
Abstract
Background/Objectives:
Neuro-developmental disorders impose a wide range of learning barriers on learners, increasing stress among their teachers. Evidence attests to the heightened stress among teachers teaching children with such conditions. This study tested the efficacy of blended Rational Emotive Behavior Therapy in reducing job stress among teachers of children with neuro-developmental disorders in Abia State, Nigeria.
Method:
The current study adopted a group-randomized waitlist control trial design with pretest, post-test, and follow-up assessments. Participants (N = 83) included teachers of children with neuro-developmental disorders in inclusive and specialized schools. The blended Rational Emotive Behavior Therapy group participated in a 2 h intersession face-to-face and online Rational Emotive Behavior Therapy (REBT) program weekly for 12 weeks. Data were collected using the Single Item Stress Questionnaire, Teachers’ Stress Inventory, and Participants’ Satisfaction questionnaire. The waitlisted group also received a blended Rational Emotive Behavior Therapy intervention after all data collection. Data collected at baseline; post-test as well as follow-up 1 and 2 evaluations were analyzed using mean, standard deviation, t-test statistics, repeated measures analysis of variance, and charts.
Results:
Results revealed that the mean perceived stress, stress symptoms, and the total teachers’ stress score of the blended Rational Emotive Behavior Therapy group at post-test and follow-up assessments reduced significantly, compared to the waitlisted group. Participants also reported a high level of satisfaction with the therapy and procedures.
Conclusion:
From the findings of this study, we conclude that blended Rational Emotive Behaviour Therapy is efficacious in occupational stress management among teachers of children with neuro-developmental disorders.
Keywords
Introduction
Children with neuro-developmental disorders (NDDs) experience multi-dimensional barriers that limit their learning and adaptation.1,2 NDDs are life-long disorders in functioning in cognition, communication, behavior, and motor skills due to impairments in brain development, placing significant limitations in learning and social life.2,3 NDDs are categorized into six classes, which are Autism Spectrum Disorder (ASD), Attention Deficit Hyperactivity Disorder (ADHD), Specific Learning Disorder (SLDs), Communication Disorder, Motor Disorder, and Intellectual Disorder.2,3 Children with diverse NDD classification tend to share some common characteristics, including poor language and communication development, which widely limit their ability to learn at the same pace as typically developing children or those with other types of disorders.1–4 Children living with NDDs also show poor executive functioning, normally linked to their poor communication skills or inability to express their feelings, and/or understand others’ feelings in a normative manner. 2 These, together with the associated learning difficulties in children with NDDs, make it unequally demanding of teachers who teach them, thereby threatening teachers’ mental health.
Teaching children with NDDs presents teachers with unspecified challenges, such as disrupted classrooms, excess workload, inability to accomplish expected learning outcomes, and poor academic performances.2,4 In addition to the regular teachers’ work, teachers of children with NDDs are required to implement curriculum adaptation; individualized education programs (IEPs), and compulsory differentiation.5–8 These generate heightened psychological stress and reduced perception of efficacy. Overall, teachers manifesting elevated levels of stress demonstrate signs of dysfunctional distress, usually symptomatized in high anxiety and low psychological well-being.1–5,9–13 Such teachers also demonstrate decreased job satisfaction, burnout, and overall physical and mental anomalies.1–15 Heightened level of job stress has been found among teachers of children with special education needs, including those teaching children with NDDs.14–17 Such high job stress threatens both the welfare of teachers and the overall development of the learners with NDDs, reducing overall outcomes.15–19
Stress among teachers in this category may arise from negative perceptions and or irrational beliefs/orientations about their teaching experiences and the children they teach,15–19 and/or cognitive appraisal of job performances and outcomes. Such job-related negative cognitive judgment of job experiences that brings unhelpful emotions leading to stress20,21 can be changed using Rational Emotive Behavior Therapy (REBT) to bring about positive outlooks regarding health and occupational outcomes.13,15 In REBT for work stress, the ABCDE model forms the basis on which the counselors and the clients work collaboratively to dispute dysfunctional thoughts and the associated emotions, 22 thereby minimizing symptoms of stress. The ABCDE model is an acronym in which, “A” represents the objective stressor which could be the events associated with working conditions (Activating events); “B” stands for beliefs, cognition, perception, and worldview about the activating event which are either functional or dysfunctional; “C” is the consequence which is the psychological/physical reactions; “D” is disputation which involves challenging irrational, dysfunctional and self-limiting thoughts; and “E” which is effective thoughts.22,23 The ABCDE approach can help workers understand the trajectory of their distress and feelings of stress and guide them to shed off such feelings and adopt a more positive and helpful approach.21,24
Although REBT intervention for workplace stress has recorded a great success among special education teachers,24–26 some beneficiaries of REBT-based treatments tend to report significant symptoms after the face-to-face intervention. 11 Further, the work demand of teachers of children with NDDs makes them highly vulnerable, needing a more innovative intervention approach that could offer additional cost-effective support that is handy, even after face-to-face intervention. Additionally, REBT approaches to psychotherapy are of more clinical benefits and produce better outcomes when face-to-face interventions are blended with online sessions.27–31
Blended Rational Emotive Behavioral Therapy (bREBT) refers to the conjunction of both therapists’ face-to-face sessions and internet-based material in psychotherapeutic interventions. 31 It can be in the form of different permutations of face-to-face and online supports in different therapeutic interventions.28–31 Blended therapy has been suggested to foster therapist–client therapeutic relationships and sustained progress after therapy.31–33 In addition to the traditional face-to-face REBT, bREBT provides the employees with increased access to the complementary support program across time and place. 34 It reduces the cost of clinical visits and increases support-seeking skills in an unspecified environment. 35 Blended therapy is more effective than face-to-face sessions. 34 In this study, bREBT was in the form of face-to-face therapy with inter-session internet-based therapy for stress reduction among teachers of children with NDDs. We, therefore, hypothesize that bREBT will lead to reduced stress among teachers of children with NDDs. It is also expected that reduced stress due to bREBT will be sustained across a 3-month follow-up.
