
Abstract
Midlife is an important time in the working lives of many people, representing a time of potential peak earnings and career success. It can also be a time of challenge, particularly in light of the increasing prevalence of onset of chronic illness and disability (CID) in this population. State Vocational Rehabilitation Agencies (SVRAs) could be a critical resource for individuals, who due to the onset of CID in midlife, are at risk for involuntary retirement. Unfortunately, SVRAs are largely unknown to people outside of the disability community. To better understand involuntary retirement, data are presented from the nationally representative Health and Retirement Study, providing insights on who is at the highest risk for involuntary retirement, and the circumstances surrounding their retirement decisions to determine whether VR agencies could fill this gap. Findings expose patterns of disparity in involuntary retirement based on race, socioeconomic status, and number of reported disabilities or health conditions. Individuals who retired involuntarily reported higher importance of health as a reason for retirement and lower importance of other reasons. Involuntary retirement appears to be a manifestation of CID, which potentially could be addressed with accommodations or vocational services available through SVRAs. Implications for rehabilitation counseling practice are presented.
Middle adulthood, considered the developmental stage between approximately 45 to 60 years of age, is defined by a constellation of events and experiences across multiple life categories including jobs and careers, family responsibilities, and life transitions (Infurna et al., 2020). It is during this life stage that individuals are confronted with increasingly complex responsibilities at work, caring responsibilities for older relatives and children, maintaining romantic partnerships and friendships, and addressing their health and well-being. Individual resources to attend to these challenges are at least partially influenced by early life factors such as socioeconomic status, educational attainment, and family life (Infurna et al., 2020). Trends suggest increasing rates of chronic illness and disability (CID) among this population, at least in part due to lifestyle factors and lack of access to quality healthcare (Infurna et al., 2020; McGrath et al., 2019).
For some, impacts of CID cause an individual to leave the workforce and are severe enough to qualify for disability benefits (Schimmel Hyde et al., 2022). Many other individuals find themselves in a situation where CID is impacting work, but they would not qualify for benefits, leaving them with threatened job security but little in the way of options to plan for retirement and remain working for the duration of their expected career. The alternative path for many is to apply for Social Security Disability Insurance (SSDI). Unfortunately, making an SSDI claim bars workers from even trying to work while they are waiting for a determination on benefits. This creates an impossible scenario for individuals who develop limitations that impact work but are not career-ending, as it is difficult for them to remain employed and economically self-sufficient absent disability assistance, but they cannot obtain assistance from SSDI without first leaving the labor force (Autor, 2011).
State Vocational Rehabilitation Agencies (SVRAs) are the predominant source of employment assistance for individuals with a wide range of disabilities (Stapleton et al., 2010). Public rehabilitation has been available to both veterans and civilians since 1920 (McFarlane et al., 2011; Wright, 1980) and includes a variety of services to help disabled adults acquire or maintain employment by way of offsetting or removing disability-related barriers. Adults with disability onset in midlife have existing work skills and employment histories and stand to benefit immediately from SVRA services with the likelihood of retaining a job or through rapid placement assistance, quickly reaching an employment outcome. Individuals who were born with disabilities, identify as being disabled, or have been part of the disability community may be familiar with resources, such as those available through SVRAs to help with job retention; however, individuals who are experiencing disability or chronic illness for the first time in midlife are likely unaware of resources or supports that would allow them to keep working (Heidkamp et al., 2012). Vocational rehabilitation is an underutilized but invaluable resource to workers who incur CID in midlife that could support individuals to keep working until their desired retirement age.
Employment and Health
The relationship between health and employment is complex and may be synergistic. Work is a powerful social determinant of health, is modifiable and amenable to intervention, and is an important area to examine as a potential “source of beneficial social and economic resources and attainment of social position and status” (National Institutes of Health, 2021). Longitudinal evidence has demonstrated that unemployment has deleterious effects on both physical and mental health (Hergenrather et al., 2015a, 2015b). Employment, above what is gained through income, provides intangible benefits such as meaning, routine, social connection, and cognitive engagement that support health, particularly as we age (Vélez-Coto et al., 2021). Work may also expose employees to hazards, exposure to illness, and occupational stress and may detract from health in some circumstances (Armenti et al., 2023). Health is a factor in the ability to work and has a role in retirement decisions for older workers (Williamson & McNamara, 2003).
