
Abstract
This review identified interventions delivered by rehabilitation counselors and evaluated their effectiveness in delivering identified outcomes. We searched eight electronic databases for quantitative studies with results of interventions that rehabilitation counselors delivered in part or entirely. The Mixed Methods Appraisal Tool identified the quality of extracted studies, and the National Health and Medical Research Council’s strength-of-evidence criteria determined intervention effectiveness. From 2,125 search citations, 35 publications reported outcomes from 23 interventions tested in 25 studies. Studies comprised nine randomized controlled trials, six non-randomized control/comparison group studies, and ten treatment-only cohort studies. Most studies were moderate to high quality and were from the United States. Fifteen interventions had adequate strength of evidence to be deemed effective compared to treatment-as-usual or comparison interventions. Effective interventions were for people with mental health and substance use conditions, learning, intellectual, and developmental disabilities, physical trauma or injury, autoimmune disease, visual loss, and broadly defined disability. Results reinforce rehabilitation counselors’ utility in effectively improving vocational and psychosocial outcomes in varied service settings and with diverse populations. Findings offer a benchmark for research development that evaluates interventions delivered by rehabilitation counselors in existing and emerging areas of practice areas.
Rehabilitation counseling has a long history of service and advocacy within diverse population groups, with common themes among client groups being the presence of disability, disadvantage, and barriers to participation. Enabling and supporting people who experience disability and disadvantage to prepare for, secure, return to, or maintain work is a guiding principle in most rehabilitation counseling interventions and settings (Buys et al., 2015; Patterson et al., 2012). In addition, work is often the goal and the outcome used to promote the integration of rehabilitation counselors in varied health and community-based settings (Fraser et al., 2019).
As acknowledgment and evidence have strengthened on the wide-ranging benefits of meaningful work and broader participation for people with disabilities (Saunders & Nedelec, 2014), so too has the vocational focus and expectation that rehabilitation counseling practice is accountable and uses evidence-based interventions (F. Chan et al., 2011; Leahy et al., 2018). Clients and their referrers expect rehabilitation counselors to use their knowledge and skills to help facilitate vocational goal achievement. While this “transaction” is generally understood and supported across diverse settings, such as workplace rehabilitation, disability employment services, mental health, and community reintegration, the “how” of rehabilitation counseling practice is less understood (F. Chan et al., 2011; Sherman et al., 2018).
Rehabilitation counseling approaches are considered effective and much-needed (Pruett et al., 2008). However, the documentation of these interventions is limited in the public domain (F. Chan et al., 2009; McLennan et al., 2021). Like other allied health professions, rehabilitation counseling stakeholders (consumers, carers, service providers, and experts) expect services to be accountable, evidence-based, empirically tested, and validated (P. Chan et al., 2016; Leahy & Arokiasamy, 2010; Leahy et al., 2018; Nerlich et al., 2022). Although regularly conducted rehabilitation counseling role and function studies identify competencies required for traditional and emerging areas of practice (Leahy et al., 2019; Matthews et al., 2015), reviews of the existing evidence base underpinning main domains of practice have been limited, not only in frequency but also by a lack of focus on rehabilitation counselors delivering the services and interventions.
There is evidence for the effectiveness of counseling and psychotherapeutic practices (Norcross & Lambert, 2011; Wampold & Imel, 2015) and supported employment (SE) interventions for people with disabilities (Frederick & VanderWeele, 2019), both of which are significant components of rehabilitation counseling practice (P. Chan et al., 2016; Matthews et al., 2010). There are also promising, highly relevant, or effective vocational rehabilitation (VR) practices, including skills training (Bolton & Akridge, 1995), vocational counseling for people with substance use disorders (Kim et al., 2022), and models of effective VR service delivery (Boeltzig-Brown et al., 2017; Fleming et al., 2013). However, there is a general lack of substantiated, published evidence to support empirically based clinical decision-making and service provision by rehabilitation counselors (Leahy et al., 2018; Sherman et al., 2018).
A recent review by Phillips et al. (2021) examined intervention literature published in rehabilitation counseling and related fields from 2007 to 2018. The results included studies with rehabilitation interventions provided by various health professionals, including some referred to by the authors as rehabilitation specialists, vocational specialists, and similar generic roles. These specialists may have been rehabilitation counselors, but this cannot be determined because the occupations of professionals undertaking these roles were often missing from the published reporting. Although the review provided an update on the state of the intervention research in rehabilitation counseling and related settings, it did not identify interventions specifically implemented or provided by rehabilitation counselors or the effectiveness of the interventions.
This study aimed to advance the findings of Phillips et al. (2021) by systematically reviewing the literature to identify interventions delivered by rehabilitation counselors and determine their effectiveness in improving outcomes for participants. Identifying which interventions have the evidence to support clients in achieving their rehabilitation goals is an essential first step toward identifying evidence-based practice (Connor et al., 2023). Findings will also assist in mapping future research that progresses the evidence base for interventions delivered by rehabilitation counselors. We focused explicitly on rehabilitation counselors rather than generalist positions or roles because rehabilitation counselors are a recognized discipline in the field, and they complete graduate-level training as part of their qualification. We aimed to answer the following research questions: (a) Are interventions delivered by rehabilitation counselors entirely or as part of a team effective in improving outcomes for people with disabilities? (b) What are the key outcomes for people who receive effective interventions delivered by rehabilitation counselors entirely or as part of a team?
Method
This review was registered with PROSPERO (#CRD42022330715). We revised the protocol to include all participants, including familites, receiving a rehabilitation program, service, or intervention, and to identify the strength-of-evidence analysis in the data synthesis strategy. We merged two research questions to eliminate elements of duplication. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Page et al., 2021).
Search Strategy
The literature search was conducted in May 2020 using the following databases: Web of Science, Scopus, CINAHL, MEDLINE, EMBASE, ProQuest, APA PsycINFO, and Google Scholar. We developed a broad search strategy in consultation with a library scientist to ensure search terms would capture relevant data: (“rehabilitation counsel*”) AND (intervention OR therapy OR treatment OR program* OR trial OR evaluat* OR model OR “best practice” OR evidence). The initial search period was from January 2000 to May 2020. We extended the search period for publications in July 2021 and again in December 2022. We also reviewed the reference lists of included studies and relevant excluded systematic reviews to find additional studies not identified by our search.
Selection Criteria and Process
All original studies in English were eligible. Two researchers screened titles and abstracts for the following inclusion criteria:
1. The study was quantitative empirical research.
2. The authors reported the original results of a defined rehabilitation program, service, or intervention within the scope of rehabilitation counseling practice.
3. Participants received a rehabilitation program, service, or intervention.
4. Authors reported data on participants’ functioning as related to the aim of the program/service or intervention.
The full texts of publications remaining after the screening were reviewed by two researchers using the same criteria listed above plus another standard for inclusion:
5. Rehabilitation counselors delivered the program, service, or intervention entirely or as part of a team.
Any screening disagreements were resolved with discussion, involving a third reviewer if necessary.
