
Abstract
A comparative case study (2017–2020) was conducted to identify demographic, social, medico-legal, and toxicological variables associated with non-fatal accidents in driving under the influence (DUI) subjects. A second aim was to identify the factors predictive of substance use disorders among subjects. Drivers charged with alcohol DUI (blood alcohol concentration (BAC) > 0.5) and/or psychoactive substance DUI were included; cases included those involved in an accident while intoxicated, and the comparison group included DUI offenders negative for road accident involvement. Significance was determined by chi-square and Mann–Whitney tests. To prevent confounding effects, a multivariate binary logistic regression analysis was performed. Our sample encompassed 882 subjects (381 in the case group and 501 in the comparison group). Parameters such as psychoactive substances and BAC at the time of the road crash/DUI and the day of the week, when subjects were involved in the road accident or found DUI, resulted in significant differences (p < 0.01) between groups. The model’s independent variables of BAC > 1.5 g/L (p = 0.013), BAC > 2.5 g/L (p < 0.001), and concurrent alcohol and psychoactive substance use (p < 0.001) were independent risk factors for an accident. Smoking >20 cigarettes/day was an independent risk factor for unfitness to drive (p < 0.01). Unfitness to drive was based primarily on ethyl glucuronide levels >30 pg/mg. Our results suggest a detailed assessment of DUI subjects with variables associated with accidents (BAC > 1.5 g/L and concurrent intake of psychoactive substances). Hair analysis, including ethylglucuronide (EtG) concentration, should be always performed. Based on our results, nicotine use should be investigated in cases of driving license regranting.
Keywords
Introduction
Human, vehicle, or infrastructure factors can cause single- or multi-vehicle road accidents. 1 One of the primary contributory factors to fatal road accidents is driving under the influence (DUI) of psychoactive substances, including alcohol, 1 which causes thousands of traffic deaths worldwide each year. 2
Both proactive and reactive strategies have been adopted to prevent road accidents and the deaths or injuries of any people involved. Proactive strategies include awareness campaigns about the risks of road accidents in a state of intoxication, the promulgation of severe laws with legal limits for DUI, heavy fines, license suspension, and jail time. 3 Reactive strategies have included diagnostic strategies highlighting the risk factors, which are conducted during driver’s license issuing or regranting; demographic and social characteristics; medico-legal data 4 ; and laboratory results associated with substance-related disorders and, thus, a higher risk of driving while intoxicated. Diagnostic strategies with the identification of a risk profile must be followed by therapeutic approaches that are differentiated according to the identified risk factors. 3
Several risk factors associated with road crashes have been investigated in the literature. The age of the driver was studied in relation to road accidents in subjects in a state of intoxication, usually with evidence of an association with the young age.2,5 However, these data are more complex than they seem at first glance and should be analyzed considering the presence of psychoactive substances other than alcohol. 6
The timing of a road accident is another widely studied factor. 5 Studies addressing this issue have highlighted different results concerning the time of occurrence 6 of accidents among subjects using alcohol, drugs, or alcohol combined with other drugs. Psychoactive substances, whether prescribed or illegal, are a relevant risk factor for alcohol-related car crash. 1 The timing of road accidents might also be related to the day of the week as a consequence of different profiles of psychoactive substance intake. Substance use disorder according to the Diagnostic and Statistical Manual of Mental Disorders, fifth Edition 7 (DSM-5), binge drinking, and occasional consumption may cause intoxication and occur on different days of the week or periods of the year.
Substance use disorder, an acknowledged risk factor for traffic accidents, is defined in the DSM-5 as “a cluster of cognitive, behavioral, and physiological symptoms indicating that the individual continues using the substance despite significant substance-related problems.” 7 The diagnosis is based on the verification of the DSM-5 diagnostic criteria by means of an interview, objective examination, and laboratory tests. In particular, laboratory tests can be useful for verifying or excluding a lack of control over the consumption of a substance, with excessive intake or an inability to stop taking the substance. An analysis of keratin matrices is also important for integrating the available clinical data. A particular marker that is useful for monitoring abstention from alcoholic beverages or excessive alcohol consumption is ethyl glucuronide (EtG). According to the World Health Organization (WHO), “Chronic excessive alcohol drinking corresponds to an average consumption of 60 g or more of pure ethanol per day over several months.”8,9
Blood alcohol concentration (BAC) is another factor studied concerning road accidents that consistently shows a positive correlation with alcohol-related altercations. 5 Some individuals, regardless of treatment for a substance use disorder, may be at risk for increased road accidents. This group is represented by those who relapse into driving while in a state of intoxication. 10 Certain demographic characteristics such as low education, low income, unemployment, divorce, separation, and widowhood have been associated with DUI recidivism 3 and, thus, with a higher risk of road accidents.
