
Abstract
Objectives
Silicone oil (SO) is a commonly used intraocular tamponade in the treatment of rhegmatogenous retinal detachment (RRD). SO emulsification is a common complication after SO injection. This study aimed to investigate correlations between SO emulsification signs on ultrasound biomicroscopy (UBM) and the real number/size of SO droplets.
Methods
An observational, cross-sectional study. Thirty-five RRD patients (19 males; 35 eyes) who underwent pars plana vitrectomy and SO injection were enrolled in the study. SO emulsification signs on UBM (endothelial deposits, floating droplets, ghost images, hyperoleon, anterior chamber angle impregnation, anterior iris surface impregnation, posterior iris surface impregnation and ciliary body impregnation) were acquired and quantified two days before SO removal, while real number/size of the SO droplets with a diameter in 0.4–20 μm in the first 2 mL washout fluid collected intraoperatively during SO removal were assessed by Coulter counter. Then the correlations between these values were explored.
Results
The grade of tissue impregnation and hyperoleon area in the anterior chamber demonstrated significant correlations with the number of large (5–20 μm) SO droplets (r = 0.336; P = 0.048 and r = 0.350; P = 0.039, respectively); however, no significant correlations were observed with the total number of droplets (0.4–20 μm)or the number of small (0.4–5 μm) droplets (both P > 0.05).
Conclusion
The UBM quantitative grade of tissue impregnation and hyperoleon area in the anterior chamber could provide a noninvasive overview of the actual degree of SO emulsification before SO removal surgery.
Keywords
Introduction
Silicone oil (SO) is the standard tamponade method for complex vitreoretinal diseases;1,2 however, SO emulsification remains a concern, 3 which accounts for most complications associated with SO, particularly the increase in intraocular pressure (IOP).4–7
Previous studies have reported the accurate evaluation of SO emulsification using Coulter counters, B-scan ultrasonography and ultrasound biomicroscopy (UBM). While Coulter counters can measure the number and size of SO droplets, this evaluation is only possible after SO removal.8–10 Similarly, B-scans can only aid in postoperative assessment, in contrast to UBM, which can be performed preoperatively. Grigera et al. 11 demonstrated that UBM can be used to examine in detail various signs of SO emulsification. Avitabile et al. 12 first reported the value of UBM in predicting SO-related complications, identifying a positive correlation between SO droplets in the anterior chamber (AC) and the occurrence of elevated IOP. Recently, we reported that UBM can be used to evaluate the degree of SO emulsification before SO removal, and higher UBM grading results were associated with younger age, male sex, and elevated IOP. 13
However, the relationship between the grading of UBM signs and the actual number of intraocular SO droplets remains unclear. Therefore, we recruited a group of patients who underwent both UBM and Coulter quantification, and we explored the correlations between the results of the two tests. The study was designed to characterize the status of SO emulsification preoperatively.
Materials and methods
Study subjects and ethics statement
This study was an observational, cross-sectional study. Consecutive rhegmatogenous retinal detachment (RRD) patients who underwent SO injection, followed by SO removal, at the Eye and Ear, Nose, and Throat (ENT) Hospital of Fudan University between January 2021 and September 2022 were enrolled. Patients who had previously received an SO injection, IOP > 21 mmHg prior to pars plana vitrectomy (PPV)+SO injection, had diabetes, under 18 years old at the time of the initial surgery or recurrence of retinal detachment after SO removal surgery were excluded in the study.
The Eye and ENT Hospital of Fudan University human research ethics committee approved this study (2014026, approved on 30 June 2014). Written informed consent was obtained from the subjects prior to study initiation.
Surgery
SO injection: All patients underwent the standard three-port, 23-gauge PPV carried out by a single surgeon (CH Jiang) using the Alcon Constellation system (Alcon Laboratories, Inc., Fort Worth, TX, USA). Following the elimination of the central vitreous, triamcinolone acetonide was administered to aid in visualizing the remaining posterior hyaloid, which was subsequently excised. The need for supplementary procedures, including membrane peeling, injection of perfluorocarbon liquid (DK-line), performing a relaxing retinotomy, and conducting an inferior peripheral iridectomy, was determined by the condition of the retina. Subsequent to a fluid–air exchange and endophotocoagulation, SO (5700 cSt; Bausch & Lomb Inc., NY, USA) was injected.