Risk of Bias/Quality Assessment
Two reviewers independently extracted the publications’ quality assessment data using the Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018). The MMAT assesses randomized controlled trials (RCTs) for appropriate randomization, concealment allocation or blinding, intervention fidelity, complete outcome data, and dropout rate. It evaluates non-randomized studies on methods for minimizing recruitment bias, appropriately validated or standardized measurement, complete data, high response rate, and follow-up. If published information was unclear, we sought study protocols, reports, or publications to assist with appraisals. Disagreements were resolved by discussion, involving a third reviewer if necessary. Each publication’s quality score was based on the percentage of quality criteria met, with five possible totals: 20%, 40%, 60%, 80%, and 100% (Hong et al., 2018). Quality ratings of 100% were classified as high quality; studies achieving 60% to 80% were graded as moderate quality; and studies meeting 40% and below were rated as low quality.
Data Extraction
A piloted template facilitated the data extraction. One reviewer completed the initial extraction, and another provided a quality control extraction. The data extracted were author names, study location, the purpose of the study, study design, sample size, and size of intervention and control groups, the nature of participants—their disability, diagnosis, or disadvantage, age, and gender, race/ethnicity, the nature of the intervention, and reported outcomes at various time points. Interventions were categorized based on target populations and primary disability.
Data Analysis
We used the Australian National Health and Medical Research Council’s 2009 Guidelines for grading evidence to identify the strength of the evidence for each intervention (see NHMRC 2009 Guidelines in the Supplementary materials). Additional steps in this method allow for the development of practice guidelines. However, these steps were not used in the analysis because all publications identified in the search were single studies.
First, we identified the number of studies reporting an intervention. We then identified the level of evidence provided by each study’s design using the NHMRC’s potential for bias hierarchy (p.15 of the Guidelines). These levels were Level II RCTs (low risk of bias), Level III non-randomized controlled studies (moderate risk of bias), and Level IV single cohort studies (high risk of bias).
The quality of the evidence for each study was rated using the MMAT criteria as identified above (i.e., high, moderate, and low quality). Where there was more than one study reporting the same intervention for the same client group, we examined the consistency in evidence, that is, no conflicting evidence. If there was contradictory evidence, we rated the evidence as weak to identify the need for further studies. The statistical precision of each study’s findings was determined by noting whether tests using significance levels (p-value) or confidence intervals ruled out the possibility that findings were not due to chance. If testing was absent, we identified the evidence as weak.
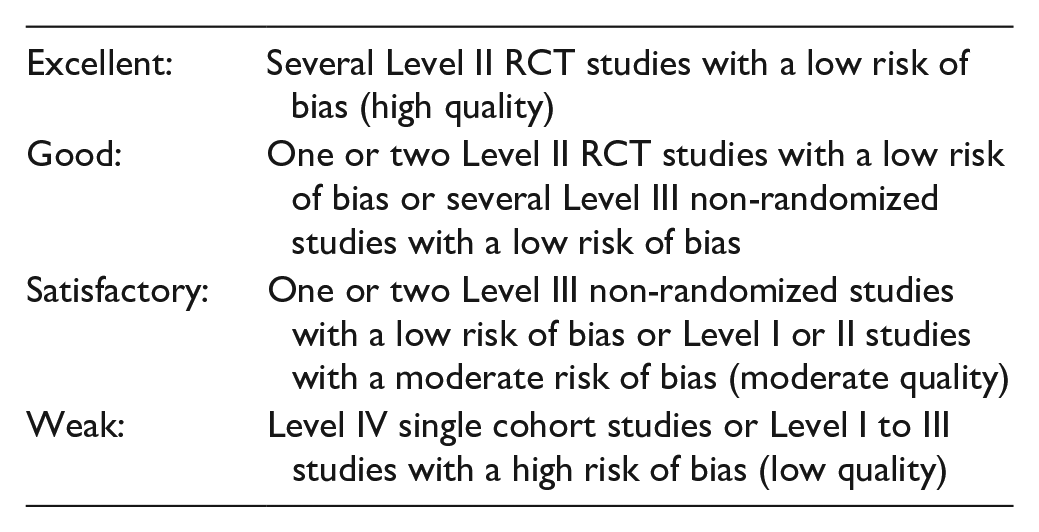
From the above, we identified the strength of evidence for each intervention using the National Health and Medical Research Council’s criteria (p.2 of the Guidelines):
An intervention must have an excellent, good, or satisfactory evidence rating to be considered effective compared to treatment-as-usual or comparison interventions. Good evidence provides more robust support for the effectiveness of intervention outcomes than satisfactory evidence. Weak evidence cannot be trusted to identify accurate differences between intervention groups and pre-post-outcome results. Therefore, it cannot identify an intervention as effective.
Results
Our search strategy identified 2,125 citations dated between 2000 and 2022, of which 183 were eligible for full review, and 36 met inclusion criteria (see Figure 1). The authors of one study’s intervention reported the same results in two publications (S. H. Allaire et al., 2003, 2005). We only included the latter study (S. H. Allaire et al., 2005) in analyses to avoid interpretation bias. Thus, our analyses included results from 35 publications that reported outcomes from 23 interventions tested in 25 studies. Most studies were field studies.