Complexities of Retirement Decisions
Retirement is a social and developmental milestone, which, due to shifts in lifespan, workforce norms, and economic conditions, has become less institutionalized in recent decades (Fisher et al., 2016; Williamson & McNamara, 2003). As workers age, several factors seem to influence their decisions regarding retirement, including quality of job, financial readiness for retirement, availability of work, and the degree to which they can continue to perform their job adequately. Other considerations may include caregiving responsibilities or other competing responsibilities to holding a paid job (Dang et al., 2022). Researchers suggest that whether retirement is planned, desired, or involuntary may influence the resulting impact on individual well-being (Filomena & Picchio, 2023).
The cumulative advantage–disadvantage framework provides a theoretical basis for understanding patterns in retirement context, not as a sudden occurrence in older age but as a result of a combination of individual experiences and interconnected systemic oppression and social structures that have implications for individuals’ economic situation, career trajectory, and health in middle and older adulthood (Choi et al., 2017; Crystal et al., 2017). Patterns of vulnerability in retirement expose two key areas of disparity: (a) good health is not uniformly distributed and racial and economic marginalization bears out in health outcomes in middle to older adults (Lowsky et al., 2014) and (b) economic and social position can increase or buffer risks to being forced out of the workplace prematurely (Han, 2021; Williamson & McNamara, 2003). Sociodemographic factors that are linked to health disparities may also be relevant to retirement.
Involuntary Retirement
Involuntary retirement, contrasted with leaving the workforce on one’s own terms, has already been associated with health, economic, and social consequences (Denton et al., 2013). Data on the prevalence of forced retirement is not readily available, but evidence suggests that some involuntary retirements are directly due to illness (Schimmel Hyde et al., 2022; Williamson & McNamara, 2003). However, the onset of CID does not necessarily cause job disconnection; disabled individuals can and do work successfully in a variety of jobs. Forced exit from the workforce is recorded at higher rates for service and working-class employees than those in skilled positions and earning higher salaries (Ebbinghaus & Radl, 2015). Identifying when, and for whom, CID onset threatens work is necessary to inform vocational services and support for workers facing forced retirement when they would prefer to continue to work. The benefits of continuing to work are great: for workers in middle age, employment is a possible source of income, identity, social connection, personal meaning, and cognitive engagement (Dang et al., 2022). Conversely, employment loss or absence places individuals at increased risk for several personal and health-related repercussions.
Consequences to Health
Retirement is associated with declines in physical and cognitive health and function (Delugas & Balia, 2019), although findings are mixed (Filomena & Picchio, 2023). Longitudinal evidence suggests that employment is predictive of better physical and mental health, with more dramatic impacts of job loss and unemployment on health indicators (Hergenrather et al., 2015a, 2015b). Strikingly, those who left their jobs on their own terms did not experience these negative changes in health, and those who became re-employed experienced positive increases in health reports after a period of re-employment (Hergenrather et al., 2015b). These patterns were also present in studies of mental health indicators, showing similar trajectories of unemployment associated with higher psychological distress and symptoms of depression and anxiety, and employment and re-employment associated with better mental health (i.e., lower distress, fewer symptoms; Hergenrather et al., 2015a).
Consequences to Well-Being
Beyond health impacts, involuntary retirement is associated with broader consequences to individuals’ well-being. Financially, individuals who retire involuntarily are worse off than those who retire by choice (Denton et al., 2013). Hawkley and colleagues (2020) found that “financial shocks” associated with sudden job loss predicted greater loneliness among older adults, over and above what was explained by health status. Patterns of adjustment to retirement and satisfaction with retirement are less favorable among those who retire earlier than expected (Fisher et al., 2016). Individuals who retire unexpectedly (i.e., due to health changes or job loss) report lower life satisfaction ratings than those who retire at a time of their own choosing (Clarke et al., 2012; Dingemans & Henkens, 2014).