The main aim of the study was to analyze demographic, social, medico-legal (circumstantial), and toxicological variables in DUI subjects involved in non-fatal road accidents and examined for driving license regranting. We also assessed the predictive factors of substance use disorder in the same population. Our findings could lead to a refinement in the judgments of fitness or unfitness to drive and to possible public health implications.
Materials and methods
Data source
The study was conducted on DUI offenders who came from the Veneto Region, Northern Italy, and were examined in the period 2017–2020 at the Unit of Legal Medicine and Toxicology, University of Padova. According to Italian legislation, DUI offenders must be examined prior to restoring their driving privileges. Examinations are performed by units with expertise in legal medicine and/or forensic toxicology in Italian territory.
Study population
Our study population comprised subjects with an alcohol-related DUI according to Italian legislation, where the BAC limit is 0.5 g/dL. Drivers who tested positive for illicit psychoactive substances were also included in the study.
The period considered was 2017–2020. Inclusion criteria for the study were as follows: subjects found guilty of DUI, and between the ages of 18 and 65 years old; and subjects had to be assessed in our unit by toxicological analysis of hair samples for alcohol and other psychoactive substances. The exclusion criteria, chosen to reduce confounding factors, included meeting the Diagnostic and Statistical Manual of Mental disorders 5 (DSM-5) criteria (APA 2013) for psychiatric disorders (e.g. major depression and psychosis), neurological (e.g. Parkinson’s disease, neurocognitive disorders), and medical disorders, aged younger than 18, and aged older than 65. A prescription for psychopharmacological therapy was also an exclusion criterion.
The examination was carried out by medico-legal staff through an integrated methodological approach based on phases used to evaluate fitness/unfitness to drive and included the following: (1) demographic data collection (age at DUI); (2) analysis of documentation regarding the DUI episode (BAC, presence of psychoactive substances other than alcohol, day of the accident) and the alteration of specific blood markers of chronic alcohol intake; (3) direct examination, including anamnestic data and objective examination; and (4) toxicological analysis of the proximal head hair segment with a length between 3 and 6 cm, which were also evaluated, by means of EtG levels in the hair. The examined subjects were considered either fit or unfit to drive based on the integrated evaluation of the results of this methodological approach. In particular, excessive alcohol intake, according to the Society of hair testing (SOHT) consensus document (EtG > 30 pg/mg; SOHT 2019), was considered cause for determining unfitness to drive; the finding of illicit psychoactive substances in hair samples was another cause for the determination of unfitness to drive.
Variables
The research was structured as a comparative case study for the period 2017–2020. Participants were then subdivided into two groups according to their involvement in a road accident. Group 1, cases, were DUI subjects involved in a road accident. Group 2, the comparison group, included DUI offenders found during a police patrol and not by involvement in an accident.
The two groups were analyzed based on their personal data, including age at DUI and tobacco use; socioeconomic conditions, encompassing education, employment situation, and marital status; parameters linked to DUI, including BAC, concurrent substance use other than alcohol at the time of the DUI, and the timing (day of the week) of the DUI; toxicological data, including hair analyses; and lastly, the judgment of fitness/unfitness to drive. For the BAC parameter, we decided to identify four ranges of values to which the subjects of our population were assigned. Specifically, the four BAC range were 0.5–0.8, 0.8–1.5, 1.5–2.5, and >2.5 g/L. We also reported ranges of EtG values to which the subject of our population were assigned. The ranges <5 pg/mg, 6–29 pg/mg, and ≥30 pg/mg, were chosen according to the Society of hair testing (SOHT) consensus document. Psychoactive substances at the moment of the road accident/DUI and detected during a medico-legal assessment of both groups were also assessed.
