
Abstract
The neuromuscular block state may affect the electroencephalogram-derived index representing the anesthetic depth. We applied an Anesthetic Depth Monitoring for Sedation (ADMS) to patients undergoing laparoscopic cholecystectomy under total intravenous anesthesia, and evaluated the requirement of propofol according to the different neuromuscular block state. Adult patients scheduled to undergo laparoscopic cholecystectomy were enrolled and randomly assigned to either the moderate (MB) or deep neuromuscular block (DB) group. The UniCon sensor of ADMS was applied to monitor anesthetic depth and the unicon value was maintained between 40 and 50 during the operation. According to the group assignment, intraoperative rocuronium was administered to maintain proper neuromuscular block state, moderate or deep block state. The unicon value, electromyography (EMG) index, and total dose of propofol and rocuronium were analyzed. At similar anesthetic depth, less propofol was used in the DB group compared to the MB group (6.19 ± 1.36 in the MB mg/kg/h group vs 4.93 ± 3.02 mg/kg/h in the DM group, p = 0.042). As expected, more rocuronium were used in the DB group than in the MB group (0.8 ± 0.2 mg/kg in the MB group vs 1.2 ± 0.2 mg/kg in the DB group, p = 0.023) and the EMG indices were lower in the DB group than in the MB group, at several time points as follows: at starting operation (p < 0.001); at 15 (p = 0.019), 45 (p = 0.011), and 60 min (p < 0.001) after the initiation of the operation; at the end of operation (p = 0.003); and at 5 min after the administration of sugammadex (p < 0.001). At similar anesthetic depth, patients under the deep neuromuscular block state required less propofol with lower intraoperative EMG indices compared to those under the moderate neuromuscular block state during general anesthesia.
Introduction
Although its incidence was reported as 0.13% in the United States, awareness with recall is one of the complications that can follow general anesthesia. 1 Since clinical symptoms such as hypertension or tachycardia cannot be used to discern intraoperative awareness, specific monitoring methods using electroencephalogram (EEG), auditory-evoked potential (AEP), or spectral entropy were developed and have been applied to monitor anesthetic depth during general anesthesia. 2
However, EEG-derived monitoring systems have some critical points, such as measurement time delay, 3 different response to some anesthetic agents, 4 sensitiveness to artifact, 5 and it was affected by the statue of the neuromuscular block. 4 For example, in volunteers who did not receive any sedative drugs, neuromuscular blocking agent alone decreased the EEG-derived index as low as the level shown in sedative state.6,7 EEG change was also observed by the reversal agents, such as neostigmine or sugammadex administered at the end of the general anesthesia. 8 These results implied that electromyography (EMG) activity can affect the detection and analysis of the EEG, even when the neuromuscular blocking agent itself had no effect on the patient’s consciousness.
Recently, deep neuromuscular block was preferential for laparoscopic surgery, due to the improved surgical condition as well as respiratory benefits.9,10 If EEG-based anesthetic depth monitoring is implemented during general anesthesia, the anesthetic dose can be varied according to the degree of neuromuscular block during the surgery. Thus, we hypothesized that the deep neuromuscular block might lower the EEG-derived index, and the propofol requirement would decrease in patients with deep neuromuscular block state during total intravenous anesthesia. To confirm our hypothesis, we applied an Anesthetic Depth Monitoring for Sedation (ADMS Q-001; Unimedics Co., Ltd., South Korea) to patients undergoing laparoscopic cholecystectomy under total intravenous anesthesia, and evaluated the requirement of propofol with the EMG level shown on the monitoring system during the operation.
Methods
This study was performed from September 2015 to September 2017 according to the Declaration of Helsinki after the approval of Institutional Review Board of Seoul National University Bundang Hospital (B-1506/304-010) and registered in ClinicalTrial.gov (NCT02575443). Adult patients, aged between 20 and 80 years, scheduled to undergo laparoscopic cholecystectomy were screened for the current study. All patients were enrolled in one site, Seoul National University Bundang Hospital, South Korea. The exclusion criteria were as follows: an American Society of Anesthesiologists physical status ≥3, current medication history of analgesic or sedative drugs, previous intra-abdominal surgery, pregnant or lactating female, body mass index of ≥30 kg/m2 or ≤16 kg/m2, neuromuscular disease, or neurological disease. Written informed consent was obtained from the enrolled patients before surgery; the enrolled patients were randomly 1:1 assigned to either the moderate block (MB) group or deep block (DB) group using a computer-generated randomization method. The number of subject per block and the number of block were 6 and 10, respectively. The sequentially numbered random allocation was prepared in opaque and sealed envelopes by one designated anesthesiologist.