Purpose of the Present Study
The goal of this study is to explore the context of involuntary retirement to identify the degree to which individuals may be at increased risk for involuntary retirement due to race, socioeconomic position, or CID and to explore the motivations for retirement based on whether retirement was forced or voluntary. A data set was selected that is nationally representative of older adults, because of the increase in CID correlated with age. This data, although not a disability-specific sample, contains a high proportion of individuals reporting at least one CID (Coyle & Putnam, 2017). Policy researchers have suggested that this data set is a valuable resource for understanding the relationship between disability and retirement (Schimmel Hyde & Stapleton, 2017). SVRAs are ideally poised to support older workers to continue to work if desired, through targeted counseling, workplace accommodations, and rapid re-employment services. Service utilization by middle-aged and older customers has been falling faster than other age groups. Highlighting risk factors for involuntary retirement can help agencies and counselors understand the needs of middle-aged and older workers and assist in developing targeted strategies to increase service utilization.
The following research questions were addressed:
Disability rates are notably higher in communities of color and among those living in poverty (Goyat et al., 2016; Maroto et al., 2019), and racial health disparities among older adults cannot solely be attributed to socioeconomic status (National Institutes on Aging, 2020). To understand the contribution of intersecting identities to risk, key demographic factors including gender, race, level of education, and self-reported CID were explored to identify potential disparities in reports of retirement circumstances.
Retirement decisions are complex and individual, reflecting a variety of circumstances and preferences of the worker, their family, and the features of a person’s job. Evaluating the motivations of individuals as a function of forced or voluntary retirement illuminates possible areas of intervention to support middle-aged and older adults to retain workforce connection.
Methodology
Sample
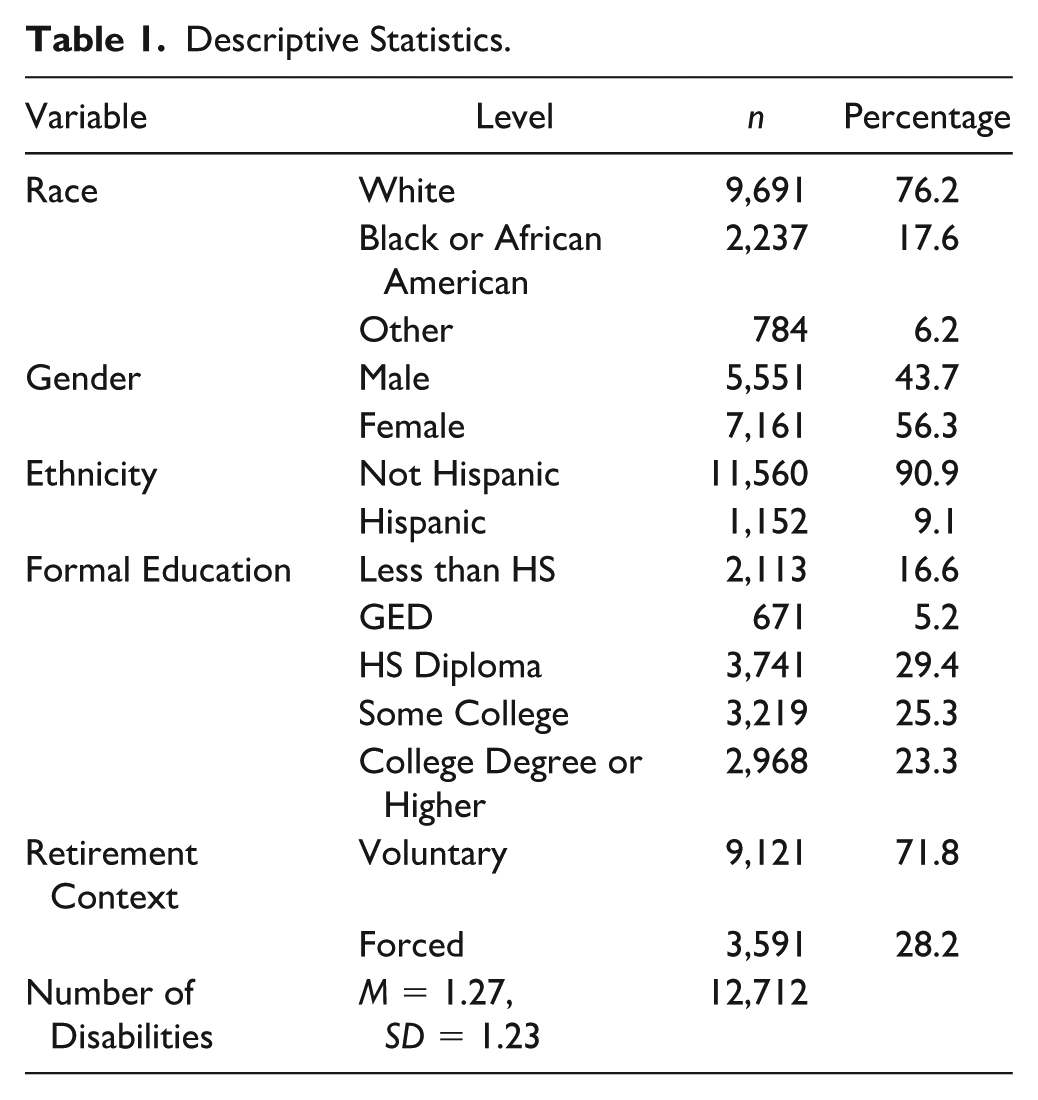
The Health and Retirement Study (HRS) is a 28-year-old panel study of adults in the United States aged 55 and older. The sample is nationally representative, enrolls new birth cohorts every 6 years, and follows individuals and their partners from enrollment until death (HRS, 2024). Data collection is extensive, leveraging phone, in-person, and internet data collection processes for primary questionnaires and examinations (HRS, 2024). For the present study, we selected participants with complete data on demographics, retirement context, and CID status. This resulted in 12,712 participants (See Table 1).
Descriptive Statistics.
Data Descriptions