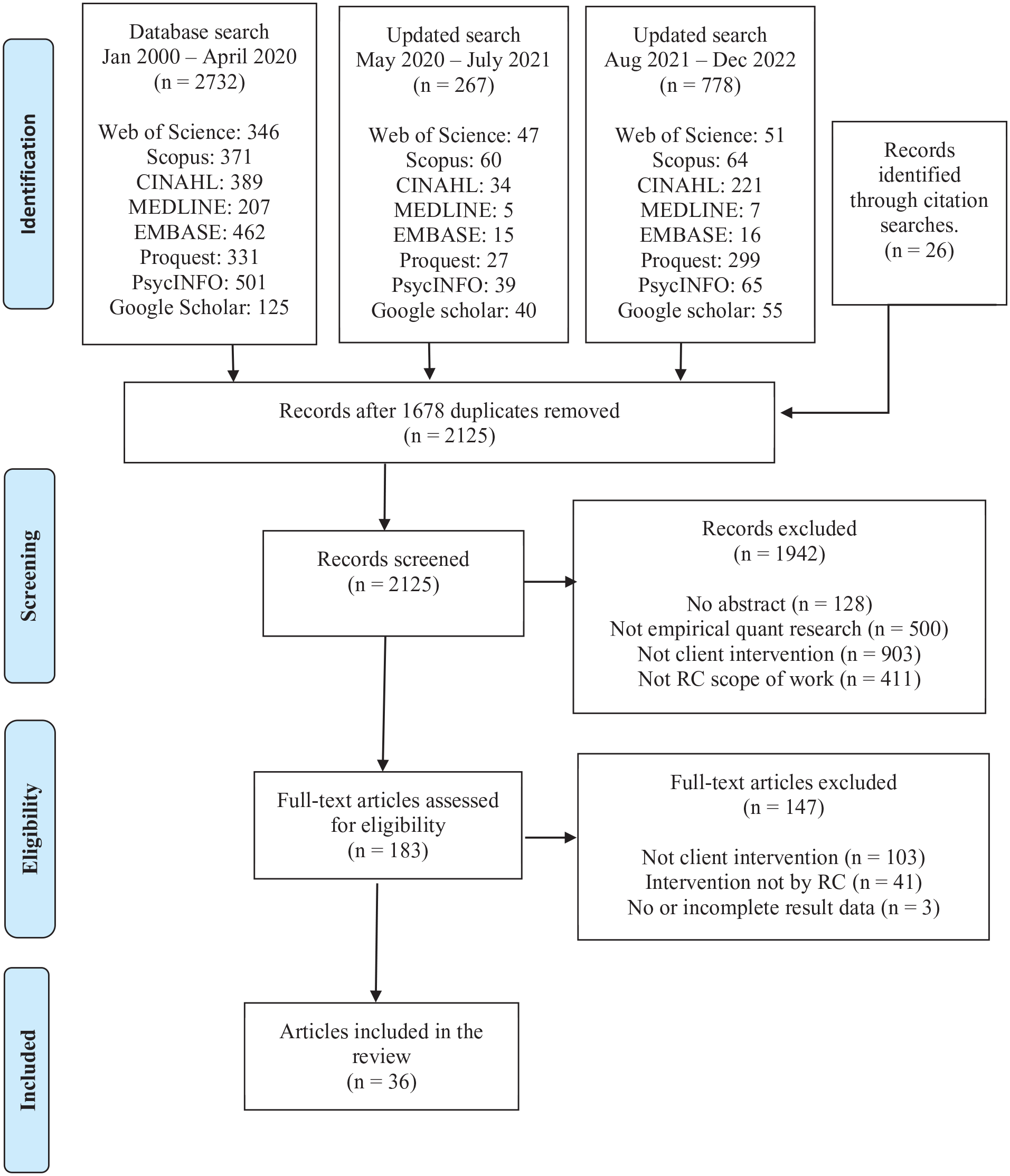
PRISMA Flowchart for Study Selection.
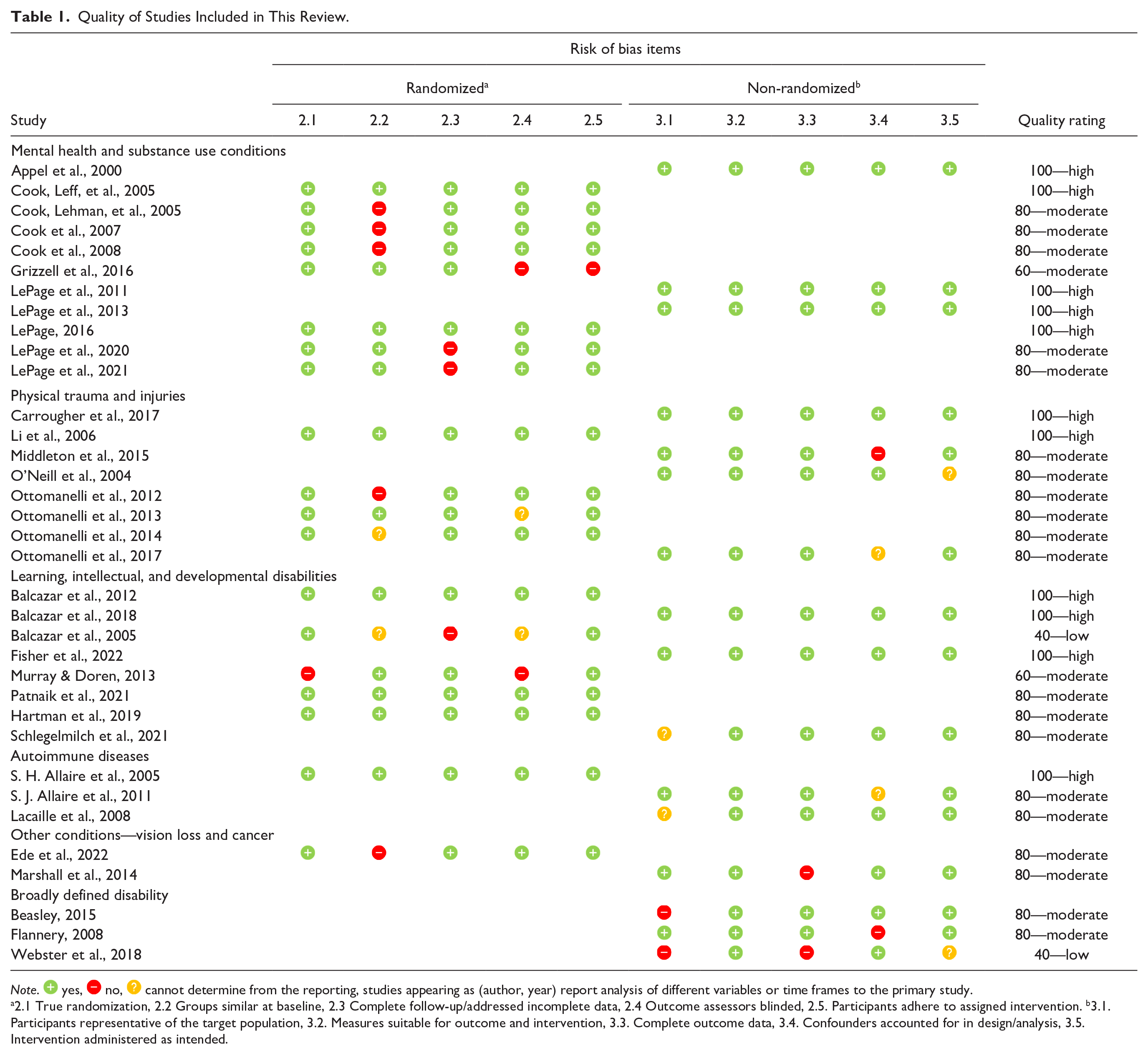
Studies comprised nine RCTs (36%), six non-randomized control or comparison group studies (24%), and 10 treatment-only cohort studies (40%). Follow-up periods were from 3 weeks (Li et al., 2006) to 4 years (S. H. Allaire et al., 2005; Hartman et al., 2019). We rated 11 studies (44%) as high quality, 12 studies (48%) as moderate quality, and two studies (8%) as low quality according to the MMAT criteria (Hong et al., 2018) (see Table 1). Most studies were conducted in the United States (n = 21, 84%), with one study each reported from Australia, Canada, Hong Kong, and Nigeria.