Methods
Ethical consideration. Ethical approval to conduct this study was obtained from the Faculty of Educational Research Committee, University of Nigeria, Nsukka, Nigeria (REC/ED/18/00037). The study also complied with the research ethical standard as specified by the American Psychological Association and World Medical Association. 36 Written informed consents were also obtained from the study participants.
Measures
The Single-Item Stress Questionnaire (SISQ)
This single-item measure of stress symptoms was used as one of the inclusion/exclusion criteria for the study. The instrument has consistently been found valid and reliable in stress research,37,38 showing Cronbach reliability indices ranging from 0.80 to 0.86. The instrument reads: “stress means a situation when a person feels tense, restless, nervous, anxious or unable to sleep at night because his or her mind is troubled all the time. Do you feel that kind of stress these days?” The SISQ is measured on a 5-point scale ranging from 1, ‘not at all’ to 5, ‘very much’. In this study, scores ranging from 1 to 2 indicate low stress; 3 indicate moderate stress; while 4–5 indicate a high stress level. The researcher found a Cronbach Alpha reliability index of 0.79 among 20 adult workers in Nigeria for SISQ.
The Teachers’ Stress Inventory (TSI)
TSI 39 used in this study is a 49-item questionnaire rated on a 5-point Likert scale. Items in the instrument cover 10 subscales, covering two major dimensions of stress (Stress Sources (SS) and Stress Manifestations (SM)). The SS dimension includes 5 subscales including Time Management (TM), Work-related Stressors (WS), Professional Distress (PD), Discipline and Motivation (DM), and Professional Investment (PI). 40 The SM dimension also includes 5 subscales of Emotional Manifestations (EM) (such as anxiety, depression, etc.), Fatigue Manifestations (FM) (e.g. changes in sleep, exhaustion, etc.), Cardiovascular Manifestations (CM) (blood pressure, heart rate, etc.), Gastronomical Manifestations (GM) (stomach pains, cramps, etc.) and Behavioral Manifestations (BM) (use of prescription drugs/alcohol, sick leave, etc.). The TSI has been found with a good psychometric property in the Greek version. 41 We also conducted a reliability test to establish the usability of the instrument in the Nigerian context. In this respect, data collected from 47 teachers in Nigeria were subjected to Cronbach alpha statistic and yielded a good reliability coefficient (α = .81).
The Satisfaction with Therapy and Therapist Scale-Revised (STTS–R):
The STTS–R for group psychotherapy developed by Oei and Shuttlewood 41 was used to ascertain the participants’ satisfaction with the REBT intervention. The STTS–R is a Likert-type scale measured in a 5-point scale of Strongly Disagree (1), Disagree (2), Neutral (3), Agree (4), and Strongly Agree (5). The measure is made up of 13 items, covering the clients’ satisfaction with the therapy, satisfaction with the therapist, and the measure of global improvement on clients’ condition. The STTS–R is of good psychometric property. 42 To validate the usability of the instrument in the Nigerian context, the STTS–R was trial tested on 47 teachers in Nigeria. Cronbach Alpha statistics gave an alpha coefficient, α = .67, suggesting that the instrument was reliable in the Nigerian teachers’ population.
Participants and procedure
A total of 87 teachers who teach children with neuro-developmental disorders: male (n = 29) and female (n = 58) in all the public and private schools for special needs in Abia State, Nigeria, participated in the study. For more demographic information of the participants see Figure 1. Participants were included based on inclusion criteria: (1.) the participant must score up to 3–5 in the Single-Item Measure of Stress Symptoms, showing moderate to high-stress level; (2.) the teacher must have been employed in a Special Education school for not <1 year; (3) the participant must possess personal smartphones with a functional email address and connected to WhatsApp; (4) participant is willing to submit personal contacts and phone numbers; and (v) the teacher signed a written consent that he/she will be available for 2 h a day in a week for the intensive intervention face-to-face and online modules.

Design/Participants' Flow chart.
At the first stage of the sampling (March 2018 to April 2018), the researcher with four trained research assistants visited 28 public and private Special Education schools in Abia State, Nigeria, to notify them of the intervention program. At each visit, they explained the stress associated with work and how it can affect the health of the workers. Also, the bREBT program and how it can be beneficial to them in their work and well-being was explained. Thereafter, the teachers were invited to the screening exercises. A total of 102 teachers volunteered to participate in the program.
The 102 volunteers were screened for eligibility based on the eligibility criteria stated earlier. Consequently, 15 volunteers were excluded based on not meeting the inclusion criteria or other reasons.