SO removal: During SO removal surgery, according to the method described by Chan et al., 8 the first 2 mL of washout fluid after the bulk of the SO was removed and collected, then fluid–air exchange was performed. Additional procedures such as membrane peeling, phacoemulsification, IOL implantation were performed depending on the state of lens or retina.
Main ophthalmic measurements
Two days before SO removal, a standard ophthalmic examination was performed, including slit-lamp microscopy, dilated fundus examination, best-corrected visual acuity (BCVA). IOP was measured using non-contact tonometry. The axial length (AL) was measured by an intraocular lenses master (version 3.01; Carl Zeiss Meditec, Jena, Germany). The SO signs were acquired by UBM (MD-300L, Meda Co., Ltd, Tianjin, China). Demographic data and clinical history including history of ophthalmic trauma or intraocular surgery, duration of in-situ SO, and lens status (aphakic/phakic/pseudophakic), were also collected for each patient.
UBM examination and analysis
UBM was performed by the same experienced ophthalmologist (HM Zhao) according to the methods reported by Grigera et al. 11 and Avitabile et al. 12 with the patient lying in the supine position. A central scan along the horizontal meridian and scans at eight-hour intervals around the clock were conducted. The following signs were suggestive of SO emulsification: (1) endothelial deposits (Figure 1(a)); (2) ghost images (Figure 1(a)); (3) hyperoleon: a massive collection of emulsified particles (Figure 1(a)); (4) floating droplets (Figure 1(b)); and (5) impregnation of tissues: impregnation of the anterior chamber angle (ACA), anterior /posterior iris surface, or ciliary body (Figure 1(a) and (b)).

Representative UBM images of SO emulsification. (a) Ghost images (arrowhead), hyperoleon (asterisk), endothelial deposits (arrow), and impregnation of the anterior ciliary body (star). (b) Floating droplets (arrowhead) and impregnation of the anterior chamber angle (arrow), the anterior iris surface (asterisk), and the posterior iris surface (star).
The grade of tissue impregnation and the mean area of hyperoleon were calculated using the method described by Zhao et al. 13 The area of hyperoleon was measured in the central scan using ImageJ software (National Institute of Health, Bethesda, MD, USA). Impregnation of ACA, anterior iris surface, posterior iris surface, and ciliary body was graded as 1 (present) or 0 (not present) on the images acquired in 8 clock-hours. The grades for each sign were summed as the total grade.
Calculation of the number of SO droplets
Then, we measured the number and size of droplets in the first washout fluid with Coulter counter (Multisizer® 3, Beckman Coulter, Brea, CA, USA); in the study, the diameter of the particles ranged from 0.4 to 20 μm. The average value of three consecutive measurements was recorded as the result.
Statistical analysis
Continuous values are presented as the mean ± standard deviation. We used Spearman correlation coefficient and the Mann–Whitney U test to assess the correlations between grade of tissue impregnation/the mean area of hyperoleon and the number of droplets in the washout fluid by SPSS version 20.0 (IBM, Armonk, NY, USA). A P-value < 0.05 was recorded as statistically significant.
Results
Thirty-five eyes in 35 patients (16 right eyes; 19 males) were included in this study, of whom mean age was 55.57 ± 13.65 years. The duration of SO in situ ranged from 14.00 to 103.57 weeks, with an average of 28.06 ± 15.99 weeks. The mean AL was 25.52 ± 2.60 mm (range: 21.61–33.13 mm), with 14 eyes (40.00%) highly myopic (AL ≥ 26 mm). Four eyes (11.43%) suffered ocular trauma before. Following SO removal, lens status (aphakic/phakic/pseudophakic) was 29/3/3, respectivley. BCVA (logarithm of the minimal angle of resolution, logMAR) before SO removal was 1.36 ± 0.78 (range: 0.15–3). And the mean IOP before SO removal was 20.11 ± 7.63 mmHg (range: 12–46 mmHg) (Table 1). There were 18 cases of ocular hypertension (IOP > 21 mmHg or use of antiglaucoma medications), 2 cases of cataract and 3 cases of epiretinal membrane at the time of SO removal.