Quality of Studies Included in This Review.
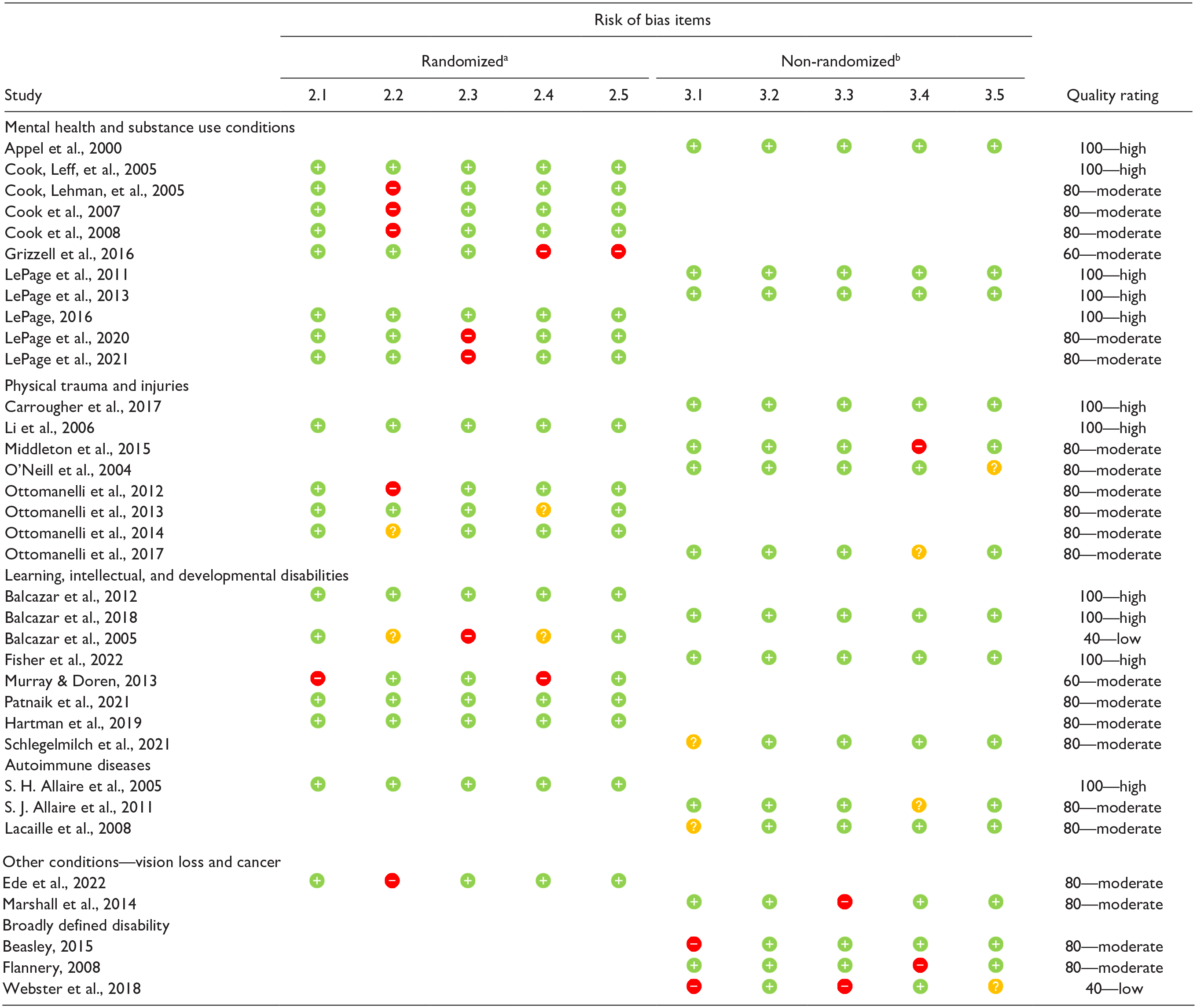
Note.  yes,
yes,  no,
no,  cannot determine from the reporting, studies appearing as (author, year) report analysis of different variables or time frames to the primary study.
cannot determine from the reporting, studies appearing as (author, year) report analysis of different variables or time frames to the primary study.
2.1 True randomization, 2.2 Groups similar at baseline, 2.3 Complete follow-up/addressed incomplete data, 2.4 Outcome assessors blinded, 2.5. Participants adhere to assigned intervention. b3.1. Participants representative of the target population, 3.2. Measures suitable for outcome and intervention, 3.3. Complete outcome data, 3.4. Confounders accounted for in design/analysis, 3.5. Intervention administered as intended.
Interventions tested were for people with mental health and substance use conditions (n = 5, 21.7%), physical trauma and injuries (n = 5, 21.7%), learning, intellectual, and developmental disabilities (n = 6, 26.1%), autoimmune diseases (n = 2, 8.7%), other conditions (n = 2, 8.7%), and broadly defined disability (n = 3, 13%). There were three interventions for military veterans within these groups.