The 87 teachers who met all the inclusion criteria were randomly assigned to the bREBT group (44 participants) and the waitlist control group (43 participants) (see Figure 2) using a sequence allocation software (participants were asked to pick 1 envelope containing pressure-sensitive paper labeled with either bREBT or WLG, Waitlist Group) from a container. Information about randomization was concealed from the participants until the intervention was assigned. For good communication about the stages of the intervention, the researcher with the help of two research assistants who are good at managing online platforms opened two WhatsApp chat groups and added the participants according to the groups they were allocated to (one for bREBT and the other for WLG).

Participants demographic information.
Thereafter, the researcher with the help of two research assistants administered a pre-test, TSI to both the REBT group and the waitlist group (WLG) to ascertain the baseline (Time 1) data. Then, the waitlisted participants were informed that they would start their intervention program after the follow-up tests. The researcher with the participants in the bREBT scheduled for commencement of the intervention.
At the fourth stage, participants in the bREBT received inter-session bREBT intervention for a period of 12 weeks (3 months), that is, from February to April 2019. During the 12 weeks, a face-to-face intervention was held for six periods of 2 h in alternated weeks with inter-session 2 h online interventions held in six alternate weeks, giving a total of 12 sessions. To ensure participants’ compliance, the researcher gave financial reinforcement to the participants, covering their transport and data bundle every month to enable them to participate in face-to-face and online sessions. Each session was followed by a practice exercise by the participants.
At the fifth stage, post-test (time 2) data were collected from both bREBT and WLG using TSI. This took place 2 weeks after the last intervention session. Further, follow-up online interactions and the collection of follow-up data (Time 3 and 4) took place at 3 and 6 months after the post-test evaluation. The same instrument (TSI) was used to collect 3 months’ follow-up (Time 3) data and 6 months’ follow-up (Time 4) after the post-test Time 2 (July and October, 2019, respectively for time 3 and Time 4 data collection exercises) (see Figure 2). All the data collection sessions were held via the online platform.
Finally, immediately after the 6 months’ follow-up assessment, the intervention program commenced for the waitlisted group (October–December, 2019). This followed the same procedure used for the bREBT group. The bREBT was delivered and moderated by the researcher, together with four research assistants (two experts in REBT and two occupational therapists who were conversant with online interventions). All the research assistants were paid by the researcher. The researcher sent reminder messages via the WhatsApp platform to the participants a day to each scheduled time, and early morning hours on each face-to-face meeting day to ensure participants’ active participation in the intervention sessions. The online module was also sent to the participants in the early morning of the scheduled day via email and also posted to the group WhatsApp. The participants were expected to complete and submit module exercises, and ask their questions before 10 pm the same day. The researcher also responded to individual queries and needs of the participants via WhatsApp and phone calls continuously. Apart from the baseline evaluations for which the participants completed and submitted questionnaires on the spot, post-test and follow-up assessments were completed via emails. Data collected from the bREBT group at each assessment were compared to that from the WLC group.
Figure 1 shows the demographic information of the participants in the bREBT group and WLG. On the whole, 29 (33.33%) of the participants were males, while 58 (66.66) were females. A total of 15 (17.24) male and 29 (33.33) female participants were in the bREBT while 13 (14.94) male and 30 (30.00) females were in the control group. A total of 11 (12.64%) and 13 (14.94) of the participants in bREBT and Wait-List control (WLC) groups, respectively, had 1–2 years of experience; 19 (21.83) and 17 (19.54) in bREBT and WLG had 3–5 years of experience, while 14 (16.09) and 13 (14.94) also had >5 years of experience in teaching children with special needs. The mean age of the participants was 31.02 and 33.31, respectively, for bREBT and WLG. A total of 49 (56.32%) participants are in primary schools while 38 (43.67%) participants were teaching in secondary schools. A total of 25 (28.73) primary school teachers and 19 (21.83) secondary school teachers were in the bREBT group, while 24 (27.58%) primary school teachers and 19 (21.83%) secondary school teachers were in the WLG group. Considering qualifications, 25 (28.73%) and 26 (29.88%) had NCE in bREBT and WLG, respectively; 18 (20.68%) and 17 (19.54%) participants had a Bachelor’s degree, respectively, in bREBT and WLG; 1 (1.15%) and 0 (0%) had a Master’s degree and above in bREBT and WLG.