Analysis
The anonymized data were entered into an Excel spreadsheet, and descriptive analyses were conducted for the two groups. We analyzed possible associations with road accidents using chi-square and Mann–Whitney tests for dichotomous or continuous variables, respectively. Variables with a p-value <0.2 were entered into a multivariate logistic regression model exploring possible predictors of road traffic crashes.
To explore the characteristics of the subjects involved in a road accident, we analyzed these drivers with respect to factors possibly predictive of a judgment of unfitness to drive. Multivariate logistic regression was also used to test predictors of unfitness to drive in these cases and in comparison subjects.
All of the analyses were performed with IBM SPSS Statistics 25.0 for Windows, Version 25.0 (Armonk, NY).
All procedures of the present study were conducted in accordance with the Declaration of Helsinki of 1975, as revised in 1983.
Additional references can be found in the bibliography in the Supplemental Appendix.
Results
The study included 882 male subjects. The number of cases in Group 1 was 381 (43.19% of the total), and the number of subjects in Group 2 was 501 (56.81% of the total). Personal data, socioeconomic factors, DUI variables, toxicological analyses, and judgment of fitness/unfitness to drive, both overall and relative to the comparison subjects, are provided in Tables 1 and 2. The majority of the subjects included in the study were found to be driving under the influence of alcohol (more than 90%); notably, 36.85% of the cases resulted in a judgment of unfit to drive after the medico-legal toxicological assessment (23.69% for excessive alcohol consumption, 4.3% for excessive alcohol consumption associated with illicit substance use, and 8.84% for illicit substance use).
Personal data and socio-economic factors, in cases and comparison subjects.

p-Value refer to chi-square test for dichotomous variables and to Mann-Whitney test for continuous data with non-parametric distribution.