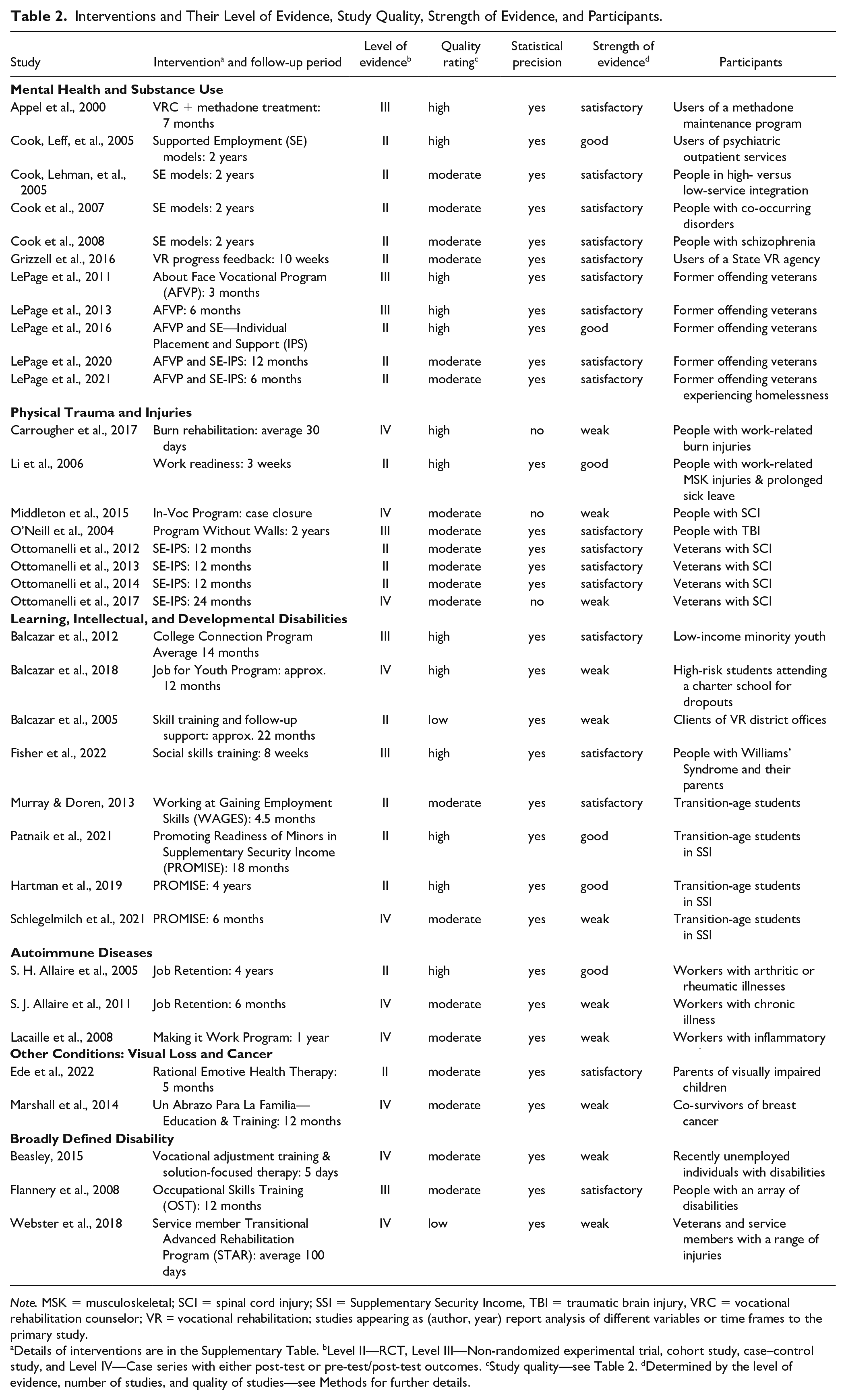
Table 1 details the results for criteria used to rate the strength of evidence for interventions. We included a rating for research presented in each publication in this review to determine the effectiveness of interventions for each reported outcome. All 23 interventions reported positive outcomes for participants, with consistent findings presented in the context of multiple studies. Fifteen interventions (65.2%) met the NHMRC’s criteria for having good or satisfactory strength of evidence. They were deemed effective interventions for participants compared to treatment as usual (TAU) or a comparison intervention.
Below is brief information about the effective interventions, the primary outcomes for participants, and differences in outcomes between the intervention and control or comparison groups. We refer readers to Table 2 and the Supplementary Table for complete details about each publication and intervention.
Interventions and Their Level of Evidence, Study Quality, Strength of Evidence, and Participants.
Note. MSK = musculoskeletal; SCI = spinal cord injury; SSI = Supplementary Security Income, TBI = traumatic brain injury, VRC = vocational rehabilitation counselor; VR = vocational rehabilitation; studies appearing as (author, year) report analysis of different variables or time frames to the primary study.
Details of interventions are in the Supplementary Table. bLevel II—RCT, Level III—Non-randomized experimental trial, cohort study, case–control study, and Level IV—Case series with either post-test or pre-test/post-test outcomes. cStudy quality—see Table 2. dDetermined by the level of evidence, number of studies, and quality of studies—see Methods for further details.
Effective Interventions
People With Mental Health and Substance Use Conditions
A large multisite randomized field trial provided good evidence that SE models combining VR and clinical services were more effective for obtaining competitive employment for people with serious mental illnesses (55% intervention vs. 34% comparison, p < .001), working over 40 hours per month (51% vs. 39%, p < .001) and having greater monthly earnings ($122 vs. $99, p = .04) than controls, even after controlling for demographics, clinical conditions, prior work history, other conditions, and receipt of disability income support (Cook, Leff, et al., 2005). Each site’s team differed depending on the SE models delivered. Arizona’s team comprised rehabilitation counselors, psychiatrists, case managers, employment specialists, job developers, and benefits specialists, and they delivered comprehensive case management and SE services to participants (Cook et al., 2008).
In the same SE trial (Cook, Leff, et al., 2005), lower quality ratings resulted in satisfactory evidence to support findings that people with comorbidities receiving SE had significantly higher average rates of competitive employment (39% vs. 29%, p < .001), hours worked (515 vs. 409, p < .05), and increased earnings ($2,882 vs. $2,262, p < .05) than those in the comparison group (Cook et al., 2007). There was satisfactory evidence to support the findings that people with schizophrenia who received SE were 4.83 times more likely to obtain competitive employment than those in the control group (Cook et al., 2008). Finally, there was satisfactory evidence that high-level integration of clinical and vocational services doubled the likelihood of participants gaining employment. Participants were also 1.25 times more likely to work more than 40 hours per month than those receiving low-level integration services (Cook, Lehman, et al., 2005).
An RCT conducted by LePage et al. (2016) tested the About Face Vocational Program (AFVP) combined with Supported Employment—Individualized Placement and Support (SE-IPS) to AFVP alone to measure the impact on employment outcomes of previously incarcerated veterans with mental health conditions. Rehabilitation counselors delivered both the AFVP and IPS programs. At the 6-month follow-up, significantly more participants receiving AFVP + SE-IPS achieved competitive employment (46% vs. 21%, p < .05, odds ratio 3.5). They attained competitive employment more quickly (131 vs. 157 days, p = .02) than those receiving AFVP alone (LePage et al., 2016). Similar findings were reported at 12 months, with a higher employment rate for those receiving the AFVP + SE-IPS (57% vs. 37%, p = .041) and more quickly attained employment (210 vs. 278 days, p = .005) than those in the AFVP group (LePage et al., 2020). Although good evidence supported the 6-month outcomes (LePage et al., 2016), the evidence supporting the 12-month results was rated as satisfactory due to the lower quality rating of the reported research (LePage et al., 2020). Analysis of a subset of veterans who were experiencing chronic homelessness reported 6-month findings similar to the patterns of those reported above, where the intervention group had outcomes significantly higher than the comparison group. The strength of the evidence underlying the results in this study was satisfactory (LePage et al., 2021).
Earlier work by LePage et al. (2011, 2013) examined the employment outcomes of veterans receiving the stand-alone AFVP intervention delivered by a rehabilitation counselor compared with those doing a self-directed program or standard vocational services. There was satisfactory evidence that the intervention resulted in significantly better competitive employment outcomes than other conditions (23.8% intervention vs. 3% self-study vs. 0% standard, p < .05) at 3 months (LePage et al., 2011). At the 6-month follow-up, competitive employment outcomes followed a similar pattern to the 3-month outcomes (40.7% vs. 11.9% vs. 16.7%, p < .05). There were no differences between the standard and self-study conditions. Participants in the AFVP program obtained employment significantly quicker and remained employed for longer than the other groups (LePage et al., 2013).