The following subsections of HRS data were leveraged for this analysis: (a) Respondent information/ demographics; (b) Retirement; and (c) Disability.
Variables
Demographics
Respondent report of gender (Male or Female), Race (White, Black/African American, or Other), Ethnicity (Hispanic or Non-Hispanic), and Level of education (Less than high school, General Educational Development [GED], High School Diploma, Some College, College Degree or Above).
Disability Report
Respondents reported whether a doctor had diagnosed them with any of the following disabilities or health conditions: Heart Disease, Cancer, Stroke, High Blood Pressure, Diabetes, Lung Disease, Mental Health Condition, or Arthritis. To calculate the number of disabilities, we created a variable that represented the sum of those reported.
Retirement Context
The retirement context variables were drawn from the biennial survey files, including the date and wave of reported retirement and whether retirement was forced or voluntary. Participants were included in the analysis if they reported either that their retirement was forced or voluntary; those who reported their retirement as “part voluntary, part forced” were excluded because it is difficult to categorize this response by group with confidence. At the wave where retirement was reported, individuals rated four reasons for retirement (poor health, wanted to do other things, did not like the work, and spending more time with family) on a scale from 1 (very important) to 4 (not important). Items were reverse-coded so that higher scores indicated greater importance.
Data Analysis
All data management, descriptives, and analyses were conducted using R version R v4.4.2 (R Core Team, 2023) and R Studio version 2024.09.1 Build 394 (RStudio Team, 2024). To assist with data preparation, the tidyverse and dplyer packages were used. The HRS data set contains data collected during 15 waves, every 2 years from 1994 to 2022. To reduce participant burden, some information (i.e., demographics) is only collected once. The RAND longitudinal data file contains a record of each participant in the HRS data set and contains a rich subset of variables from the Core interviews, biennial surveys, and exit interviews (RAND, 2023). This data file was used as the primary source of information on participant demographics and disability reports. The retirement information was drawn from the biennial surveys and merged using the participant identification variable (HRS, 2023). Data were examined for complete cases, resulting in a final sample of 12,712. Variance Inflation Factors were calculated with no evidence of multicollinearity. A description of the sample is available in Table 1.
A secondary data analysis of HRS data was employed to address the following questions:
A logistic regression model was used to explore this question, using demographics (i.e., race, ethnicity, gender, level of education, and report of CID) with retirement context (involuntary or voluntary) as the outcome variable.