Intervention
An REBT program manual2 used in Onyishi, et al. 23 was adopted and blended with an online module and used in the study. The adapted modules utilized the “ABCDE” model (Activating event, Beliefs, Consequences, Disputing, and Effective new philosophy) to change dysfunctional and irrational beliefs associated with work experiences. The major aim of the bREBT was to use an ABCDE face-to-face group therapeutic model combined with the online module in “disputing” – challenging and questioning employees’ work-related irrational and dysfunctional beliefs and replacing them with rather helpful and functional beliefs.20,25,26
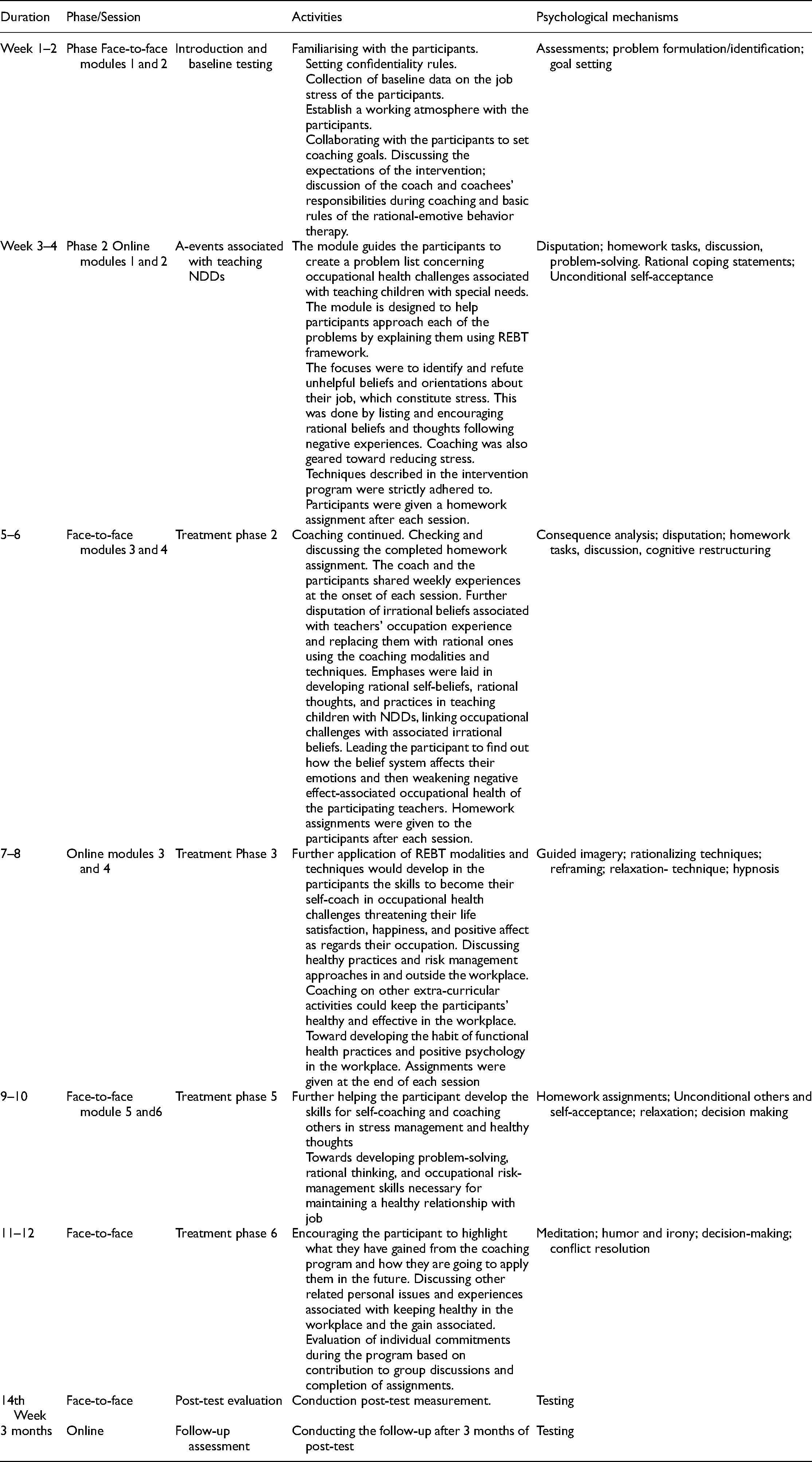
The researcher adopted the ABCDE model in explaining the relationships existing between activating (A) events associated with teaching children with ASD, dysfunctional thoughts, beliefs, or cognitions arising from those events (B); and the emotional and behavioral consequences of the beliefs (C).34,35 Activating event (A) in teaching children with NDDs could be a challenging situation associated with learning difficulties of the children, behavioral problems, extra work-load, and teachers’ personal experiences; the belief (B) is the interpretation and cognitive imagery formed due to “A”. Such cognition about the event (B) elicits a consequence/effect (C) for the teacher, which may be adaptive or maladaptive. The maladaptive consequences may include anxiety, depression, and stress symptomatology. Then, disputation techniques (D) are used to eliminate the maladaptive, dysfunctional, and self-limiting beliefs and cognitions.43–45 Disputation involves challenging and comparing the maladaptive thoughts with more adaptive ones. According to Ellis, 6 the best way to counter irrational beliefs is by considering realistic and logical ones. Hence, as participants become aware of and counteract their dysfunctional beliefs, they come up with more effective worldviews (E). bREBT uses strategies, including disputation, homework tasks, discussion, and role-play together with cognitive, behavioral, and emotional techniques to help participants to change negative perceptions, navigate unhelpful emotions, and reduce stress.15,23,25,26 This ABCDE model as used in the earlier study by the first author formed the basis of activities throughout the intervention (See Table 1).
Summary of the blended rational emotive behavour therapy program.
The internet component of therapy is made accessible in mobile apps to enable clients to engage in therapy and complete homework tasks in therapists’ absence and increase participants’ compliance to intervention. Hence, in bREBT we designed a face-to-face combined with inter-session internet-based therapy in 12 modules (six face-to-face modules were delivered in alternate sessions with six internet-based modules). Each of the modules includes information, exercises, worksheets, images, examples, homework exercises, and a template for progress feedback. Additional audio and video files are also in the internet-based sessions.