Patient demographic information and clinical characteristics (N = 35).

Values are expressed as the number of patients/eyes or as mean ± standard deviation (range), as appropriate.
AL: axial length; IOP: intraocular pressure; SO: silicone oil. BCVA :best-corrected visual acuity; logMAR: logarithm of the minimum angle of resolution.
Using UBM, we detected signs of emulsification in all 35 eyes (100%). Among these signs, tissue impregnation and hyperoleon area were quantified. The mean grade of tissue impregnation in the 35 eyes was 22.03 ± 10.24 (range: 0–32). The mean area of hyperoleon was 4.94 ± 5.86 mm2 (range: 0.10–17.78 mm2). The results of the subdivision of the impregnated tissues, including the anterior and posterior iris surface, ciliary body, and ACA, were also analyzed (Supplemental Table S1). Floating droplets, the presence of hyperoleon, endothelial deposits and ghost images were considered qualitative signs. Floating droplets were detected in 35 eyes (100%), hyperoleon in 17 eyes (48.57%), endothelial deposits in 24 eyes (68.57%) and ghost images in 23 eyes (65.71%).
The number of different sizes of emulsified SO droplets in the first washout fluid was successfully assessed. The mean total number of droplets (diameter between 0.4 and 20 μm) was 1.22 ± 0.24 × 107/mL (range: 0.02–12.26 × 107/mL). In particular, the droplets with a diameter between 0.4 and 5 μm were 1.12 ± 2.38 × 107/mL (range: 0.01–12.26 × 107/mL), and those between 5 and 20 μm in diameter were 3.15 ± 2.21 × 104/mL (range: 0.00–7.58 × 104/mL). The number of large droplets (5–20 μm) in the washout fluid was positively correlated with the number of small droplets (0.4–4.9 μm) (P = 0.007).
The grade of tissue impregnation and area of hyperoleon were positively correlated with the number of large droplets (5–20 μm) in the washout fluid (P = 0.048 and P = 0.039, respectively), whereas the correlation with the numbers of total and small droplets (0.4–5 μm) was not significant (Table 2).
Correlation between quantitative signs of SO emulsification observed on UBM and number of emulsified SO droplets counted using Coulter counter.

SO: silicone oil; UBM: ultrasound biomicroscopy; ACA: anterior chamber angle. *P < 0.05 was considered statistically significant.
In addition, there was no significant correlation between the total number and numbers of small or large SO droplets and the presence of ghost images, hyperoleon, floating droplets or endothelial deposits (Table 3).
Correlation between qualitative signs of SO emulsification observed on UBM and number of emulsified SO droplets counted using Coulter counter.