A Multivariate Analysis of Variance (MANOVA) was conducted to explore the four reasons (health, wanted to do other things with time, did not like the work, wanted to spend more time with family) to retire by involuntary or voluntary retirement context.
Results
Racial, Socioeconomic, and Health Disparities in Forced Retirement
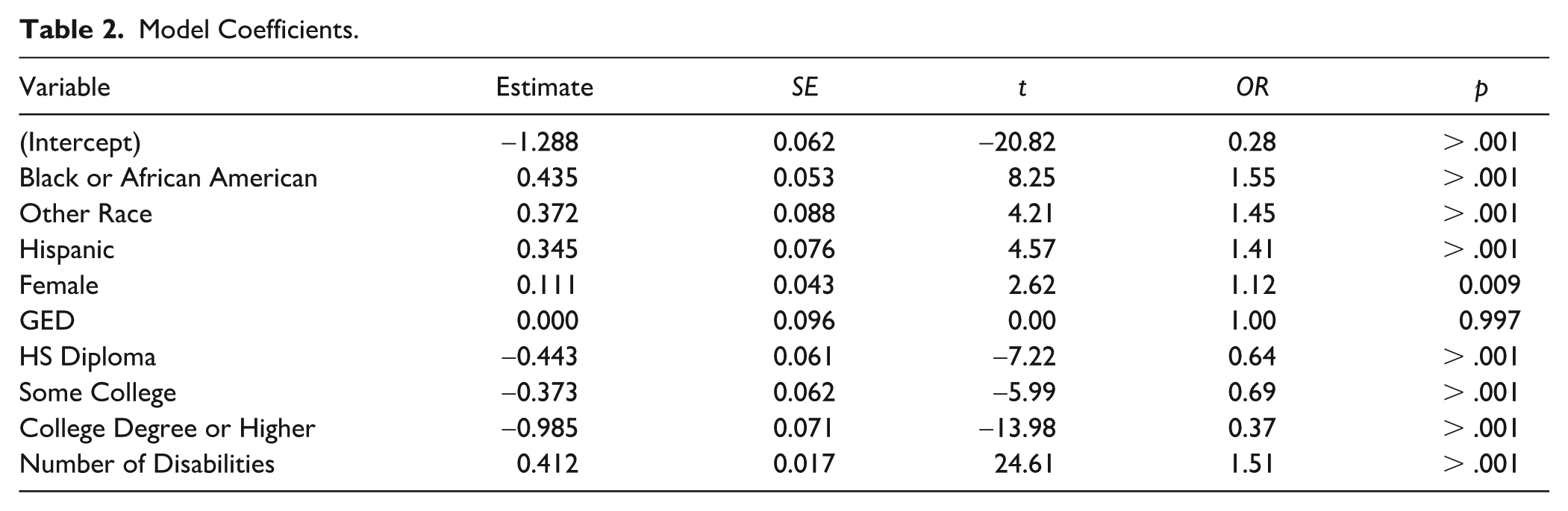
To address RQ1, a logistic regression model was used to predict voluntary or forced (involuntary) retirement while examining the significance and odds ratio of each demographic predictor. Model fit was assessed using multiple indicators, including a chi-square test of Pearson’s residuals (χ2 = 12,744.5, p = .39) and the Hosmer and Lemeshow goodness-of-fit test (χ2 = 8.6411, df = 8, p = .37), both suggesting that the model is an adequate fit for the data. Table 2 shows full model results. Race, ethnicity, gender, level of education, and number of disabilities reported all showed a significant relationship to the retirement group. For racial categories, Black or African American respondents were 55% more likely than White respondents to retire involuntarily, and those reporting another race were 44% more likely than White respondents. Hispanic respondents were 41% more likely to retire involuntarily compared to non-Hispanics. By level of education, the reference category in the model was set to less than a high school education. Those with a GED were about as likely to report involuntary retirement, while those with a high school diploma were 36% less likely, some college 31% less likely, and a college degree or higher were 63% less likely than people with less than a high school education. For each additional disability reported, respondents were 51% more likely to report involuntary retirement. While significant in the model, the odds ratio for females as compared to males was modest, suggesting little practical difference between groups.
