difficult for the control group to collect patients with poor temporal bone pneumatization and meet the inclusion criteria, which resulted in certain limitations of the data and failed to fully reveal the correlation between S/V value and the risk of tinnitus. Further studies are needed.
Although the S/V value objectively reflects the average size of the air cell, due to the measurement method, the air cell covers the tympanic cavity and tympanic sinus, which cannot reflect the local distribution of the air cell around the defect. We observed in clinical practice that some patients had large air cells around the defect. When the mastoid cortex was grounded out, the integrity of the resonance cavity was destroyed, and tinnitus disappeared. However, the specific mechanism and measurement parameters still need to be further explored.
This study explored the clinical characteristics of SST, and systematically analyzed the imaging anatomical parameters of the transmission path of SST, which will help to further clarify the role of transmission path in the pathogenesis of SST and provide further guidance for clinical treatment. For example, adequate repair and reinforcement of the sigmoid sinus bone wall to block blood flow sounds; Removal of the mastoid air chamber near the weakness of the sigmoid sinus bone wall in order to reduce sound resonance and so on. This study also has limitations, mainly including the following: first, this is a single-center retrospective study, and the conclusions of this study need to be further verified by multi-center prospective studies in the future; Secondly, this study did not quantitatively evaluate the sound source, but only analyzed it from the perspective of propagation path. It is necessary to include both of them in further research to obtain a completer and more reliable conclusion. Thirdly, due to the lack of postoperative imaging follow-up data, it is impossible to compare and analyze the preoperative and postoperative imaging anatomical parameters.
Conclusions
SST patients are mainly young and middle-aged, and the tinnitus is gradually aggravated with the progress of the disease. The superior curvature and descending defects of sigmoid sinus are more likely to cause tinnitus than the inferior curvature defects; the maximum transverse diameter of SSWD defect is an independent risk factor for tinnitus. The larger the transverse diameter of the defect, the higher the risk of tinnitus. The S/V value of SSWD without tinnitus group was lower than that of SSWD group, suggesting that the over-pneumatized temporal bone may not be conducive to the transmission of sigmoid sinus blood flow murmur. Based on the above conclusions, we suggest that in the transmastoid approach to repair the superior curvature and descending part of sigmoid sinus defect, some peripheral air cells should be eliminated, and the distribution of specific air cells should be destroyed, which may achieve better therapeutic effect. In addition, in the follow-up study, we will try to cooperate with scientific and technological universities to establish a dynamic model of fluid circulation in the sigmoid sinus for further research and discussion of this study.
Footnotes
Acknowledgements
The authors sincerely thank all the patients and their families involved in this study, as well as the Chongqing Municipal Health Commission for providing financial support.
Authors’ contributions
HK, XO, and BX designed the study, XW, JX, and JH collected information, HK, XO, and BX analyzed the data and drafted the manuscript, DY designed, funded, reviewed the manuscript, and approved the final version of the article for publication. All the listed authors meet the authorship criteria and agree with the final content and submission of the manuscript.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Financial support from the Chongqing Municipal Health Commission was gratefully acknowledged (2024WSJK075).
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.