For clients attending a methadone maintenance treatment program, a satisfactory strength of evidence supported the inclusion of a VR counselor in the clinic to improve vocational and educational activity and outcomes for participants (Appel et al., 2000). The intervention increased non-working participants’ chances of being vocationally involved at 7 months post-intervention by 2.4 times more than those receiving standard treatment. Positive changes were achieved significantly quicker (within 3 months) by recipients of the intervention (65%) than for those who did not receive the intervention (30%). Work history played a role in vocational outcomes, as did the rehabilitation counselor’s clinical judgments and assessments of participant readiness.
Grizzell et al.’s (2016) RCT evaluated the impact of incorporating feedback on progress with vocational goals on mental health and perceived employment by people receiving rehabilitation services in the State VR system. Rehabilitation counselors delivered the intervention within a group-based VR counseling intervention. There was satisfactory evidence that the intervention (M = 5.54, SD = 3.26) was more effective than group-based VR counseling alone (M = 4.42, SD = 3.18, p = .006) for improving participants’ perceptions of employment progress. The effect of the intervention for three elements of mental health—interpersonal relationships (p = .025), social role performance (p = .021), and overall mental health functioning (p = .028)—was conditional on receiving public benefits. Employment rates increased significantly over time for the entire sample (17% to 50%, p = .012) but did not differ significantly between groups.
People With Physical Trauma and Injuries
An RCT conducted by Li et al. (2006) evaluated the effectiveness of a 3-week work readiness training program for workers with musculoskeletal injuries on long-term sick leave compared to being advised on job placement. Based on the employment readiness model, the program helped injured workers address psychological and psychosocial problems and facilitate return to work. Good evidence supported findings that the intervention resulted in better outcomes for injured workers than solely advising on job placement. The training program, delivered by a multidisciplinary team including rehabilitation counselors, occupational therapists, and social workers, involved individual vocational counseling and group-based interventions on skill-building and pain and stress management. Compared to controls, recipients of the intervention reported significant improvements in anxiety (p < .05), self-perceived health status (p < .02), and work readiness (p < .05).
O’Neill et al. (2004) reported the utility of the Program Without Walls (PWW) intervention, a person-centered community-based approach to VR, in promoting employment after traumatic brain injury (TBI) when compared to traditional VR services. The PWW was designed and managed by rehabilitation counselors who recruited, trained, and supervised freelance consultants to deliver the program components to participants. There was satisfactory evidence of PWW delivering higher rates of successful case closure (57% vs. 24%, p = .03), more significant improvements in participants’ mean income ($328.70 vs. $124.99, p = .03), and number of hours worked per week (32.08 vs. 17.80, p = .04), than those receiving traditional VR.
There was satisfactory evidence from a 2-year multisite randomized field trial (Ottomanelli et al., 2012) that SE-IPS was more effective for veterans with spinal cord injuries (SCIs) in obtaining competitive employment (SE, 25.9%) than TAU (10.5%) and TAU at an observation site (TAU-OS, 2.3%) at 1-year follow-up (p < .002). Participants in the SE group worked significantly more hours than TAU and TAU-OS (6.5 vs. 2.0 vs. 0.7, p < .001) and earned significantly more income than TAU-OS ($234 vs. $150, p < .05) but not TAU-IS ($279, p < .05) (Ottomanelli et al., 2012). There was a similar pattern in results for competitive employment at the 2-year follow-up, with the SE group obtaining and maintaining higher rates of SE (18.5%) than TAU-IS (6.6%, p = .036). However, hours worked by SE were fewer than TAU-IS (4.1 vs. 2.7, p < .001), and earnings were higher than TAU-IS ($251 vs. $74, p < .05). There was no new employment in the TAU-OS (Ottomanelli et al., 2014). Rehabilitation counselors integrated into the SCI clinical team delivered the intervention. The health and disability function of participants in the study did not differ post-intervention. However, those from both groups who became employed reported improved social integration (p < .05) and mobility (p < .05) (Ottomanelli et al., 2013).
People With Learning, Intellectual, and Developmental Disabilities
The College Connection Program (CCP; Balcazar et al., 2012) provided outreach and training, post-secondary support, job development, and on-the-job support to low-income minority youth with disabilities. Case managers worked with special education personnel, staff from disability services, teachers, rehabilitation counselors, local employers, business managers, and supervisors to deliver the program. Rehabilitation counselors contributed to CCP’s job development activities. There was satisfactory evidence of CCP’s effectiveness in achieving significantly higher enrollment in and completion of post-secondary education (82% vs. 50%, p < .01) and better employment outcomes (74% vs. 23%, p < .01) than those in the comparison group. Intervention participants reported a significant wage increase after completing the program ($6.58 pre vs. $8.02 post, p < .01).
Fisher and colleagues (2022) conducted a non-randomized controlled study that provided satisfactory evidence for the effectiveness of a social skills program for adults with Williams Syndrome (WS; neurodevelopmental disability). The program comprised synchronous online training delivered in 16 group sessions over 8 weeks to adults with WS and their parents. It involved social skills instruction, practice, and feedback. The lead facilitator was a rehabilitation counselor, and the assistant facilitator was a teacher. Compared with the waitlist control group, intervention participants showed more significant gains in social skills knowledge (p = .014). Parents rated their adult children as displaying significant gains in social skills post-intervention (p < .001).
Studies by Patnaik et al. (2021) and Hartman et al. (2019) reported the outcomes of the Promoting Readiness of Minors in Supplementary Security Income (PROMISE) intervention for youth and their families, evaluated using a multisite RCT. Patnaik et al. (2021) reported the large-scale six-model demonstration site project results. Hartman et al. (2019) provided the Wisconsin PROMISE study findings. Both provided good evidence to support the effectiveness of PROMISE delivering better results for a wide range of components. These included VR enrollment, which was >300% of the control group mean, and families’ use of support services, which reported a 65% increase in the control group mean (Patnaik et al., 2021). Employment outcomes increased from 1% in 2013 to 67% in 2018, 10% higher than observed in the control group (Hartman et al., 2019).
The PROMISE intervention included case management, motivational interviewing, work incentive benefits counseling, financial capability building, career development counseling, and support navigating transition resources. Teams delivered services, and the staff varied between sites. Teams from the California and Wisconsin sites included rehabilitation counselors, project staff, and other specialists, including financial literacy coaches, education specialists, and benefits counselors. Rehabilitation counselors at the California site delivered employment services with project staff and job coaches. In contrast, rehabilitation counselors at the Wisconsin site delivered case management services, including developing employment plans, school support, and assisting participants in completing health promotion and literacy training.