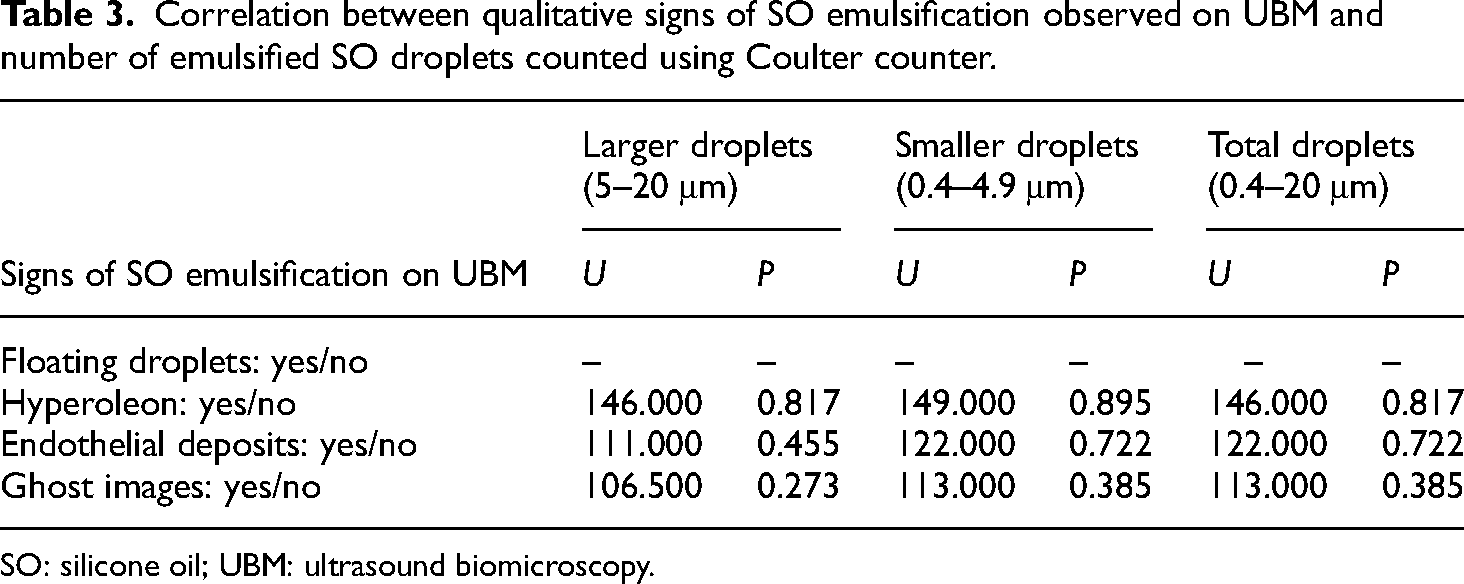
SO: silicone oil; UBM: ultrasound biomicroscopy.
Discussion
This study evaluated different signs of SO emulsification visible on UBM before SO removal, in relation to the number of emulsified SO droplets in the first washout fluid collected during SO removal and measured using Coulter counter. The grade of tissue impregnation and the area of hyperoleon in the AC were correlated with the number of larger (5–20 μm) SO droplets significantly.
UBM presents two main advantages to evaluate SO emulsification compared to alternative methods. Firstly, it is highly cost-effective and noninvasive, in contrast to the Coulter counter. Secondly, UBM can be performed prior to SO removal. In a previous study, 13 we introduced a method for the semi-quantification of the signs of SO emulsification in UBM images, demonstrating high repeatability and reliability. To the best of our knowledge, this study is the first to explore the correlations between UBM signs of SO emulsification and actual SO droplet counts.
The grade of tissue impregnation and the area of hyperoleon in the AC were positively correlated with the number of larger SO droplets (5–20 μm). This result is not surprising; however, the mechanisms underlying the correlation between the impregnation grade and the number of larger droplets, in contrast to the smaller ones, remain to be elucidated. The following factors may account for this discrepancy: first, the UBM resolution is limited, 14 and small droplets may not be detected; second, droplets with a diameter < 5 μm are more easily drained from the eye through the trabecular mesh than the larger ones due to the oval-shaped scleral meshwork, which minor axes is 5 μm. 15 Thus, the between-subject variations in the number of smaller droplets were markedly low. A similar phenomenon was noticed in a previous study, as the number of droplets with a larger diameter (5–12 μm) was negatively correlated with age whereas the number of droplets < 5 μm was not. 10
In contrast, there was no correlation between the size and number of SO droplets and the presence of the UBM signs of ghost images, hyperoleon, floating droplets, or endothelial deposits. Among the UBM findings considered, only the area of hyperoleon and grade of tissue impregnation were quantitative, while the others were qualitative. These quantitative methods allow the systematic measurement of SO emulsification. 16 Only these two quantitative results were found to be correlated with the number of large droplets, suggesting that a quantitative analysis might be superior to a qualitative assessment of SO emulsification within the eye.