Model Coefficients.
Reasons to Retire by Group
Groups (voluntary vs. forced retirement) were compared on the four reasons to retire included in the retirement survey: (a) poor health, (b) wanted to do other things, (c) didn’t like the work, and (d) wanted to spend more time with my family. A MANOVA revealed a significant effect of retirement context (forced or voluntary) for the importance of these reasons to retire, Wilks’ Lambda = 0.70, F(4, 11) = 1239.7, p < .001, effect size = 0.52. Univariate tests showed significant differences between groups for all reasons (p < .001). These findings suggest poor health is a more important reason to retire among those who retire involuntarily, and doing other things, disliking work, and spending time with family are more important reasons for those who retire voluntarily. Table 3 shows means and standard deviations for importance ratings across all categories.
Retirement Reason by Group.

Notes. All variables are on a scale of 1 to 4, 1 = not important, 4 = very important.
Discussion
This study was designed to explore the context of involuntary retirement in a nationally representative sample of middle-aged and older adults, to identify the degree to which individuals may be at increased risk for involuntary retirement due to race, socioeconomic position, or CID and to explore the motivations for retirement based on whether retirement was forced or voluntary. Findings revealed increased risk for involuntary retirement for Black or African American respondents, as well as those reporting another race as compared to White respondents. Hispanic respondents were also more likely to retire involuntarily. Respondents with a high school diploma, some college, or a college degree were less likely to report involuntary retirement than those with less than a high school education. Disability condition was also positively related to involuntary retirement. Group comparisons of reasons for retirement, including poor health, wanting to do other things, not liking the work, and spending more time with family revealed significant differences in motivation for retirement. Specifically, the involuntary retirement group showed an average higher endorsement of poor health as a reason, while the voluntary retirement group showed a higher average endorsement of the other reasons.
Study findings align with previous research suggesting that CID is associated with a significant risk of involuntary retirement (Denton et al., 2013; Han, 2021; Welsh et al., 2018; Williamson & McNamara, 2003). For many workers, leaving their jobs before they planned introduces additional financial hardship, which is particularly concerning given the higher likelihood of early, unplanned, or forced retirement among those with lower socioeconomic status (Ebbinghaus & Radl, 2015; Han, 2021; Williamson & McNamara, 2003) who are less likely to have significant retirement savings. Among other consequences, involuntary retirement poses risks to mental health and well-being through several mechanisms including financial strain and loss of psychosocial resources such as identity and community (Han, 2021; Rhee et al., 2016).
Consistent with the cumulative advantage/disadvantage framework, the relationship between race, ethnicity, and levels of formal education and retirement status reflects previous work exploring the relationships between job quality and self-reported health, as well as sociodemographic predictors of workers more likely to hold jobs that are more precarious, flexible, and secure (Choi et al., 2017; Eisenberg-Guyot et al., 2020). It is likely that there are aspects of jobs that make retention more or less possible within the context of CID, and that jobs with greater security and flexibility are not as threatened by health challenges as jobs with higher rates of unemployment, low control over tasks or schedule, and low employer commitment to workers (Eisenberg-Guyot et al., 2020). Furthermore, individuals in higher-status jobs may have more social capital to request accommodations as they need them, while individuals in lower-status or more precarious employment sectors may need outside support to navigate situations where health and work conflict.
Findings expose an underexamined manifestation of onset of CID in midlife, that rehabilitation counselors are well-situated to address. Data suggest that, for some, the onset of CID may push them out of the workforce and into retirement before they planned and when they would otherwise prefer, or need, to work. In addition, findings indicate that this situation is not uniformly distributed across the sample and that sociodemographic risk factors for health disparities also appear to be linked to involuntary retirement. Researchers in other fields who have explored features of early retirement for reasons of disability have focused on the strain that it places on public benefits (Autor, 2011; Hill et al., 2016; Stapleton et al., 2010). Without minimizing the importance of maintaining a robust social safety net, this approach fails to recognize the impact of forced retirement due to the onset of CID on individuals and treats the occurrence of forced retirement due to CID as an immovable or unavoidable consequence. Rehabilitation counselors would disagree, as they are familiar with accommodations and resources that can support disabled workers and help them continue to perform their jobs. Yet, rehabilitation services are underutilized and not well known to those outside of the disability community. Different from a person who is born with a disability or who sees disability as a central part of their identity, individuals who experience a chronic illness for the first time in midlife may not see disability-related or rehabilitation services as “for them.” The Americans with Disabilities Act Amendments Act (ADAAA) provided an expanded definition of disability to include individuals who experience chronic illness (Rumrill & Bishop, 2015). This ensures access to civil rights protection in employment, as well as public services and accommodations. Relative to work, individuals experiencing CID for the first time in midlife may not be aware of these protections or the avenues available to them to support their continued engagement with their jobs.