Murray and Doren (2013) conducted an RCT to identify the impact of the Working at Gaining Employment Skills (WAGES) intervention, which focused on increasing the social and occupational skills of adolescents with disabilities. A team, including teachers, school personnel, and rehabilitation counselors, delivered the intervention. There was satisfactory evidence that students receiving WAGES achieved better results than students receiving TAU. Students receiving the intervention reported higher vocational expectations (p < .05) and empathy (p < .05) post-intervention than students in the control group. Teacher-rated outcomes noted significantly better occupational skills (p < .001), cooperation (p < .01), and assertiveness (p < .01) in students receiving WAGES than students in the control group.
People With Autoimmune Diseases
An RCT testing the impact of a job retention program for employed people with rheumatic diseases provided good evidence for the effectiveness of VR compared to the provision of printed disability management resources (S. H. Allaire et al., 2005). For the intervention group, rehabilitation counselors delivered services and support by identifying work barriers and solutions, providing vocational counseling and education, and helping with self-advocacy. More intervention group participants remained employed at 12 months (96%), 24 months (92%), and 36 months (84%) than controls for the same periods (90%, 76%, and 70%, respectively, p = .03).
Other Conditions
An RCT conducted by Ede et al. (2022) evaluated a manualized program of rational emotive family health therapy delivered to parents of children with visual impairment in Nigeria. The 12-weekly sessions used rational emotive behavior therapy, and a 4-week top-up following the treatment used motivational interviewing and motivational enhancement, with assessments and treatments conducted by rehabilitation counselors, mental health counselors, and clinical psychologists. The intervention group reported significantly increased self-rated family values (p < .001) and quality of family life (p < .001) post-intervention when compared to the control group. The impact of the intervention and top-up sessions continued over time, with differences between groups on both measures remaining significant at the 5-month follow-up (p < .001).
People With Broadly Defined Disabilities
The Occupational Skills Training (OST) program, evaluated by Flannery et al. (2008), provided satisfactory evidence of its effectiveness for those completing OST, who attained significantly higher hourly wages ($9.35 vs. $7.89, p < .05), work hours (291 vs. 197, p < .05) and worked more than 75% of the possible quarters 1 year after exit (46.2% vs. 14%) than non-completers. The OST program primarily used individualized and worksite-based training plans. A collaboration between a skills trainer who developed training plans, an employment specialist who developed the training work site, a worksite employer who provided the direct skills training, and a rehabilitation counselor and high school transition specialist who delivered case management helped students with disabilities to improve employment outcomes.
Discussion
This review identified interventions delivered in part or entirely by rehabilitation counselors published between 2000 and 2022. In addressing our research questions, all interventions identified by our search reported positive participant rehabilitation outcomes. However, an analysis of the scientific evidence supporting the interventions found that only 15 of the 23 interventions met the strength of evidence required to verify their effectiveness in improving vocational, educational, and quality-of-life outcomes for people with disabilities. Our findings add a suite of interventions to existing effective rehabilitation counseling practices such as counseling, skill training, and working alliance (P. Chan et al., 2016; Pruett et al., 2008) by providing evidence of the value to recipients of the identified interventions compared to TAU. They also provide a benchmark for future research that bolsters the evidence base underpinning rehabilitation counseling practice.
Our findings build on those of Phillips et al. (2021) by identifying the effectiveness of interventions explicitly delivered by rehabilitation counselors, as opposed to rehabilitation professionals more generally, and by providing a broader capture of studies relating to rehabilitation counseling interventions with disadvantaged youth, people with learning, intellectual, and developmental disabilities. Specifically, our results show that rehabilitation counselors effectively deliver interventions to client groups for which others have noted employment and other vocational outcomes as particularly challenging. These include people with severe mental health and substance use disorders (Fossey & Harvey, 2010), military veterans with mental health and substance use disorders (Romaniuk et al., 2023), disadvantaged youth with disabilities (Iwanaga et al., 2021), and people with physical trauma and injuries (Sveen et al., 2020).
Building on the findings from previous VR systematic reviews, the studies included in this review also provide compelling evidence of the effectiveness of VR in improving work outcomes for people with disabilities (Bolton & Akridge, 1995; Fleming et al., 2013; Pruett et al., 2008). The findings reveal that rehabilitation counselors have effectively used VR in numerous ways, including vocational assessment and counseling, job development and placement, occupation and social skills training, and case management. With common elements across multiple studies, these interventions have proven successful in helping individuals with disabilities achieve their vocational goals.
A feature of several effective interventions was integrating VR services provided by rehabilitation counselors, often in teams, in partnership with two or more organizations. Partnerships with special education, disability services, state VR agencies, local high schools, the university sector, and local employers enabled a collaboration of expertise that improved outcomes for youth and young adults with disabilities. The success of these integrations supports previous work that identified interagency collaborations as widely referenced as best practices (Fleming et al., 2013). For example, the effectiveness of integrating vocational and clinical services in SE models reported in this review has accumulated through the decades of SE research to which rehabilitation counselors have contributed (F. Chan et al., 2011). Furthermore, our findings support those of previous authors that suggest integrating VR counseling services and a return-to-work focus with other needed interventions may be essential to augmenting recovery and rehabilitation outcomes (Fadyl & McPherson, 2010; Kim et al., 2022; Malec & Moessner, 2006), although further investigation of these synergistic effects is warranted.
Successful interventions by rehabilitation counselors significantly improved employment- and education-related functioning, which ultimately helped people meet their personal, academic, and career goals. These interventions reduced time attaining employment, improved income, increased education, increased vocational activity, enhanced work readiness and expectations, and improved work retention. Beyond employment and education, these interventions have also improved people’s health and well-being by enhancing their social skills and mental health, reducing stress and anxiety, and improving their quality of family life. Intervention recipients also had health improvements, including better mobility and other health statistics. Some high-quality studies in this review reported other positive outcomes. However, factors like lack of control or comparison groups limited the strength of the evidence for those interventions. As a result, it was impossible to determine whether the outcomes achieved were entirely due to the intervention.
As expected, the roles of rehabilitation counselors in their contributions to effective interventions varied. In large multisite SE and PROMISE RCTs, rehabilitation counselors worked as part of integrated multidisciplinary teams that provided clients with the required services to achieve their goals. However, rehabilitation counselors were leading in delivering services in smaller SE RCTs. Some studies had rehabilitation counselors designing, delivering, and supervising the intervention, while others integrated rehabilitation counselors into existing rehabilitation teams. The evidence from these different modes and degrees of rehabilitation counselor contribution suggests the value of their skill sets in individual and team-based capacities.