Non-invasive arterial pressure, electrocardiogram, and pulse oximetry were monitored on arrival at the operating room. In addition, a UniCon sensor (Unimedics Co., Ltd., South Korea) was applied to the patient’s forehead and connected to the ADMS (ADMS Q-001; Unimedics Co., Ltd., South Korea). Neuromuscular depth was monitored on the forearm using TOF-Watch® SX (Organon Ltd, Dublin, Ireland). Two surface electrodes were attached on the skin over the flexor carpi ulnaris muscle to stimulate the ulnar nerve, and a transducer was placed against the thumb. After routine monitoring was established and initial vital signs were measured, remifentanil and propofol were administered to induce general anesthesia using a target-controlled infusion (TCI) system (Orchestra®; Fresenius vial, Brezins, France). The initial effect site concentrations (Ce) of propofol and remifentanil were set at 4 μg/ml and 3 ng/ml, respectively. TOF-Watch® SX was calibrated following the loss of consciousness. All patients received 0.6 mg/kg of rocuronium to achieve adequate neuromuscular relaxation before tracheal intubation was performed. The patient’s lungs were ventilated with medical air and oxygen (0.5 of inspired oxygen fraction).
During the laparoscopic cholecystectomy, train-of-four (TOF) stimulation was automatically provided every 10 s; the post-tetanic count (PTC) was evaluated every 10 min. The neuromuscular block was controlled by rocuronium infusion (from 0.1 to 1 mg/kg/h), according to the group arrangement. For the MB group, the goal was to maintain the TOF count at 1 or 2. For the DB group, however, the goal was to maintain the PTC at 1–2, with no twitch in the TOF. The Ce of propofol was titrated to maintain a unicon value of 40–50; the Ce of propofol was increased or decreased by 0.5 μg/ml appropriately. The Ce of remifentanil was changed, by 0.5 ng/ml, to maintain a systolic arterial pressure within ±20% of the preoperative baseline value. The control range of Ce of remifentanil was 0–6 ng/ml. Uncontrolled hypertension or tachycardia, even at 6 ng/ml of remifentanil, was managed using either an appropriate calcium channel blocker or beta blocker. If hypotension continued after discontinuing remifentanil, ephedrine or phenylephrine was administered to the patient. Bradycardia, which was defined as under 45 beats/min, was treated with 0.5 mg of atropine.
Infusion of rocuronium was discontinued when pneumoperitoneum was finally decompressed. In the MB group, 0.04 mg/kg of neostigmine (with 0.01 mg/kg of glycopyrrolate) was injected for the reversal of neuromuscular block when their TOF count became 4. In the DB group, 4 mg/kg of sugammadex was injected to patients when at least one of TOF count appeared. When spontaneous respiration was restored and the patient had regained consciousness, the endotracheal tube was extubated from the patient’s trachea. All the patients were transferred to the post-anesthetic care unit.
The primary outcome of the current study was the propofol requirement during the general anesthesia. The secondary outcomes were the electromyography (EMG) index, which were displayed on the ADMS Q-001 monitor and intraoperative vital signs. The secondary outcomes were recorded at the following time points: before induction (baseline); after sedation; after the rocuronium injection; at intubation; at the start of the operation; at 15, 30, 45, and 60 min after initiating the operation; at the end of the operation; at 5 min after the administration of neostigmine or sugammadex; and at extubation.
A sample size analysis was performed based on our pilot data. To detect a 1.16 mg/kg/h of difference in the total propofol requirement with a common standard deviation of 1.48 mg/kg/h, it was determined that 27 patients per group were required with a statistical power of 80% and type I error of 5%. Assuming an overall dropout rate of 10%, 30 patients per group were required. Data were presented as mean ± standard deviation (SD) or numbers (%). The normality of data was evaluated using a Shapiro–Wilk test. The Mann–Whitney U-test (Student’s t-test), chi-square test, or Friedman test (Repeated measures of ANOVA) was used for statistical analyses where appropriate. SPSS software (ver. 21, IBM Co., Armonk, NY, USA) was used for statistical analyses and the statistical significance was set as p < 0.05.
Results
Although a total of 60 patients were enrolled, data of 59 patients were analyzed in the final study (Figure 1). The characteristics of the patient cohort, anesthesia administration, and the surgeries are outlined in Table 1.

Flow diagram of patients’ enrollment.
The characteristics of patient, anesthesia, and operation.

Data were presented as mean ± SD or number (proportion).