Data may be incomplete for some subjects. The sum of the numbers and of the percentages with reference to the variable considered may not correspond to the total or to 100%.
Conditions at DUI, toxicological analysis, and judgment of fitness/unfitness to drive in cases and comparison subjects.
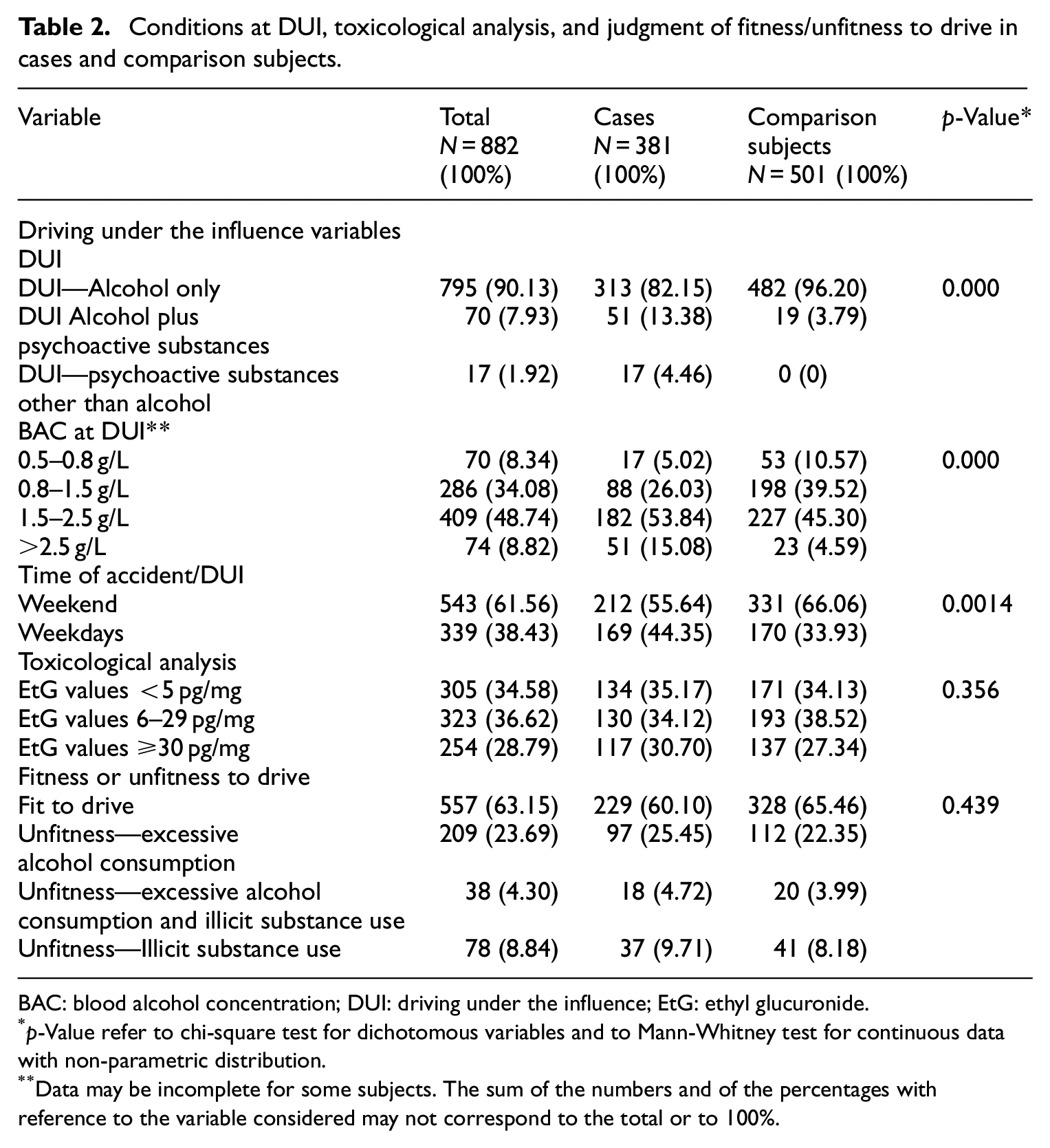
BAC: blood alcohol concentration; DUI: driving under the influence; EtG: ethyl glucuronide.
p-Value refer to chi-square test for dichotomous variables and to Mann-Whitney test for continuous data with non-parametric distribution.
Data may be incomplete for some subjects. The sum of the numbers and of the percentages with reference to the variable considered may not correspond to the total or to 100%.
The distribution of the parameters of being found to have used psychoactive substances at the moment of the accident/DUI, BAC, and the timing of the road accident/DUI was statistically different between the two groups (p < 0.01). A DUI for alcohol associated with other psychoactive substances or a DUI for psychoactive substances other than alcohol were significantly associated with road accident involvement (p < 0.01). A BAC lower than 1.5 g/L was associated with a lowered probability of belonging to Group 1 (odds ratio (OR), 0.481; confidence interval (CI), 0.361–0.640; p < 0.01).
In our sample, the distribution with regard to the time of the road accident/DUI differed between the cases and the comparison subjects (p < 0.01).
We further analyzed the type of psychoactive substances that had been used at the moment of DUI and the substances found during the medico-legal evaluation (Tables 3 and 4, respectively). Cocaine and cannabinoids were found in more than 70% of the cases involving substance use (exclusively or in combination with alcohol).
Psychoactive substances at the moment of the accident/DUI.

DUI: driving under the influence.
p-Value refer to chi-square test.
Psychoactive substances detected during medico-legal ascertainment.