Recruitment, response rates, dropouts, and adherence
Before recruitment, we obtained informed consent from all potential participants. A total of 102 potential participants responded to the invitation to participate in the study out of which 87 participants were included in the study. Others were excluded based on not meeting the inclusion criteria. The entire 87 participants who were randomized for the study completed the sessions and evaluations. However, during the last phase of the research, which was an intervention for the waitlisted group, two participants did not respond to the invitation to participate. The researchers communicated through e-mail and WhatsApp, but they did not reply. So, there was a high adherence rate in this study. Generally, the participants responded to both face-to-face and online contacts with few delay cases, which were subsequently covered.
Design and data analyses
The current study adopted a group-randomized waitlist control trial design with pretest, post-test, and follow-up assessments. 46 This design guided the researcher to assess the effectiveness of bREBT intervention on job stress. Participants were randomized into bREBT and waitlist groups. Baseline data were analyzed using t-test statistics. A two-way analysis of variance (ANOVA) with repeated measures was used to compare baseline, post-intervention, and follow-up 1 and 2 data. Partial Eta squared was used to report the effect size of the intervention on the dependent measure (TSI).
A paired sample t-test was used to determine the difference in participants’ ratings across Time 1and 2; Time 2 and 3; as well as Time 3 and 4. Further, 2 × 3 analysis of variance (ANOVA) statistics was conducted to find out the interaction effects of group × Time on the study SS, SM, and TSI. The percentage was used to analyze the participants’ satisfaction with therapy. Statistical Package for Social Sciences (SPSS) version 24.0 and Microsoft Excel were used for analyses. Results are presents in tables and charts.
Results
Table 2 showed a non-significant difference in the mean stress sources (SS) scores of the bREBT group and waitlist group (WLG) at Time 1, t = 1.80, p = .993. This suggests that participants in both REBT group and WLG had equally high sources of job-demands perception (bREBT group = 3.54 ± .42; WLC = 3.38 ± .42). Both bREBT group (3.50 ± .52) and WLG (3.49 ± .66) did not vary significantly in their Stress Manifestation scores at baseline, t (85) = 2.28, p = .120. On the whole, participants in both bREBT and WLC groups did not vary significantly in their total TSI rating. A non-significant difference was also recorded (t (85) = 2.16, p = .492) for the bREBT group (3.52 ± .45) and WLG (3.41 ± 51) in their TSI scores at baseline data. Mean scores of the two groups indicated the participants in both groups not only perceived their jobs as stressful but also experience symptoms associated with stress.
t-test analysis of the baseline data on participants’ Teachers’ Stress Inventory dimensions.

SS: Stress Sources; SM: Stress Manifestation; TTSIS: Total Teachers’ Stress Inventory Score;
Data in Table 3 shows the repeated measures ANOVA of the effect of the bREBT on participant post-test, follow-up 1, and follow-up 2 ratings in SS, SM, and TTSI. The results revealed significant main effects of bREBT on stress sources, at Time 2, 3, and 4 (post-treatment) evaluations. Participants in the bREBT group (1.91 ± .96) had significantly (F (1, 84) = 106.69, p = .000, ŋ2 = .56) lower mean score than WLG (3.59 ± .43) at Time 2 as measured by SS. There is a significant difference, F (1, 84) = 77.22, p = .000, ŋ2 = .47 in the mean rating of participants in bREBT (1.97 ± 1.11) and WLG (3.58 ± .43) as measured by SS at Time 3 evaluation. At follow-up 2 (Time 4), a significant difference, F (1, 84) = 291.74, p = .000, ŋ2 = .77 was also shown in the mean rating of participants in the bREBT group (1.74 ± .58) and WLG (3.61 ± .38) as measured by SS. These indicated that reduced perception of stress sources among beneficiaries of bREBT was sustained across the times of 2 follow-up evaluations at 3 and 6 months, respectively.
Repeated measure analysis of variance of the effectiveness of the REBT intervention on post-test, follow-up 1 and follow-up 2 scores of participants’ on TSI.

SS: Stress Sources; SM: Stress Manifestation; TTSIS: Total Teachers’ Stress Inventory Score;
The mean rating of the bREBT group on stress manifestation (1.30 ± .28) reduced significantly (F (1, 84) = 633.03, p = .000, ŋ2 = .88), compared to WLG (3.56 ± .46) during Time 2 measurement. This reduction in SM was sustained as there was still significant differences in the SM scores of the two groups at follow-up 1 (F (1, 84) = 478.89, p = .000, ŋ2 = .85) and follow-up 2 (F (1, 84) = 180.94, p = .000, ŋ2 = .69). This implies that bREBT could reduce the negative perception of occupational stress as well as stress symptoms of the participants.
Considering the total score of data from the TSI at post-test (Time 1), the bREBT group showed lower mean rating (1.65 ± .52) than the waitlist group (3.58 ± .44), which was significant (F (1, 84) = 327.02, p = .000, ŋ2 = .79). At follow-up 1 (Time 3) TSI mean rating of the REBT group (1.78 ± .63) was lower compared to the WLG (3.57 ± .44). This difference was significant (F (1, 84) = 224.60, p = .000, ŋ2 = .72). Also, a significant difference (F (1, 84) = 240.00, p = .000, ŋ2 = .71) in TSI ratings of the bREBT group (19.61 ± 6.87) and WLG (43.13 ± 10.87) was recorded at follow-up 2 (Time 3). Also, a significant difference (F (1, 21) = 31.26, p = .000, ŋ2 = .81) was recorded in the mean Stress Sources (SSS) ratings of the bREBT group (1.86 ± .56) and WLG (3.57 ± .43).