Strengths of This Study
A notable strength is the inaugural nature of the review, the first to focus solely on interventions delivered in part or entirely by rehabilitation counselors. Another strength was using the National Health and Medical Research Council’s 2009 scientific system for grading the strength of evidence for each intervention, which advanced the analysis from evidence identified by study design (evidence hierarchies) to a broader evaluation of several study domains.
Another noteworthy strength of the evidence was the overall high quality of the extracted publications, with most studies satisfying 80% or more of the MMAT quality criteria. This finding was noteworthy because most interventions were evaluated in the field rather than in a clinical setting where variables are easier to control. Although testing interventions in participants’ environment and context increases the external validity of the findings, it also increases the logistical complexity of undertaking the research; it reduces researchers’ ability to control confounding elements, including recruitment biases and contamination (Smith et al., 2015). Further bolstering the evidence base was the dominance of RCTs and non-randomized studies, as opposed to single cohort studies. The preponderance of longitudinal, repeated measures experimental designs and the overall high quality of the studies examined paint a positive picture of the research capacity of the rehabilitation counseling profession.
Study Limitations
We used a broad search strategy to capture as many relevant citations as possible. Still, the search may have found only some publications due to inconsistent database indexing and the limited search period applied to the search. Compared to the number of studies identified in the Phillips et al. (2021) review, very few intervention studies identified rehabilitation counselors as having a role in their delivery, despite the call for research documenting professional efficacy in the vocational domain since the 1990s, possibly earlier (Millington & Reed, 1997). Rehabilitation counselors likely contributed to intervention research during the review period not identified by this review, possibly because authors identified them as rehabilitation professionals, rehabilitation practitioners, or similar. Hence, the strength of evidence identified for some interventions may be a partial calculation but an underestimation. Furthermore, we excluded some intervention studies conducted by rehabilitation counselors for not reporting complete post-intervention data in the publication (Ferdinandi & Bethea, 2006; Ferdinandi & Eschenauer, 2008; Ferdinandi & Li, 2007). We also excluded studies where rehabilitation counseling students delivered interventions (Lu, Oursler, Herrick, Gao, Beninato, Durante, et al., 2022; Lu, Oursler, Herrick, Socha, et al., 2022; Lu, Oursler, Herrick, Gao, Beninato, Bazan, et al., 2022; Lu, Oursler, Herrick, Gao, Beninato, Minor, et al., 2022).
There remains a substantial portion of stand-alone studies with no extension or duplication of results, also previously mentioned by those conducting related systematic reviews (see Fleming et al., 2013; Phillips et al., 2021; Saunders & Nedelec, 2014). Although SE models included in this review already have a substantial body of evidence supporting their effectiveness and standing as an evidence-based practice, the effectiveness of other interventions has not been validated sufficiently for designation as an evidence-based practice because of a lack of high-quality replication research.
All citations in the review reported positive findings, which may reflect publication bias, in which studies reporting no or negative impact were not published. Related to publication bias was the language bias arising from limiting studies to those in English in that significant intervention results are more likely to be published in English (Egger & Smith, 1998). Most studies were published in the United States, so readers need caution when generalizing findings to other countries with different health, social, and economic systems.
Some limitations inherent in rehabilitation research were evident in included studies, for example, small sample sizes, which may present reporting bias, and problems establishing control groups due to ethical and empowerment considerations for rehabilitation clients (Grizzell et al., 2016; O’Neill et al., 2004). Furthermore, two studies were limited by restrictions related to COVID-19, leading to minor changes in the study protocol and outcome assessment (Ede et al., 2022; Fisher et al., 2022). Incomplete reporting of study methods and procedures limited the ability to identify potentially good evidence. For example, in some cases, we could not determine whether samples were similar at baseline because the authors did not provide this information in the text or via analyses. In some cases, it was difficult to distinguish the independence of reported samples that evaluated the same intervention, so the number of studies testing interventions may not be accurate.
Future Research
Phillips et al. (2021) noted, as we have done, that while rehabilitation counselors have a clear role in improving psychosocial outcomes for diverse population groups, some rehabilitation counseling interventions remain insufficiently validated due to limited evaluation resourcing and a lack of high-quality replication research. We also note that for nearly 20 years, rehabilitation counseling scientists have called for replication research to enable the discipline to move closer toward evidence-based practices (see Saunders et al. 2006). We echo their sentiments. Although funding and other systemic barriers remain significant hurdles to conducting intervention research (Fleming et al., 2013; Phillips et al., 2021), rehabilitation counselors must have meaningful discussions on ways to advance the discipline’s intervention evidence base. This action is vital to meeting the community’s and stakeholders’ expectations of rehabilitation counseling services as evidence-based, empirically tested, and validated. Such research must design and replicate relevant intervention studies using robust study designs, comprehensive reporting, and reporting rehabilitation counselors’ contributions to interventions to allow for the evidence synthesis required to build the evidence needed for evidence-based practice.
Rehabilitation counselors’ use of evidence identified in this and previous reviews in their practice is a related focus. Not all interventions relevant to rehabilitation counseling get published in rehabilitation counseling journals (Phillips et al., 2021), and not all published interventions are effective in delivering better outcomes than TAU, as this review identifies. To encourage the adoption of the expanding evidence in ways that best support the rehabilitation counseling profession’s aims and the people it serves, it is essential to understand how rehabilitation counselors use the evidence in their practice and engage in targeted translation activities.
Conclusion
This review and its analysis provide new information about the science that supports client interventions delivered by rehabilitation counselors and their effectiveness for participants. Adequate evidence supported the effectiveness of 15 interventions delivered in part or entirely by rehabilitation counselors that improved educational, vocational, and psychosocial outcomes in varied service settings and with diverse populations compared to TAU and comparison interventions. Areas of practice covered include people with psychiatric and substance use disorders, chronic illness and disability, injured workers, military veterans, and transition-age youth with disability. These interventions add to existing effective rehabilitation counseling practices and provide a benchmark to measure the growth of research evaluating interventions delivered by rehabilitation counselors. Future research must focus on validating relevant existing or required interventions using high-quality study designs and replicating studies. Overall, our findings reinforce rehabilitation counselors’ utility in improving outcomes for people who experience disability, disadvantage, and barriers to participation, therefore taking another step closer to strengthening the evidence base for rehabilitation counseling.
Supplemental Material
sj-pdf-1-rcb-10.1177_00343552251320949 – Supplemental material for Effectiveness of Interventions Provided by Rehabilitation Counselors
Supplemental material, sj-pdf-1-rcb-10.1177_00343552251320949 for Effectiveness of Interventions Provided by Rehabilitation Counselors by Lynda R. Matthews, Vanette McLennan, Glenda M. Jessup, Roxanna N. Pebdani and Julia Bloom in Rehabilitation Counseling Bulletin
Footnotes
Authors’ Notes
All study data are publicly available via the tables accompanying the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.