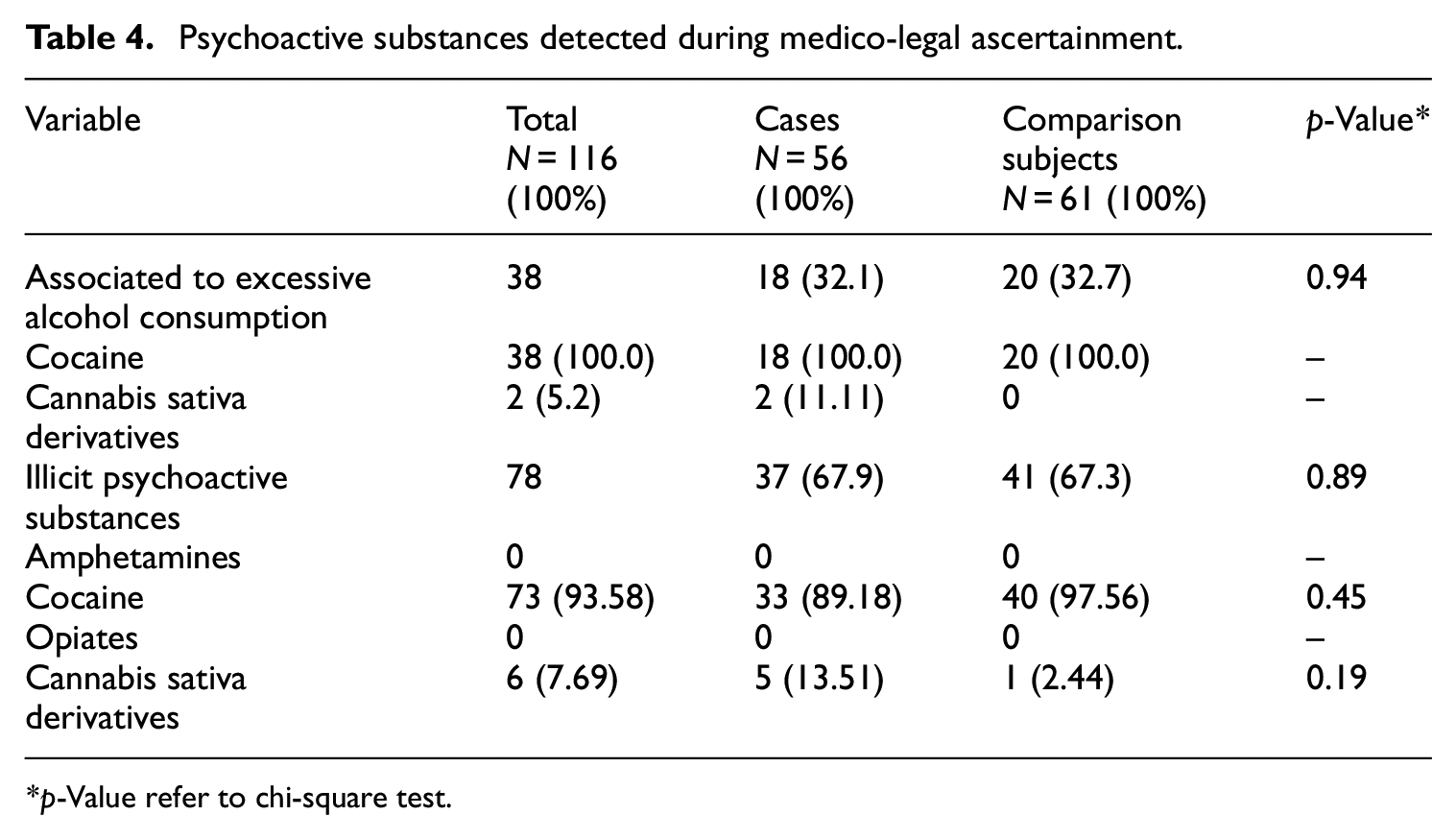
p-Value refer to chi-square test.
In a model including the independent variables BAC and psychoactive substances other than alcohol at DUI, the variables of BAC > 1.5 g/L (p = 0.013), BAC > 2.5 g/L (p < 0.001), and alcohol in combination with psychoactive substances (p < 0.001) were found to be independent risk factors for road accident involvement (Table 5). Given that all the subjects found guilty of DUI of psychoactive substances other than alcohol were involved in a road accident, they were excluded from the binary regression analysis. The time of road accident/DUI was also not included in the binary regression analysis because this parameter was influenced by the timing of police patrols, which was concentrated on weekends.
Predictors of road traffic crash using a multiple logistic regression model.