In comparison to the MB group, the DB group required less propofol (6.19 ± 1.36 in the MB mg/kg/h group vs 4.93 ± 3.02 mg/kg/h in the DM group, p = 0.042) and more rocuronium (0.8 ± 0.2 mg/kg in the MB group vs 1.2 ± 0.2 mg/kg in the DB group, p = 0.023).
The unicon values and EMG indices are presented in Table 2. The unicon values were comparable between the two groups during the anesthesia period. The EMG indices, however, were lower in the DB group than in the MB group at several time points as follows: at starting operation (p < 0.001); at 15 (p = 0.019), 45 (p = 0.011), and 60 min (p < 0.001) after the initiation of the operation; at the end of operation (p = 0.003); and at 5 min after the administration of sugammadex (p < 0.001).
The unicon value and electomyography index.

Data were presented as mean ± SD.
The mean arterial pressure and heart rate of the two groups were shown in Figure 2. The mean arterial pressure was significantly lower in the DB group than in the MB group, at the end of the operation (p < 0.001) and at the time of extubation (p = 0.002). The heart rate also significantly differed at 60 min after the operation (p = 0.046), at the end of operation (p < 0.001), at 5 min after the administration of neostigmine or sugammadex (p < 0.001), and at the time of extubation (p < 0.001). Intraoperative awareness was not observed in any patients during general anesthesia.
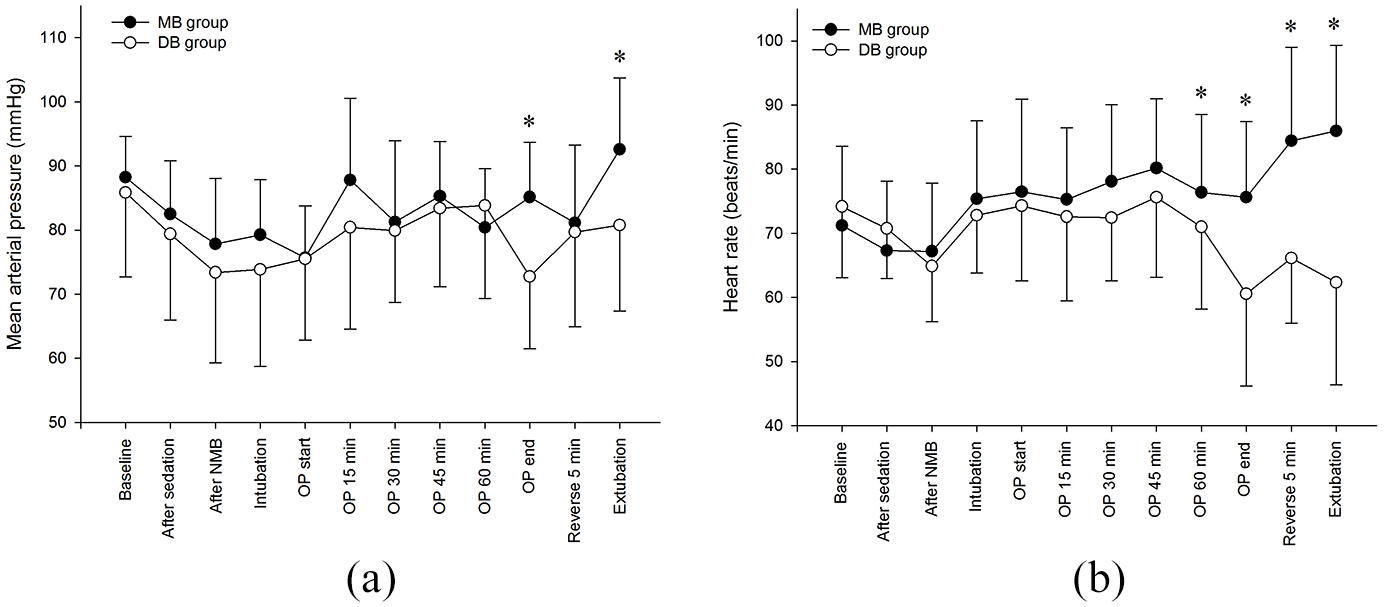
Intraoperative vital signs: (a) mean arterial pressure and (b) heart rate.
Discussion
In the current study, despite the similar anesthetic depth, the propofol requirement was lower in patients with deep neuromuscular block status, compared to those with moderate neuromuscular block status.
In general anesthesia, it is important to maintain appropriate depth of anesthesia, which is measured by various methods. Bispectral index (BIS) is a representative and widely-used method to measure intraoperative anesthetic depth,11,12 and there are several reports to evaluate the influence of neuromuscular block on the depth of anesthesia using BIS.