Implications for Rehabilitation Counseling Practice
The HRS data include older adults in the United States with and without disabilities. While some participants have lifelong disabilities (Coyle & Putnam, 2017), most do not identify as disabled. A high proportion of the sample reports being diagnosed with at least one CID. Based on available data, it is not known whether accommodations were pursued for any of the individuals who reported forced retirement. Whether individuals pursued any kind of support with job retention is also unknown. The SVRA services could be a valuable source of support for middle-aged and older workers who are experiencing disability-related barriers to job performance and job retention (Rumrill & Bishop, 2015), but agencies are largely unknown to the general public. Vocational rehabilitation counselors can help individuals understand how CID may impact their work performance (now, and in the future) and provide resources to reduce the negative impact. They may also provide support for coping with a condition that may be unpredictable or progressive.
Job accommodations or modifications are a critical resource for both employees and their employers who may wish to maintain valued employees with CID. Hill et al. (2016) found that only about a quarter of older workers received any kind of job accommodation, and no clear patterns emerged suggesting that a particular kind of employer, or a person with a particular disability barrier, seemed to receive accommodation at higher or lower rates. Similarly, Maestas and Mullen (2019) defined a subpopulation of workers as “accommodation sensitive,” defined as “individuals on the margin of working or not working depending on whether they are accommodated” (p. 3), estimating that approximately 23% of working age adults fall into this category and that between 47% and 58% of accommodation-sensitive workers lack accommodations. However, accommodations remain an effective strategy to help people keep their jobs when CID symptoms impact work (Hill et al., 2016; Job Accommodation Network, 2024; Maestas & Mullen, 2019). Longitudinal data suggest that workers with CID who had accommodations were more likely to be working 4 years later than similar workers who did not have accommodations (Maestas & Mullen, 2019).
The job accommodation process requires knowledge on the employee’s part (what is an accommodation, how do I get one), and self-advocacy skills to navigate the request process (Hill et al., 2016). For those who have not had experience or awareness of disability, this process is likely inaccessible. A significant barrier to work retention for older workers is that employees are not asking for accommodations, thus never setting off the process of determining whether an employee was qualified, or a request was reasonable (Hill et al., 2016; Maestas & Mullen, 2019). Rehabilitation counselors working at SVRAs are well-versed in accommodation requests and job modifications and can provide education to both the worker and their supervisor about potential solutions and implementation. Beyond accommodations, SVRA services that could support an individual with CID include counseling and guidance if a person needs to consider a new job, training, job placement, self-advocacy training, or assistive technology (Rumrill & Bishop, 2015). These services can help a person retain engagement in the workforce if their current job is no longer feasible or they do not want to continue but still want to work in some capacity. Individuals who leave the workforce and begin receiving disability benefits rarely return (Maestas & Mullen, 2019), underscoring the importance of increasing awareness of SVRA services and potential mechanisms to keep people working before they reach the point of acquiescing to involuntary retirement (Gould-Werth et al., 2018).