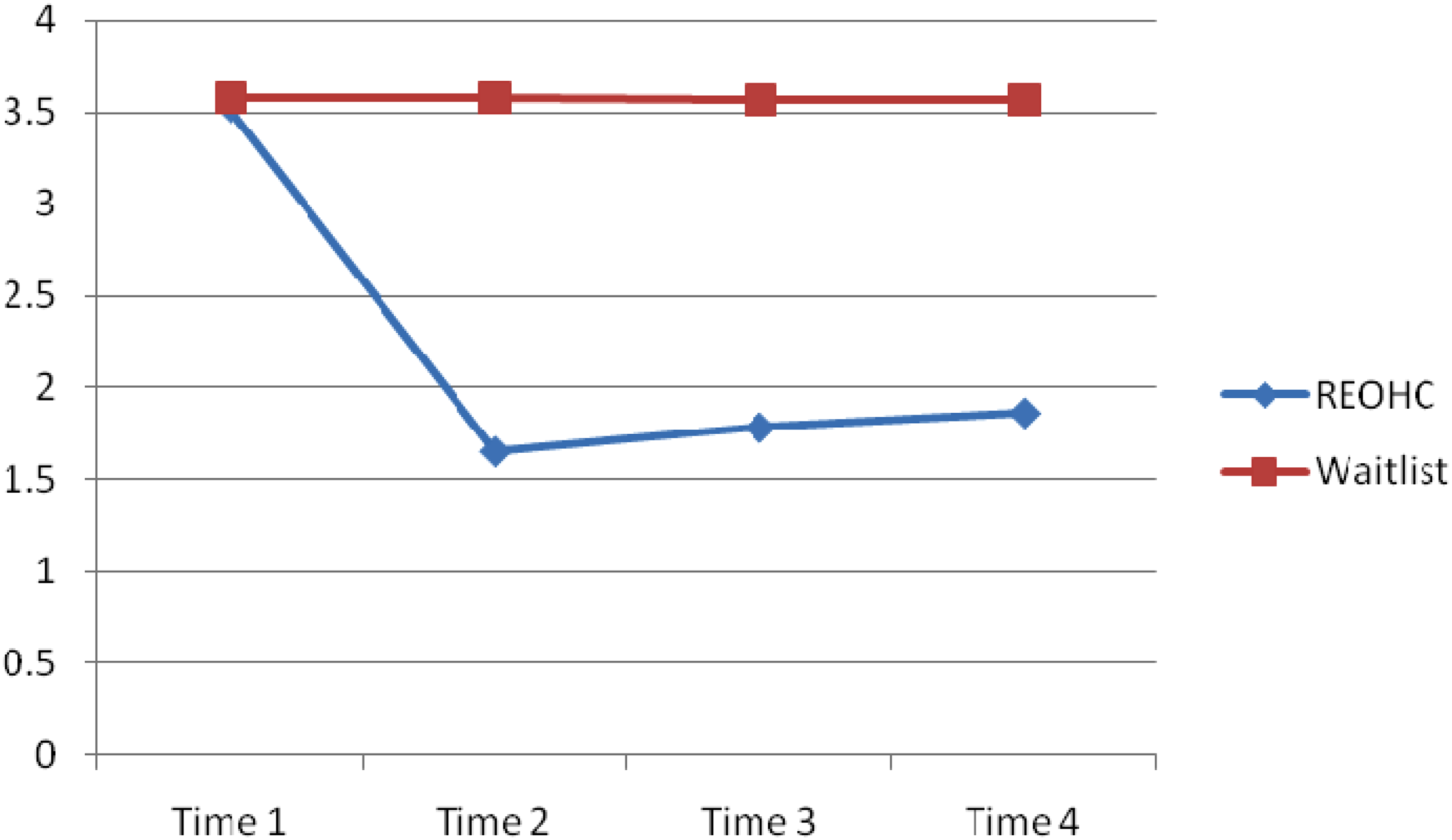
An independent sample t-test was conducted to explore changes in the measures across pre, post and follow-up 1 and 2 scores in bREBT and WLC groups. The main effects of Time (baseline data, post-test, follow-up 1 and follow-up 2) were significant with respect to the SS, F (82) = 278.88, p = .000, ŋ2 = .78 (See Figure 1), SM, F (2, 82) = 244.15, p = .000, ŋ2 = .90 (Figure 3), and TSI scores F (2, 82) = 256.00, p = .000, ŋ2 = .82 (Figure 3).

Interaction effect of time and intervention on participants’ Stress Sources scores.