Bruhn et al. 13 reported a case, where the BIS decreased after the administration of a neuromuscular blocking agent during constant infusion of propofol and remifentanil. In another study, decreased BIS was also observed even in fully awake volunteers following neuromuscular block alone. 6 These results are based on the theory that neuromuscular blocking agent reduced cerebral cortical activity by blocking the proprioceptive afferent input from the muscle to the cerebral cortex.14,15 Similarly, BIS value was increased depending on the presence of EMG activity while reversal of NMB with sugammadex or neostigmine.8,16
However, contradictory results were reported that neuromuscular block was not related with the anesthetic depth, and therefore did not reduce the anesthetic requirement.17–19 In addition, BIS values were not affected by different level of neuromuscular block.20,21
In our study, ADMS is used to monitor the depth of anesthesia, which is also designed to monitor the depth of sedation by analyzing the EEG waveform. The ADMS applies qCON and qNOX monitor technology, and pCON was reported to have acceptable correlation with the BIS. 22 The algorithm calculating qCON is based on the adaptive neuro fuzzy inference system composed of the energy of four frequency ratios and the value of the EEG suppression rate. 23 The ADMS and BIS values were measured similarly during dental-procedural sedation and general anesthesia.23,24
We aimed to conduct the current study while maintaining either moderate or deep neuromuscular block status using TOF-Watch® SX monitoring. In deep neuromuscular block group, propofol was not required as much as in the moderated neuromuscular block group in order to maintain similar anesthetic depth. Since a deep neuromuscular block lowered the unicon value of ADMS much more, propofol did not seem to be required by patients in the deep block group to maintain a unicon score of 40–50. In this study, we enrolled patients undergoing laparoscopic cholecystectomy which did not take long. The total anesthesia time was around 100 min. The anesthetic requirement may show more differences between the MB and DB group in more complicated and long surgery.
It should be assessed what other factors can affect anesthetic requirement when monitoring anesthetic depth. The frequency and amplitude of EEG are 0.5–100 Hz and 2–100 μV, while those of EMG are 20–1000 Hz and 50–2000 μV, respectively. 25 Thus, the ranges of biopotential signals overlap in a certain range of the frequency and amplitude. It is currently unknown exactly how the EEG and EMG recordings interact with each other in EEG-derived anesthetic depth monitoring. However, it has been known that EEG responses are attenuated by muscle paralysis and more affected by EMG in sedative or light anesthesia state.26,27 During ADMS, samples of EEG and EMG are acquired in the ranges of 0.5–45 Hz and 30–75 Hz, respectively. 28 Chi et al. 23 reported that an EEG signal recorded by ADMS is acceptable despite high EMG values.
As a limitation of this study, the clinical relevance of these results is not yet clear. Avidan et al. 29 reported that intraoperative BIS monitoring did not seem to affect the control of inhaled anesthetic gas concentration, which is even directly related to the depth of anesthesia, or intraoperative awareness in a standard clinical practice. In this study, the additional dose of propofol was approximately 1 mg/kg/h in the moderate block group. It is unclear how clinically significant 1 mg/kg/h of propofol is. Additionally, we could find that the resulting mean intraoperative EMG value measured using an ADMS decreased during the deep neuromuscular block state. We cannot, however, accurately report how well the EMG values of ADMS and the TOF-Watch® SX monitoring correlate with each other in this study. Further study can be performed to confirm how accurately the EMG value of ADMS can reflect the degree of neuromuscular block. Last, the age range was between 20 and 80 in this study. In the elderly patients, the cortical response might be different from that of the younger patients. In the patients aged over 65 years, BIS and entropy was maintained within the recommended range in 45% and 32%, respectively. 30 It should be considered that age-related differences could act as a confounding factor.
Conclusion
At similar anesthetic depth, patients under the deep neuromuscular block state required less propofol compared to those under the moderate neuromuscular block state during general anesthesia. We could know that neuromuscular block state affected the EMG indices of ADMS; however, the exact relationship between the EMG index and Unicon value of ADMS is uncertain.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant [No. 06-2015-145] from the research fund of Unimedics, Seoul, South Korea.
Ethics approval
Ethical approval for this study was obtained from Institutional Review Board of Seoul National University Bundang Hospital (B-1506/304-010), in accordance with national law and in accordance with the 1975 Helsinki Declaration (as revised).
Informed consent
Written informed consent was obtained from all subjects before the study.