For older workers who incur CID, employer discrimination due to age and disability status (real or perceived) is a threat to maintaining a job or finding a new one. Evidence from age-related employment discrimination data shows the highest rates of charges filed under the Age in Employment Act are from individuals ages 62 to 65, those just approaching retirement age, which may align with a perception of being forced out of the workplace before the individual is ready to retire (Miller & Bruère, 2023; von Schrader & Nazarov, 2016). Disability-related employment discrimination charges also reflect a relationship to age; nearly 60% of employment discrimination charges under the Americans with Disabilities Act are filed by individuals 40 and older, with 16% filed by those 55 and older (Miller & Bruère, 2023). Despite these obvious connections, aging as a topic is rarely included in disability literature nor is it addressed sufficiently in pre-service counselor training (Kettaneh et al., 2015). Authors concluded, “Age-related disabilities, in tandem with increasing numbers of older workers, call attention to the importance of research to ensure that rehabilitation counseling training, policies, and practice are in step with meeting the job accommodation needs of this population” (p. 84).
Implications for SVRAs
In the most recently available Rehabilitation Services Administration (RSA, 2022) administrative report, the number of participants ages 45 and over fell by nearly 28,000 from Fiscal Year (FY) 2017 through 2019—the largest proportional decrease of any age group. This trend stands in stark contrast with demographic shifts in the U.S. population where the combined effect of an aging “baby boomer” generation and a declining birth rate over the past 5 decades has yielded an unprecedented demographic shift in the U.S. population. As a method for SVRAs to maintain their relevance as a public service and resource, they may consider expanding their outreach to include sources of client referrals that cater to middle-aged adults who are experiencing CID. Recommended sources include medical centers, pain management centers, or even larger employers within the community of local offices, emphasizing SVRA resources available to help individuals maintain employment, and support both individuals and employees to navigate accommodation negotiations and job retention services. Assistive technology and diagnostic services could also be useful for this population (Fleming et al., 2015), and explaining these services to the relevant stakeholders with examples may help raise awareness and interest among potential clients and their employers. In these community partnerships, employers may be encouraged to learn that many accommodations can be implemented without direct cost, and others may involve a one-time cost (Job Accommodation Network, 2024) that could potentially be ameliorated by the SVRA. The SVRAs may also share additional resources to defray the costs of accommodations and provide consultation on workplace practices that could make the workplace more accessible to all employees.
Limitations
The results of this study should be considered within the context of several limitations. First, HRS data is nationally representative but does not include much detail on the gender, racial, and ethnic identity of respondents. The categories presented limit our ability to consider identity-related dynamics in retirement and likely obscure important subgroup differences. Second, disability conditions were defined based on respondents’ reports that they received a doctor’s diagnosis of a provided list of conditions. Individuals may be diagnosed with other disabilities or health conditions that were not captured in this data, for example, Multiple Sclerosis, or a spinal cord injury. The finding of gender differences was difficult to interpret because of the significant social changes that women have experienced in the workplace concerning their careers, and their expected roles within families and as caretakers. The women in the sample belong to different age cohorts, including those born before 1924. This issue, combined with the odds ratio, suggested a conservative approach to the interpretation of the finding that women were slightly more likely than men to experience forced retirement. Future research, with better contextual information on retirement and career context, should explore gender more fully. A sensitivity analysis was conducted to identify any potential differences for those who retired before age 55 compared with 55 or older, and the results were largely the same. Future research may also consider subgroup analyses to explore potential differences between age cohorts within the broader middle-aged worker population. As with other secondary data analyses, the concepts of interest were defined based on an available set of variables. Other conclusions may have been drawn if other data were collected or considered. For example, the role of work accommodations was not available for this analysis but is an important area of future research as it pertains to older workers with CID and retirement contexts. Finally, results are based on cross-sectional analyses and are not meant to imply causality. The interpretation that the presence of CID puts individuals at increased risk of forced retirement is reasonable and aligned with previous research. Alternative conclusions are also possible.
Conclusion
Sociodemographic risk factors for health disparities also emerge as related to involuntary retirement, and health appears to be a significant driver of involuntary retirement among middle-age and older workers. SVRAs are an available resource that could be leveraged to support continued employment among those who incur CID, but would like to retain their jobs. Unfortunately, they are largely unknown to those outside of the disability community. The SVRAs, to support older workers with CID seeking job retention support, may consider expanding their community outreach to medical centers and facilities that specialize in chronic illness treatment, and advertising the availability of expertise in job accommodations and assistive technology to get the attention of employers who may wish to retain valued employees.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.