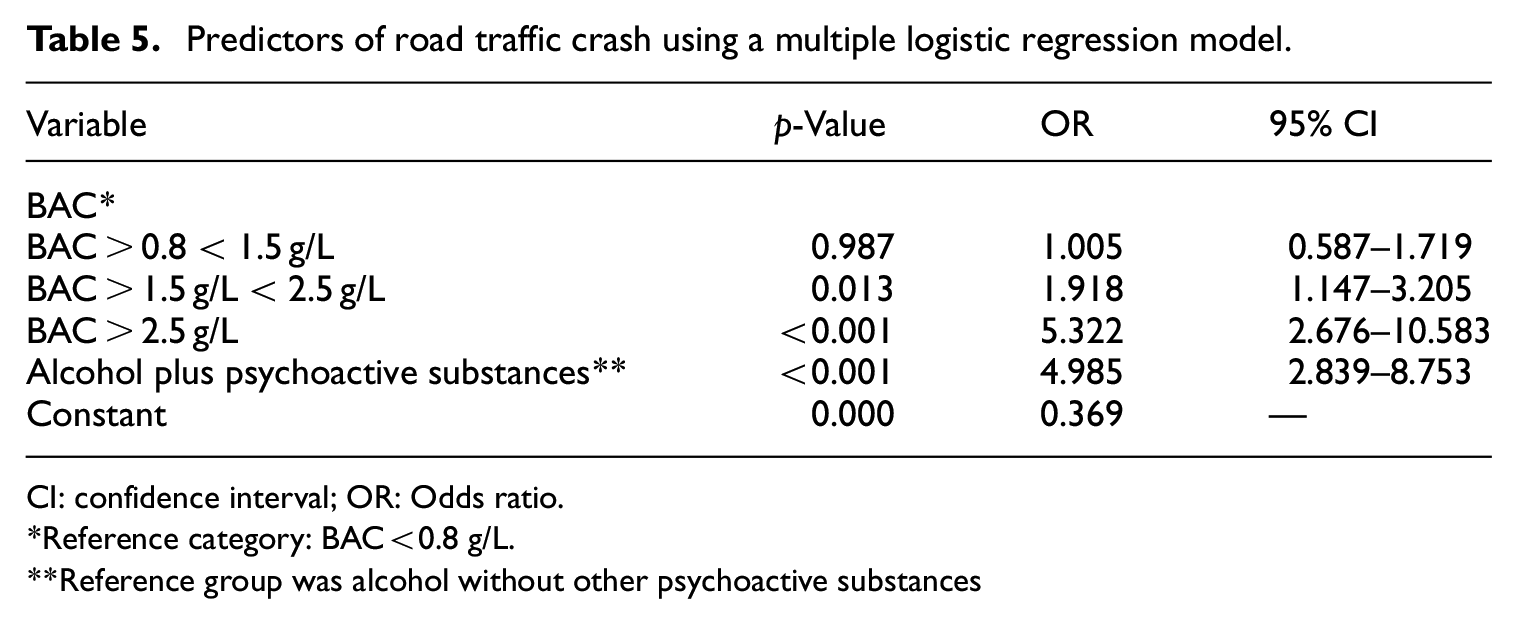
CI: confidence interval; OR: Odds ratio.
Reference category: BAC<0.8 g/L.
Reference group was alcohol without other psychoactive substances
We ran a logistic regression analysis and found that smoking more than 20 cigarettes per day was associated with a judgment of unfitness to drive (OR, 1.973; 95% CI, 1.102–3.530, p = 0.022). EtG was not further considered in the logistic regression analysis, as the finding of this parameter led to a judgment of unfitness to drive due to excessive alcohol consumption. The same analysis was performed in the comparison group, in which we confirmed the association of smoking more than 20 cigarettes/day and judgment of unfitness to drive (OR, 1.726; 95% CI, 1.025–2.909; p = 0.04).
We further analyzed the relationship between BAC and the day of the road accident among the case group. The distribution of BAC in subjects involved in a road accident during a weekend was statistically significant (p = 0.0062) as compared to the BAC of subjects involved in road accidents on a weekday. On weekends, 142 (67.61%) subjects had a BAC higher than 1.5 g/L, and 68 (32.38%) had a BAC lower than 1.5, while on weekdays, 91 (53.84%) subjects had a BAC higher than 1.5 g/L, and 78 (46.15%) had a BAC lower than 1.5.