The bREBT group recorded a significant decreases in SS scores between Time 1 and 2 (t (86) = 5.501, p = .000, CI = .45,.98) and non-significant differences in Time 2 and 3 (t (86) = −.270, p = .78, CI = −.23, −.18), and Time 3 and 4 (t (86) = 1.126, p = .263, CI = .097, −.084) scores. However, the WLC group did not have significant change across Time 1–2 (t (86) = −.311, p = .631, CI = −.35, -.09)); 2–3 (t (86) = −.167, p = .319, CI = .085, −.073); and 3–4 (t (86) = 1.300, p = .311, CI = .071, −.067). This indicates that the reduction in bREBT group's SS score from pre-test to post-test was sustained through 3 and 6 months’ follow-up (See Figure 3)

Interaction effect of time and intervention on participants’ Stress Manifestation scores.
In respect of SM, there was also significant reduction in SM scores across Time 1 and 2 (t (86) = 5.81, p = .000, CI = .58, 1.20) but non-significant differences in Time 2 and 3 (t (86) = −3.09, p = .312, CI = −.16, −.03); and Time 3 and Time 4 (t (66) = −4.27, p = .567, CI = −.27, −.09) in the bREBT group. On the contrary, participants in the WLC group did not vary significantly in their SM scores across Time 1–2 (t (86) = −4.01, p = .301, CI = −.17, −.04); 2–3 (t (86) = −1.99, p = .193, CI = −.17, −.27); and 3–4 (t (86) = −6.27, p = .873, CI = −.39, −.07). This suggests that the reduced SM at post-test was a product of interaction effect of the coaching intervention and was sustained across 3 and 6 months’ follow-up (See Figure 4).
Participants also had significant reduction in overall TSI scores across Time 1 and 2 (t (86) = 5.95, p = .000, CI = .53, 1.07); but not significant across Time 2–3 (t (86) = −1.08, p = .280, CI = −.18, −.05) and Time 3–Time 4 (t (86) = −.624, p = .534, CI = −.15,.08). However, participants in the WLC group did not record significant changes in their TSI scores across Time 1–2 (t (86) = −2.17, p = .313, CI = −.17, −.02); Time 2–3 (t (86) = −2.09, p = .550, CI = −.18, −.02); and Time 3–4 (t (86) = −4.12, p = .614, CI = −.19, −.07) (See Figure 5).
Interaction effect of time and intervention on participants’ Teachers’ Stress InventoryTSI scores
To further validate the efficacy of the bREBT on participants’ emotions, we collected data on the participants’ satisfaction with the therapy. Data collected in this respect are presented in Table 4 and Figure 5. Data in Table 4 show the participants’ satisfaction with the bREBT intervention program. The majority of the participants (81 (93.1%)) reported a high degree of satisfaction with the quality of the therapy received. A total of 76 (87%) reported a high degree of satisfaction with the therapists and 68 (78.2%) scored high in their global improvement with the bREBT intervention.
Frequency and percentage of participants satisfaction with therapy.

The majority of the participants (75 (86.2%)) were highly satisfied with the bREBT program as measured by the Overall STTS–R score. These attest to the efficacy of bREBT on teachers’ stress management.
Discussion
The current study sought to validate the effectiveness of bREBT in reducing job- stress among teachers of children with special needs. Results showed that bREBT and WLG groups did not vary significantly in their SS, SM and the Total Teachers’ Stress Inventory (TTSI) scores at baseline evaluation. The bREBT intervention led to a significant reduction in all dimensions of teachers’ stress (SS, SM, and TTSI) of the bREBT group at Time 2 (post-test), which were sustained through Time 3 (follow-up 1) and Time 4 (follow-up 1) compared to the WCG. The results further indicated significant interaction effects of Time and Intervention on the measures of participants' stress. This affirms that the reduction in the stress scores of the bREBT at posttest and follow up were due to the bREBT intervention. While stress scores of the WLG did not vary significantly across baseline, post-intervention, and follow-up evaluations, the bREBT group reported a significant reduction in their stress between baseline and post-treatment evaluations. Further results show high participant satisfaction with the bREBT intervention. About 93% of the bREBT participants reported their high satisfaction with therapy, 87.4% reported high satisfaction with the therapists and 78.2% reported satisfactory Global improvement in their stress conditions. This indicates that bREBT alters the participants’ self-defeating cognitions associated with the work experiences.
The significant reduction in the teachers’ stress through bREBT shows that even when the objective working conditions (stress sources) remain constant, a teacher through bREBT can change his/her perceptions about stressful experiences associated with teaching children with NDDs, leading to reduced stress symptoms. Findings from earlier studies have also noted the ability of internet-based programs to sustain treatment benefits post-discharge from face-to-face treatment. 47 In addition, Kenter, van de Ven, Cuijpers, Koole, Niamat, Gerrits, … and van Straten 47 concluded in their study that blended care is more expensive than established face-to-face treatments and does not lead to additional benefits in terms of general functioning.
Going by the three models of stress-stimulus-based, response-based, and transaction-based models,47–50 it is expected that the three models could be explained using the ABCDE therapeutic modalities, thereby bringing about relief on the part of the teachers. The stimulus-based model of stress proposes that stress occurs when there is an objective activating event (A), called stressor; On the other hand, the response-based model suggests that stress prompts emotional, physiological, and behavioral reactions (C) towards the stressor (A). Finally, transaction-based model suggests that stress is a consequence (C) of the negative subjective interpretation/cognitions perspective (B) of activating situation/stress (A).15,40,49–51 Thus, bREBT works by disputing (D) the negative and dysfunctional perception ‘B’ about the stressful situation ‘A’ and replacing them with the healthier ones (E).