Notably, further analysis revealed that the number of large emulsified SO droplets was correlated with the impregnation grade of the anterior and posterior iris surface, whereas the ciliary body or ACA impregnation was not significantly correlated. However, the results may be imprecise; the large surface area of the iris compared to the ciliary body or ACA may be a reason for this discrepancy. Additionally, the iris stroma is a loose connective tissue rich in blood vessels and pigmented cells, possibly promoting the adhesion of SO droplets. 17 Recently, an intraocular emulsion of SO (items) grading system has been published. 18 However, many of these exams such as gonioscopy and ultra-wide-field fundus photography were not routinely used in the clinic, we are unable to analyze the correlation between this grade system and UBM findings. Future study would be carried out to explore this.
In this study, hyperleon was observed in 7 cases using the slit lamp; however, on UBM images, it was observed in 17 cases. Not all instances of hyperleon detected on UBM could be visualized by the slit lamp. The detection range of the machine used in this experiment (Multisizer® 3) was from 0.4 to 20 μm. The size range reported in other studies was slightly different – ranging from 1 to 30 μm in Chan's study 8 and from 1 to 12 μm in Yu's study.9,10 But these studies also confirmed that the majority of emulsified SO particles are within the 1–2 μm size range, comprising over 65% in Chan's study and over 80% in Yu's study. Additionally, most particles were within the 1–7 μm range, accounting for 97% in Chan's study and 98% in Yu's study. So the impact on the overall results should be limited.
Our study was limited by its single center, one surgeon design and limited case number. On the other hand, partly due to the high cost of Coulter counter, a priori sample size and power analysis was not performed. This might affect the generalizability of our findings and highlights the need for larger, well-powered studies to confirm and extend our observations. Further research with larger sample sizes and longitudinal designs is needed to determine how UBM findings could help in the clinical management of patients with SO emulsification after PPV.
Conclusion
In conclusion, the UBM quantitative grade of tissue impregnation and hyperoleon area in the AC could provide a noninvasive overview of the actual degree of SO emulsification before surgery.
Supplemental Material
sj-docx-1-sci-10.1177_00368504241281255 - Supplemental material for Quantitative signs on ultrasound biomicroscopy images associated with the status of silicone oil emulsification within the eye
Supplemental material, sj-docx-1-sci-10.1177_00368504241281255 for Quantitative signs on ultrasound biomicroscopy images associated with the status of silicone oil emulsification within the eye by Hongmei Zhao, Kaicheng Wu, Yuan Zong, Qian Chen and Chunhui Jiang in Science Progress
Supplemental Material
sj-docx-2-sci-10.1177_00368504241281255 - Supplemental material for Quantitative signs on ultrasound biomicroscopy images associated with the status of silicone oil emulsification within the eye
Supplemental material, sj-docx-2-sci-10.1177_00368504241281255 for Quantitative signs on ultrasound biomicroscopy images associated with the status of silicone oil emulsification within the eye by Hongmei Zhao, Kaicheng Wu, Yuan Zong, Qian Chen and Chunhui Jiang in Science Progress
Footnotes
List of abbreviations
Author contributions
All the authors participated in the conceptualization and planning of the study. Hongmei Zhao, Kaicheng Wu and Yuan Zong were responsible for preparing the materials, collecting the data and conducting the analysis. Hongmei Zhao and Kaicheng Wu drafted the original manuscript. Chunhui Jiang did all the surgeries, joined the preparation and the approval of the final manuscript. All authors commented on previous versions of the manuscript. The published version of the manuscript has been reviewed and approved by all authors for publication.
Data availability
The research data used to support the findings of this study are included within the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from ‘Eye and ENT Hospital of Fudan University human research ethics committee (2014026)’.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by National Key R&D Program of China (Grant number 2022YFC2404203); Shanghai Sailing Program, grant/award number: 23YF1445400.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki. Approval from the Eye and ENT Hospital of Fudan University human research ethics committee was obtained prior to commencement of the study (2014026), and all experimental methods were carried out in accordance with the approved guidelines.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.