Subjects with a DUI for psychoactive substances differed in relation to the time of occurrence (p < 0.001) when compared to subjects with an alcohol-related DUI (alone or in association with psychoactive substances). There were no differences in the independent variable of BAC in cases and the variable of judgment of fitness/unfitness to drive. There were also no differences when comparing fitness/unfitness to drive in cases in relation to the type of DUI and the time of occurrence.
Discussion
Our study is innovative due to the methodological approach adopted in a peculiar population consisting of subjects undergoing a medico-legal examination to regrant driving privileges. The integrated medico-legal and toxicological approach allowed the collection of multiple data (demographic, DUI episode, clinical parameters from direct examination of the individuals, and toxicological) with the possibility of simultaneously investigating excessive alcohol consumption and comorbidity with other substance use disorders. Using careful anamnesis, we were able to assess possible variables associated with a road accident and/or psychoactive substances misuse. Our results confirmed the findings of previous studies and correlated nicotine use in our population to a judgment of unfitness to drive independently from road accident involvement.
In particular, the two groups were rather homogeneous in terms of their personal data, socioeconomic factors, and toxicological analysis results, but they differed significantly with respect to the variables associated with DUI episodes. BAC, the simultaneous consumption of psychoactive substances and the time of the road accident/DUI, were statistically different between the two groups.
An alcohol-related DUI (which represented more than 90% of our total sample) is a recognized risk factor for road accidents, according to experimental and epidemiological research. 11 This is due to reduced attentional and cognitive capacities, delays in taking actions, and a higher degree of risk-taking. 1 The higher proportion of a BAC greater than 1.5 g/L among cases than among comparison subjects suggests a dose–response relationship between BAC and the risk of traffic accident involvement, consistent with the demonstrated effect of alcohol intoxication. 12 High BAC levels could be related to an alcohol use disorder or to other pathological patterns of alcohol use. The hypothesis regarding the presence of an alcohol use disorder was not confirmed in our sample, where the integrated methodological approach based on the EtG hair analysis did not yield evidence of a greater prevalence in cases of subjects unfit to drive due to excessive alcohol use. A possible explanation may be found in different patterns of alcohol use, such as binge drinking. 13
The data regarding the greater prevalence of concurrent consumption of psychoactive substances in cases when compared with subjects of the comparison group are not unexpected and are consistent with other studies.5,14 The combination of alcohol and other psychoactive substances (medicinal or illicit) causes a cumulative risk effect, 15 which increases the chance of accident. Cannabis and cocaine were the most frequently detected illegal substances in both groups, consistent with the prevalence of use of these substances in Italy. Notably, 50% of the subjects involved in a car accident and found with at least one psychoactive substance other than alcohol tested positive for cannabis. Although experimental studies provide evidence that cannabis is related to decreased attention, increased reaction time, and reduced ability to control direction, 16 along with a reduction in cognitive and motor functions related to driving, 1 the effect of consuming cannabis on traffic accident involvement is more controversial. 1 Our data on cannabis-related disability should be considered with even more caution due to the lack of blood values for tetrahydrocannabinol.
The joint use of cocaine and alcohol is another important risk factor for road accident involvement. 15 The presence of this substance reflects, as for cannabis, the prevalence of use in the general population. This data is confirmed by the fact that 13.38% (51 out of 381) of the cases involving cocaine use resulted in a judgment of unfit to drive during the medico-legal assessment.
The timing of the DUI/road accident was statistically different between the two groups, with a greater prevalence of DUI subjects without involvement in an accident on weekends. These findings are probably due to DUI police checkpoints on weekends and the fact that there are more people driving under the influence of substances over weekends than on weekdays. 17
Our data showed that in both cases and comparison subjects, the consumption of more than 20 cigarettes/day was associated with a judgment of unfitness to drive. Some factors may explain this data. The first possibility is that the use of more than 20 cigarettes/day suggests a more severe form of tobacco use disorder, a condition that may be related to an alcohol or substance use disorder, as suggested by the fact that daily smokers are more likely to meet the criteria for alcohol-related diagnoses. 18 The second factor may be that tobacco use disorder, independent of alcohol use disorder, is associated with impaired and risky decision-making 19 ; in this way, DUI might be considered a consequence of impaired and risky decision-making rather than an alcohol use disorder. Third, tobacco use might decrease the subjective intoxicating and sedating effects of alcohol, leading to heavier drinking episodes. In other words, individuals using tobacco and alcohol concurrently may have a decrease in the subjective effects of alcohol. Fourth, tobacco use while driving has been related to road accidents. 20
Our findings, regardless of the reasons, may suggest the opportunity to deeply assess tobacco use in DUI subjects or in subjects with a tobacco use disorder. In both cases, the examiner in a forensic or clinical context may discover the potential harmful use of psychoactive substances while driving.