This could cause a significant reduction in the cognitive physical and/or emotional impacts on health and well-being (C).22–27 bREBT helps the clients to develop self-evaluation strategies that equip them to understand their thoughts to deal positively with them. So, as the participants continue to apply these skills, they tend to continue to acquire more expertise in stress management and how stressful they view their jobs. 13 Thus, supporting works on REBT,15,45,47–49 this work shows that blended modality (bREBT) is successful in reducing occupational stress and other psychological disorders among teachers of children with NDDs.
Considering how the intervention may be effective in ameliorating the subscales of teachers’ stress inventory (TSI), which are stress sources (SS), stress manifestation (SM), and total TSI score, intervention may take multiple mechanisms for stress reduction. For instance, intervention may not act on the stress sources (SS), as they are the objective stressors that trigger stress reactions.15,45,46 However, research has shown that as perception changes through bREBT intervention, stress manifestations/symptoms are minimized and the stress sources become rather less harmful.49,50 However, through bREBT, teachers can learn practical ways to deal with some sources of stress through proactive management behaviors, thereby reducing the stress sources (SS)/stressors.50,52 When it is not possible to control the objective stress sources bREBT can assist clients to shake off the symptomatic manifestations of stress (SM), thereby minimizing the TSI score53–55 by building a new perspective about their situation. Hence, the outcome of this study support previous findings showing that interventions are effective in helping teachers regain control over stressors, reduce the intense psychosomatic symptoms and use effective strategies for dealing with stressful situations associated with teaching.15,40,45,46,49–55
Consequently, an earlier study 56 showed that a positive change in perception of stress can lead to a reduction in physiological and psychological symptoms associated with job stress. This is well conventional in the bREBT viewpoint, which works through opposing negative thoughts, feelings, emotions associated with stressors (occupational environments) and replacing them with more helpful ones. Other Nigerian studies showed that REBT was effective in stress management13,25 and improving subjective well-being 23 of employees. However, to the best of our knowledge, the finding of the current study is a new finding that has not been observed previously, given that all previous studies on REBT are face-to-face. None of the stated works on REBT was blended with online treatment sessions. Hence, the present findings serve as the base for further studies, and researchers are encouraged to replicate and confirm in other studies using a blended treatment format. Results of the present study also strengthen other studies on blended approaches using other psychotherapeutic modalities such as cognitive behavioral therapy (CBT)/ rational emotive behavior therapy (REBT)27,30–35,47,57–60 which have yielded positive results.
A high participant satisfaction with the bREBT intervention was recorded in the study. Few studies have assessed satisfaction with blended treatments for psychological disorders, in respect of treatment preferences, expectations, usability, and satisfaction.61–64 Simon, Leah McGillivray, Neil Roberts, Kali Barawi, Catrin Lewis andBisson 64 based on a review of empirical studies found internet-based CBT to be acceptable to participants. Other studies27,60–64 found a high degree of satisfaction with the therapy and study procedures. In blended therapy, online sessions offer participants unrestricted access to treatment materials and exercises at the comfort of their own home thereby reducing the cost and frequency of meetings.63,64 Additionally, blended therapy reduces therapist time compared to only face-to-face sessions, yet offers the benefit of face-to-face therapeutic relationships, which is very necessary for psychotherapy. 47
Reducing workplace stress reduces psychopathological symptoms such as headache, anxiety, and musculoskeletal problems14,15,51 that could undermine employees’ effectiveness. As such reduction of stress in teachers could reduce negative health conditions and increase their classroom effectiveness.40,65,66 The improvement in teachers’ effectiveness translates to positive outcomes in children with special needs kept under their care. Furthermore, negative thoughts and emotional stress reactions tend to reduced productivity and increase health challenges.17,67–70 Additionally, bREBT is a cost-effective scheme improving teachers’ well-being and positive outcomes in students with NDDs.47,57
Limitations of the study
Due to the relatively small sample used in this study, the outcome cannot be generalized outside the context. Further study could apply a larger sample to confirm the effectiveness of the bREBT. The package (bREBT) may also be tried in different populations of employees with chronic stress. The present study did not compare blended with face-to-face REBT. Information about the relative efficacy is needed for future decision-making about the best approach. Future studies may be designed to compare bent and traditional face-to-face REBT as the current study did not consider the area.
Practical implications
Coaching practitioners working with teachers can consider bREBT in managing stress for intervention needful for teachers of children with NDDs. Experts in school occupational health and behavioral coaching should adopt bREBT in handling teachers of special needs learners who have moderate and/or severe stress associated with their work.
Conclusion
From the findings of this study, we conclude that blended REBT is efficacious in stress management among teachers of children with NDDs. We further conclude that the clients who receive bREBT are satisfied with the intervention. The bREBT is cost and time-effective and could be utilized across contexts.
Footnotes
Acknowledgements
All the authors were involved in writing and conducting the research. The author wish to thank the research assistants and therapists who aided the research processes. Thanks to our participants and the analyst for assisting in the completion of this study.
Data Accessibility statement
Data pertaining to this study were not deposited in any repository, but can be accessed from the corresponding author on reasonable demand.
Declaration of conflicting interests
The authors declared no existing, or potential potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.