The importance of a medico-legal and toxicological-forensic analysis clearly emerges with the findings of a high percentage of illicit substance users in conjunction with an alcohol problem at DUI among both cases and subjects of the comparison group. 4 Unfitness to drive judgment in the cases and comparison subjects was mostly motivated by the detection of an EtG value higher than 30 pg/mg. These data show the relevance of this strategy for assessing alcohol intake in living persons in a medico-legal context.
The higher BAC levels observed over weekends in cases and the higher prevalence of DUI of psychoactive substances in cases over weekends suggest a different pattern of psychoactive substance use on weekends.
A limitation of the present study is the lack of data concerning blood concentrations of psychoactive substances other than alcohol at the time of DUI. It is not possible to evaluate blood detection thresholds, and there are no data on the concentration of psychoactive substances in urine samples or regarding the time of blood sampling. Thus, it is not possible to establish the presence of a disability related to the presence of a psychoactive substance. Another limitation of the study is the lack of clinical data concerning the physical and/or mental conditions of the cases and comparison subjects at the moments of DUI. The correlation between clinical and laboratory data is essential to demonstrate a driving disability.
Future studies should consider a deeper analysis of tobacco use, clarifying the presence of smoking hours before or during the road accident. A broader sample population that includes female subjects to examine gender-related tobacco use in the context of road accidents may provide useful insights. Validated data from such studies could justify a legislative analysis regarding driving while smoking.
Conclusions
Our study compared a group of DUI subjects involved in non-fatal car accidents with a comparison group of DUI subjects who had not been involved in a car accident. A BAC higher than 1.5 g/L and the concurrent ingestion of psychoactive substances are risk factors for involvement in a road accident, with cannabinoids and cocaine associated with excessive alcohol intake. The integrated medico-legal toxicological-forensic approach did not show statistically significant differences between the two groups in relation to a diagnosis of substance use disorder, confirming that the subjects involved in a road accident while intoxicated are a very heterogeneous population that includes abusers, occasional users, and binge drinkers. The importance of a medico-legal and toxicological-forensic analysis is clearly shown by the finding of a high percentage of users of illicit substances among alcohol-related DUI subjects. Hair EtG concentration was found to be an important parameter in the judgment of fitness/unfitness to drive. Smoking habits appeared to be related to a judgment of unfitness to drive, thus suggesting a possible relationship between tobacco use and other substance use disorders.
Practical implications of our findings include the need to pay more attention to driving license regranting for DUI subjects with a BAC > 1.5 g/L or illicit substance use due to an epidemiological association of these behaviors with road accidents. The proposed methodological approach should always include the use of markers for chronic alcohol consumption, as well as the analysis of keratin matrices that assess illicit substances. This approach should highlight the unrecognized consumption of psychoactive substances in alcohol-related DUI subjects. The modulation of the duration of fitness to drive with periodic checks in subjects most at risk for the identified factors could allow the subject to be monitored periodically and could perhaps have a deterrent effect on the costs of the analysis borne by the subjects. Finally, the data relating to tobacco consumption suggest the advisability of evaluating subjects with DUI paying attention because tobacco could represent a possible clue of a substance use disorder or of a tendency toward risky driving behaviors.
Supplemental Material
sj-docx-1-sci-10.1177_00368504211033702 – Supplemental material for Driving license regranting in DUI subjects: Road accident variables and predictive factors of substance use disorder
Supplemental material, sj-docx-1-sci-10.1177_00368504211033702 for Driving license regranting in DUI subjects: Road accident variables and predictive factors of substance use disorder by Elena Beccegato, Angelo Ruggeri, Massimo Montisci and Claudio Terranova in Science Progress
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, [CT], upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.